Introduction: Sarcoidosis is a systemic granulomatosis of unknown aetiology characterised by the formation of non-caseating granulomas in organs. Hepatic involvement can be difficult to diagnose. Material and method: We report the case of a 30-year-old female patient with a long history of intractable pruritus revealing systemic sarcoidosis. Case report: A 30-year-old female patient presented with a persistent pruritus without jaundice or fever. Examination revealed tender hepatomegaly and scratch lesions. Laboratory tests revealed elevated liver enzymes with cholestasis, and serum protein electrophoresis showed an inflammatory profile. The different viral hepatitis tests were non-contributory. Alpha fetoprotein was normal. Abdominal ultrasound and CT scans revealed a heteronodular hepatomegaly. The first liver biopsy was consistent with autoimmune hepatitis lesions. The disease improved with general corticosteroid therapy and azathioprine. Two years later, with the persistence of the pruritus, blood calcium levels and angiotensin-converting enzyme tests were found to be elevated. A new liver biopsy showed epitheliogigantocellular granulomas without caseous necrosis. A thoracic CT scan revealed mediastinal adenopathy. This suggested systemic sarcoidosis. The patient progressed well clinically and radiologically on general corticosteroids with adjuvant therapy and azathioprine. Conclusion: Sarcoidosis is a systemic disease that can affect most tissues and organs. Hepatic involvement is frequent and more often difficult to diagnose.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Sarcoidosis is a systemic granulomatosis of unknown aetiology characterised by granuloma formation in affected organs and may result from gene-environment interactions in predisposed individuals. The disease is more common in women, with a sex ratio of 1.2 - 1.5:1
[1]
Valeyre D et al. Sarcoïdose. Lancet. 2014; 383(9923): 1155-1167.
[1]
.
Studies have found liver involvement in 33% and 56% of cases of sarcoidosis
[2]
Ketari J. Maamouri N. Ben Dhaou D. et al. Hepatic involvement in sarcoidosis: study of seven cases. Rev med int. 2010; 31(1): 12-16.
[3]
Elloumi H. Marzouk S. Tahri N. Bahloul Z. Sarcoidosis and liver disease: a series of 25 patients. Rev med int. 2012; 33(11): 607-614.
[2, 3]
. We report the case of a 30-year-old female patient seen for a persistent and insomnious pruritus of insidious onset whose diagnosis of systemic sarcoidosis was confirmed after 2 years.
2. Case Report
The case was a 30-year-old female patient with a history of pleurisy that was attributed to tuberculosis in 2012, treated and declared cured. She was referred in 2019 for the management of persistent, insomnious pruritus that had been present for three weeks without fever.
On examination, she presented with scratch lesions without jaundice, tender hepatomegaly without signs of portal hypertension nor joint nor cardiac manifestations, and no peripheral tumour syndrome.
Blood count was normal (HGB=13.7g/dl, VGM=86.4fl, GB=4340 elements/µl, PLT=394000 elements/µl), C-reactive protein was normal (5.3mg/l), prothrombin level (100%) and bilirubin level (5.7mg/l) were normal. Serum protein electrophoresis revealed polyclonal hypergammaglobulinaemia.
There was hepatic cytolysis with ALT increased to twice normal and AST to thrice normal, and cholestasis with GGT increased to 1.13 times normal and ALP to 1.7 times normal.
Viral markers: HBsAg, anti-HCV, HIV were negative. Anti-HBc and anti-HBS antibodies were positive. The anti-HBS antibody titre was greater than 1000 IU/L.
