Iron deficiency is one of the most widespread nutritional disorders in the world. It affects almost 60% of the population in developing countries, i.e. 3.5 billion people. Women of childbearing age and young children are the most vulnerable. Iron deficiency occurs when the intake and absorption of iron cannot compensate physiological needs, which are particularly high in young children because of their growth. Due to its impact on children's health, iron deficiency remains a major public health problem in Togo, with 70% of children aged between 6 and 59 months suffering from anaemia. In the face of this problem, the present study aims to establish the adequacy between dietary iron intake and physiological needs in order to contribute to strategies for handling this nutritional deficiency. To achieve this, 479 children (243 urban and 236 rural) aged 6-59 months from 447 households were the subject of this study. Food consumption was assessed using the 24-hour recall method; the nutritional value of the rations was assessed using the food composition table available in Africa. The results showed that 62% of the children studied had dietary iron intakes below the recommended levels and only 38% were able to cover their iron requirements. In fact, the mother's level of school education and the mother's economic activity were found to be strongly correlated with iron status in children. In the light of these data, it would seem wise to consider better nutritional intervention strategies, including nutritional education for women of childbearing age. The introduction of nutritional counselling through Information, Education and Communication (IEC), mobilisation and social marketing campaigns should therefore be promoted.
| Published in | American Journal of BioScience (Volume 12, Issue 2) |
| DOI | 10.11648/j.ajbio.20241202.14 |
| Page(s) | 61-74 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Young Children, Iron Deficiency, Socio-Demographic Status, Iron Deficiency Anaemia, Kara, Togo
2.1. Study Setting and Sample Considered
2.2. Household Recruitment Method
2.3. Ethical Considerations Child Eligibility Criteria
2.4. Survey Methods
2.5. Food Consumption by Weighing and its Frequency
2.6. Questionnaire on the Socio-Economic Situation of Households
2.7. Calculation Micronutrient Intakes and Coverage
2.8. Questionnaires and Information Collection Forms
2.9. Food Measuring Equipment and Timetable for the Investigation
ACTIVITY | DATE | OBSERVATION |
|---|---|---|
Interviewer training and pre-testing of questions | 11 to 13/08/2023 | Training at the USP of Awandjelo and Lama Kpeda. 1) Pre-test in the field in around thirty households. 2) Taking into account the inadequacies and reformulating some questions in the questionnaire. |
Investigation in Awandjelo | 14/08 to 16/08/2023 | Rural survey |
Investigation in Lama | 02/09 to 04/09/2023 | Urban survey |
2.10. Statistical Processing of Data
3.1. Results
3.1.1. Socio-Demographic Status of Children
(i). Age
(ii). Sex
3.1.2. Sociodemographic Status of Mothers
(i). Age
(ii). Educational Level of Children's Mothers
(iii). Environment Before Married life
(iv). Socio-Professional Category
(v). Religion
(vi). Breastfeeding Practice
3.1.3. Coverage Rate of Iron Requirements in Young Children
Child's living environment | Proportion of children not having full coverage of their iron requirements (n) | Proportion of children with full coverage of their iron requirements (n) | Total (n) |
|---|---|---|---|
Rural | 66.58% (155) | 34.32% (81) | 100%(236) |
Urban | 59.26 %(144) | 40.74 % (99) | 100%(243) |
All environments considered | 62.42 % (299) | 37.58 % (180) | 100%(479) |
P-value (Rural vs Urban ) | 0.349 ( p > 0.05) | ||
3.1.4. Variation in Coverage of Children's Iron Requirements According to Their Characteristics
Age of child (months) | Proportion of children not having total coverage of their iron requirements (n) | Proportion of children with total coverage of their iron requirements (n) | Total (n) |
