Premature infants have less nutritional storage capacity and an underdeveloped body, which makes them particularly susceptible to malnutrition. Nutrient surplus and deficiency are possibilities when supplemental feeding is unbalanced. However, little is known about what kids should eat once they are discharged from the hospital. Since many bodily processes depend on micronutrients, it's critical to plan supplemental nutrition with an optimum consumption in mind. This written summary describes the requirements for long-chain polyunsaturated fatty acids (LCPUFA), iron, zinc, vitamin D, calcium, and phosphate for premature newborns receiving supplemental feeding. The scientific community is beginning to acknowledge the advantages of giving premature babies iron and vitamin D supplements. But as of right now, there isn't enough information available to make firm recommendations about the addition of calcium, phosphorus, zinc, and LCPUFAs. Nonetheless, the health of premature infants depends on the following micronutrients: Large chain polyunsaturated fats (LCPUFAs) support the development of the retina and brain, while calcium and phosphorus dosages are necessary to prevent metabolic bone disease (MBD) in preterm infants. It is obvious how understanding the variability of the premature population may help adapt nutritional planning in connection to the development rate, comorbidities, and thorough clinical history of the preterm newborn, even while we wait for consensus on these micronutrients.
| Published in | European Journal of Preventive Medicine (Volume 12, Issue 2) |
| DOI | 10.11648/j.ejpm.20241202.12 |
| Page(s) | 35-46 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Premature Infants, Low Birth Weight Infants, Optimizing Nutrition, Enteral Feeding, Expressed Breast Milk, Complementary Feeding, Micronutrients, Fortification
3.1. An Important Micronutrient for Preterm LBW Infants Is Iron
3.2. Zinc Is an Essential Component for Preterm Low Birth Weight Infants
3.3. Premature Babies Frequently Experience Early Neonatal Hypocalcemia; This Is Where Calcium and Phosphorus Come in
AAP 2013 | ESPGHAN 2010 Other | Guidelines |
|---|---|---|
Birth Weight <1500 g: 200-400 IU/day | 400—800UI/day | 800—1000UI/day |
Birth Weight >1500 g: 200-400 IU/day | ||
AAP: American Academy of Pediatrics; g: grams; UI: International Unit; ESPGHAN: European Society for Paediatric Gastroenterology Hepatology and Nutrition | ||
6.1. Growth Rate with Basic Nutritional Practices
6.2. Existing Nutritional Strategies
6.2.1. Expressed Breast Milk
Recommendations in agreement about the use of breast milk to nourish premature infants: |
|---|
1) Mother-expressing breast milk is the primary option for human milk used to nourish preterm newborns; donor pasteurized human milk is the second option.2) The term "donor pasteurized human milk" should be used for donor milk.3) Human milk should be pasteurized in a pasteurizer; donor human milk should never be served unpasteurized.4) Donor pasteurized human milk should be screened for bacterial growth, hepatitis B antigen (HBsAg), hepatitis C virus (HCV), HIV, and venereal disease using pertinent tests and cultures.5) Within six months of donating milk, the donor mother should also be tested for HIV, HCV, HBsAg, and venereal disease. |
1) Pooled milk may be utilized if there are local milk banks, as long as the right permissions have been granted.2) When it comes to pasteurizing pooled tiny aliquots of breast milk, milk banks should communicate with agencies.3) Although the human milk analyzer is a useful tool to analyze the nutrient content of human milk and enable subsequent fortification, it is currently only being used as a research tool and not in day-to-day clinical practice.4) Donor human milk may be stored at -20°C for six months. Preterm infants should not be fed milk stored for more than three months. In everyday clinical situations, the conventional fortification technique is advised. |
