Abstract
HIV remains the most significant public health and development challenge in the world. Youth in sub-Saharan Africa are primarily affected by the HIV epidemic. Despite the availability of HIV prevention options, new infections among youth in Kenya only reduced by 56% between 2015 and 2021. Various HIV prevention interventions have been implemented among youth with little or no assessment of their effects on risky sexual behavior. The objective of the study was to investigate effect of comprehensive HIV prevention information package on uptake of HIV prevention services among youth in Kenya. A non-randomized control trial was conducted with Kakamega and Kericho as intervention and Comparison County respectively. The pretest questionnaire was administered in December 2021. The posttest questionnaire was administered after nine months of providing HIV prevention information package. Quantitative data was analyzed using chi square and t-test. Qualitative data was transcribed and analyzed thematically. The youth significantly utilized HIV prevention services (83.6%) and information on, abstinence, consistent and correct condom use (t = 12.248, df=2, p = 0.0001). The intervention significantly increased utilization of HIV testing services from 60.1% to 83.0% (t = 6.547, df = 2, p = 0.023). There was a significant difference in number of youths in Kakamega than Kericho who plan to use condoms in future (χ2 = 100.236, P = 0.0001). The comprehensive HIV prevention information package increased uptake of HIV services. The findings will inform national rollout of the intervention to contribute to safer sexual behaviors among youth.
|
Published in
|
Central African Journal of Public Health (Volume 11, Issue 4)
|
|
DOI
|
10.11648/j.cajph.20251104.15
|
|
Page(s)
|
192-200 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2025. Published by Science Publishing Group
|
Keywords
Comprehensive HIV Information, Combination HIV Prevention, Non-randomized Trial, HIV, Sexual Behavior, Youth
1. Introduction
Human immuno-deficiency virus (HIV) is the World’s most significant challenge in public health
| [1] | UNAIDS. HIV Estimates. Joint United Nations Programme on HIV/AIDS, 2022. |
[1]
. Globally, over 1.5 million people became newly infected with HIV in 2021 compared with 1.6 million in 2019 representing 7% decline. Approximately 400 000 young people aged 15-24 years in the world were newly infected with HIV in 2021 down from 450 000 in 2019
| [1] | UNAIDS. HIV Estimates. Joint United Nations Programme on HIV/AIDS, 2022. |
[1]
. An estimated 269 000 young people aged 15-24 years got newly infected in 2021 in the Sub-Saharan region down from 332 100 in 2019. The East and South African region had the highest reduction in new HIV infections at 38% since 2010. Only 30% males and 19% females aged 15-24 in sub-Saharan Africa have comprehensive knowledge on HIV. Condom use among men with more than one sexual partner was only 58.6%, far from the global target of 90% by 2020
.
New HIV infections in Kenya have stabilized at an average of 34 540 people in 2021 down from 41 408 in 2019
| [3] | MOH. Kenya HIV Estimates Report. National AIDS Control Counci, 2022. |
[3]
. The youth contribute 42% of all new HIV infections in Kenya
| [3] | MOH. Kenya HIV Estimates Report. National AIDS Control Counci, 2022. |
[3]
. Only 42.6% of females and 69.6% of males aged 15-24 years with more than one sexual partner reported using a condom in their past sexual intercourse
| [4] | MOH. Kenya Demographic and Health survey Kenya National Bureau of Statistics, 2022. |
[4]
. Additionally, only 54% females and 55% males aged 15-24 years have comprehensive knowledge of HIV prevention
| [4] | MOH. Kenya Demographic and Health survey Kenya National Bureau of Statistics, 2022. |
[4]
. Kakamega and Kericho county have a projected population of 1 867 579 and 995 566
| [5] | KNBS. Kenya Population and Housing Census. Kenya National Bureau of Statistics, 2022. Available from www.knbs.or.ke |
[5]
. New HIV infections among youth in Kakamega and Kericho counties reduced by 32 and 18.4% respectively between 2020 and 2022. Youths in Kakamega and Kericho counties contribute 31% and 39% of all new cases of HIV infections in the county respectively
| [3] | MOH. Kenya HIV Estimates Report. National AIDS Control Counci, 2022. |
[3]
.
The correlates of and motivations for HIV testing were explored using the Health Belief Model (HBM) on youth from informal settlements in Nairobi, Kenya. The findings indicated that perceived risk for HIV infection may drive HIV testing among youth
| [6] | Kabiru CW, Beguy D, Crichton J and Zulu ME: HIV/AIDS among youth in urban informal (slum) settlements in Kenya: What are the correlates of and motivations for HIV testing?. BMC Public Health 11, 685, 2011. https://doi.org/10.1186/1471-2458-11-685 |
[6]
. A cross sectional study conducted among among youth aged 15~24 years in Gambia, found that socio-demographic factors, HIV knowledge and sexual risk behaviors influence utilization of HIV testing services
. A study conducted among Mozambican women found that having more than 6 years of education and being younger and single were significant predictors for current sexual activity and condom use. Condom use negotiation self-efficacy is a significant predictor for condom use
| [8] | Patrão AL and McIntyre T: Socio-demographic, marital and psychosocial predictors of safe sex behaviour among Mozambican women at risk for HIV/AIDS. African Journal of AIDS Research, 17(4), 323-331, 2018. https://doi.org/10.2989/16085906.2018.1536672 |
[8]
. A study in the Free State province in South Africa found that the strongest predictor of condom use was its perceived need followed by knowledge of correct use, condom availability, young age, being single and higher education. In addition to existing social marketing campaigns, tailored approaches should focus on establishing the perceived need for condom-use and improving skills for correct usage. They should also incorporate interventions to reduce the shame associated with condoms and individual counselling of those likely to refuse condoms
| [9] | Chandran TM, Berkvens D, Chikobvu P, Nöstlinger C, Colebunders R, Williams GB and Speybroeck N: Predictors of condom use and refusal among the population of Free State province in South Africa. BMC Public Health 12, 381(2012). https://doi.org/10.1186/1471-2458-12-381 |
[9]
.
