Percutaneous kyphoplasty (PKP) and Percutaneous vertebroplasty (PVP) have become very effective to treating the Osteoporosis vertebral compression fractures (OVCFs) and patients can get immediate relief from the pain and it can improve the motor functions of patient’s health status and widely used in clinical practice. Vertebroplasty and kyphoplasty are minimally invasive procedures for the treatment of painful vertebral compression fractures (VCF), which are fractures involving the vertebral bodies that make up the spinal column. Vertebroplasty are most often used to treat an injury called a compression fracture. This kind of injuries are most often caused by osteoporosis, which is the reason of bone weakness and osteoporosis are most common in older people. This study aimed to examine the osteoporosis vertebral compression fractures (OVCFs) of Jinan, Shandong province, China, between male and female participants who were over 50 years of age. There are very few pertinent data regarding the relative or absolute contraindication of percutaneous vertebroplasty (PVP) and percutaneous kyphoplasty (PKP) for severe osteoporotic vertebral compression fractures (OVCFs). The purpose of this research was to assess and contrast the effectiveness of traditional kyphoplasty and vertebroplasty using high-viscosity cement in the treatment of severe OVCFs. In aged people, osteoporotic vertebral compression fractures (OVCFs) are prevalent and can result in significant osteoporosis vertebral compression fractures. Treatment options for individuals with these types of fractures include conservative measures, percutaneous vertebroplasty (PVP), and percutaneous kyphoplasty (PKP). We compared the clinical effectiveness of PVP and PKP in treating osteoporotic vertebral compression fractures in this investigation. Therefore, we conducted a comparative study on Osteoporosis vertebral compression fractures (OVCFs) patients who received either PVP or PKP treatment in our hospitals from January 2020 to December 2020 to investigate the clinical efficacy, advantages and disadvantages of the surgical methods, and to provide a reference for clinical selection of treatment methods.
| Published in | Journal of Surgery (Volume 12, Issue 2) |
| DOI | 10.11648/j.js.20241202.15 |
| Page(s) | 45-65 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Percutaneous Vertebroplasty (PVP), Percutaneous Kyphoplasty (PKP), Severe Osteoporotic Vertebral Compression Fractures (OVCFs)
2.1. Selection Criteria
2.1.1. Inclusion Criteria
2.1.2. Exclusion Criteria
2.2. Patients
2.3. Sample Size Determination and Baseline Data
2.4. Demographic Information and Medical History
2.5. Baseline Measurements and Pain Intensity
2.6. Functional Status
2.7. Quality of Life
2.8. Surgical Procedures and Conduct
2.8.1. Surgical Information
2.8.2. Clinical and Radiologic Assessment
2.9. Data Analysis
| [1] | Tsoumakidou, G., C. W. Too, G. Koch, et al., 2017. CIRSE Guidelines on Percutaneous Vertebral Augmentation. Cardiovascular and interventional radiology. 40, 331-342. |
| [2] | Clark, W., P. Bird, P. Gonski, et al., 2016. Safety and efficacy of vertebroplasty for acute painful osteoporotic fractures (VAPOUR): a multicentre, randomised, double-blind, placebo-controlled trial. Lancet (London, England). 388, 1408-1416. |
| [3] | Wang, H., F. Lin, G. Liang, et al., 2022. Percutaneous vertebroplasty in osteoporotic vertebral compression fracture with huge spinal epidural hematoma: A case report. Medicine. 101, e29340. |
| [4] | Diamond, T., W. Clark, P. Bird, et al., 2020. Early vertebroplasty within 3 weeks of fracture for acute painful vertebral osteoporotic fractures: subgroup analysis of the VAPOUR trial and review of the literature. European spine journal: official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 29, 1606-1613. |
| [5] | Schupfner, R., K. Koniarikova, C. Pfeifer, et al., 2021. An anatomical study of transpedicular vs. extrapedicular approach for kyphoplasty and vertebroplasty in the thoracic spine. Injury. 52 Suppl 5, S63-s69. |
| [6] | Rebolledo, B. J., B. P. Gladnick, A. Unnanuntana, et al., 2013. Comparison of unipedicular and bipedicular balloon kyphoplasty for the treatment of osteoporotic vertebral compression fractures: a prospective randomised study. The bone & joint journal. 95-b, 401-406. |
| [7] | Hinde, K., J. Maingard, J. A. Hirsch, et al., 2020. Mortality Outcomes of Vertebral Augmentation (Vertebroplasty and/or Balloon Kyphoplasty) for Osteoporotic Vertebral Compression Fractures: A Systematic Review and Meta-Analysis. Radiology. 295, 96-103. |
| [8] | Zuo, X. H., Y. B. Chen, P. Xie, et al., 2021. Finite element analysis of wedge and biconcave deformity in four different height restoration after augmentation of osteoporotic vertebral compression fractures. Journal of orthopaedic surgery and research. 16, 138. |
| [9] | Li, T., S. Pang, R. England, et al., 2023. Clinical Outcomes and Safety Comparison of Vertebroplasty, Balloon Kyphoplasty, and Vertebral Implant for Treatment of Vertebral Compression Fractures. AJNR. American journal of neuroradiology. 44, 1345-1351. |
| [10] | Ding, X., Q. Zhang, Y. Zhao, et al., 2022. Location and Effect of Bone Cement in Percutaneous Vertebroplasty for Osteoporotic Vertebral Compression Fractures. BioMed research international. 2022, 6127620. |
| [11] | Chen, M., C. Yang, Z. Cai, et al., 2022. Lumbar posterior group muscle degeneration: Influencing factors of adjacent vertebral body re-fracture after percutaneous vertebroplasty. Frontiers in medicine. 9, 1078403. |
| [12] | Hackbarth, C. B., T. J. Vogl, N. Naguib, et al., 2021. Long-term evaluation of pain reduction after vertebroplasty and kyphoplasty. Acta radiologica open. 10, 20584601211028994. |
| [13] | Sanli, I., S. M. J. van Kuijk, R. A. de Bie, et al., 2020. Percutaneous cement augmentation in the treatment of osteoporotic vertebral fractures (OVFs) in the elderly: a systematic review. European spine journal: official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 29, 1553-1572. |
| [14] | Zhang, J., X. He, Y. Fan, et al., 2019. Risk factors for conservative treatment failure in acute osteoporotic vertebral compression fractures (OVCFs). Archives of osteoporosis. 14, 24. |
| [15] | Ren, H., T. Feng, Y. Hu, et al., 2022. The Value of Dynamic Fracture Mobility in Determining the Optimum Operation Choice for Acute Osteoporotic Vertebral Compression Fracture. Journal of pain research. 15, 2327-2336. |
| [16] | Dai, C., G. Liang, Y. Zhang, et al., 2022. Risk factors of vertebral re-fracture after PVP or PKP for osteoporotic vertebral compression fractures, especially in Eastern Asia: a systematic review and meta-analysis. Journal of orthopaedic surgery and research. 17, 161. |
| [17] | He, C. J. and G. D. Liu, 2018. Comparison of the Efficacy and Safety of Bone-filling Mesh Container and Simple Percutaneous Balloon Kyphoplasty in the Treatment of Osteoporotic Vertebral Compression Fractures. Pain physician. 21, 259-268. |
| [18] | Hu, K. Z., S. C. Chen and L. Xu, 2018. Comparison of percutaneous balloon dilation kyphoplasty and percutaneous vertebroplasty in treatment for thoracolumbar vertebral compression fractures. European review for medical and pharmacological sciences. 22, 96-102. |