6.2.2. Improved Human Milk
6.2.3. Formula Milk
| [1] |
March of Dimes, Partnership for Maternal Newborn and Child Health, Save the Children, World Health Organization. Howson CP, Kinney MV, Lawn JE, editors. Born Too Soon: the Global Action Report on Preterm Birth (2012). Available from:
http://www.who.int/pmnch/media/news/2012/201204_born-toosoon-report.pdf |
| [2] | Doyle LW, Anderson PJ. Adult outcome of extremely preterm infants. Pediatrics (2010) 126: 342–51. |
| [3] | Colombo, J.; Gustafson, K. M.; Carlson, S. E. Critical and Sensitive Periods in Development and Nutrition. Ann. Nutr. Metab. 2019, 75, 34–42. |
| [4] | Langley-Evans, S. C. Nutrition in Early Life and the Programming of Adult Disease: A Review. J. Hum. Nutr. Diet 2015, 28, 1–14. |
| [5] | Ruys, C. A.; van de Lagemaat, M.; Rotteveel, J.; Finken, M. J. J.; Lafeber, H. N. Improving Long-Term Health Outcomes of Preterm Infants: How to Implement the Findings of Nutritional Intervention Studies into Daily Clinical Practice. Eur. J. Pediatri. 2021. |
| [6] | Cooke, R. J. Improving Growth in Preterm Infants during Initial Hospital Stay: Principles into Practice. Arch. Dis Child. Fetal Neonatal Ed. 2016, 101, F366–F370. |
| [7] | Gidi, N. W.; Mekasha, A.; Nigussie, A. K.; Goldenberg, R. L.; McClure, E. M.; Worku, B.; Amaru, G. M.; Tazu Bonger, Z.; Demtse, A. G.; Kebede, Z. T.; et al. Preterm Nutrition and Clinical Outcomes. Glob. Pediatric Health 2020, 7, 2333794X2093785. |
| [8] | Cormack, B. E.; Harding, J. E.; Miller, S. P.; Bloomfield, F. H. The Influence of Early Nutrition on Brain Growth and Neurodevelopment in Extremely Preterm Babies: A Narrative Review. Nutrients 2019, 11, 2029. [CrossRef] |
| [9] | Crippa, B. L.; Morniroli, D.; Baldassarre, M. E.; Consales, A.; Vizzari, G.; Colombo, L.; Mosca, F.; Giannì, M. L. Preterm’s Nutrition Sfrom Hospital to Solid Foods: AreWe Still Navigating by Sight? Nutrients 2020, 12, 3646. |
| [10] | Hay, W. W. Nutritional Support Strategies for the Preterm Infant in the Neonatal Intensive Care Unit. Pediatric Gastroenterol. Hepatol. Nutr. 2018, 21, 234–247. [CrossRef] [PubMed] |
| [11] | Cerasani, J.; Ceroni, F.; De Cosmi, V.; Mazzocchi, A.; Morniroli, D.; Roggero, P.; Mosca, F.; Agostoni, C.; Giannì, M. L. Human Milk Feeding and Preterm Infants’ Growth and Body Composition: A Literature Review. Nutrients 2020, 12, 1155. |
| [12] | Boquien, C.-Y. Human Milk: An Ideal Food for Nutrition of Preterm Newborn. Front. Pediatr. 2018, 6, 295. |
| [13] | Morgan, J. A.; Young, L.; McCormick, F. M.; McGuire, W. Promoting Growth for Preterm Infants Following Hospital Discharge. Arch. Dis Child. Fetal Neonatal Ed. 2012, 97, F295–F298. [CrossRef] [PubMed] |
| [14] | Giannì, M.; Bezze, E.; Colombo, L.; Rossetti, C.; Pesenti, N.; Roggero, P.; Sannino, P.; Muscolo, S.; Plevani, L.; Mosca, F. Complementary Feeding Practices in a Cohort of Italian Late Preterm Infants. Nutrients 2018, 10, 1861. [CrossRef] [PubMed] |
| [15] | Baldassarre, M. E.; Giannì, M. L.; Di Mauro, A.; Mosca, F.; Laforgia, N. Complementary Feeding in Preterm Infants: Where Do We Stand? Nutrients 2020, 12, 1259. [CrossRef] [PubMed] |
| [16] | Obbagy, J. E.; English, L. K.; Psota, T. L.; Wong, Y. P.; Butte, N. F.; Dewey, K. G.; Fox, M. K.; Greer, F. R.; Krebs, N. F.; Scanlon, K. S.; et al. Complementary Feeding and Micronutrient Status: A Systematic Review. Am. J. Clin. Nutr. 2019, 109, 852S–871S. [CrossRef] |
| [17] | Brion, L. P.; Heyne, R.; Lair, C. S. Role of Zinc in Neonatal Growth and Brain Growth: Review and Scoping Review. Pediatr. Res. 2020. |