|---|---|---|---|
6-11 | 97.73% (43) | 2.27% (1) | 100% (126) |
12-23 | 77.78% (98) | 22.22% (28) | 100% (309) |
24-59 | 51.13% (158) | 48.87% (151) | 100% (44) |
All ages considered | 62.42% (299) | 37.58% (180) | 100% (479) |
P-value (Rural vs Urban ) | 3,364.10 -12 (p < 0.05) | ||
Gender of child | Proportion of children not having total coverage of their iron requirements (n) | Proportion of children with total coverage of their iron requirements (n) | Total (n) |
|---|---|---|---|
Female | 60.57% (149) | 39.34% (97) | 100% (236) |
Male | 64.38% (150) | 35.62% (83) | 100% (243) |
All sexes considered | 62.42% (299) | 37.58% (180) | 100% (479) |
P-value (Rural vs Urban) | P-value = 0.39 (p > 0.05) | ||
3.1.5. Variation in Coverage of Children's Iron Requirements According to the Socio-Demographic Characteristics of the Mother
(i). Influence of Age
Age of mother (years) | Proportion of children not having total coverage of their iron requirements (n) | Proportion of children with total coverage of their iron requirements (n) | Total (n) |
|---|---|---|---|
18-35 | 63.81% (238) | 36.19% (135) | 100% (373) |
More than 35 | 57.55% (61) | 42.45% (45) | 100% (106) |
All ages considered | 62.42% (299) | 37.58% (180) | 100% (479) |
P-value (Rural vs Urban) | 0.269 (p > 0.05) | ||
(ii). Influence of the Mother's Educational level
Level of School education | Proportion of children not having total coverage of their iron requirements (n) | Proportion of children with total coverage of their iron requirements (n) | Total (n) |
|---|---|---|---|
None | 61.54% (8) | 38.46% (5) | 100% (13) |
Primary | 74.12% (63) | 25.88% (22) | 100% (85) |
Secondary and above | 59.84% (228) | 40.16% (153) | 100% (381) |
All levels combined | 62.42% (299) | 37.58% (180) | 100% (479) |
P-value (Rural vs Urban ) | 0.049 (p < 0.05) | ||
(iii). Influence of the Mother's Living Environment Before Her Married life
Living environment | Proportion of children not having total coverage of their iron requirements (n) | Proportion of children with total coverage of their iron requirements (n) | Total (n) |
|---|---|---|---|
Rural | 63.67% (149) | 36.33% (85) | 100% (234) |
Urban | 61.22% (150) | 38.78% (95) | 100% (245) |
All environments considered | 62.42% (299) | 37.58% (180) | 100% (479) |
P-value (Rural vs Urban ) | 0.58 (p > 0.05) | ||
(iv). Influence of Socio-Professional Category
Mothers' activities | Proportion of children not having total coverage of their iron requirements (n) | Proportion of children with total coverage of their iron requirements (n) | Total (n) |
|---|---|---|---|
Farmer/trader/artisan | 62.31% (248) | 37.69% (150) | 100% (398) |
Official | 57.97% (40) | 42.03% (29) | 100% (69) |
Unemployed | 91.67% (11) | 8.33% (1) | 100% (12) |
Any professional situation considered | 62.42% (299) | 37.58% (180) | 100% (479) |
P-value (Rural vs Urban ) | 0.084 (P < 0.05) | ||
(v). Influence of Religion
Mother's religion | Proportion of children not having total coverage of their iron requirements (n) | Proportion of children with total coverage of their iron requirements (n) | Total (n) |
|---|---|---|---|
Animist | 66.99% (69) | 33.01% (34) | 100% (103) |
Christianity | 60.90% (176) | 39.10% (113) | 100% (289) |
Muslim | 62.07% (54) | 37.93% (33) | 100% (87) |
Any religion considered | 62.48% (299) | 37.58% (180) | 100% (479) |
P-value (Rural vs Urban) | 0.547 (p > 0.05) | ||
3.1.6. Iron- Rich Foods
3.2. Discussions
3.2.1. Coverage Rate of Iron Requirements in Young Children
3.2.2. Influence of the Socio-Demographic Status of the Mother on Iron Deficiency in Children
| [1] | Xie H., Perez N., Anderson W., Ringler C., You L. (2020): Can Sub-Saharan Africa feed itself? The role of irrigation development in the region’s drylands for food security: In Virtual Water. Routledge; 80-98. |
| [2] |
ONU (2004): Fifth report on the world nutrition situation. Nutrition for improved development outcomes; UN SCN, Geneva, 22-27.