| [19] | Papanastassiou, I. D., F. M. Phillips, J. Van Meirhaeghe, et al., 2012. Comparing effects of kyphoplasty, vertebroplasty, and non-surgical management in a systematic review of randomized and non-randomized controlled studies. European spine journal: official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 21, 1826-1843. |
| [20] | Liu, J., J. Tang, Y. Zhang, et al., 2019. Percutaneous Vertebral Augmentation for Osteoporotic Vertebral Compression Fracture in the Midthoracic Vertebrae (T5-8): A Retrospective Study of 101 Patients with 111 Fractured Segments. World neurosurgery. 122, e1381-e1387. |
APA Style
Hossain, M. Z., Ning, B., Reyad-ul-Ferdous, M. (2024). Analysis of Clinical Outcomes of Percutaneous Kyphoplasty and Vertebroplasty in the Treatment of Osteoporosis-Induced Vertebral Compression Fracture . Journal of Surgery, 12(2), 45-65. https://doi.org/10.11648/j.js.20241202.15
ACS Style
Hossain, M. Z.; Ning, B.; Reyad-ul-Ferdous, M. Analysis of Clinical Outcomes of Percutaneous Kyphoplasty and Vertebroplasty in the Treatment of Osteoporosis-Induced Vertebral Compression Fracture . J. Surg. 2024, 12(2), 45-65. doi: 10.11648/j.js.20241202.15
AMA Style
Hossain MZ, Ning B, Reyad-ul-Ferdous M. Analysis of Clinical Outcomes of Percutaneous Kyphoplasty and Vertebroplasty in the Treatment of Osteoporosis-Induced Vertebral Compression Fracture . J Surg. 2024;12(2):45-65. doi: 10.11648/j.js.20241202.15
@article{10.11648/j.js.20241202.15,
author = {Md. Zakaria Hossain and Bin Ning and Md. Reyad-ul-Ferdous},
title = {Analysis of Clinical Outcomes of Percutaneous Kyphoplasty and Vertebroplasty in the Treatment of Osteoporosis-Induced Vertebral Compression Fracture
},
journal = {Journal of Surgery},
volume = {12},
number = {2},
pages = {45-65},
doi = {10.11648/j.js.20241202.15},
url = {https://doi.org/10.11648/j.js.20241202.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.js.20241202.15},
abstract = {Percutaneous kyphoplasty (PKP) and Percutaneous vertebroplasty (PVP) have become very effective to treating the Osteoporosis vertebral compression fractures (OVCFs) and patients can get immediate relief from the pain and it can improve the motor functions of patient’s health status and widely used in clinical practice. Vertebroplasty and kyphoplasty are minimally invasive procedures for the treatment of painful vertebral compression fractures (VCF), which are fractures involving the vertebral bodies that make up the spinal column. Vertebroplasty are most often used to treat an injury called a compression fracture. This kind of injuries are most often caused by osteoporosis, which is the reason of bone weakness and osteoporosis are most common in older people. This study aimed to examine the osteoporosis vertebral compression fractures (OVCFs) of Jinan, Shandong province, China, between male and female participants who were over 50 years of age. There are very few pertinent data regarding the relative or absolute contraindication of percutaneous vertebroplasty (PVP) and percutaneous kyphoplasty (PKP) for severe osteoporotic vertebral compression fractures (OVCFs). The purpose of this research was to assess and contrast the effectiveness of traditional kyphoplasty and vertebroplasty using high-viscosity cement in the treatment of severe OVCFs. In aged people, osteoporotic vertebral compression fractures (OVCFs) are prevalent and can result in significant osteoporosis vertebral compression fractures. Treatment options for individuals with these types of fractures include conservative measures, percutaneous vertebroplasty (PVP), and percutaneous kyphoplasty (PKP). We compared the clinical effectiveness of PVP and PKP in treating osteoporotic vertebral compression fractures in this investigation. Therefore, we conducted a comparative study on Osteoporosis vertebral compression fractures (OVCFs) patients who received either PVP or PKP treatment in our hospitals from January 2020 to December 2020 to investigate the clinical efficacy, advantages and disadvantages of the surgical methods, and to provide a reference for clinical selection of treatment methods.
},
year = {2024}
}
TY - JOUR T1 - Analysis of Clinical Outcomes of Percutaneous Kyphoplasty and Vertebroplasty in the Treatment of Osteoporosis-Induced Vertebral Compression Fracture AU - Md. Zakaria Hossain AU - Bin Ning AU - Md. Reyad-ul-Ferdous Y1 - 2024/04/17 PY - 2024 N1 - https://doi.org/10.11648/j.js.20241202.15 DO - 10.11648/j.js.20241202.15 T2 - Journal of Surgery JF - Journal of Surgery JO - Journal of Surgery SP - 45 EP - 65 PB - Science Publishing Group SN - 2330-0930 UR - https://doi.org/10.11648/j.js.20241202.15 AB - Percutaneous kyphoplasty (PKP) and Percutaneous vertebroplasty (PVP) have become very effective to treating the Osteoporosis vertebral compression fractures (OVCFs) and patients can get immediate relief from the pain and it can improve the motor functions of patient’s health status and widely used in clinical practice. Vertebroplasty and kyphoplasty are minimally invasive procedures for the treatment of painful vertebral compression fractures (VCF), which are fractures involving the vertebral bodies that make up the spinal column. Vertebroplasty are most often used to treat an injury called a compression fracture. This kind of injuries are most often caused by osteoporosis, which is the reason of bone weakness and osteoporosis are most common in older people. This study aimed to examine the osteoporosis vertebral compression fractures (OVCFs) of Jinan, Shandong province, China, between male and female participants who were over 50 years of age. There are very few pertinent data regarding the relative or absolute contraindication of percutaneous vertebroplasty (PVP) and percutaneous kyphoplasty (PKP) for severe osteoporotic vertebral compression fractures (OVCFs). The purpose of this research was to assess and contrast the effectiveness of traditional kyphoplasty and vertebroplasty using high-viscosity cement in the treatment of severe OVCFs. In aged people, osteoporotic vertebral compression fractures (OVCFs) are prevalent and can result in significant osteoporosis vertebral compression fractures. Treatment options for individuals with these types of fractures include conservative measures, percutaneous vertebroplasty (PVP), and percutaneous kyphoplasty (PKP). We compared the clinical effectiveness of PVP and PKP in treating osteoporotic vertebral compression fractures in this investigation. Therefore, we conducted a comparative study on Osteoporosis vertebral compression fractures (OVCFs) patients who received either PVP or PKP treatment in our hospitals from January 2020 to December 2020 to investigate the clinical efficacy, advantages and disadvantages of the surgical methods, and to provide a reference for clinical selection of treatment methods. VL - 12 IS - 2 ER -
Department of Orthopedic, Cheeloo College of Medicine, Shandong University, Jinan, China; Department of Orthopedic, Jinan Central Hospital, Jinan, China
Biography: Md. Zakaria Hossain has completed his Bachelor of medicine and Bachelor of surgery (MBBS) from Nanchang University, worked in Al-Haramain Hospital Sylhet, Bangladesh as an assistant doctor, 2021 awarded by Chinese government scholarship in Shandong University for master’s degree, at present in Shandong University Research works in orthopedic surgery related diseases. Bone and spinal injuries.
Research Fields: Orthopedic surgery