| [18] | Oliver, C.; Watson, C.; Crowley, E.; Gilroy, M.; Page, D.; Weber, K.; Messina, D.; Cormack, B. Vitamin and Mineral Supplementation Practices in Preterm Infants: A Survey of Australian and New Zealand Neonatal Intensive and Special Care Units. Nutrients 2019, 12, 51. |
| [19] | Hanson C, Sundermeier J, Dugick L, Lyden E, Anderson-Berry AL. Imple-mentation, process, and outcomes of nutrition best practices for infants <1500 g. Nutr Clin Pract (2011) 26: 614–24. |
| [20] | Donovan R, Puppala B, Angst D, Coyle BW. Outcomes of early nutrition support in extremely low-birth-weight infants. Nutr Clin Pract (2006) 21: 395–400. |
| [21] | Ganapathy S. Long chain polyunsaturated fatty acids and immunity in infants. Indian Pediatr (2009) 46(9): 785–90. |
| [22] | Lee KA, Hayes BC. Head size and growth in the very preterm infant: a litera-ture review. Res Rep Neonatol (2015) 5: 1–7. |
| [23] | Vinall J, Grunau RE, Brant R, Chau V, Poskitt KJ, Synnes AR, et al. Slower post-natal growth is associated with delayed cerebral cortical maturation in preterm newborns. Sci Transl Med (2013) 5: 168ra8. |
| [24] | Barker DJ, Winter PD, Osmond C, Margetts B, Simmonds SJ. Weight in infancy and death from ischaemic heart disease. Lancet (1989) 2: 577–80. |
| [25] | Barker DJ, Eriksson JG, Forsén T, Osmond C. Fetal origins of adult disease: strength of effects and biological basis. Int J Epidemiol (2002) 31: 1235–9. |
| [26] | Domellöf, M. Nutritional Care of Premature Infants: Microminerals. In World Review of Nutrition and Dietetics; Koletzko, B., Poindexter, B., Uauy, R., Eds.; S. KARGER AG: Basel, Switzerland, 2014; Volume 110, pp. 121–139. ISBN 978-3-318-02640-5. |
| [27] | Chaparro, C. M. Timing of Umbilical Cord Clamping: Effect on Iron Endowment of the Newborn and Later Iron Status. Nutr. Rev. 2011, 69, S30–S36. [CrossRef] |
| [28] | Cao, C.; O’Brien, K. O. Pregnancy and Iron Homeostasis: An Update. Nutr Rev. 2013, 71, 35–51. [CrossRef] Life 2021, 11, 331 11 of 13. |
| [29] | Domellöf, M.; Georgieff, M. K. Postdischarge Iron Requirements of the Preterm Infant. J. Pediatr. 2015, 167, S31–S35. [CrossRef] |
| [30] | Chockalingam, U. M.; Murphy, E.; Ophoven, J. C.; Weisdorf, S. A.; Georgieff, M. K. Cord Transferrin and Ferritin Values in Newborn Infants at Risk for Prenatal Uteroplacental Insufficiency and Chronic Hypoxia. J. Pediatr. 1987, 111, 283–286. [CrossRef] |
| [31] | Baker, R. D.; Greer, F. R.; The Committee on Nutrition. Diagnosis and Prevention of Iron Deficiency and Iron-Deficiency Anemia in Infants and Young Children (0–3 Years of Age). Pediatrics 2010, 126, 1040–1050. |
| [32] | Raffaeli, G.; Manzoni, F.; Cortesi, V.; Cavallaro, G.; Mosca, F.; Ghirardello, S. Iron Homeostasis Disruption and Oxidative Stress in Preterm Newborns. Nutrients 2020, 12, 1554. |
| [33] | Ghirardello, S.; Dusi, E.; Cortinovis, I.; Villa, S.; Fumagalli, M.; Agosti, M.; Milani, S.; Mosca, F. Effects of Red Blood Cell Transfusions on the Risk of Developing Complications or Death: An Observational Study of a Cohort of Very Low Birth Weight Infants. Amer. J. Perinatol. 2016, 34, 88–95. |
| [34] | Kelly, A. M.; Williamson, L. M. Neonatal Transfusion. Early Hum. Dev. 2013, 89, 855–860. |
| [35] | Siddappa AM, Rao R, Long JD, Widness JA, Georgieff MK. The assessment of newborn iron stores at birth: a review of the literature and standards for ferritin concentrations. Neonatology. 2007; 92: 73–82. |
| [36] | Tuerk, M. J.; Fazel, N. Zinc Deficiency. Curr. Opin. Gastroenterol. 2009, 25, 136–143. |
| [37] | International Zinc Nutrition Consultative Group (IZiNCG); Brown, K. H.; Rivera, J. A.; Bhutta, Z.; Gibson, R. S.; King, J. C.; Lönnerdal, B.; Ruel, M. T.; Sandtröm, B.; Wasantwisut, E.; et al. International Zinc Nutrition Consultative Group (IZiNCG) Technical Document #1. Assessment of the Risk of Zinc Deficiency in Populations and Options for Its Control. Food Nutr. Bull. 2004, 25, S99–S203. |