Various HIV prevention interventions have been implemented among the youth with little or no assessment of their effect on risky sexual behavior. There is currently no effective HIV vaccine and reducing risky sexual behaviors among youth is essential in reducing their exposure to HIV virus. If we prevent new infections among youth, we will enhance health and productivity and reduce future treatment costs and ill-health liabilities. The study will provide new evidence to inform design and implementation of intervention to reduce risky sexual behavior among youth. The aim of the study was to investigate effect of comprehensive HIV prevention information package on uptake of HIV prevention services among youth in Kenya.
2. Materials and Methods
2.1. Study Design
A Nonrandomized control trial was conducted for 9 months from December 2021 using qualitative and quantitative methods. Nonrandomized control trials are typically much cheaper and may be more politically feasible to conduct
| [10] | Campbell DT and Stanley J: Experimental and Quasi-Experimental Designs for Research. Houghton Mifflin, 1966. Boston, USA. |
[10]
.
2.2. Setting
The study was undertaken in Kakamega as intervention and Kericho as comparison county. These two were purposively selected because they are medium incidence
| [3] | MOH. Kenya HIV Estimates Report. National AIDS Control Counci, 2022. |
[3]
. The three sub counties in the two counties were randomly selected to represent urban, cosmopolitan and rural youth. Nandi county is geographically located between Intervention area and Comparison area to prevent effect of spillover or mixing of youth from the two study counties.
2.3. Study Population
The research population of interest were all youth in Kakamega and Kericho County. A target of 495 youth was the study subjects. The study participants were selected from youth group meetings to represent various youth segments and from tertiary instutions to represent the in-school youth. Consenting youth residing in the intervention and control counties between December 2021 and September 2022 were the study participants.
2.4. Selection Criteria
2.4.1. Inclusion Criteria
1) Confirmed young person residing in the study counties for at least one year
2) Youth aged 15 -24 years and able to give informed consent
3) Youth below 18 years who assent in addition to parental consent
2.4.2. Exclusion Criteria
1) Young people who don’t consent
2) Youths who don’t consent
3) Mentally disturbed youths
2.5. Sampling
2.5.1. Sampling Strategy
Stratified sampling was used to select three sub counties in the intervention and control county to represent urban, cosmopolitan and rural youth. Simple random sampling was used to select colleges or technical institutes to represent in-school youth and youth groups to represent out of school youth in the intervention and control counties. Individual youth who consented in both counties were invited to fill a questionnaire at baseline and after 9 months of providing comprehensive HIV prevention information package in the intervention county. Consecutive sampling was used to include all accessible individual study participants to provide information on the study questions. The change in usage of condoms and HIV testing services in the intervention county was compared with the comparison county.
2.5.2. Sample Size Determination
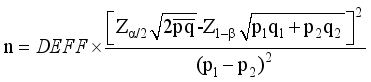
A representative sample size for the non-randomised control trial was determined using a formula developed for intervention studies
| [11] | Suresh KP and Chandrashekara S: Sample Size Estimation and Power Analysis for Clinical Research Studies. Journal of Human Reproductive Science, 2012; 5, 7-13. |
[11]
.
According to the Kenya Demographic and Health Survey, only 59% of youth in Kenya have comprehensive knowledge on HIV and AIDS
| [12] | MOH. Kenya Demographic and Health survey. KenyaNational Bureau of Statistics, 2014. |
[12]
. We estimate that the intervention will increase comprehensive knowledge among this age group by 10%. Adjusting for 10% non-response rate
| [13] | Israel GD: Sampling The Evidence Of Extension Program Impact. IFAS, 1992. University of Florida. |
[13]
.
The sample size was 495 youth for the baseline survey and 495 in the follow-up survey. We will use stratified probability proportional to size (PPS) method
to obtain the number of young people to be sampled per county. The population of interest in each county was sampled proportional to its size as summarized in
Table 1.
Table 1. Population size and sample size of participants in each sample locations.
| County | Sub county | Youth (15-24 years) | Sample |
1 | Kakamega | Lurambi | 42322 | 140 |
2 | Kakamega | Lugari | 25431 | 85 |
3 | Kakamega | Navakholo | 32100 | 106 |
Sub total | 99853 | 331 |
4 | Kericho | Ainamoi | 37122 | 68 |
5 | Kericho | Kipkelion East | 25638 | 47 |
6 | Kericho | Sigowet/Soin | 26724 | 49 |
Sub total | 89484 | 164 |
Total | | 495 |
2.5.3. Pre-testing
Pre-test study was conducted using 50 youth in Machakos County that formed 10% of the sample size. Data was collected from 25 youth in a randomly selected sample of 3 youth groups and 25 young people from two Colleges or technical institutes in Machakos County. Data was collected through use of detailed questionnaire, structured interviews and some use of direct observation. The pretest county is medium incidence and was characteristically similar to participant counties. Pre-testing of instruments was also intended to improve clarity, precision, reliability and validity of data. Following analysis of the pretest study data, ambiguous or unclear questions were either be rephrased or removed.
