Introduction: Antiphospholipid antibody syndrome (APS) is a condition that can affect obstetric prognosis. We conducted a study to determine the frequency of this condition in our hospital. Materials and methods: This was a prospective cross-sectional study conducted in the internal medicine department of Abdou Aziz Sy Hospital. We included all patients who had arguments in favor of APS. Results: We included 19 patients. The average age was 32 years, with extremes of 31 and 42 years. The average duration of the condition was 6.7 years, with extremes of 1 and 10 years. The average number of pregnancies was 5.79, ranging from 4 to 14 pregnancies. Obstetric manifestations included abortions (in all patients), retained dead fetuses in 3 patients, and intrauterine fetal death in 3 patients. Extra-gynecological and obstetric signs included inflammatory polyarthralgia (in 6 patients), erythematosquamous lesions (4 patients), and physical asthenia (4 patients). Antinuclear antibodies were positive in 13 patients, and anti-ECT antibodies were positive in 7 patients. Circulating lupus anticoagulant was found in 6 patients, anticardiolipin in 7 patients, and anti-glycoprotein I in 5 patients. APS was primary in 10 patients and seronegative in 2 patients. Abortions were more closely correlated with the presence of circulating lupus anticoagulant and the co-occurrence of antibodies. Treatment consisted of conventional immunosuppressants in patients monitored for secondary APS and curative heparin therapy in six patients who became pregnant during follow-up, with a favorable outcome in three patients. Conclusion: APS is an underdiagnosed condition with a serious obstetric prognosis that compromises the maternal-fetal prognosis.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Antiphospholipid syndrome is a common autoimmune disorder with multiple clinical manifestations. Its numerous obstetric complications are often underdiagnosed and underreported in most countries. They are responsible for high fetal mortality rates despite appropriate treatment in some cases
[1]
Branch DW, Lim MY. How I diagnose and treat antiphospholipid syndrome in pregnancy. Blood. 2024; 143(9): 757-768.
[1]
. In Africa, there have been sporadic reports in several countries. Constantly improving diagnostic methods, particularly in immunology, have made it possible to better classify this condition using clinical and biological criteria
[2]
Khefacha L, Rassas R, Bergaoui H, Mustapha H, Faleh R, Sakly N, Sassi M. Antiphospholipid antibodies in the obstetric antiphospholipid syndrome: Detection and antibodies profile at the Maternity and Neonatal Medicine Center of Monastir, Tunisia. J Obstet Gynaecol Res. 2022; 48(3): 673-681.
[2]
. We conducted a study with the aim of describing the obstetric manifestations of APS in women of childbearing age.
2. Materials and Methods
We conducted a prospective study from January 2022 to February 2025 at Abdou Aziz Sy Hospital in Tivaouane. We worked closely with the gynecology department to recruit women with a gynecological-obstetric history of fetal morbidity. As a result, they were referred to internal medicine for a more comprehensive examination. We systematically ruled out HIV, viral hepatitis, rubella, and toxoplasmosis infections, arguments for primary thrombophilia especially for seronegative forms.
The diagnosis of APS was made according to the 2023 ACR/EULAR criteria. All patients presented with obstetric morbidity. Antiphospholipid levels were measured twice, three months apart. A search for secondary etiology was conducted.
An investigation form was created and included the following items:
1) Clinical: sociodemographic data, gestation, parity, number of abortions, prematurity, retroplacental hematoma, HELLP syndrome, etc.
2) Other clinical signs: skin, joint, neuromuscular, etc.
3) Other complications (eclampsia, placental abruption), etc.
5) Other: anti-CCP, anatomopathology of salivary gland biopsy, etc.
6) Treatment followed.
7) Occurrence of new pregnancies and obstetric follow-up.
Pregnancy trends
The analysis was performed using PRISM 8.0 software.
3. Results
3.1. Sociodémographic Data
We included 19 patients, with a mean age of 32.055 years and extremes of 21 and 42 years. The 30-40 age group was the most represented (63%). The average duration of the disease was 6.68 years, ranging from 1 to 10 years. Sociodemographic data are shown in Table 1.
Table 1. Distribution of patients according to sociodemographic data.