| [38] | Hambidge, K. M.; Krebs, N. F. Zinc Deficiency: A Special Challenge. J. Nutr. 2007, 137, 1101–1105. [CrossRef] |
| [39] | Harris, T.; Gardner, F.; Podany, A.; Kelleher, S. L.; Doheny, K. K. Increased Early Enteral Zinc Intake Improves Weight Gain in Hospitalised Preterm Infants. Acta Paediatr. 2019, 108, 1978–1984. [CrossRef] [PubMed] |
| [40] | Maggini, S.; Wenzlaff, S.; Hornig, D. Essential Role of Vitamin C and Zinc in Child Immunity and Health. J. Int. Med. Res. 2010, 38, 386–414. |
| [41] | Terrin, G.; Berni Canani, R.; Di Chiara, M.; Pietravalle, A.; Aleandri, V.; Conte, F.; De Curtis, M. Zinc in Early Life: A Key Element in the Fetus and Preterm Neonate. Nutrients 2015, 7, 10427–10446. |
| [42] | Sabatier, M.; Garcia-Rodenas, C. L.; De Castro, C. A.; Kastenmayer, P.; Vigo, M.; Dubascoux, S.; Andrey, D.; Nicolas, M.; Payot, J. R.; Bordier, V.; et al. Longitudinal Changes of Mineral Concentrations in Preterm and Term Human Milk from Lactating Swiss, Women. Nutrients 2019, 11, 1855. |
| [43] | Lowe, N. M.; Fekete, K.; Decsi, T. Methods of Assessment of Zinc Status in Humans: A Systematic Review. Am. J. Clin. Nutr. 2009, 89, 2040S–2051S. |
| [44] | Pediatric Nutrition in Practice, 2nd ed.; Koletzko, B. (Ed.) World Review of Nutrition and Dietetics; Karger: Basel, Switzerland; New York, NY, USA, 2015; ISBN 978-3-318-02690-0. |
| [45] | Maret, W.; Sandstead, H. H. Zinc Requirements and the Risks and Benefits of Zinc Supplementation. J. Trace Elem. Med. Biol. 2006, 20, 3–18. |
| [46] | Hess, S. Y.; Brown, K. H. Impact of Zinc Fortification on Zinc Nutrition. Food Nutr. Bull. 2009, 30, S79–S107. |
| [47] | Griffin, I. J.; Domellöf, M.; Bhatia, J.; Anderson, D. M.; Kler, N. Zinc and Copper Requirements in Preterm Infants: An Examination of the Current Literature. Early Hum. Dev. 2013, 89, S29–S34. |
| [48] | Fewtrell, M.; Bronsky, J.; Campoy, C.; Domellöf, M.; Embleton, N.; Fidler Mis, N.; Hojsak, I.; Hulst, J. M.; Indrio, F.; Lapillonne, A.; et al. Complementary Feeding: A Position Paper by the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) Committee on Nutrition. J. Pediatric Gastroenterol. Nutr. 2017, 64, 119–132. |
| [49] | Krebs, N. F. Update on Zinc Deficiency and Excess in Clinical Pediatric Practice. Ann. Nutr. Metab. 2013, 62, 19–29. |
| [50] | Kovacs, C. S. Bone Development and Mineral Homeostasis in the Fetus and Neonate: Roles of the Calciotropic and Phosphotropic Hormones. Physiol. Rev. 2014, 94, 1143–1218. |
| [51] | Koo, W. Maternal Calcium Supplementation and Fetal Bone Mineralization. Obstet. Gynecol. 1999, 94, 577–582. |
| [52] | Bozzetti, V.; Tagliabue, P. Metabolic Bone Disease in Preterm Newborn: An Update on Nutritional Issues. Ital. J. Pediatr. 2009, 35, 20. |
| [53] | Faienza, M. F.; D’Amato, E.; Natale, M. P.; Grano, M.; Chiarito, M.; Brunetti, G.; D’Amato, G. Metabolic Bone Disease of Prematurity: Diagnosis and Management. Front. Pediatr. 2019, 7, 143. |
| [54] | Chacham, S.; Pasi, R.; Chegondi, M.; Ahmad, N.; Mohanty, S. B. Metabolic Bone Disease in Premature Neonates: An Unmet Challenge. JCRPE 2020, 12, 332–339. |
| [55] | Saggese, G.; Vierucci, F.; Boot, A. M.; Czech-Kowalska, J.; Weber, G.; Camargo, C. A.; Mallet, E.; Fanos, M.; Shaw, N. J.; Holick, M. F. Vitamin D in Childhood and Adolescence: An Expert Position Statement. Eur. J. Pediatr. 2015, 174, 565–576. |
| [56] | Boy, E.; Mannar, V.; Pandav, C.; de Benoist, B.; Viteri, F.; Fontaine, O.; Hotz, C. Achievements, Challenges, and Promising New Approaches in Vitamin and Mineral Deficiency Control. Nutr. Rev. 2009, 67, S24–S30. |