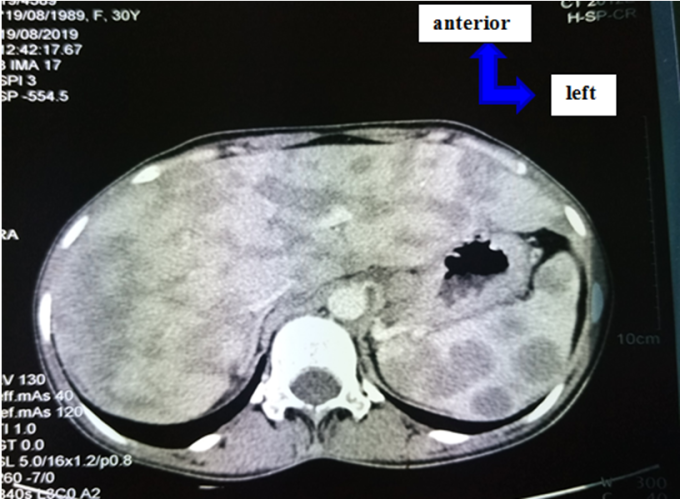
Abdominal ultrasound revealed hepatomegaly with diffuse micronodules without signs of portal hypertension. Computed tomography revealed heterogeneous multinodular hepatomegaly with multiple focal splenic and hepatic lesions of varying degrees of confluence and hypovascularisation (Figure 1).
Figure 1. Heterogeneous multinodular hepatomegaly with multiple focal hypovascularised +/- confluent splenic and hepatic lesions.
Upon completion of these biological and radiological tests, the alphafoetoproteins came back normal. Anti-nuclear antibodies were positive (1/320) with homogeneous fluorescence. Anti-LKM1, anti-mitochondrial and anti-smooth muscle antibodies were negative. Fibroscan revealed a median elasticity of 13.4 KPA, F4 fibrosis.
Liver biopsy showed cirrhosis in an autoimmune hepatitis lesion. There was no histological evidence of sclerosing cholangitis or biliary cirrhosis, and no evidence of tuberculosis, lymphoma, haemochromatosis, NASH or chronic viral hepatitis.
On the basis of the latest data, seronegative autoimmune hepatitis was considered. The patient was started on prednisone 1mg/kg/day with adjuvant therapy and azathioprine 3mg/kg/day.
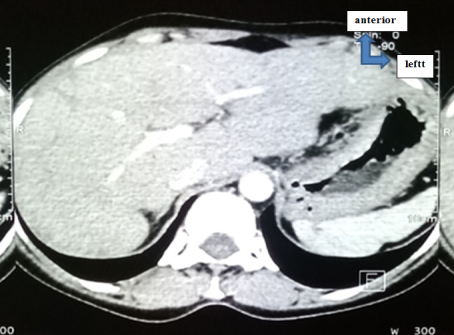
We noted a good clinical, biological and radiological evolution with almost complete disappearance of the lesions on the CT scan performed at the fourth month (M4) after the start of treatment (Figure 2).
The fibroscan returned a median elasticity of 5.4KPA at M4 (fourth month).
We also noted a good improvement in biological markers, as shown in Table 1.
Figure 2. CT scan of nodular lesions in the liver after treatment (M4).
Table 1. Trends in biological markers of liver involvement.
Analyses
18/12/2019
28/01/2020
18/06/2020
09/02/2021
28/12/2022
07/11/2023
30/01/2024
Direct Bilirubine (DB)
2,87mg/l
2,43mg/l
2,7mg/l
Total Bilirubin (TB)
6,10mg/l
7,59mg/l
5,5mg/l
GGT
616UI/l
88,03UI/l
514,8UI/l
54,42UI/l
644UI/l
406UI/l
180UI/l
ALP
2833,25UI/l
752,8 (3,1N)
1057,27UI/l
639,80UI/l
476UI/l
360UI/l
429UI/l
AST
56,2 (10-40)
72,07UI/l
73,87UI/l
38,41UI/l
86UI/l
39UI/l
25UI/l
ALT
63 (10-45)
152,06UI/l
38,12UI/l
44,46UI/l
66UI/l
21UI/l
20UI/l
Normal: DB <2mg; BT<12mg; PAL 30 – 130U/L; GGT<35 IU/L
A year later, in September 2022, we noted a recrudescence of pruritus with asthenia. The physical examination was normal.