2.5.4. Validity
The questionnaire was comprehensive enough to collect all the information needed to address the purpose and objectives of the study. A field test was conducted before the questionnaire was used for the pilot study. To test validity, the questionnaire was also reviewed by an expert at Kenyatta University. Data from other sources was compared with results from this study. The findings from this study can be generalized for the effect comprehensive HIV prevention information package on risk sexual behavior among youth in Kenya.
2.5.5. Reliability
Pretesting the questionnaire helped enhance reliability of the instrument. The Research Assistants were trained on administering the research instruments. Reliability was established using a pilot test by collecting data from subjects not included in the sample. The same questionnaire was used during the interviews and all its subparts were measured using the same characteristic. To increase reliability of data collected, efforts for triangulation was undertaken including performing two separate interviews per county in addition to direct observation made
.
2.6. Intervention
The comprehensive HIV prevention information package was provided to the youth in the intervention county after the baseline assessment. The HIV prevention information package had 3 contact sessions offered termly for 9 months. Each contact session was 3 hours long consisting of presentation, experience sharing, group discussion and practical demonstration. The package consisted of frequently asked questions on HIV and AIDS, overview of HIV including transmission and prevention options, condom use dialogue, key HIV and STIs messages and documentary. Two local peer facilitators were trained on the comprehensive HIV Prevention information package to facilitate termly sessions with the youth. The out of school youth were meeting at the county Youth Empowerment center every last Saturday of the month to receive the intervention. Youthful HIV testing counselors from partner organizations were referred to the youth empowerment center to offer the service. Youth in the comparison county continued to receive routine HIV services offered at health facilities.
2.7. Data Collection
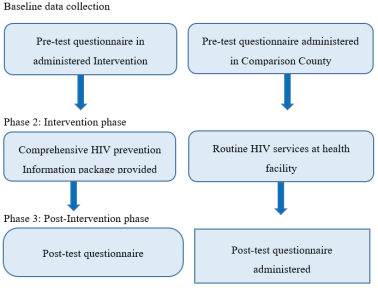
The quantitative data was collected from respondents at baseline and at endline after 9 months by using a self-administered questionnaire which had both structured and unstructured questions. The questionnaire was constructed through literature review and consultation with subject experts at the University. Four key informant interviews were also conducted with program implementers to establish HIV prevention strategies available for young people. Six Focus Group Discussions with 8-10 youth were conducted for the qualitative study at baseline and at endline. A similar questionnaire was administered at baseline and end line period in both intervention and comparison counties. The questionnaire also collected information on potential confounding factors such as age, gender, residence and other prevention programs that they had attended. The post test data was collected 9 months after implementing the comprehensive HIV prevention information package as shown in
Figure 1 below. Data was checked for completeness and internal consistency throughout the data collection period. The questionnaire together with participants’ responses was then coded and entered into a computer for analysis.
Figure 1. Intervention Flow Chart.
2.7.1. Data Collection Process
The quantitative data collection method involved individual interviews using pretested structured questionnaire that was well designed as per the research objectives. All respondents signed consent and assent form before participating in the study. Eligible participants who declined to participate were not coerced. The data collection process took 7 days at baseline and at endline in both intervention and comparison county. Each interview took an average of 45 minutes. The endline data was collected after 9 months of providing HIV Prevention information package to youth in the intervention county while youth in comparison county continued to receive routine health services. The researcher and research assistants analyzed the interview data and checked for inconsistencies and clarification.
The qualitative data was collected by conducting individual indepth interviews and focus group discussions. The researcher conducted 4 Key informant interview guides with key youth program implementers and 6 focus group discussions with youths per county. Participants for the qualitative study were purposefully selected based on their experience in the research study. After explaining the study objectives and obtaining consent from respondents, the researcher requested permission to record and take notes during the session. Participants were assured of confidentiality and the information provided will be strictly used for the study. Participants were asked to respect each other’s opinion since there was no wrong response during the session. The researcher moderated the one hour discussion with participants while the research assistant took notes. The researcher finally thanked participants for their time.
2.7.2. Data Analysis
The qualitative data was transcribed and translated then entered into NVivo qualitative data software for coding and thematic analysis. The quantitative data was entered into SPSS and analyzed using descriptive statistics. These include mean, median, frequencies and standard deviation. The Difference-In-Difference (DID) regression model was used to compare outcomes between intervention and comparison county at baseline and after 9 months of the intervention at end line. A Chi square test was used to determine the effect of the comprehensive HIV prevention information package and testing for any significant difference. Potential confounders were measured at baseline and end line and analysis and the results adjusted for possible confounders using logistic regression to ensure unbiased estimation of the intervention effect.