| [57] | Negri, M.; Gentile, A.; de Angelis, C.; Montò, T.; Patalano, R.; Colao, A.; Pivonello, R.; Pivonello, C. Vitamin D-Induced Molecular Mechanisms to Potentiate Cancer Therapy and to Reverse Drug-Resistance in Cancer Cells. Nutrients 2020, 12, 1798. |
| [58] | Charoenngam, N.; Holick, M. F. Immunologic Effects of Vitamin D on Human Health and Disease. Nutrients 2020, 12, 2097. |
| [59] | de la Guía-Galipienso, F.; Martínez-Ferran, M.; Vallecillo, N.; Lavie, C. J.; Sanchis-Gomar, F.; Pareja-Galeano, H. Vitamin D and Cardiovascular Health. Clin. Nutr. 2020, S0261561420307007. |
| [60] | Abrams, S. A. Vitamin D in Preterm and Full-Term Infants. Ann. Nutr. Metab. 2020, 76, 6–14. |
| [61] | Council on Environmental Health and Section on Dermatology. Ultraviolet Radiation: A Hazard to Children and Adolescents. Pediatrics 2011, 127, 588–597. |
| [62] | Saggese, G.; Vierucci, F.; Prodam, F.; Cardinale, F.; Cetin, I.; Chiappini, E.; de’ Angelis, G. L.; Massari, M.; Miraglia Del Giudice, E.; Miraglia Del Giudice, M.; et al. Vitamin D in Pediatric Age: Consensus of the Italian Pediatric Society and the Italian Society of Preventive and Social Pediatrics, Jointly with the Italian Federation of Pediatricians. Ital. J. Pediatr. 2018, 44, 51. |
| [63] | Kovacs, C. S. Maternal Vitamin D Deficiency: Fetal and Neonatal Implications. Semin. Fetal Neonatal Med. 2013, 18, 129–135. |
| [64] | Isaacs EB, Gadian DG, Sabatini S, Chong WK, Quinn BT, Fischl BR, et al. The effect of early human diet on caudate volumes and IQ. Pediatr Res (2008) 63: 308–14. |
| [65] | Franz AR, Pohlandt F, Bode H, Mihatsch WA, Sander S, Kron M, et al. Intrauterine, early neonatal, and postdischarge growth and neurodevel-opmental outcome at 5.4 years in extremely preterm infants after intensive neonatal nutritional support. Pediatrics (2009) 123: e101–9. |
| [66] | Stephens BE, Walden RV, Gargus RA, Tucker R, McKinley L, Mance M, et al. First-week protein and energy intakes are associated with 18-month devel-opmental outcomes in extremely lowbirth weight infants. Pediatrics (2009) 123: 1337–43. |
| [67] | Brandt I, Sticker EJ, Lentze MJ. Catch-up growth of head circumference of very low birth weight, small for gestational age preterm infants and mental development to adulthood. J Pediatr (2003) 142: 463–8. |
| [68] | Morgan C, McGowan P, Herwitker S, Hart AE, Turner MA. Postnatal head growth in preterm infants: a randomized controlled parenteral nutrition study. Pediatrics (2014) 133: e120–8. |
| [69] | Leppänen M, Lapinleimu H, Lind A, Matomäki J, Lehtonen L, Haataja L, et al. Antenatal and postnatal growth and 5-year cognitive outcome in very preterm infants. Pediatrics (2014) 133(1): 63–70. |
| [70] | Ehrenkranz RA. Early, aggressive nutritional management for very low birth weight infants: what is the evidence? Semin Perinatol (2007) 31: 48–55. |
| [71] | Ziegler EE, Carlson SJ. Early nutrition of very low birth weight infants. J Matern Fetal Neonatal Med (2009) 22: 191–7. |
| [72] | Puntis JW. Nutritional support in the premature newborn. Postgrad Med J (2006) 82: 192–8. |
| [73] | Clark RH, Thomas P, Peabody J. Extrauterine growth restriction remains a serious problem in prematurely born neonates. Pediatrics (2003) 111: 986–90. |
| [74] | Ehrenkranz RA, Dusick AM, Vohr BR, Wright LL, Wrage LA, Poole WK. Growth in the neonatal intensive care unit influences neurodevelopmental and growth outcomes of extremely low birth weight infants. Pediatrics (2006) 117: 1253–61. |
| [75] | Su BH. Optimising nutrition in preterm infants. Pediatr Neonatol (2014) 55: 5–13. |
| [76] | Preterm and low birth weight babies. In: Bentley D, Aubrey S, Bentley M, editors. Infant Feeding and Nutrition for Primary Care. Abingdon: Radcliffe Medical Press Ltd (2004). p. 47–51. |