Department of Orthopedic, Cheeloo College of Medicine, Shandong University, Jinan, China; Department of Orthopedic, Jinan Central Hospital, Jinan, China; Central Hospital Affiliated to Shandong First Medical University, Shandong First Medical University & Shandong Academy of Medical Sciences, Jinan, China
Biography: Bin Ning Chief Physician MD, Phd. Associate Dean, Associate Director of Spine Surgery, Master and PhD Students Supervisor. Jinan central hospital vice president, Shandong University and Shandong First Medical University Professor. Deputy director of spinal surgery, Director of Jinan Key Lab of Biomechanics and Metabolism, member of the 14th Council of Shandong Medical Association, standing committee member of Jinan Youth Federation, and the chairman of Jinan Young Medical Workers Association, Shandong Provincial Committee of Spinal Surgery, Regeneration of nerve and the chairman of Jinan Medical Association, Natural Science Foundation of China and the disserta-tion reviewer of the Academic Degree and Graduate Education, BMC Musculobone Diseases, NRR and other SCI Journal Editor, published more than 30 papers in domestic nuclear journal and SCI magazine, Has been rated as Shandong Province Top Ten doctors, clinical research work of spine surgery for 18 years, govern-ment-sponsored study in Germany to learn spine surgery technology.
Research Fields: Orthopedic surgery