Variables
Frequency
percentage
Age
20-30 ans
5
26%
30-40 ans
12
63%
>40 ans
2
11%
Occupation
Primary
14
73, 68%
tertiary
5
26, 32%
origin
Urban
16
84%
Semi-urban
2
11%
rural
1
5%
Duration of progression
0-5 years
10
53%
5-10 years
5
26%
10-15 years
3
16%
>15 years
1
5%
History
Gougerot
1
5%
Phytotherapy
1
5%
Dermatosis
2
10, 5%
Chronic Rheumatism
1
5%
3.2. Clinical
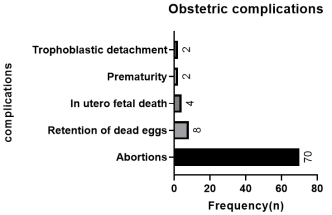
Obstetric manifestations: The total number of pregnancies was estimated at 110. The average gestation was 5.78947368, ranging from 2 to 14. The average parity was 1.33, ranging from 1 to 3 births. The average number of abortions was 3.68, ranging from 1 to 14. The various obstetric complications are shown in Figure 1.
Figure 1. Distribution of patients according to different obstetric complications.
Non-obstetric signs: Extra-gynecological signs are dominated by inflammatory polyarthralgia (32%) and chronic asthenia (26%). These various manifestations are listed in Table 2.
Table 2. Distribution of patients according to extra-gynecological signs.
Signs
Frequency (n)
Percentage (n)
Inflammatory polarthritis
6
32%
Chronic asthenia
5
26%
Diffuse pain
1
5%
muscle cramps
1
5%
Dry eye, mouth, and genital syndrome
2
11%
Erythematosquamous lesions
3
16%
Fever
2
11%
Arterial Hypotension
1
5%
Dyspnea
1
5%
Palpitations
1
5%
leukorrhea
3
16%
Metrorrhagia
2
11%
3.3. Biology
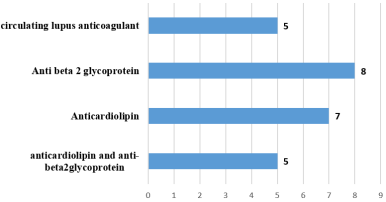
Anemia was found in one patient, hyperleukocytosis and thrombocytopenia in one patient each, and elevated CRP in three patients. Antinuclear antibodies were positive in 13 patients with a mean titer of 2575 IU (100–10,000), with speckled fluorescence in 11 patients, nucleolar in one patient, and cytoskeletal in one patient. Anti-Sm antibodies were positive in four patients, anti-CCP in two patients, anti-SSA and anti-Ro52 in two patients, anti-Mi2A in three patients, and anti-DNA in two patients. The other antibodies were found in one case each: anti-nucleosomes, anti-Scl 70, anti-Pm-Scl 100, anti-Rp11, anti-Rp155, and anti-PCNA. Anti-phospholipid antibodies were measured in all patients and the result is reported in Figure 2. One patient had stage 3 lymphocytic sialadenitis according to Chisolm and Masson.
Figure 2. Distribution of patients according to antiphospholipid antibodies.
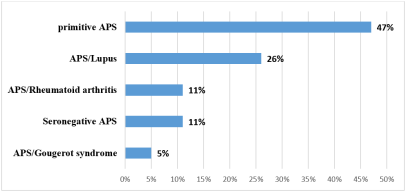
APS was primary in 9 patients (47%), secondary to lupus in 5 patients, and secondary to rheumatoid arthritis in 2 patients. The different etiologies are listed in Figure 3.
Figure 3. Distribution of patients according to etiology.
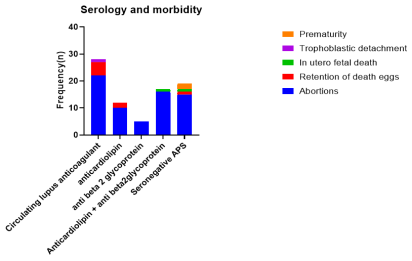
We found that Circulating lupus anticoagulant was more strongly correlated with recurrent miscarriages, with a significant difference, p=0.0057, R2 = 0,8395. The various obstetric complications associated with different antiphospholipid antibodies are listed in Figure 4.
Figure 4. Distribution and correlation between obstetric complications and the antiphospholipid antibodies.
During follow-up, we recorded pregnancies in some patients. We observed one full-term pregnancy and three cesarean sections, some of which were related to the threat. The children are alive and well. During these pregnancies, the patients were treated with low molecular weight heparin 100 IU/kg/12 hours.