2.8. Ethical Considerations
Research proposal was approved by Kenyatta University Ethical Review Committee as No. PKU/2302/11441 before start of the study. The research permit was obtained from NACOSTI. Kakamega and Kericho counties gave clearance to collect data from colleges and youth groups. Written informed consent was obtained from all the study participants. Parental permission for adolescents aged 15-17 years was sought first before the minor’s assent was sought. No participant name appeared on the questionnaire. Participants were informed that there will be no penalties for declining to participate or for withdrawing from the study in the course of data collection and that no invasive procedures will be used. Access to database was restricted by password. Completed questionnaires were kept in lockable office.
3. Results
3.1. Demographic Information of the Sampled Population
A total of 495 respondents from Kericho and Kakamega were involved in this study with 100% response rate. Most of the respondents were from Kakamega (66.7%) based on the proportionate sample size. Both male and female young adults in the ages of 15 - 24 years were involved. Majority of the respondents 61.2% were in their tertiary education level and only 10.7% were married as summarized in
Table 2.
Table 2. Respondents’ demographic information.
Demographic information | Category | At Baseline (N = 495) | End line (N = 495) |
County | Kericho | 164 (33.1%) | 164 (33.1%) |
Kakamega | 331 (66.9%) | 331 (66.9%) |
Gender | Male | 233 (47.1%) | 233 (47.1%) |
Female | 262 (52.9%) | 262 (52.9%) |
Age (Years) | 15 - 19 | 185 (373.6%) | 183 (37.0%) |
20 - 24 | 306 (61.8%) | 312 (63.0%) |
Non-response | 3 (0.6%) | - |
Education level | None | 10 (2.0%) | 10 (2.0%) |
Primary | 58 (11.7%) | 26 (5.3%) |
Secondary | 113 (22.8%) | 95 (19.2%) |
Tertiary | 303 (61.2%) | 355 (71.7%) |
Non -response | 11 (2.2%) | 10 (2.0%) |
Religion | Christians | 456 (92.1%) | 466 (94.1%) |
Muslims | 32 (6.5%) | 26 (5.3%) |
Others | 3 (0.6%) | 2 (0.4%) |
Non-response | 4 (0.8%) | 1 (0.2%) |
Marital status | Married | 53 (10.7%) | 57 (11.5%) |
Single | 400 (80.8%) | 414 (83.6%) |
*Others | 34 (6.9%) | 21 (4.2%) |
Non-response | 8 (1.6%) | 3 (0.6%) |
3.2. HIV Prevention Strategies Utilized by the Youth
During the baseline survey, more youth from Kakamega utilized HIV prevention services compared to those youth in Kericho. However, using independent t -test, there was no significant difference in usage of Information on HIV transmission (P = 0.444) and no significant difference in HIV testing services (HTS) with active reference to lifelong ART for HIV- positive (P = 0.135). These results changed after the intervention where there was a significant positive difference in all the test items on HIV prevention services utilized at endline in Kakamega than Kericho due to exposure to comprehensive HIV prevention information package that empowered them to utilize HIV services (P < 0.05).
Table 3. Comparison of HIV prevention services utilized at baseline and at end of study.
HIV Preventive services | Proportional responses (%) |
Baseline | Endline |
Kericho (n = 164) | Kakamega (n = 331) | P- value | Kericho | Kakamega | P-value |
HIV information | 98 (59.8) | 217 (65.6) | 0.444 | 93 (56.7) | 321 (96.9) | 0.011* |
HIV testing services | 22 (13.4) | 64 (19.3) | 0.135 | 28 (17.1) | 218 (65.9) | 0.0001* |
PrEP | 5 (3.0) | 28 (8.5) | 0.028 | 10 (6.1) | 28 (8.5) | 0.0001* |
Post violence care | 6 (3.6) | 29 (8.8) | 0.045 | 8 (4.9) | 18 (5.4) | 0.0001* |
Enrollment to ART | 4 (2.4) | 24 (7.3) | 0.034 | 7 (4.3) | 15 (4.5) | 0.0001* |
PMTCT for pregnant AGYW | 7 (4.3) | 33 (9.9) | 0.035 | 9 (5.5) | 23 (6.9) | 0.0001* |
Condom promotion | 22 (13.4) | 70 (21.1) | 0.052 | 29 (17.7) | 104 (31.4) | 0.0001* |
VMMC | 11 (6.7) | 59 (17.8) | 0.001 | 12 (7.3) | 49 (14.8) | 0.0001* |
STI screening and treatment | 15 (9.1) | 35 (10.6) | 0.694 | 18 (10.9) | 49 (14.8) | 0.0001* |
Prevention &reatment of TB | 12 (7.3) | 44 (13.3) | 0.054 | 11 (6.7) | 32 (9.7) | 0.0001* |
Other prevention strategies | 1 (2.1) | 7 (2.1) | - | 4 (2.4) | 9 (2.7) | 0.0001* |
3.3. HIV Prevention Strategies the Youth Plan to Use in Future
At the endline, a comparison of the two counties on HIV services youths plan to utilize in future showed that there was a significant difference in use of strategies during the baseline and after the intervention (P < 0.05). More youth were willing to; use condom promotion and distribution, negotiation skills and facilitated access; Information on HIV transmission, abstinence, consistent and correct condom; willing to go for HIV testing services (HTS) with active referrals to lifelong ART for HIV positive; VMMC, PrEP, PMTCT, get STI screening and treatment; ready for prevention, diagnostics and treatment of Tuberculosis (TB). Results of the focus group discussion with the youths indicated that the HIV prevention services available to them and their peersare being faithful to a sexual partner, HIV self-testing, Screening of blood before transfusion, Correct and consistent Condom use, Abstinence, PrEP, PEP and health education.