Department of Orthopedic, Cheeloo College of Medicine, Shandong University, Jinan, China; Institute of Biopharmaceutical and Health Engineering, Tsinghua Shenzhen International Graduate School, Tsinghua University, Shenzhen, China
Biography: Md. Reyad-ul-Ferdous B. Pharm. M. Pharm, PhD. He enrolled distance learning from The University of California San Francisco (USA); Course: Diabetes: Diagnosis, Treatment, and Opportunities, University of California San Francisco. University of Maryland, College Park (USA); Course: Genes and the Human Condition (From Behavior to Biotechnology). Vanderbilt University (USA); Case Studies in Personalized Medicine. He enrolled as a postdoctoral research scientist at department of Endocrinology and Metabolism, Shandong University. At present he also enrolls as a postdoctoral research scientist at Institute of Biopharmaceutical and Health Engineering, Tsinghua Shenzhen International Graduate School, Tsinghua University, Shenzhen, China. He has published more than 90 articles in international journals as a first and corresponding author. At present his research interests are Disease model, human genetic and metabolic diseases, Mitochondrial function and associated diseases, establishing mitochondrial uncoupling protein (UCP1) upregulated drug candidate to treat obesity related comorbidities, Pharmacology, Obesity, Metabolic diseases, Lipid metabolism in liver, Hormonal effect on NASH, Liver cancer (NASH, NAFALD, fibrosis, Liver cirrhosis), Ovarian Cancer, Neurodegenerative disease, Bone regeneration, formulation development, antioxidant, Herbal drugs and Epigenetic drugs, drug development, Phytochemistry and Phytomedicine.
Research Fields: Pharmacology, Obesity, Metabolic diseases, Lipid metabolism in liver, Hormonal effect on NASH, Liver cancer (NASH, NAFALD, fibrosis, Liver cirrhosis), Ovarian Cancer, Neurodegenerative disease, Bone regeneration, formulation development, antioxidant, Herbal drugs and Epigenetic drugs, drug development, Phytochemistry and Phytomedicine.