4. Discussion
Antiphospholipid syndrome (APS) is considered a rare disease. Its prevalence is generally estimated at around 20 to 50 cases per 100,000 individuals in the general population. Some sources indicate a prevalence of less than 1 case per 2,000 individuals (which is the definition of a rare disease in Europe). Another estimate suggests that around 0.5% of the population is affected
[3]
General information: Antiphospholipid Syndrome (APS). Fair, Rare Autoimmune and Autoinflammatory Diseases Health Network. Available at:
Durcan L, Petri M. Epidemiology of the antiphospholipid syndrome. Dans: Cervera R, Espinosa G, Khamashta MA, editeurs. Antiphospholipid Syndrome in Systemic Autoimmune Diseases. 2e ed. Amsterdam: Elsevier; 2016. p. 17–30.
[3, 4]
.
The incidence is approximately 5 new cases per 100,000 people per year. It is a disease that affects young women (4 to 5 times more women than men for primary APS). It is often diagnosed in women of childbearing age. APS can be primary (isolated) or secondary (associated with other autoimmune diseases, most commonly systemic lupus). The mere presence of antiphospholipid antibodies (aPL) is more common (found in 1 to 5% of the general population), but the majority of these asymptomatic carriers never develop the syndrome. The diagnosis of APS requires the combination of antibodies with clinical manifestations (thrombosis or obstetric complications)
[5]
Matraszek VV, Heřman H, Hromadníková I. The relevance of antiphospholipid antibodies in obstetrics. Ceska Gynekol. 2024; 89(3): 237-244.
[5]
.
Obstetric APS is defined by the combination of the presence of aPL and specific obstetric complications (fetal loss, premature delivery, severe preeclampsia, etc.).
The frequency of antiphospholipid antibodies (aPL) is significantly higher in women with a history of pregnancy complications. APS is responsible for approximately 10 to 20% of cases of unexplained early and/or recurrent spontaneous miscarriages. In some series of patients with at least three consecutive miscarriages, the prevalence of aPL is estimated to be between 3.6% and 21%, depending on the laboratory criteria used. The prevalence of aPL is also higher in patients who have had one or more unexplained fetal deaths after 10 weeks of amenorrhea. aPLs are also associated with an increased risk of intrauterine growth restriction (IUGR) and severe preeclampsia or eclampsia requiring premature delivery before 34 weeks of amenorrhea. In summary, APS is a rare but important cause of obstetric complications, and testing for antiphospholipid antibodies is routinely recommended in cases of a history of serious pregnancy complications
[6]
Prado D, Dujardin F, Goutouly A, et al. Prevalence of Antiphospholipid Antibody Syndrome Among Patients with Recurrent Pregnancy Loss: Impact of the Revised 2023 ACR/EULAR Antiphospholipid Syndrome Criteria. J Clin Med. 2024; 13(24): 7698.
[7]
Abreu I, Dantas L, Pinho J, et al. Antiphospholipid syndrome in pregnancy: a comprehensive literature review. BMC Pregnancy Childbirth. 2024; 24(1): 159.
[6, 7]
.
Obstetric complications are common in women with APS, who are considered high-risk pregnancies. There is a high risk of recurrent spontaneous miscarriages (SMs) (15 to 20% of pregnancies) (three or more consecutive SMs before 10 weeks of amenorrhea), which is one of the criteria for classifying the syndrome. It is estimated that at least 15% of recurrent miscarriages are due to APS. The overall prevalence of fetal loss in untreated women with APS is reported to range from 50 to 75%. One or more unexplained fetal deaths after 10 weeks of amenorrhea of a morphologically normal fetus is another diagnostic criterion for APS. It increases the risk of premature birth before 34 weeks of amenorrhea of a morphologically normal newborn due to severe preeclampsia or severe placental insufficiency (with intrauterine growth restriction (IUGR), for example (3 to 9% of pregnancies). An increased risk of preeclampsia and hypertensive disorders has been reported in women with APS
[8]
Gupta D, Goel M, Dhiman P, et al. Antiphospholipid syndrome in pregnancy: A comprehensive review. World J Obstet Gynecol. 2025; 12(2): 103837.
[9]
French National College of Gynecologists and Obstetricians (CNGOF). Preeclampsia 2023 RPC. Paris: CNGOF; 2023.
[8, 9]
.