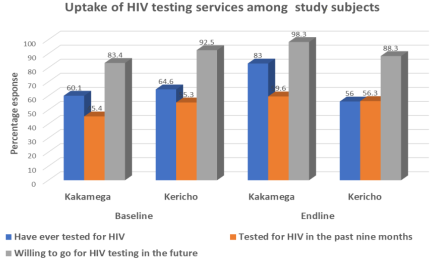
3.4. HIV Testing Services Uptake
In Kakamega, the percentage of youth who had been examined for HIV in the end of the survey increased from 60.1% to 83.0%) and the youth who were willing to go for HIV testing in the future after survey significantly increased from 83.4% to 98.3% (t = 6.547, df = 2, p = 0.023). This was due to the intervention package that included key messages on HIV testing and the importance of knowing HIV status.
The findings from FGDs indicated that the main reasons youth don’t test for HIV is fear of the HIV testing outcomes due to lifelong drug burden. Other reasons the youth gave was exposure through unprotected sex, multiple partnerships and to protect the breastfeeding baby. The youth fear being ssuspected as high risk by health worker when go for HIV testing. The youth also mentioned shortage of HIV Testing Services providers and unavailability of HIV testing kits in health facilities.
Figure 2. Youths uptake of HIV testing services in the two counties.
3.5. Use of Condoms by the Youth in the Last 9 Months
In the last nine months at the time of baseline study, most of the youths (34.9%) used condoms more than three times. Merely 26.1% of the youths used condoms only once. At the end of survey, more youth (47.1%) used condoms more than three times in the last nine months whereas 21.8% used them once as shown in
Table 4.Table 4. Use of condoms by the respondents in the last 9 months.
| Proportional responses (%) |
Frequency of condom use | During baseline | At endline | r value | P value |
Once | 129 (26.1) | 108 (21.8) | | |
Twice | 47 (9.5) | 58 (11.7) | | |
Three times | 60 (12.1) | 65 (13.1) | | |
More than three times | 173 (34.9) | 233 (47.1) | | |
Non - response | 86 (17.4) | 31 (6.3) | 0.877 | 0.051 |
() Represents% proportional responses
3.6. Reasons for Failure to Use Condoms
During their last sex, at the baseline, 18.0% of the youths failed to use condoms mainly because they trusted the partner and 14.9% because it does not make sex enjoyable. Other reasons given were; Condom not available, not safe, the partner objected the use condom. At the end line, trusting the sexual partner was main reason the youth did not use condoms. Other reasons why the youth did not use condoms at endline include condoms are too expensive, condoms not available, condoms do not make sex enjoyable, partner objected, use other contraceptives, condoms not safe and did not think it was necessary to use condoms.
3.7. Plans to Use Condoms
More youths (87.1%) in Kakamega than those in Kericho county (43.0%) plan to use condoms in the near future. Using chi square statistics, the finding showed a χ2 of 100.236, P = 0.0001 showing a significant difference in Kakamega youth to Kericho youth plan to use condoms in future. During focus group discussions and key informant interviews, the youths recommended introduction of condom pick up points or condom dispensing machines in tertiary institutions.
4. Discussion
Comparison of HIV prevention services utilized at baseline and at endline in both counties indicated that there was a significant difference in all the HIV preventive services utilized by the youth in the intervention county (P < 0.05). There was also significant difference in the HIV prevention services the youth will be willing to utilize in future. This was due to the comprehensive HIV prevention package that empowered the youth in the intervention county on the importance of utilizing HIV services. This concurs with an evaluation of the Impact of the adolescent and youth sexual and reproductive health strategy on service utilization and health outcomes in Zimbabwe
| [16] | Muchabaiwa L and Mbonigaba J: Impact of the adolescent and youth sexual and reproductive health strategy on service utilisation and health outcomes in. PLoS Zimbabwe ONE 14(6): e0218588, 2019. https://doi.org/10.1371/journal.pone.0218588 |
[16]
that increased HIV testing, STIs screening and treatment in the intervention group. The national HIV prevention education program increased uptake of HIV prevention services among men who have sex with men and transgender women in Thailand
| [17] | Jommaroeng R, Richter KA, Chamratrithirong A and Soonthorndhada A: "The effectiveness of national HIV prevention education program on behavioral changes for men who have sex with men and transgender women in Thailand", Journal of Health Research, Vol. 34 No. 1, pp. 2-12, 2018. https://doi.org/10.1108/JHR-12- 2018-0163 |
[17]
. The predisposing factors (socio-demographic and HIV knowledge) and the need-for-care factors (sexual risk behaviors) predict healthcare utilization services (HIV testing)
.