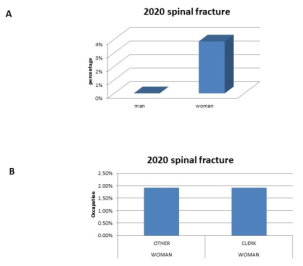
Figure 1. Displayed the percentage of spinal fractures among men and women in 2020 by employment.

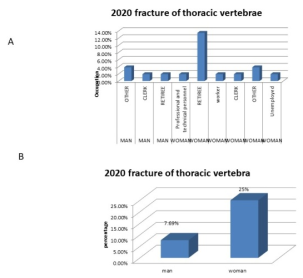
Figure 2. Demonstrated the fracture of thoracic vertebrae occupation and percentage between man and woman in the year of 2020.

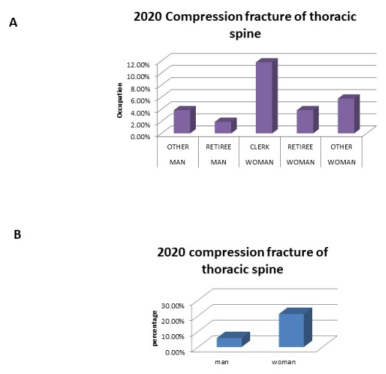
Figure 3. Demonstrated the compression fracture of thoracic spine occupations and percentage between man and woman in the year of 2020.