Bilirubin levels and prothrombin levels were normal. There was hepatic cytolysis with AST at 86 IU/L and ALT at 66 IU/L. Serum calcium was increased to 104mg/l. Angiotensin converting enzyme was elevated to 73ECA (N: 20-70). Serum protein electrophoresis revealed polyclonal hypergammaglobulinaemia. Intradermal tuberculin reaction revealed anergy. Changes in biological markers are shown in Table 1.
Given the fluctuating anicteric hepatic cholestasis and occasional episodes of transient pruritus and disappearance of fibrosis on fibroscan, a liver biopsy was repeated at M22 and revealed: granulomatous chronic hepatitis with multinucleolated giant epithelioid cells without central necrosis and no inflammatory damage to the bile ducts, steatosis or haemosiderosis.
We then looked for other organ manifestations. Chest CT revealed poorly systematised reticulonodular opacities, linear fibrosis and apical and posterosuperior left pre-scissural tubular bronchiectasis with nonspecific middle mediastinal lymph nodes.
Spirometry, electrocardiogram and echocardiography were normal.
In summary, we concluded that the patient had systemic sarcoidosis (hepatosplenic, pulmonary and lymph node).
Prednisone 1mg/kg/day with adjuvant therapy was reintroduced for one month. A good clinical evolution was noted with stabilisation of the cholestasis.
3. Discussion
The prevalence of sarcoidosis is estimated at 30.2 cases per 10,000 people, with an incidence of 4.85/10000/year, varying according to sex, age, ethnic origin and geographical location
[4]
Geri G. Saadoun D. Cacoub P. Hepatic manifestations of systemic diseases. Rev med int. 2011; 32: 486–493.
[4]
.
Pulmonary involvement is more common in sarcoidosis, accounting for 90% of cases. It is most often the mode of revelation. Extrapulmonary involvement is common and may involve most organs and viscera. The clinical presentation, disease course and severity of sarcoidosis are highly variable, which has an impact on treatment and prognosis
[5]
Oumnia N. Lahcene M. Tebaibia A. et al. Hepatic sarcoidosis: 20 observations. Multicentre study in Algeria. In JFHOD. 2023. P135.
[5]
.
Sarcoidosis has many clinical manifestations. Asymptomatic in 30-60% of cases, the disease is often discovered incidentally during a chest X-ray. Persistent respiratory symptoms such as dyspnoea, dry cough or chest pain may be present.
In one third of patients, the onset symptoms are accompanied by systemic manifestations. Diagnosis is difficult, which explains why almost 50% of cases are diagnosed post mortem after histopathological study
[4]
Geri G. Saadoun D. Cacoub P. Hepatic manifestations of systemic diseases. Rev med int. 2011; 32: 486–493.
[4]
.
Although often asymptomatic, liver involvement may be revealed by abdominal pain and pruritus. Fever accompanied by arthralgia is present in 60% of patients with liver disease. One of the most revealing signs is hepatomegaly. This was observed in our patient and found in the studies of Kétari medicine in 2010 and Elloumi in 2012
[2]
Ketari J. Maamouri N. Ben Dhaou D. et al. Hepatic involvement in sarcoidosis: study of seven cases. Rev med int. 2010; 31(1): 12-16.
[3]
Elloumi H. Marzouk S. Tahri N. Bahloul Z. Sarcoidosis and liver disease: a series of 25 patients. Rev med int. 2012; 33(11): 607-614.
[2, 3]
.
Pruritus is a relatively rare manifestation of sarcoidosis and most often indicates liver, pancreatic or renal involvement. A clinical observation was published in the journal of internal medicine in 2014 in which the authors found severe hepatic involvement with pruritus in one patient
[6]
Garnier C. Pugnet G. Moulis G. et al. A rare cause of pruritus in severe sarcoidosis. Rev Med Int. 2014; 35(S1): 149.
[6]
.