For a diagnosis of APS to be made, one of the above clinical manifestations must be associated with the persistent presence of at least one of the following three types of antiphospholipid antibodies, measured at least 12 weeks apart:
1) Circulating lupus anticoagulant (LCA or LA)
2) Anti-cardiolipin antibodies (aCL) (IgG and/or IgM, at moderate or high levels)
3) Anti-β2-glycoprotein I antibodies (anti-β2GPI) (IgG and/or IgM, at moderate or high levels)
4) The fundamental criterion is that the biological result must be positive on two occasions, at least 12 weeks apart
According to classification criteria (including the most recent ACR/EULAR 2023 criteria, which use an additive scoring system for classification), a diagnosis of obstetric SAPL is generally made if the patient presents with: At least one obstetric clinical criterion+ At least one persistent biological criterion
[10]
Bagou G, Sentilhes L, Mercier F-J, Berveiller P, Blanc J, Cesareo E, et al. Recommendations for professional practice 2022. Management of obstetric emergencies in emergency medicine. Ann Fr Med Urgence. 2022; 12: 249-265.
[10]
.
The diagnosis of APS is often made and managed by a multidisciplinary team, involving obstetricians, internists, and/or immunologists
[11]
Barbhaiya M, Zuily S, Naden R, Hendry A, Manneville F, Amigo M-C, et al. The 2023 ACR/EULAR Antiphospholipid Syndrome Classification Criteria. Arthritis Rheumatol. 2023 Nov; 75(11): 1887-1901.
[11]
.
APS is classified as secondary when it occurs in a patient who already has or develops another autoimmune disease. The most common and significant association is with systemic lupus erythematosus (SLE). This is referred to as lupus-associated APS. Primary (or isolated) antiphospholipid syndrome (APS) is defined by the presence of the diagnostic criteria for APS without any other associated systemic autoimmune disease
[11]
Barbhaiya M, Zuily S, Naden R, Hendry A, Manneville F, Amigo M-C, et al. The 2023 ACR/EULAR Antiphospholipid Syndrome Classification Criteria. Arthritis Rheumatol. 2023 Nov; 75(11): 1887-1901.
[12]
Lupus Reference Center. Antiphospholipid Syndrome in Adults and Children: National Protocol for Diagnosis and Care. Saint-Ouen: Head Authority for Health (HAS); Oct 2022 [cited 2025 Sep 29]. Available from:
Seronegative Antiphospholipid Syndrome is a distinct and controversial clinical entity used to describe patients who present with typical clinical manifestations of APS but whose laboratory tests for antiphospholipid antibodies (aPL) are persistently negative. The hypothesis of seronegative APS is raised when physicians suspect that the thrombotic or obstetric event is still related to antiphospholipid syndrome, but the antibodies are not detectable by conventional methods. Given that seronegative APS is a diagnosis of exclusion and does not meet formal criteria, its management is a subject of debate among experts. It is crucial to rule out all other possible causes of thrombosis (other inherited or acquired thrombophilias) or obstetric morbidity before considering this hypothesis. If the risk of recurrence is considered high (e.g., history of severe thrombosis), patients are often treated as if they had definite APS with anticoagulation (for thrombosis) or treatment with aspirin and low molecular weight heparin (for obstetric morbidity), due to strong clinical suspicion Other antibodies directed against phospholipids or cofactors can be tested in specialized laboratories (Anti-phosphatidylethanolamin (aPE), Anti-phosphatidylinositol (aPI), Anti-acid phosphatidic (aPA), Anti-Annexin A5)
[13]
Miyakis S, Giannakopoulos S, Zampeli E, Vlachogiannis N, Tesser N, Vlachoyiannopoulos PG. Seronegative antiphospholipid syndrome: refining the value of “non-criteria” antibodies for diagnosis and clinical management. Haematologica. 2020 Feb; 105(2): 315-23.
[14]
Arnaud L, Mathian A, Devilliers H, Lefèvre G, Hie M, Amoura Z. Seronegative antiphospholipid syndrome. Autoimmun Rev. 2 013; 12(9): 923-7.
[15]
Tektonidou MG, Andreoli L, Limper M, et al. EULAR recommendations for the management of antiphospholipid syndrome in adults. Ann Rheum Dis. 2019; 78(10): 1296-1304.
[13-15]
.