Uptake of HIV testing services increased by 23% in the intervention county compared to comparison county where there was marginal decrease from a baseline of 58.4%
| [18] | Khasewa J, Mwanzo I and Orago A: Risky sexual behaviour and associated factors among youth in Kakamega and Kericho counties, Kenya, African Journal of Health Sciences, Vol. 36 No. 1. https://doi.org/10.4314/ajhs.v36i1.8 2023. |
[18]
. The Key messages on HIV testing influenced the youths in the intervention county to get tested for HIV. This concurs with a 3-week smartphone-based pilot HIV prevention intervention consisting of short videos and text messages that significantly increased intentions to undergo HIV testing post-intervention
| [19] | Chakrapani V, Kumar P, Kaur J. Shunmugam M and Mukherjee D: A Smartphone- Based Pilot HIV Prevention Intervention (Sakhi) among Transgender Women Who Engage in Sex Work in India: Efficacy of a Pre- and Post- Test Quasi-ExperimentalTrial, Venereology 2023, 2(1), 30-42; https://doi.org/10.3390/venereology2010003 |
[19]
. A similar study on effectiveness of national HIV prevention education program on behavioral changes for men who have sex with men and transgender women in Thailand was successful in increasing uptake of HIV testing services
| [17] | Jommaroeng R, Richter KA, Chamratrithirong A and Soonthorndhada A: "The effectiveness of national HIV prevention education program on behavioral changes for men who have sex with men and transgender women in Thailand", Journal of Health Research, Vol. 34 No. 1, pp. 2-12, 2018. https://doi.org/10.1108/JHR-12- 2018-0163 |
[17]
. Targeted interventions to help youth correctly assess their level of risk and to increase awareness of the potential value of HIV testing may help enhance uptake of testing services
| [6] | Kabiru CW, Beguy D, Crichton J and Zulu ME: HIV/AIDS among youth in urban informal (slum) settlements in Kenya: What are the correlates of and motivations for HIV testing?. BMC Public Health 11, 685, 2011. https://doi.org/10.1186/1471-2458-11-685 |
[6]
.
Condom use was higher in the intervention county than comparison county at endline. Similarly, there was a significant difference in percentage of youth in intervention county to comparison county who plan to use condoms in future (χ
2 = 100.236, P = 0.0001). This was due to condom advocacy and dialoque sessions that addressed misconceptions and improved condom use skills among youth in the intervention county. This concurs with a peer education intervention in selected schools Northern Malawi that resulted in increasing condom use and lowering multiple sexual partnerships in the intervention after 8 months
| [20] | Mwale M and Muula SA: The efficacy of peer education in sexual behavioral change among school-going adolescents in Northern Malawi: A quasi experiment, Journal of HIV/AIDS & Social Services, 18: 3, 229247, 2019, https://doi.org/10.1080/15381501.2019.1620664 |
[20]
. A similar cross sectional -quantitative study that was conducted to assess the impact of comprehensive HIV prevention interventions on the sexual behavior of oil and gas workers in Bonny Island, Nigeria succeeded in tripling condom use among respondents after the intervention
| [21] | Onoja AJ, Sanni FO, Abiodun PO: Sexual Behaviours among Oil and Gas Workers in the Niger-Delta Region of Nigeria: Assessing the Impact of Comprehensive HIV/AIDS Prevention Programs. International Journal of Occupational Safety and Health, 2021, 11(2), 80-88. https://doi.org/10.3126/ijosh.v11i2.36371 |
[21]
. In addition to existing social marketing campaigns, tailored approaches should focus on establishing the perceived need for condom-use and improving skills for correct use
| [9] | Chandran TM, Berkvens D, Chikobvu P, Nöstlinger C, Colebunders R, Williams GB and Speybroeck N: Predictors of condom use and refusal among the population of Free State province in South Africa. BMC Public Health 12, 381(2012). https://doi.org/10.1186/1471-2458-12-381 |
[9]
.
5. Recommendations
1. Review the minimum package for young people in the Fast Track plan to include Frequently asked questions on HIV and AIDS and key HIV testing messages.
2. Utilize existing infrastructure and delivery platforms for national roll-out of the comprehensive HIV prevention package.
3. Expand condom promotion campaigns to include condom advocacy and dialogues.
6. Conclusions
The comprehensive HIV prevention information package was successful in increasing utilization of combination HIV prevention strategies. The key HIV message increased uptake of HIV testing services. The condom advocacy and dialogue forums increased condom uptake among the youth in the intervention county.
Abbreviations
AIDS | Acquired Immune Deficiency Virus |
AYP | Adolescent and Young People |
DID | Difference-in-difference |
FGD | Focus Group Discussions |
HIV | Human Immunodeficiency Virus |
HTS | HIV Testing Services |
ICF | Inner City Fund |
KDHS | Kenya Demographic and Health Survey |
KII | Key Informant Interview |
NACOSTI | National Commission for Science, Echnology and Innovations |
UNAIDS | Joint United Nations Programme on AIDS |
SPSS | Statistical Package for Social Sciences |
STI | Sexually Transmitted Infection |
TVET | Technical and Vocational Education and Training |
Acknowledgments
Authors wish to acknowledge Dr Chrispinus Wamalwa and Peter Cheruiyot for permission to conduct the research in TVET Colleges in Kakamega and Kericho counties. We appreciate the support of TVET Principals and the youths who agreed to participate in the study. Thanks to Lawrence Alaro, Joseph Wanyonyi, Aggrey Indeje, Sylvia Dianga, Catherine Washira, Abdi Swaleh Geoffrey Kigen, Sylvia Chepngetich, George Dianga and Cyphrene Wasike for their assistance throughout this study. The support of the research Assistants Fatuma Maalim, Gideon Korir, Josephat Marumbu and Damaris Momanyi cannot be overemphasized.