| [77] | Section on Breastfeeding. Breastfeeding and the use of human milk. Pediatrics (2012) 129: e827–41. |
| [78] | Schanler RJ, Shulman RJ, Lau C. Feeding strategies for premature infants: beneficial outcomes of feeding fortified human milk versus preterm formula. Pediatrics (1999) 103: 1150–7. |
| [79] | Ganapathy V, Hay JW, Kim JH. Costs of necrotizing enterocolitis and cost-effectiveness of exclusively human milk-based products in feeding extremely premature infants. Breastfeed Med (2012) 7: 29–37. |
| [80] | Vohr BR, Poindexter BB, Dusick AM, McKinley LT, Higgins RD, Langer JC, et al. Persistent beneficial effects of breast milk ingested in the neonatal inten-sive care unit on outcomes of extremely low birth weight infants at 30 months of age. Pediatrics (2007) 120: e953–9. |
| [81] | Zhou J, Shukla VV, John D, Chen C. Human milk feeding as a protective factor for retinopathy of prematurity: a meta-analysis. Pediatrics (2015) 136: e1576–86. |
| [82] | Singhal A, Cole TJ, Lucas A. Early nutrition in preterm infants and later blood pressure: two cohorts after randomised trials. Lancet (2001) 357: 413–9. |
| [83] | Singhal A, Cole TJ, Fewtrell M, Lucas A. Breastmilk feeding and lipoprotein profile in adolescents born preterm: follow-up of a prospective randomised study. Lancet (2004) 363: 1571–8. |
| [84] | Lewandowski AJ, Lamata P, Francis JM, Piechnik SK, Ferreira VM, Boardman H, et al. Breast milk consumption in preterm neonates and cardiac shape in adulthood. Pediatrics (2016) 138(1): e20160050. |
| [85] | Fewtrell MS, Williams JE, Singhal A, Murgatroyd PR, Fuller N, Lucas A. Early diet and peak bone mass: 20 year follow-up of a randomized trial of early diet in infants born preterm. Bone (2009) 45: 142–9. |
| [86] | Lucas A, Morley R, Cole TJ, Lister G, Leeson-Payne C. Breast milk and subsequent intelligence quotient in children born preterm. Lancet (1992) 339: 261–4. |
| [87] | Anderson JW, Johnstone BM, Remley DT. Breast-feeding and cognitive development: a meta-analysis. Am J Clin Nutr (1999) 70: 525–35. |
| [88] | Horta BL, Loret de Mola C, Victora CG. Breastfeeding and intelligence: a sys-tematic review and meta-analysis. Acta Paediatr (2015) 104: 14–9. |
| [89] | Belfort MB, Rifas-Shiman SL, Kleinman KP, Guthrie LB, Bellinger DC, Taveras EM, et al. Infant feeding and childhood cognition at ages 3 and 7 years: effects of breastfeeding duration and exclusivity. JAMA Pediatr (2013) 167: 836–44. |
| [90] | Deoni SC, Dean DC III, Piryatinsky I, O’Muircheartaigh J, Waskiewicz N, Lehman K, et al. Breastfeeding and early white matter development: a cross-sectional study. Neuroimage (2013) 82: 77–86. |
| [91] | Northam GB, Liégeois F, Chong WK, Wyatt JS, Baldeweg T. Total brain white matter is a major determinant of IQ in adolescents born preterm. Ann Neurol (2011) 69: 702–11. |
| [92] | Isaacs EB, Fischl BR, Quinn BT, Chong WK, Gadian DG, Lucas A. Impact of breast milk on intelligence quotient, brain size, and white matter development. Pediatr Res (2010) 67: 357–62. |
| [93] | ESPGHAN Committee on Nutrition, Agostoni C, Braegger C, Decsi T, Kolacek S, Koletzko B, et al. Role of dietary factors and food habits in the devel-opment of childhood obesity: a commentary by the ESPGHAN Committee on Nutrition. J Pediat. |
| [94] | Di Natale C, Coclite E, Di Ventura L, Di Fabio S. Fortification of maternal milk for preterm infants. J Matern Fetal Neonatal Med (2011) 24(Suppl 1): 41–3. |
| [95] |
National Neonatology Forum, India. Bhakoo ON, Kumar P, Jain N, Thakre R, Murki S, Venkataseshan S, editors. Evidence Based Clinical Practice Guidelines. (2010). Available from:
http://www.nnfi.org/images/pdf/nnf_cpg_consoli-dated_file-january102011.pdf |