The treatment of obstetric antiphospholipid syndrome (APS) is a form of secondary prevention and aims to reduce the risk of pregnancy complications (miscarriages, fetal death, preeclampsia, etc.). The standard and most effective treatment is a combination of low-dose aspirin and low molecular weight heparin (LMWH): Acetylsalicylic acid (ASA) (75 to 100 mg per day) and low molecular weight heparin (LMWH) administered by daily subcutaneous injection. Treatment is generally continued until the end of pregnancy and sometimes extended for 4 to 6 weeks postpartum, due to the increased risk of maternal thrombosis during this period. If the patient has obstetric APS AND a history of maternal thrombosis (secondary APS), the LMWH dose may be increased to a full therapeutic dose during pregnancy and postpartum to prevent both obstetric complications and recurrence of thrombosis in the mother. Hydroxychloroquine is often continued in patients with secondary APS due to systemic lupus, as it has an antithrombotic and protective effect. Treatment should always be managed by a multidisciplinary team including an internist and an obstetrician specializing in high-risk pregnancies
[16]
Comont T. Syndrome des antiphospholipides et grossesse. Real Gynecol Obstet. 2017; 188: 15–17.
[16]
.
Regular, specialized monitoring is essential throughout pregnancy. This includes:
1) Regular consultations with a team of experts (internist, specialized obstetrician).
2) Frequent ultrasounds to monitor fetal growth and placental function (Doppler).
3) Blood pressure checks to screen for preeclampsia.
In most cases, these therapeutic and monitoring measures enable the pregnancy to be carried to term with a favorable outcome
[15]
Tektonidou MG, Andreoli L, Limper M, et al. EULAR recommendations for the management of antiphospholipid syndrome in adults. Ann Rheum Dis. 2019; 78(10): 1296-1304.
[16]
Comont T. Syndrome des antiphospholipides et grossesse. Real Gynecol Obstet. 2017; 188: 15–17.
[15, 16]
.
5. Conclusion
APS is a little-known condition. It can cause thromboembolic events as well as maternal-fetal complications, the management of which requires close collaboration between internists and gynecologists. Pregnancy requires careful monitoring with regular clinical and biological surveillance.
Branch DW, Lim MY. How I diagnose and treat antiphospholipid syndrome in pregnancy. Blood. 2024; 143(9): 757-768.
[2]
Khefacha L, Rassas R, Bergaoui H, Mustapha H, Faleh R, Sakly N, Sassi M. Antiphospholipid antibodies in the obstetric antiphospholipid syndrome: Detection and antibodies profile at the Maternity and Neonatal Medicine Center of Monastir, Tunisia. J Obstet Gynaecol Res. 2022; 48(3): 673-681.
[3]
General information: Antiphospholipid Syndrome (APS). Fair, Rare Autoimmune and Autoinflammatory Diseases Health Network. Available at:
Durcan L, Petri M. Epidemiology of the antiphospholipid syndrome. Dans: Cervera R, Espinosa G, Khamashta MA, editeurs. Antiphospholipid Syndrome in Systemic Autoimmune Diseases. 2e ed. Amsterdam: Elsevier; 2016. p. 17–30.
[5]
Matraszek VV, Heřman H, Hromadníková I. The relevance of antiphospholipid antibodies in obstetrics. Ceska Gynekol. 2024; 89(3): 237-244.
[6]
Prado D, Dujardin F, Goutouly A, et al. Prevalence of Antiphospholipid Antibody Syndrome Among Patients with Recurrent Pregnancy Loss: Impact of the Revised 2023 ACR/EULAR Antiphospholipid Syndrome Criteria. J Clin Med. 2024; 13(24): 7698.
[7]
Abreu I, Dantas L, Pinho J, et al. Antiphospholipid syndrome in pregnancy: a comprehensive literature review. BMC Pregnancy Childbirth. 2024; 24(1): 159.
[8]
Gupta D, Goel M, Dhiman P, et al. Antiphospholipid syndrome in pregnancy: A comprehensive review. World J Obstet Gynecol. 2025; 12(2): 103837.
[9]
French National College of Gynecologists and Obstetricians (CNGOF). Preeclampsia 2023 RPC. Paris: CNGOF; 2023.
[10]
Bagou G, Sentilhes L, Mercier F-J, Berveiller P, Blanc J, Cesareo E, et al. Recommendations for professional practice 2022. Management of obstetric emergencies in emergency medicine. Ann Fr Med Urgence. 2022; 12: 249-265.
[11]
Barbhaiya M, Zuily S, Naden R, Hendry A, Manneville F, Amigo M-C, et al. The 2023 ACR/EULAR Antiphospholipid Syndrome Classification Criteria. Arthritis Rheumatol. 2023 Nov; 75(11): 1887-1901.