Finally, my special thanks go to Leon and Fleming for staying with me until very late at night as I worked on this.
Author Contributions
Joab Khasewa: Conceptualization, methodology, formal analysis, investigation, Writing - original draft
Isaac Mwanzo: Supervision, methodology, data curation, validation, Writing - review & editing
Alloys Orago: Supervision, methodology, data curation, validation, Writing - review & editing
Funding
This research was funded by (Royal Society of Tropical Medicine and Hygiene (RSTMH) small grants programme.
Data Availability Statement
Data available upon writing to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
UNAIDS. HIV Estimates. Joint United Nations Programme on HIV/AIDS, 2022.
|
| [2] |
ICF. The DHS Program, ICF International, 2018. Retrieved From
https://www.dhsprogram.com/
|
| [3] |
MOH. Kenya HIV Estimates Report. National AIDS Control Counci, 2022.
|
| [4] |
MOH. Kenya Demographic and Health survey Kenya National Bureau of Statistics, 2022.
|
| [5] |
KNBS. Kenya Population and Housing Census. Kenya National Bureau of Statistics, 2022. Available from
www.knbs.or.ke
|
| [6] |
Kabiru CW, Beguy D, Crichton J and Zulu ME: HIV/AIDS among youth in urban informal (slum) settlements in Kenya: What are the correlates of and motivations for HIV testing?. BMC Public Health 11, 685, 2011.
https://doi.org/10.1186/1471-2458-11-685
|
| [7] |
Sonko I, Chung MH, Hou WH, Chen WT and Chang P C: Predictors of HIV testing among youth aged 15-24 years in The Gambia. PLoS One. 2022 Feb 18; 17(2): e0263720.
https://doi.org/10.1371/journal.pone.0263720
|
| [8] |
Patrão AL and McIntyre T: Socio-demographic, marital and psychosocial predictors of safe sex behaviour among Mozambican women at risk for HIV/AIDS. African Journal of AIDS Research, 17(4), 323-331, 2018.
https://doi.org/10.2989/16085906.2018.1536672
|
| [9] |
Chandran TM, Berkvens D, Chikobvu P, Nöstlinger C, Colebunders R, Williams GB and Speybroeck N: Predictors of condom use and refusal among the population of Free State province in South Africa. BMC Public Health 12, 381(2012).
https://doi.org/10.1186/1471-2458-12-381
|
| [10] |
Campbell DT and Stanley J: Experimental and Quasi-Experimental Designs for Research. Houghton Mifflin, 1966. Boston, USA.
|
| [11] |
Suresh KP and Chandrashekara S: Sample Size Estimation and Power Analysis for Clinical Research Studies. Journal of Human Reproductive Science, 2012; 5, 7-13.
|
| [12] |
MOH. Kenya Demographic and Health survey. KenyaNational Bureau of Statistics, 2014.
|
| [13] |
Israel GD: Sampling The Evidence Of Extension Program Impact. IFAS, 1992. University of Florida.
|
| [14] |
Cochran WG: Sampling Techniques, 2nd Ed. John Wiley and Sons Inc 1963. New York, USA;
https://doi.org/10.1002/bimj.19650070312
|
| [15] |
Khasewa J, Keraka M and Ayugi J: Barriers to utilization of provider initiated HIV counseling and testing services among TB patients; a case of Rhodes Chest Clinic, Nairobi, Kenya, 2011.
https://ir-library.ku.ac.ke/items/73c6a455-bdfb-47f3-aabb-667861fd5d04
|
| [16] |
Muchabaiwa L and Mbonigaba J: Impact of the adolescent and youth sexual and reproductive health strategy on service utilisation and health outcomes in. PLoS Zimbabwe ONE 14(6): e0218588, 2019.
https://doi.org/10.1371/journal.pone.0218588
|
| [17] |
Jommaroeng R, Richter KA, Chamratrithirong A and Soonthorndhada A: "The effectiveness of national HIV prevention education program on behavioral changes for men who have sex with men and transgender women in Thailand", Journal of Health Research, Vol. 34 No. 1, pp. 2-12, 2018.
https://doi.org/10.1108/JHR-12- 2018-0163
|
| [18] |
Khasewa J, Mwanzo I and Orago A: Risky sexual behaviour and associated factors among youth in Kakamega and Kericho counties, Kenya, African Journal of Health Sciences, Vol. 36 No. 1.
https://doi.org/10.4314/ajhs.v36i1.8
2023.
|
| [19] |
Chakrapani V, Kumar P, Kaur J. Shunmugam M and Mukherjee D: A Smartphone- Based Pilot HIV Prevention Intervention (Sakhi) among Transgender Women Who Engage in Sex Work in India: Efficacy of a Pre- and Post- Test Quasi-ExperimentalTrial, Venereology 2023, 2(1), 30-42;
https://doi.org/10.3390/venereology2010003
|
| [20] |
Mwale M and Muula SA: The efficacy of peer education in sexual behavioral change among school-going adolescents in Northern Malawi: A quasi experiment, Journal of HIV/AIDS & Social Services, 18: 3, 229247, 2019,
https://doi.org/10.1080/15381501.2019.1620664
|
| [21] |
Onoja AJ, Sanni FO, Abiodun PO: Sexual Behaviours among Oil and Gas Workers in the Niger-Delta Region of Nigeria: Assessing the Impact of Comprehensive HIV/AIDS Prevention Programs. International Journal of Occupational Safety and Health, 2021, 11(2), 80-88.