Hepatic involvement is characterised by cholestasis (80%) and cytolysis (60%), which were found in Elloumi's study of a series of 25 patients followed for hepatic sarcoidosis
[3]
Elloumi H. Marzouk S. Tahri N. Bahloul Z. Sarcoidosis and liver disease: a series of 25 patients. Rev med int. 2012; 33(11): 607-614.
[3]
. These biological abnormalities (cholestasis and hepatic cytolysis) may be absent in some patients, resulting in an incidental finding. Lymphopenia and biological inflammatory syndrome may be present. These biological disturbances are not specific
[7]
Kheder M. Saïd F. Hamzaoui A. et al. Hepatosplenic involvement in sarcoidosis: a case report of 31 patients. Rev med int. 2018; 39(01): A195.
[7]
.
Hepatic sarcoidosis is asymptomatic in 2/3 of cases, with liver disturbances essentially consisting of anicteric cholestasis, and the characteristic histological lesion is a non-necrotising epithelio-gigantocellular granuloma in the portal spaces. Complications include chronic cholestasis and Portal Hypertension, which occur in 5% of cases. Most of these manifestations were found in our patient
[6]
Garnier C. Pugnet G. Moulis G. et al. A rare cause of pruritus in severe sarcoidosis. Rev Med Int. 2014; 35(S1): 149.
[6]
. The frequency of granulomas varies in the literature from 24 to 78%, which explains why their absence cannot rule out the disease
[2]
Ketari J. Maamouri N. Ben Dhaou D. et al. Hepatic involvement in sarcoidosis: study of seven cases. Rev med int. 2010; 31(1): 12-16.
[2]
.
This anicteric cholestasis was described in a 41-year-old female patient followed for systemic sarcoidosis (hepatosplenic and pulmonary) by Bouchra in 2013
[8]
Bouchra I. Kabbaj N. Rimani M. et al. Cytolysis and anicteric cholestasis revealing pulmonary sarcoidosis (a case report). Hegel. 2013; 1(1): 33-38.
[8]
.
Ultrasound can reveal an echogenic liver with nodules and calcifications. On CT scan, granulomas have a hypodense image. Magnetic resonance imaging may show multiple diffuse nodules that are slightly signal-enhanced. T2-weighted images show a liver with a decreased signal, in contrast to malignant lesions which have an increased T2 signal
[9]
Lyko C. Bart PA. Pruvot E. et al. extrapulmonary sarcoidosis, a little-known entityRev Med suisse. 2010; 6: 2056-2060.
[9]
.
Hepatosplenic nodular involvement has been described by some authors. In a series of 31 patients in 2018, Kheder M found nodular hepatosplenomegaly on CT in 30% of patients. This hepatosplenic involvement was often associated with pulmonary involvement
[7]
Kheder M. Saïd F. Hamzaoui A. et al. Hepatosplenic involvement in sarcoidosis: a case report of 31 patients. Rev med int. 2018; 39(01): A195.
[7]
.
In studies by Elloumi
[3]
Elloumi H. Marzouk S. Tahri N. Bahloul Z. Sarcoidosis and liver disease: a series of 25 patients. Rev med int. 2012; 33(11): 607-614.
[3]
and Ketari
[2]
Ketari J. Maamouri N. Ben Dhaou D. et al. Hepatic involvement in sarcoidosis: study of seven cases. Rev med int. 2010; 31(1): 12-16.
[2]
, nodular hepatomegaly was found on CT scan and was often associated with systemic involvement.
Ultrasound-guided biopsy of the liver can also be performed on the spleen with good results, allowing histopathological investigation of granulomas
[10]
Frappard T. LePendu C. Meignin V. et al. Ultrasound-guided splenic biopsy: an efficient diagnostic tool in sarcoidosis? Rev med int. 2019. 40(9): 609-612.
[10]
.
Diagnosis is based on the demonstration of a non-caseating granuloma on anatomopathology, combined with clinical, biological and radiological evidence, after exclusion of other granulomatosis. Non-caseating granulomas are found in 60-90% of liver biopsies from patients with sarcoidosis, as in our patient's first biopsy
[4]
Geri G. Saadoun D. Cacoub P. Hepatic manifestations of systemic diseases. Rev med int. 2011; 32: 486–493.