[12]
Lupus Reference Center. Antiphospholipid Syndrome in Adults and Children: National Protocol for Diagnosis and Care. Saint-Ouen: Head Authority for Health (HAS); Oct 2022 [cited 2025 Sep 29]. Available from:
Miyakis S, Giannakopoulos S, Zampeli E, Vlachogiannis N, Tesser N, Vlachoyiannopoulos PG. Seronegative antiphospholipid syndrome: refining the value of “non-criteria” antibodies for diagnosis and clinical management. Haematologica. 2020 Feb; 105(2): 315-23.
[14]
Arnaud L, Mathian A, Devilliers H, Lefèvre G, Hie M, Amoura Z. Seronegative antiphospholipid syndrome. Autoimmun Rev. 2 013; 12(9): 923-7.
[15]
Tektonidou MG, Andreoli L, Limper M, et al. EULAR recommendations for the management of antiphospholipid syndrome in adults. Ann Rheum Dis. 2019; 78(10): 1296-1304.
[16]
Comont T. Syndrome des antiphospholipides et grossesse. Real Gynecol Obstet. 2017; 188: 15–17.
Diallo, B. M., Fall, K., Sow, A., Wade, A., Thiam, A. I., et al. (2026). Obstetric Morbidity and Mortality Associated with Antiphospholipid Syndrome: A Study Conducted in Tivaouane, Senegal. American Journal of Internal Medicine, 14(1), 11-17. https://doi.org/10.11648/j.ajim.20261401.12
Diallo, B. M.; Fall, K.; Sow, A.; Wade, A.; Thiam, A. I., et al. Obstetric Morbidity and Mortality Associated with Antiphospholipid Syndrome: A Study Conducted in Tivaouane, Senegal. Am. J. Intern. Med.2026, 14(1), 11-17. doi: 10.11648/j.ajim.20261401.12
Diallo BM, Fall K, Sow A, Wade A, Thiam AI, et al. Obstetric Morbidity and Mortality Associated with Antiphospholipid Syndrome: A Study Conducted in Tivaouane, Senegal. Am J Intern Med. 2026;14(1):11-17. doi: 10.11648/j.ajim.20261401.12
@article{10.11648/j.ajim.20261401.12,
author = {Bachir Mansour Diallo and Khalifa Fall and Aboubakry Sow and Adama Wade and Abo Ibrahima Thiam and Mafing Aya Sylla and Stephane Bacourine and Haolatou Gano and Aicha Kaneye and Aminata Dia Gueye and Yanidou Ndiaye and Adama Berthe and Papa Souleymane Toure and Madoky Magatte Diop and Mamadou Mourtalla Ka},
title = {Obstetric Morbidity and Mortality Associated with Antiphospholipid Syndrome: A Study Conducted in Tivaouane, Senegal},
journal = {American Journal of Internal Medicine},
volume = {14},
number = {1},
pages = {11-17},
doi = {10.11648/j.ajim.20261401.12},
url = {https://doi.org/10.11648/j.ajim.20261401.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajim.20261401.12},
abstract = {Introduction: Antiphospholipid antibody syndrome (APS) is a condition that can affect obstetric prognosis. We conducted a study to determine the frequency of this condition in our hospital. Materials and methods: This was a prospective cross-sectional study conducted in the internal medicine department of Abdou Aziz Sy Hospital. We included all patients who had arguments in favor of APS. Results: We included 19 patients. The average age was 32 years, with extremes of 31 and 42 years. The average duration of the condition was 6.7 years, with extremes of 1 and 10 years. The average number of pregnancies was 5.79, ranging from 4 to 14 pregnancies. Obstetric manifestations included abortions (in all patients), retained dead fetuses in 3 patients, and intrauterine fetal death in 3 patients. Extra-gynecological and obstetric signs included inflammatory polyarthralgia (in 6 patients), erythematosquamous lesions (4 patients), and physical asthenia (4 patients). Antinuclear antibodies were positive in 13 patients, and anti-ECT antibodies were positive in 7 patients. Circulating lupus anticoagulant was found in 6 patients, anticardiolipin in 7 patients, and anti-glycoprotein I in 5 patients. APS was primary in 10 patients and seronegative in 2 patients. Abortions were more closely correlated with the presence of circulating lupus anticoagulant and the co-occurrence of antibodies. Treatment consisted of conventional immunosuppressants in patients monitored for secondary APS and curative heparin therapy in six patients who became pregnant during follow-up, with a favorable outcome in three patients. Conclusion: APS is an underdiagnosed condition with a serious obstetric prognosis that compromises the maternal-fetal prognosis.},
year = {2026}
}
TY - JOUR