https://doi.org/10.3126/ijosh.v11i2.36371
|
Cite This Article
-
APA Style
Khasewa, J., Mwanzo, I., Orago, A. (2025). Effect of Comprehensive HIV Prevention Information Package on Uptake of HIV Services Among Youth In Kenya: A Non- randomized Trial. Central African Journal of Public Health, 11(4), 192-200. https://doi.org/10.11648/j.cajph.20251104.15
 Copy
|
Copy
|
 Download
Download
ACS Style
Khasewa, J.; Mwanzo, I.; Orago, A. Effect of Comprehensive HIV Prevention Information Package on Uptake of HIV Services Among Youth In Kenya: A Non- randomized Trial. Cent. Afr. J. Public Health 2025, 11(4), 192-200. doi: 10.11648/j.cajph.20251104.15
Copy
|
Download
AMA Style
Khasewa J, Mwanzo I, Orago A. Effect of Comprehensive HIV Prevention Information Package on Uptake of HIV Services Among Youth In Kenya: A Non- randomized Trial. Cent Afr J Public Health. 2025;11(4):192-200. doi: 10.11648/j.cajph.20251104.15
Copy
|
Download
-
@article{10.11648/j.cajph.20251104.15,
author = {Joab Khasewa and Isaac Mwanzo and Alloys Orago},
title = {Effect of Comprehensive HIV Prevention Information Package on Uptake of HIV Services Among Youth In Kenya: A Non- randomized Trial
},
journal = {Central African Journal of Public Health},
volume = {11},
number = {4},
pages = {192-200},
doi = {10.11648/j.cajph.20251104.15},
url = {https://doi.org/10.11648/j.cajph.20251104.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cajph.20251104.15},
abstract = {HIV remains the most significant public health and development challenge in the world. Youth in sub-Saharan Africa are primarily affected by the HIV epidemic. Despite the availability of HIV prevention options, new infections among youth in Kenya only reduced by 56% between 2015 and 2021. Various HIV prevention interventions have been implemented among youth with little or no assessment of their effects on risky sexual behavior. The objective of the study was to investigate effect of comprehensive HIV prevention information package on uptake of HIV prevention services among youth in Kenya. A non-randomized control trial was conducted with Kakamega and Kericho as intervention and Comparison County respectively. The pretest questionnaire was administered in December 2021. The posttest questionnaire was administered after nine months of providing HIV prevention information package. Quantitative data was analyzed using chi square and t-test. Qualitative data was transcribed and analyzed thematically. The youth significantly utilized HIV prevention services (83.6%) and information on, abstinence, consistent and correct condom use (t = 12.248, df=2, p = 0.0001). The intervention significantly increased utilization of HIV testing services from 60.1% to 83.0% (t = 6.547, df = 2, p = 0.023). There was a significant difference in number of youths in Kakamega than Kericho who plan to use condoms in future (χ2 = 100.236, P = 0.0001). The comprehensive HIV prevention information package increased uptake of HIV services. The findings will inform national rollout of the intervention to contribute to safer sexual behaviors among youth.},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Effect of Comprehensive HIV Prevention Information Package on Uptake of HIV Services Among Youth In Kenya: A Non- randomized Trial
AU - Joab Khasewa
AU - Isaac Mwanzo
AU - Alloys Orago
Y1 - 2025/07/24
PY - 2025
N1 - https://doi.org/10.11648/j.cajph.20251104.15
DO - 10.11648/j.cajph.20251104.15
T2 - Central African Journal of Public Health
JF - Central African Journal of Public Health
JO - Central African Journal of Public Health
SP - 192
EP - 200
PB - Science Publishing Group
SN - 2575-5781
UR - https://doi.org/10.11648/j.cajph.20251104.15
AB - HIV remains the most significant public health and development challenge in the world. Youth in sub-Saharan Africa are primarily affected by the HIV epidemic. Despite the availability of HIV prevention options, new infections among youth in Kenya only reduced by 56% between 2015 and 2021. Various HIV prevention interventions have been implemented among youth with little or no assessment of their effects on risky sexual behavior. The objective of the study was to investigate effect of comprehensive HIV prevention information package on uptake of HIV prevention services among youth in Kenya. A non-randomized control trial was conducted with Kakamega and Kericho as intervention and Comparison County respectively. The pretest questionnaire was administered in December 2021. The posttest questionnaire was administered after nine months of providing HIV prevention information package. Quantitative data was analyzed using chi square and t-test. Qualitative data was transcribed and analyzed thematically. The youth significantly utilized HIV prevention services (83.6%) and information on, abstinence, consistent and correct condom use (t = 12.248, df=2, p = 0.0001). The intervention significantly increased utilization of HIV testing services from 60.1% to 83.0% (t = 6.547, df = 2, p = 0.023). There was a significant difference in number of youths in Kakamega than Kericho who plan to use condoms in future (χ2 = 100.236, P = 0.0001). The comprehensive HIV prevention information package increased uptake of HIV services. The findings will inform national rollout of the intervention to contribute to safer sexual behaviors among youth.
VL - 11
IS - 4
ER -
Copy
|
Download