[4]
.
First-line treatment is based on systemic corticosteroids such as prednisone 1mg/kg/d (20 to 40mg) for 1 to 3 months as initial dose with adjuvant means. Weaning should be gradual, with a reduction of 5-10mg/d every 2 to 4 weeks to a maintenance dose of 5 to 10mg for 9 months. The total duration is approximately 12 months. This treatment is generally effective, particularly with regard to changes in imaging. Second-line treatment is based on azathioprine and methotrexate in cases of corticosteroid resistance or contraindication to corticosteroid therapy. In the absence of efficacy of these latter molecules, anti TNF alpha drugs such as infliximab may be used
[11]
Rochat TS. Janssens JP. Soccal PM. Et al. Update on the treatment of sarcoidosis. Rev Med Suisse. 2016; 539(2): 1966–1971.
[12]
Sah BP. Goyal S. Iannuzzi MC. Novel pharmacotherapy of sarcoidosis. Pharmacol Ther. 2016; 157: 1–9.
[13]
Ndili Obi O. Saketkoo LA. Russel AM. Baughman RP. Sarcoidosis: updates on therapeutic drug trials and new treatment approaches. Front Med (Lausanne). 2022; 9: 1-27.
[11-13]
.
4. Conclusion
Sarcoidosis is a systemic granulomatous disease that is difficult to diagnose, and is based on a number of factors. Extrapulmonary involvement is frequent and is marked by multifaceted and sometimes paucisymptomatic liver involvement. Treatment is based on systemic corticosteroids and rarely immunotherapy.
Abbreviations
GGT
Gamma-Glutamyltransferase
ALT
Alanine Transaminase
AST
Aspartate Transaminase
HGB
Hemoglobin
MCV
Mean Corpuscular Volume
HBV
Hepatitis B Virus
HIV
Human Immunodeficiency Virus
CT scan
Computed Tomography
Anti-LKM antibody
Anti–Liver-Kidney Microsomal Antibody
NASH
Nonalcoholic Steatohepatitis
Author Contributions
Diallo Bachir Mansour: Conceptualization, Methodology, Writing – original draft
Faye Fulgence Abdou: Data curation, Formal Analysis
Ndour Jean Noel Ndour: Formal Analysis, Investigation
Mbaye Serigne Abdou Khadr: Formal Analysis
Berthé Adama: Data curation, Supervision, Validation
Touré Papa Souleymane: Data curation, Supervision, Validation, Visualization
Diop Madoky Magatte: Supervision
Ka Mamadou Mourtalla: Data curation, Supervision, Validation
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
Valeyre D et al. Sarcoïdose. Lancet. 2014; 383(9923): 1155-1167.
[2]
Ketari J. Maamouri N. Ben Dhaou D. et al. Hepatic involvement in sarcoidosis: study of seven cases. Rev med int. 2010; 31(1): 12-16.
[3]
Elloumi H. Marzouk S. Tahri N. Bahloul Z. Sarcoidosis and liver disease: a series of 25 patients. Rev med int. 2012; 33(11): 607-614.
[4]
Geri G. Saadoun D. Cacoub P. Hepatic manifestations of systemic diseases. Rev med int. 2011; 32: 486–493.
[5]
Oumnia N. Lahcene M. Tebaibia A. et al. Hepatic sarcoidosis: 20 observations. Multicentre study in Algeria. In JFHOD. 2023. P135.
[6]
Garnier C. Pugnet G. Moulis G. et al. A rare cause of pruritus in severe sarcoidosis. Rev Med Int. 2014; 35(S1): 149.
[7]
Kheder M. Saïd F. Hamzaoui A. et al. Hepatosplenic involvement in sarcoidosis: a case report of 31 patients. Rev med int. 2018; 39(01): A195.