T1 - Obstetric Morbidity and Mortality Associated with Antiphospholipid Syndrome: A Study Conducted in Tivaouane, Senegal
AU - Bachir Mansour Diallo
AU - Khalifa Fall
AU - Aboubakry Sow
AU - Adama Wade
AU - Abo Ibrahima Thiam
AU - Mafing Aya Sylla
AU - Stephane Bacourine
AU - Haolatou Gano
AU - Aicha Kaneye
AU - Aminata Dia Gueye
AU - Yanidou Ndiaye
AU - Adama Berthe
AU - Papa Souleymane Toure
AU - Madoky Magatte Diop
AU - Mamadou Mourtalla Ka
Y1 - 2026/03/23
PY - 2026
N1 - https://doi.org/10.11648/j.ajim.20261401.12
DO - 10.11648/j.ajim.20261401.12
T2 - American Journal of Internal Medicine
JF - American Journal of Internal Medicine
JO - American Journal of Internal Medicine
SP - 11
EP - 17
PB - Science Publishing Group
SN - 2330-4324
UR - https://doi.org/10.11648/j.ajim.20261401.12
AB - Introduction: Antiphospholipid antibody syndrome (APS) is a condition that can affect obstetric prognosis. We conducted a study to determine the frequency of this condition in our hospital. Materials and methods: This was a prospective cross-sectional study conducted in the internal medicine department of Abdou Aziz Sy Hospital. We included all patients who had arguments in favor of APS. Results: We included 19 patients. The average age was 32 years, with extremes of 31 and 42 years. The average duration of the condition was 6.7 years, with extremes of 1 and 10 years. The average number of pregnancies was 5.79, ranging from 4 to 14 pregnancies. Obstetric manifestations included abortions (in all patients), retained dead fetuses in 3 patients, and intrauterine fetal death in 3 patients. Extra-gynecological and obstetric signs included inflammatory polyarthralgia (in 6 patients), erythematosquamous lesions (4 patients), and physical asthenia (4 patients). Antinuclear antibodies were positive in 13 patients, and anti-ECT antibodies were positive in 7 patients. Circulating lupus anticoagulant was found in 6 patients, anticardiolipin in 7 patients, and anti-glycoprotein I in 5 patients. APS was primary in 10 patients and seronegative in 2 patients. Abortions were more closely correlated with the presence of circulating lupus anticoagulant and the co-occurrence of antibodies. Treatment consisted of conventional immunosuppressants in patients monitored for secondary APS and curative heparin therapy in six patients who became pregnant during follow-up, with a favorable outcome in three patients. Conclusion: APS is an underdiagnosed condition with a serious obstetric prognosis that compromises the maternal-fetal prognosis.
VL - 14
IS - 1
ER -
Diallo, B. M., Fall, K., Sow, A., Wade, A., Thiam, A. I., et al. (2026). Obstetric Morbidity and Mortality Associated with Antiphospholipid Syndrome: A Study Conducted in Tivaouane, Senegal. American Journal of Internal Medicine, 14(1), 11-17. https://doi.org/10.11648/j.ajim.20261401.12
Diallo, B. M.; Fall, K.; Sow, A.; Wade, A.; Thiam, A. I., et al. Obstetric Morbidity and Mortality Associated with Antiphospholipid Syndrome: A Study Conducted in Tivaouane, Senegal. Am. J. Intern. Med.2026, 14(1), 11-17. doi: 10.11648/j.ajim.20261401.12
Diallo BM, Fall K, Sow A, Wade A, Thiam AI, et al. Obstetric Morbidity and Mortality Associated with Antiphospholipid Syndrome: A Study Conducted in Tivaouane, Senegal. Am J Intern Med. 2026;14(1):11-17. doi: 10.11648/j.ajim.20261401.12
@article{10.11648/j.ajim.20261401.12,
author = {Bachir Mansour Diallo and Khalifa Fall and Aboubakry Sow and Adama Wade and Abo Ibrahima Thiam and Mafing Aya Sylla and Stephane Bacourine and Haolatou Gano and Aicha Kaneye and Aminata Dia Gueye and Yanidou Ndiaye and Adama Berthe and Papa Souleymane Toure and Madoky Magatte Diop and Mamadou Mourtalla Ka},
title = {Obstetric Morbidity and Mortality Associated with Antiphospholipid Syndrome: A Study Conducted in Tivaouane, Senegal},
journal = {American Journal of Internal Medicine},
volume = {14},
number = {1},
pages = {11-17},
doi = {10.11648/j.ajim.20261401.12},
url = {https://doi.org/10.11648/j.ajim.20261401.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajim.20261401.12},