Figure 4. In 2020, the percentage of lumbar spinal compression fractures by occupation and the percentage of lumbar fractures by occupation were displayed.

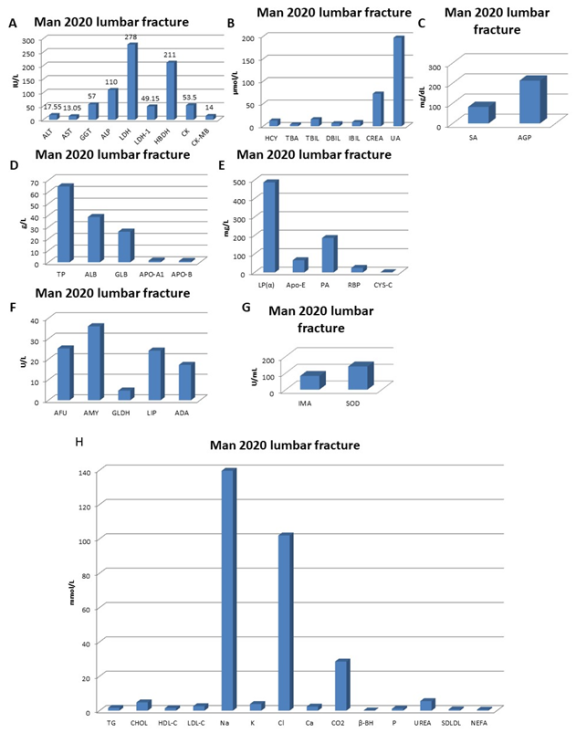
Figure 5. Man 2020's lumbar spinal compression fracture blood parameters (A-G).

Figure 6. Man 2020 with a lumbar spinal compression fracture and blood parameters.

Figure 7. Man's blood parameters for lumbar fracture in 2020 (A-H).

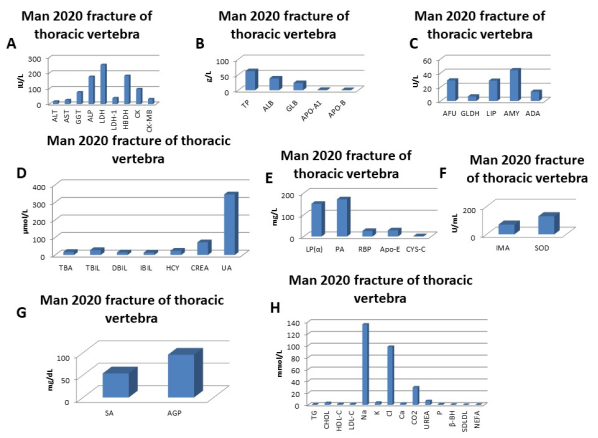
Figure 8. Blood parameter of man 2020 fracture of thoracic vertebrae (A-H).

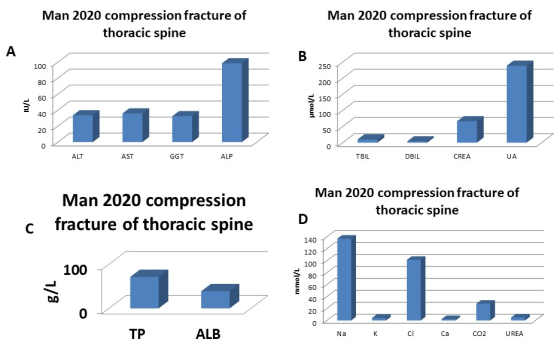
Figure 9. Blood parameter of man 2020 Compression fracture of thoracic spine (A-D).