[8]
Bouchra I. Kabbaj N. Rimani M. et al. Cytolysis and anicteric cholestasis revealing pulmonary sarcoidosis (a case report). Hegel. 2013; 1(1): 33-38.
[9]
Lyko C. Bart PA. Pruvot E. et al. extrapulmonary sarcoidosis, a little-known entityRev Med suisse. 2010; 6: 2056-2060.
[10]
Frappard T. LePendu C. Meignin V. et al. Ultrasound-guided splenic biopsy: an efficient diagnostic tool in sarcoidosis? Rev med int. 2019. 40(9): 609-612.
[11]
Rochat TS. Janssens JP. Soccal PM. Et al. Update on the treatment of sarcoidosis. Rev Med Suisse. 2016; 539(2): 1966–1971.
[12]
Sah BP. Goyal S. Iannuzzi MC. Novel pharmacotherapy of sarcoidosis. Pharmacol Ther. 2016; 157: 1–9.
[13]
Ndili Obi O. Saketkoo LA. Russel AM. Baughman RP. Sarcoidosis: updates on therapeutic drug trials and new treatment approaches. Front Med (Lausanne). 2022; 9: 1-27.
Mansour, D. B., Abdou, F. F., Baba, N. M., Adama, W., Mamadou, D., et al. (2024). Anicteric Cholestasis Syndrome with Pruritus Revealing Systemic Sarcoidosis. American Journal of Internal Medicine, 12(2), 16-20. https://doi.org/10.11648/j.ajim.20241202.11
Mansour, D. B.; Abdou, F. F.; Baba, N. M.; Adama, W.; Mamadou, D., et al. Anicteric Cholestasis Syndrome with Pruritus Revealing Systemic Sarcoidosis. Am. J. Intern. Med.2024, 12(2), 16-20. doi: 10.11648/j.ajim.20241202.11
@article{10.11648/j.ajim.20241202.11,
author = {Diallo Bachir Mansour and Faye Fulgence Abdou and Nana Mamoudou Baba and Wade Adama and Diack Mamadou and Ndour Ndour Jean Noel Ndour and Mbaye Serigne Abdou Khadr and Ndiaye Yanidou and Berthé Adama and Touré Papa Souleymane and Diop Madoky Magatte and Ka Mamadou Mourtalla},
title = {Anicteric Cholestasis Syndrome with Pruritus Revealing Systemic Sarcoidosis
},
journal = {American Journal of Internal Medicine},
volume = {12},
number = {2},
pages = {16-20},
doi = {10.11648/j.ajim.20241202.11},
url = {https://doi.org/10.11648/j.ajim.20241202.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajim.20241202.11},
abstract = {Introduction: Sarcoidosis is a systemic granulomatosis of unknown aetiology characterised by the formation of non-caseating granulomas in organs. Hepatic involvement can be difficult to diagnose. Material and method: We report the case of a 30-year-old female patient with a long history of intractable pruritus revealing systemic sarcoidosis. Case report: A 30-year-old female patient presented with a persistent pruritus without jaundice or fever. Examination revealed tender hepatomegaly and scratch lesions. Laboratory tests revealed elevated liver enzymes with cholestasis, and serum protein electrophoresis showed an inflammatory profile. The different viral hepatitis tests were non-contributory. Alpha fetoprotein was normal. Abdominal ultrasound and CT scans revealed a heteronodular hepatomegaly. The first liver biopsy was consistent with autoimmune hepatitis lesions. The disease improved with general corticosteroid therapy and azathioprine. Two years later, with the persistence of the pruritus, blood calcium levels and angiotensin-converting enzyme tests were found to be elevated. A new liver biopsy showed epitheliogigantocellular granulomas without caseous necrosis. A thoracic CT scan revealed mediastinal adenopathy. This suggested systemic sarcoidosis. The patient progressed well clinically and radiologically on general corticosteroids with adjuvant therapy and azathioprine. Conclusion: Sarcoidosis is a systemic disease that can affect most tissues and organs. Hepatic involvement is frequent and more often difficult to diagnose.