abstract = {Introduction: Antiphospholipid antibody syndrome (APS) is a condition that can affect obstetric prognosis. We conducted a study to determine the frequency of this condition in our hospital. Materials and methods: This was a prospective cross-sectional study conducted in the internal medicine department of Abdou Aziz Sy Hospital. We included all patients who had arguments in favor of APS. Results: We included 19 patients. The average age was 32 years, with extremes of 31 and 42 years. The average duration of the condition was 6.7 years, with extremes of 1 and 10 years. The average number of pregnancies was 5.79, ranging from 4 to 14 pregnancies. Obstetric manifestations included abortions (in all patients), retained dead fetuses in 3 patients, and intrauterine fetal death in 3 patients. Extra-gynecological and obstetric signs included inflammatory polyarthralgia (in 6 patients), erythematosquamous lesions (4 patients), and physical asthenia (4 patients). Antinuclear antibodies were positive in 13 patients, and anti-ECT antibodies were positive in 7 patients. Circulating lupus anticoagulant was found in 6 patients, anticardiolipin in 7 patients, and anti-glycoprotein I in 5 patients. APS was primary in 10 patients and seronegative in 2 patients. Abortions were more closely correlated with the presence of circulating lupus anticoagulant and the co-occurrence of antibodies. Treatment consisted of conventional immunosuppressants in patients monitored for secondary APS and curative heparin therapy in six patients who became pregnant during follow-up, with a favorable outcome in three patients. Conclusion: APS is an underdiagnosed condition with a serious obstetric prognosis that compromises the maternal-fetal prognosis.},
year = {2026}
}
TY - JOUR
T1 - Obstetric Morbidity and Mortality Associated with Antiphospholipid Syndrome: A Study Conducted in Tivaouane, Senegal
AU - Bachir Mansour Diallo
AU - Khalifa Fall
AU - Aboubakry Sow
AU - Adama Wade
AU - Abo Ibrahima Thiam
AU - Mafing Aya Sylla
AU - Stephane Bacourine
AU - Haolatou Gano
AU - Aicha Kaneye
AU - Aminata Dia Gueye
AU - Yanidou Ndiaye
AU - Adama Berthe
AU - Papa Souleymane Toure
AU - Madoky Magatte Diop
AU - Mamadou Mourtalla Ka
Y1 - 2026/03/23
PY - 2026
N1 - https://doi.org/10.11648/j.ajim.20261401.12
DO - 10.11648/j.ajim.20261401.12
T2 - American Journal of Internal Medicine
JF - American Journal of Internal Medicine
JO - American Journal of Internal Medicine
SP - 11
EP - 17
PB - Science Publishing Group
SN - 2330-4324
UR - https://doi.org/10.11648/j.ajim.20261401.12
AB - Introduction: Antiphospholipid antibody syndrome (APS) is a condition that can affect obstetric prognosis. We conducted a study to determine the frequency of this condition in our hospital. Materials and methods: This was a prospective cross-sectional study conducted in the internal medicine department of Abdou Aziz Sy Hospital. We included all patients who had arguments in favor of APS. Results: We included 19 patients. The average age was 32 years, with extremes of 31 and 42 years. The average duration of the condition was 6.7 years, with extremes of 1 and 10 years. The average number of pregnancies was 5.79, ranging from 4 to 14 pregnancies. Obstetric manifestations included abortions (in all patients), retained dead fetuses in 3 patients, and intrauterine fetal death in 3 patients. Extra-gynecological and obstetric signs included inflammatory polyarthralgia (in 6 patients), erythematosquamous lesions (4 patients), and physical asthenia (4 patients). Antinuclear antibodies were positive in 13 patients, and anti-ECT antibodies were positive in 7 patients. Circulating lupus anticoagulant was found in 6 patients, anticardiolipin in 7 patients, and anti-glycoprotein I in 5 patients. APS was primary in 10 patients and seronegative in 2 patients. Abortions were more closely correlated with the presence of circulating lupus anticoagulant and the co-occurrence of antibodies. Treatment consisted of conventional immunosuppressants in patients monitored for secondary APS and curative heparin therapy in six patients who became pregnant during follow-up, with a favorable outcome in three patients. Conclusion: APS is an underdiagnosed condition with a serious obstetric prognosis that compromises the maternal-fetal prognosis.
VL - 14
IS - 1
ER -