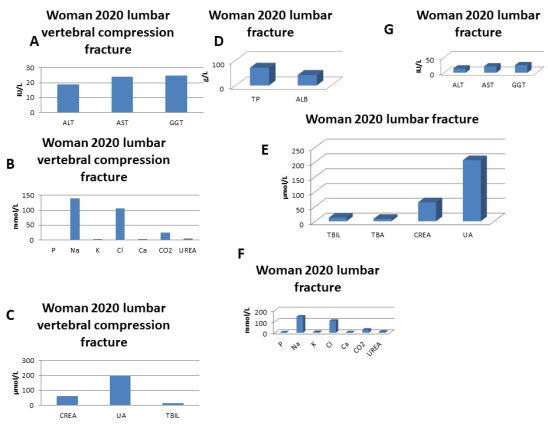
Figure 10. Blood parameter of woman 2020 lumbar vertebral compression fracture and Lumbar fracture (A-G).

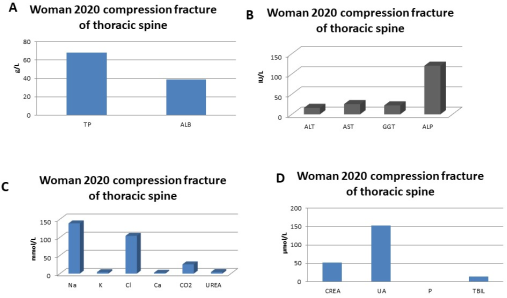
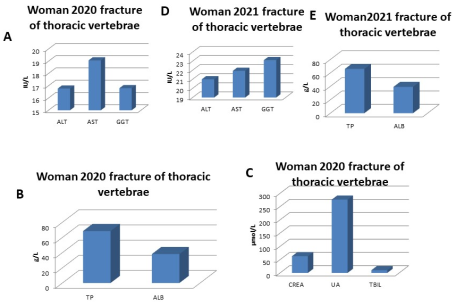
Figure 11. Blood parameter of woman 2020 Compression fracture of thoracic spine (A-D).

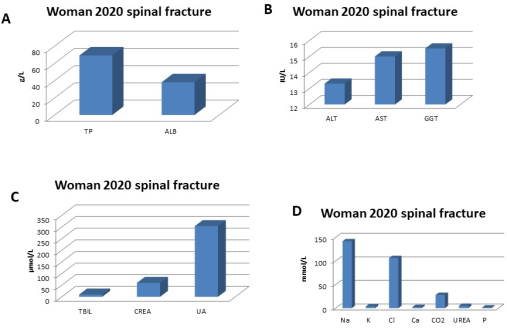
Figure 12. Blood parameter of women 2020 spinal fracture (A-D).

Figure 13. Blood parameter of woman 2020 fracture of thoracic vertebrae (A-C).

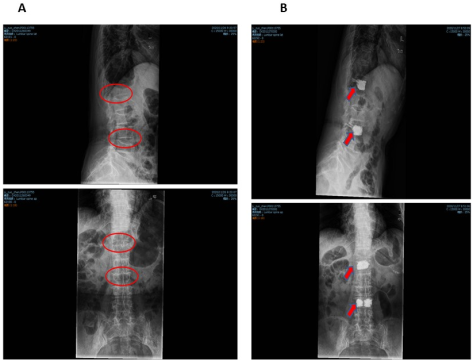
Figure 14. A. 2020 Lumbar vertebral compression, Fracture before surgery, (Female, age 88). B. 2020 Lumbar vertebral compression, Fracture after surgery, (Female, age 88).

Figure 15. A. 2020 Lumbar fracture before surgery, Female, age 81. B. 2020 Lumbar fracture after surgery, Female, age 81.

Figure 16. A. 2020 fracture of thoracic vertebrae before surgery, Female, age 80. B. 2020 fracture of thoracic vertebrae after surgery, Female, age 80.

Figure 17. A. 2020 fracture of thoracic vertebrae before surgery, Male, age 57. B. 2020 fracture of thoracic vertebrae after surgery, Male, age 57.

Figure 18. A. 2020 spinal fracture after surgery, Male, age 75. B. 2020 spinal fracture before surgery, Male, age 75.
Information