https://www.unscn.org/layout/modules/resources/files/rwns5.pdf (Consulté le 20 décembre 2023) |
| [3] |
DeMaeyer E. M., Dallman P., Gurney J. M., Hallberg L., Sood S. K., Srikantia S. G. (1991): Prévenir et combattre l’anémie ferriprive dans le cadre des soins de santé primaire. Guide à l’usage des administrateurs de la santé et des responsables de programme. Disponible en ligne sur:
https://iris.who.int/handle/10665/40024 (Consulté le 29 décembre 2023) |
| [4] | Lozoff B., De Andraca I., Castillo M., Smith J. B., Walter T., Pino P. (2003): Behavioral and developmental effects of preventing iron-deficiency anemia in healthy full-term infants. Pediatrics; 112(4): 846-854. |
| [5] | Konofal E., Lecendreux M., Arnulf I., Mouren M.-C. (2004): Iron deficiency in children with attention-deficit/hyperactivity disorder. Archives of Pediatrics & Adolescent Medicine; 158(12): 1113-1115. |
| [6] | Sharma C., Dhandoria R. (2019): Assessment of prevalence of iron deficiency anemia among Known population. Journal of Advanced Medical and Dental Sciences Research; 7(7): 175-177. |
| [7] |
EDST (2014): Enquête Démographique de Santé au Togo III (2013-2014). Disponible en ligne sur:
http://160.242.193.218:8082/nada/index.php/catalog/6 (Consulté le 02 décembre 2023) |
| [8] | Hercberg S. (1988): La carence en fer en nutrition humaine: Diététique-Nutrition, Editions Médicales Internationales; 250p. |
| [9] |
Lestienne I., Icard-Vernière C., Picq C., Trèche S. (2003): Effets du trempage des graines et de farines de céréales et de légumineuses sur leur teneur en phytates et leurs rapports molaires Phy/Fe et Phy/Zn. 2ème Atelier international sur les voies alimentaires d’amélioration des situations nutritionelles; 479‑487. Disponible en ligne sur:
https://www.documentation.ird.fr/hor/fdi:010036330 (Consulté le 12 décembre 2023) |
| [10] |
FAO (2002): La situation mondiale de l'alimentation et de l'agriculture (SOFA). ISBN 925204762x; 254p. Disponible en ligne sur:
https://www.fao.org/documents/card/fr/c/18953eb8-ade2-5e6a-92d7-e80be49a3b64 (Consulté le 02 décembre 2023) |
| [11] | Fokui J. V. (2007): La malnutrition à l’Unité de Soins nutritionnels Pédiatrique de l’Hôpital Régional de Gao. Thèse de doctorat en Médecine; Université de Bamako (Mali), 92p. |
| [12] | Dupin H. (1992): Alimentation et nutrition humaines, Aliments et Nutriments; ESF éditeur; 87-166. |
| [13] | Amoussa Hounkpatin W. (2011): Evaluation du potentiel de couverture des besoins en vitamine a des jeunes enfants à partir des sauces accompagnant les aliments de base consommés au Bénin; Thèse de Doctorat en Nutrition, Santé; Université de Montpellier 2 (France), 266p. |
| [14] |
OMS (1998): Alimentation complémentaire des jeunes enfants dans les pays en développement: un examen de connaissances scientifiques actuelles. Organisation mondiale de la santé: Genève. Disponible en ligne sur:
https://apps.who.int/gb/ebwha/pdf_files/WHA51/eaid3.pdf (Consulté le 17fao/ novembre 2023) |
| [15] |
FAO/WHO (2004): Rapport de la Consultation OMS/FAO d’experts sur le régime alimentaire, la nutrition et la prévention des maladies chroniques. 54p. Disponible en ligne sur:
https://www.fao.org/3/a1296f/a1296f.pdf (Consulté le 02 décembre 2023) |
| [16] | Mengue Y. W. (1991): Institut de formation et de recherche démographiques. Master Professionnel en Démographie; Institut de Formation et de Recherche Démographiques; Universite de Yaounde II (Cameroun). |
| [17] | Berger J., Dillon J.-C. (2002): Stratégies de contrôle de la carence en fer dans les pays en développement. Sante; 12(1): 22‑30. |
| [18] | Maman M. S. (2012): Étude des pratiques d’alimentation des enfants âgés entre 0-6 mois issus de milieux défavorisés dans la commune urbaine de Tessaoua région de Maradi au Niger. Thèse de Doctorat en Science des Aliments et Nutrition; Université Laval Québec (Canada), 178p. |
| [19] | Alaimo K., Olson C. M., Frongillo Jr E. A., Briefel R. R. (2001): Food insufficiency, family income, and health in US preschool and school-aged children. American Journal of Public Health; 91(5): 781. |
| [20] |
Dackam N. R. (1990): L’éducation de la mère et la mortalité des enfants en Afrique. Les Cahiers de l’IFORD, 2. Disponible en ligne sur:
http://www.iford-cm.org/images/CAHIER_IFORD/02-Cahier_IFORD_N_2.pdf (Consulté le 04 décembre 2023) |
| [21] | Payant-Hébert R. (2013): La contribution des jardins collectifs urbains à la lutte contre l’insécurité alimentaire. Thèse de Doctorat études urbaines; Université de Québec (Canada), 175p. |
| [22] | Séguin L., Xu L., Potvin L., Zunzunegui M., Frohlich K. L. (2003): Effets du faible revenu sur la santé des nourrissons. Canadian Medical Association Journal; 168(12): 1533-1538. |
| [23] | Sabban F., Grignon C., Aymard M. (1994): Le temps de manger: Alimentation, emploi du temps et rythmes sociaux, Enfants et soupes. Edition Quaé, 161-336. |
| [24] | Dufumier M. (2004): Agricultures et paysanneries des Tiers mondes. Tiers mondes. Karthala Editions; 705-706. |
| [25] |
OMS/UNICEF (2001): Iron deficiency anemia, assessment, prevention and control: a guide for programme managers. Geneva, WHO, 2001. Disponible en ligne sur:
https://www.who.int/fr/publications/m/item/iron-children-6to23--archived-iron-deficiency-anaemia-assessment-prevention-and-control (Consulté le 14 novembre 2023) |
| [26] | Kobelembi F. (2004): La malnutrition chronique chez les enfants de moins de cinq ans: L’enfant en Centrafrique. Famille, santé, scolarité, travail. Edition Karthala; 113-157. |
| [27] | Guérin C. (2015): Le bien-fondé du petit-déjeuner dans le rythme alimentaire occidental. Thèse de doctorat en Médecine. Université de Paris Descartes (France), 132p. |
| [28] | Akoto E. (1993): Déterminants socio-culturels de la mortalité des enfants en Afrique noire: Hypothèses et recherche d’explication; Monographie. Éditions Academia; Volume 4 de monographie de l'Université de Louvain (1970); Institut de démographie, Série Démographique. ISBN: 287209265X, 9782872092656, 269p. |
APA Style
Tossavi, D., Mamatchi, M., Novignon, D., Mawabena, K., Koffi, D., et al. (2024). Evaluation of the Coverage of Iron Requirements in Young Children Aged 6 to 59 Months from Basic Foods in Two Localities in North Togo: Awandjelo and Lama (Kara). American Journal of BioScience, 12(2), 61-74. https://doi.org/10.11648/j.ajbio.20241202.14
ACS Style
Tossavi, D.; Mamatchi, M.; Novignon, D.; Mawabena, K.; Koffi, D., et al. Evaluation of the Coverage of Iron Requirements in Young Children Aged 6 to 59 Months from Basic Foods in Two Localities in North Togo: Awandjelo and Lama (Kara). Am. J. BioScience 2024, 12(2), 61-74. doi: 10.11648/j.ajbio.20241202.14
AMA Style
Tossavi D, Mamatchi M, Novignon D, Mawabena K, Koffi D, et al. Evaluation of the Coverage of Iron Requirements in Young Children Aged 6 to 59 Months from Basic Foods in Two Localities in North Togo: Awandjelo and Lama (Kara). Am J BioScience. 2024;12(2):61-74. doi: 10.11648/j.ajbio.20241202.14
@article{10.11648/j.ajbio.20241202.14,
author = {Dandonougbo Tossavi and Melila Mamatchi and Dandonougbo Novignon and Kadanga Mawabena and Dandonougbo Koffi and Mensah Labité Komlan and Amouzou Kou’santa},
title = {Evaluation of the Coverage of Iron Requirements in Young Children Aged 6 to 59 Months from Basic Foods in Two Localities in North Togo: Awandjelo and Lama (Kara)
},
journal = {American Journal of BioScience},
volume = {12},
number = {2},
pages = {61-74},
doi = {10.11648/j.ajbio.20241202.14},
url = {https://doi.org/10.11648/j.ajbio.20241202.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajbio.20241202.14},
abstract = {Iron deficiency is one of the most widespread nutritional disorders in the world. It affects almost 60% of the population in developing countries, i.e. 3.5 billion people. Women of childbearing age and young children are the most vulnerable. Iron deficiency occurs when the intake and absorption of iron cannot compensate physiological needs, which are particularly high in young children because of their growth. Due to its impact on children's health, iron deficiency remains a major public health problem in Togo, with 70% of children aged between 6 and 59 months suffering from anaemia. In the face of this problem, the present study aims to establish the adequacy between dietary iron intake and physiological needs in order to contribute to strategies for handling this nutritional deficiency. To achieve this, 479 children (243 urban and 236 rural) aged 6-59 months from 447 households were the subject of this study. Food consumption was assessed using the 24-hour recall method; the nutritional value of the rations was assessed using the food composition table available in Africa. The results showed that 62% of the children studied had dietary iron intakes below the recommended levels and only 38% were able to cover their iron requirements. In fact, the mother's level of school education and the mother's economic activity were found to be strongly correlated with iron status in children. In the light of these data, it would seem wise to consider better nutritional intervention strategies, including nutritional education for women of childbearing age. The introduction of nutritional counselling through Information, Education and Communication (IEC), mobilisation and social marketing campaigns should therefore be promoted.
},
year = {2024}
}
TY - JOUR T1 - Evaluation of the Coverage of Iron Requirements in Young Children Aged 6 to 59 Months from Basic Foods in Two Localities in North Togo: Awandjelo and Lama (Kara) AU - Dandonougbo Tossavi AU - Melila Mamatchi AU - Dandonougbo Novignon AU - Kadanga Mawabena AU - Dandonougbo Koffi AU - Mensah Labité Komlan AU - Amouzou Kou’santa Y1 - 2024/04/29 PY - 2024 N1 - https://doi.org/10.11648/j.ajbio.20241202.14 DO - 10.11648/j.ajbio.20241202.14 T2 - American Journal of BioScience JF - American Journal of BioScience JO - American Journal of BioScience SP - 61 EP - 74 PB - Science Publishing Group SN - 2330-0167 UR - https://doi.org/10.11648/j.ajbio.20241202.14 AB - Iron deficiency is one of the most widespread nutritional disorders in the world. It affects almost 60% of the population in developing countries, i.e. 3.5 billion people. Women of childbearing age and young children are the most vulnerable. Iron deficiency occurs when the intake and absorption of iron cannot compensate physiological needs, which are particularly high in young children because of their growth. Due to its impact on children's health, iron deficiency remains a major public health problem in Togo, with 70% of children aged between 6 and 59 months suffering from anaemia. In the face of this problem, the present study aims to establish the adequacy between dietary iron intake and physiological needs in order to contribute to strategies for handling this nutritional deficiency. To achieve this, 479 children (243 urban and 236 rural) aged 6-59 months from 447 households were the subject of this study. Food consumption was assessed using the 24-hour recall method; the nutritional value of the rations was assessed using the food composition table available in Africa. The results showed that 62% of the children studied had dietary iron intakes below the recommended levels and only 38% were able to cover their iron requirements. In fact, the mother's level of school education and the mother's economic activity were found to be strongly correlated with iron status in children. In the light of these data, it would seem wise to consider better nutritional intervention strategies, including nutritional education for women of childbearing age. The introduction of nutritional counselling through Information, Education and Communication (IEC), mobilisation and social marketing campaigns should therefore be promoted. VL - 12 IS - 2 ER -
Department of Life and Earth Sciences, Faculty of Sciences and Technology, University of Kara, Kara, Togo
Department of Biochemistry, Faculty of Sciences, University of Lomé, Lomé, Togo
Department of Life and Earth Sciences, Faculty of Sciences and Technology, University of Kara, Kara, Togo
Department of Biochemistry, Faculty of Sciences, University of Lomé, Lomé, Togo
Department of Biochemistry, Faculty of Sciences, University of Lomé, Lomé, Togo
Department of Life and Earth Sciences, Faculty of Sciences and Technology, University of Kara, Kara, Togo
Department of Life and Earth Sciences, Faculty of Sciences and Technology, University of Kara, Kara, Togo; Department of Biochemistry, Faculty of Sciences, University of Lomé, Lomé, Togo
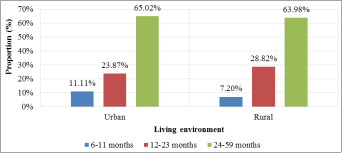
Figure 1. Distribution of children by age group and living area.