| [96] | Paraskevi C. Fragkou1, Dareilena Karaviti, Michael Zemlin and Chrysanthi Skevaki: Impact of Early Life Nutrition on Children’s Immune System and Noncommunicable Diseases Through Its Effects on the Bacterial Microbiome, Virome and Mycobiome: March 2021: Frontiers in Immunology 12: 644269. |
| [97] | Francesca Manzoni, Valeria Cortesi, Giacomo Cavallaro, Fabio Mosca, Stefano Ghirardello: Iron Homeostasis Disruption and Oxidative Stress in Preterm Newborns: Nutrients 2020, 12(6), 1554; |
| [98] | Brion, L. P., Heyne, R. & Lair, C. S. Role of zinc in neonatal growth and brain growth: review and scoping review. Pediatr Res 89, 1627–1640 (2021). |
| [99] | S. H. Ralston, R. Coleman, W. D. Fraser, S. J. Gallagher, D. J. Hosking, J. S. Iqbal, E. McCloskey, D. Sampson; Medical Management of Hypercalcemia: Calcif Tissue Int (2004) 74: 1–11 |
APA Style
Khan, A. U., Hasan, S., Siddiqua, F., Sultana, S., Moniruzzaman, et al. (2024). The Significance of Providing the Optimal Micronutrients to the Preterm Low Birth Weight Infants to Prevent Long-Term Health Consequences . European Journal of Preventive Medicine, 12(2), 35-46. https://doi.org/10.11648/j.ejpm.20241202.12
ACS Style
Khan, A. U.; Hasan, S.; Siddiqua, F.; Sultana, S.; Moniruzzaman, et al. The Significance of Providing the Optimal Micronutrients to the Preterm Low Birth Weight Infants to Prevent Long-Term Health Consequences . Eur. J. Prev. Med. 2024, 12(2), 35-46. doi: 10.11648/j.ejpm.20241202.12
AMA Style
Khan AU, Hasan S, Siddiqua F, Sultana S, Moniruzzaman, et al. The Significance of Providing the Optimal Micronutrients to the Preterm Low Birth Weight Infants to Prevent Long-Term Health Consequences . Eur J Prev Med. 2024;12(2):35-46. doi: 10.11648/j.ejpm.20241202.12
@article{10.11648/j.ejpm.20241202.12,
author = {Abbas Uddin Khan and Shohrab Hasan and Farzana Siddiqua and Sabiha Sultana and Moniruzzaman and Manir Hossain and Shahidul Islam Shaheed and Aiyasha Shahid},
title = {The Significance of Providing the Optimal Micronutrients to the Preterm Low Birth Weight Infants to Prevent Long-Term Health Consequences
},
journal = {European Journal of Preventive Medicine},
volume = {12},
number = {2},
pages = {35-46},
doi = {10.11648/j.ejpm.20241202.12},
url = {https://doi.org/10.11648/j.ejpm.20241202.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ejpm.20241202.12},
abstract = {Premature infants have less nutritional storage capacity and an underdeveloped body, which makes them particularly susceptible to malnutrition. Nutrient surplus and deficiency are possibilities when supplemental feeding is unbalanced. However, little is known about what kids should eat once they are discharged from the hospital. Since many bodily processes depend on micronutrients, it's critical to plan supplemental nutrition with an optimum consumption in mind. This written summary describes the requirements for long-chain polyunsaturated fatty acids (LCPUFA), iron, zinc, vitamin D, calcium, and phosphate for premature newborns receiving supplemental feeding. The scientific community is beginning to acknowledge the advantages of giving premature babies iron and vitamin D supplements. But as of right now, there isn't enough information available to make firm recommendations about the addition of calcium, phosphorus, zinc, and LCPUFAs. Nonetheless, the health of premature infants depends on the following micronutrients: Large chain polyunsaturated fats (LCPUFAs) support the development of the retina and brain, while calcium and phosphorus dosages are necessary to prevent metabolic bone disease (MBD) in preterm infants. It is obvious how understanding the variability of the premature population may help adapt nutritional planning in connection to the development rate, comorbidities, and thorough clinical history of the preterm newborn, even while we wait for consensus on these micronutrients.