},
year = {2024}
}
TY - JOUR
T1 - Anicteric Cholestasis Syndrome with Pruritus Revealing Systemic Sarcoidosis
AU - Diallo Bachir Mansour
AU - Faye Fulgence Abdou
AU - Nana Mamoudou Baba
AU - Wade Adama
AU - Diack Mamadou
AU - Ndour Ndour Jean Noel Ndour
AU - Mbaye Serigne Abdou Khadr
AU - Ndiaye Yanidou
AU - Berthé Adama
AU - Touré Papa Souleymane
AU - Diop Madoky Magatte
AU - Ka Mamadou Mourtalla
Y1 - 2024/05/24
PY - 2024
N1 - https://doi.org/10.11648/j.ajim.20241202.11
DO - 10.11648/j.ajim.20241202.11
T2 - American Journal of Internal Medicine
JF - American Journal of Internal Medicine
JO - American Journal of Internal Medicine
SP - 16
EP - 20
PB - Science Publishing Group
SN - 2330-4324
UR - https://doi.org/10.11648/j.ajim.20241202.11
AB - Introduction: Sarcoidosis is a systemic granulomatosis of unknown aetiology characterised by the formation of non-caseating granulomas in organs. Hepatic involvement can be difficult to diagnose. Material and method: We report the case of a 30-year-old female patient with a long history of intractable pruritus revealing systemic sarcoidosis. Case report: A 30-year-old female patient presented with a persistent pruritus without jaundice or fever. Examination revealed tender hepatomegaly and scratch lesions. Laboratory tests revealed elevated liver enzymes with cholestasis, and serum protein electrophoresis showed an inflammatory profile. The different viral hepatitis tests were non-contributory. Alpha fetoprotein was normal. Abdominal ultrasound and CT scans revealed a heteronodular hepatomegaly. The first liver biopsy was consistent with autoimmune hepatitis lesions. The disease improved with general corticosteroid therapy and azathioprine. Two years later, with the persistence of the pruritus, blood calcium levels and angiotensin-converting enzyme tests were found to be elevated. A new liver biopsy showed epitheliogigantocellular granulomas without caseous necrosis. A thoracic CT scan revealed mediastinal adenopathy. This suggested systemic sarcoidosis. The patient progressed well clinically and radiologically on general corticosteroids with adjuvant therapy and azathioprine. Conclusion: Sarcoidosis is a systemic disease that can affect most tissues and organs. Hepatic involvement is frequent and more often difficult to diagnose.
VL - 12
IS - 2
ER -
Mansour, D. B., Abdou, F. F., Baba, N. M., Adama, W., Mamadou, D., et al. (2024). Anicteric Cholestasis Syndrome with Pruritus Revealing Systemic Sarcoidosis. American Journal of Internal Medicine, 12(2), 16-20. https://doi.org/10.11648/j.ajim.20241202.11
Mansour, D. B.; Abdou, F. F.; Baba, N. M.; Adama, W.; Mamadou, D., et al. Anicteric Cholestasis Syndrome with Pruritus Revealing Systemic Sarcoidosis. Am. J. Intern. Med.2024, 12(2), 16-20. doi: 10.11648/j.ajim.20241202.11
@article{10.11648/j.ajim.20241202.11,
author = {Diallo Bachir Mansour and Faye Fulgence Abdou and Nana Mamoudou Baba and Wade Adama and Diack Mamadou and Ndour Ndour Jean Noel Ndour and Mbaye Serigne Abdou Khadr and Ndiaye Yanidou and Berthé Adama and Touré Papa Souleymane and Diop Madoky Magatte and Ka Mamadou Mourtalla},
title = {Anicteric Cholestasis Syndrome with Pruritus Revealing Systemic Sarcoidosis
},
journal = {American Journal of Internal Medicine},
volume = {12},
number = {2},
pages = {16-20},
doi = {10.11648/j.ajim.20241202.11},
url = {https://doi.org/10.11648/j.ajim.20241202.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajim.20241202.11},