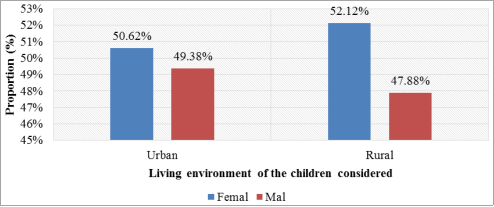
Figure 2. Distribution of children by sex and living environment.
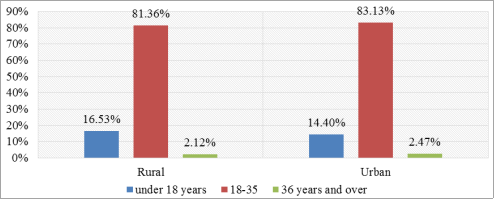
Figure 3. Distribution of mothers according to age groups and living environment.
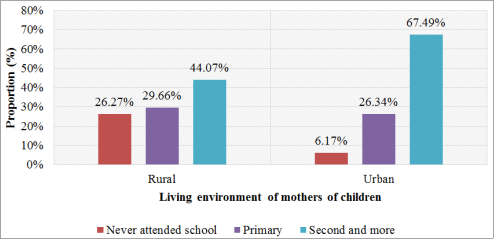
Figure 4. Distribution of mothers according to level of education and living environment.
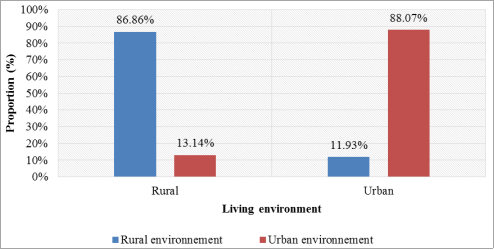
Figure 5. Distribution of mothers according to living environment before married life.

Figure 6. Distribution of mothers according to socio-professional category and living environment.

Figure 7. Distribution of mothers according to religion practiced and living environment.
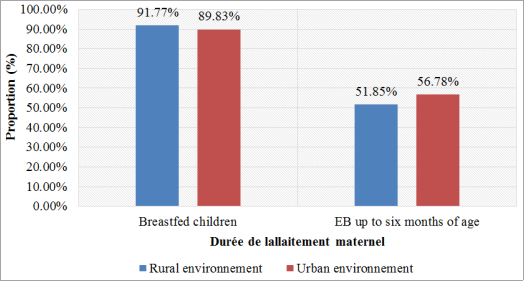
Figure 8. Distribution according Breastfeeding practice.
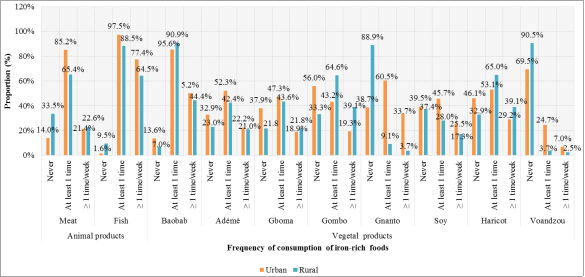
Figure 9. Distribution of children according to frequency of consumption of iron-rich foods per week.
Information