},
year = {2024}
}
TY - JOUR T1 - The Significance of Providing the Optimal Micronutrients to the Preterm Low Birth Weight Infants to Prevent Long-Term Health Consequences AU - Abbas Uddin Khan AU - Shohrab Hasan AU - Farzana Siddiqua AU - Sabiha Sultana AU - Moniruzzaman AU - Manir Hossain AU - Shahidul Islam Shaheed AU - Aiyasha Shahid Y1 - 2024/04/17 PY - 2024 N1 - https://doi.org/10.11648/j.ejpm.20241202.12 DO - 10.11648/j.ejpm.20241202.12 T2 - European Journal of Preventive Medicine JF - European Journal of Preventive Medicine JO - European Journal of Preventive Medicine SP - 35 EP - 46 PB - Science Publishing Group SN - 2330-8230 UR - https://doi.org/10.11648/j.ejpm.20241202.12 AB - Premature infants have less nutritional storage capacity and an underdeveloped body, which makes them particularly susceptible to malnutrition. Nutrient surplus and deficiency are possibilities when supplemental feeding is unbalanced. However, little is known about what kids should eat once they are discharged from the hospital. Since many bodily processes depend on micronutrients, it's critical to plan supplemental nutrition with an optimum consumption in mind. This written summary describes the requirements for long-chain polyunsaturated fatty acids (LCPUFA), iron, zinc, vitamin D, calcium, and phosphate for premature newborns receiving supplemental feeding. The scientific community is beginning to acknowledge the advantages of giving premature babies iron and vitamin D supplements. But as of right now, there isn't enough information available to make firm recommendations about the addition of calcium, phosphorus, zinc, and LCPUFAs. Nonetheless, the health of premature infants depends on the following micronutrients: Large chain polyunsaturated fats (LCPUFAs) support the development of the retina and brain, while calcium and phosphorus dosages are necessary to prevent metabolic bone disease (MBD) in preterm infants. It is obvious how understanding the variability of the premature population may help adapt nutritional planning in connection to the development rate, comorbidities, and thorough clinical history of the preterm newborn, even while we wait for consensus on these micronutrients. VL - 12 IS - 2 ER -
Department of Paediatric, Tairunnessa Memorial Medical College and Hospital, Dhaka, Bangladesh
Department of Paediatric, International Medical College and Hospital, Dhaka, Bangladesh
Department of Paediatric, Popular Diagnostics Center Gazipur, Dhaka, Bangladesh
Department of Paediatric, Shahid Tajuddin Ahmed Medical College Hospital, Dhaka, Bangladesh
Department of Paediatric, Monno Medical College and Hospital, Manikgonj, Bangladesh
Department of Paediatric, Kumudini Womens Medical College and Hospital, Mirzapur, Bangladesh
Department of Paediatric, Enam Medical College and Hospital, Savar, Bangladesh
Department of Paediatric, Enam Medical College and Hospital, Savar, Bangladesh

Figure 1. Nutritional parameters affecting positively or negatively the development of the immune system and the risk of noncommunicable diseases during the first 1000 days of life [96].

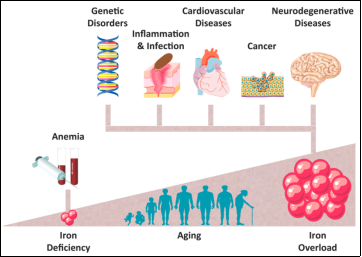
Figure 2. Iron Homeostasis Disruption and Oxidative Stress in Preterm Newborns [97].

Figure 3. Zinc role in growth and brain growth and development [98].

Figure 4. Diagnostic evaluation for hypercalcemia [99].
Information