abstract = {Introduction: Sarcoidosis is a systemic granulomatosis of unknown aetiology characterised by the formation of non-caseating granulomas in organs. Hepatic involvement can be difficult to diagnose. Material and method: We report the case of a 30-year-old female patient with a long history of intractable pruritus revealing systemic sarcoidosis. Case report: A 30-year-old female patient presented with a persistent pruritus without jaundice or fever. Examination revealed tender hepatomegaly and scratch lesions. Laboratory tests revealed elevated liver enzymes with cholestasis, and serum protein electrophoresis showed an inflammatory profile. The different viral hepatitis tests were non-contributory. Alpha fetoprotein was normal. Abdominal ultrasound and CT scans revealed a heteronodular hepatomegaly. The first liver biopsy was consistent with autoimmune hepatitis lesions. The disease improved with general corticosteroid therapy and azathioprine. Two years later, with the persistence of the pruritus, blood calcium levels and angiotensin-converting enzyme tests were found to be elevated. A new liver biopsy showed epitheliogigantocellular granulomas without caseous necrosis. A thoracic CT scan revealed mediastinal adenopathy. This suggested systemic sarcoidosis. The patient progressed well clinically and radiologically on general corticosteroids with adjuvant therapy and azathioprine. Conclusion: Sarcoidosis is a systemic disease that can affect most tissues and organs. Hepatic involvement is frequent and more often difficult to diagnose.
},
year = {2024}
}
TY - JOUR
T1 - Anicteric Cholestasis Syndrome with Pruritus Revealing Systemic Sarcoidosis
AU - Diallo Bachir Mansour
AU - Faye Fulgence Abdou
AU - Nana Mamoudou Baba
AU - Wade Adama
AU - Diack Mamadou
AU - Ndour Ndour Jean Noel Ndour
AU - Mbaye Serigne Abdou Khadr
AU - Ndiaye Yanidou
AU - Berthé Adama
AU - Touré Papa Souleymane
AU - Diop Madoky Magatte
AU - Ka Mamadou Mourtalla
Y1 - 2024/05/24
PY - 2024
N1 - https://doi.org/10.11648/j.ajim.20241202.11
DO - 10.11648/j.ajim.20241202.11
T2 - American Journal of Internal Medicine
JF - American Journal of Internal Medicine
JO - American Journal of Internal Medicine
SP - 16
EP - 20
PB - Science Publishing Group
SN - 2330-4324
UR - https://doi.org/10.11648/j.ajim.20241202.11
AB - Introduction: Sarcoidosis is a systemic granulomatosis of unknown aetiology characterised by the formation of non-caseating granulomas in organs. Hepatic involvement can be difficult to diagnose. Material and method: We report the case of a 30-year-old female patient with a long history of intractable pruritus revealing systemic sarcoidosis. Case report: A 30-year-old female patient presented with a persistent pruritus without jaundice or fever. Examination revealed tender hepatomegaly and scratch lesions. Laboratory tests revealed elevated liver enzymes with cholestasis, and serum protein electrophoresis showed an inflammatory profile. The different viral hepatitis tests were non-contributory. Alpha fetoprotein was normal. Abdominal ultrasound and CT scans revealed a heteronodular hepatomegaly. The first liver biopsy was consistent with autoimmune hepatitis lesions. The disease improved with general corticosteroid therapy and azathioprine. Two years later, with the persistence of the pruritus, blood calcium levels and angiotensin-converting enzyme tests were found to be elevated. A new liver biopsy showed epitheliogigantocellular granulomas without caseous necrosis. A thoracic CT scan revealed mediastinal adenopathy. This suggested systemic sarcoidosis. The patient progressed well clinically and radiologically on general corticosteroids with adjuvant therapy and azathioprine. Conclusion: Sarcoidosis is a systemic disease that can affect most tissues and organs. Hepatic involvement is frequent and more often difficult to diagnose.
VL - 12
IS - 2
ER -