Introduction: Erectile dysfunction (ED) refers to inability to achieve and sustain erection sufficient for satisfactory penetrative sexual experience. Lower Urinary Tract Symptoms (LUTS) includes storage, voiding and post-micturition symptoms due to bladder outlet obstruction. LUTS may be a risk factor for ED. Objectively, international prostate symptoms score (IPSS) is an essential tool for assessing the bothersome nature of lower urinary tract symptoms while the abridged version of international index of erectile function (IIEF-5) is objectively useful in assessing ED. This study is focused on establishing the relationship between severity of ED and IPSS in patients with bladder outlet obstruction (BOO) caused by prostate enlargement. Methodology: By simple random sampling, patients presenting in clinic with bladder outlet obstruction not due to urethral stricture were evaluated for ED. Two questionnaires (IIEF-5 and IPSS) and a specially designed proforma were administered to all the patients who met the criteria for inclusion. The questionnaires objectively evaluated the ED and severity of LUTS respectively. The data obtained were analyzed using Statistical Package for Social Sciences (SPSS) version 21.0. P-value of < 0.05 was seen as statistically significant. Results: One hundred and seventeen male patients with bladder outlet obstruction were enrolled in this study. Ninety patients (77%) varying severity of IIEF-5 score while twenty-seven patients (23%) normal IIEF-5 score. Mean age of patients with severe IIEF-5 score was 64 while the mean age of patients with moderate IIEF-5 score, mild to moderate IIEF-5 score, mild IIEF-5 score and normal IIEF-5 score were 64, 65, 60 and 58 respectively. Over seventy one percent (71.4%) of patients between 41-50 years had varying degree of ED based on IIEF-5 score. 65% of patients between the age range of 51-60 abnormal IIEF-5 score while 89% and 94% of patients between the age range of 61-70 and 71-80 respectively varying degree of ED. Patients with severe IIEF-5 score had the highest mean IPSS of 23 while patients with normal IIEF-5 score had the lowest mean IPSS. The P-value (0.21) was not significant. Conclusion: This study shows that IIEF-5/ED has a direct relationship with IPSS. There was a positive link between ED/IIEF-5 and IPSS/LUTS. This may also be part of the rationale for administering low dose tadalafil to improve sexual performance in patients with bladder outlet obstruction.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Erectile dysfunction (ED) refers to inability to achieve and maintain erection sufficient for satisfactory penetrative sexual experience
[1]
Hatzimouratidis K, Amar E, Eardley I, Giuliano F, Hatzichristou D, Montorsi F, Vardi Y, Wespes E; European Association of Urology. Guidelines on male sexual dysfunction: erectile dysfunction and premature ejaculation. Eur Urol. 2010 May; 57(5): 804-14.
. Normal erectile function remains a vital aspect of human existence and has a negative impact on quality of life (QoL) and performance.Prevalence of ED increases with age
[1]
Hatzimouratidis K, Amar E, Eardley I, Giuliano F, Hatzichristou D, Montorsi F, Vardi Y, Wespes E; European Association of Urology. Guidelines on male sexual dysfunction: erectile dysfunction and premature ejaculation. Eur Urol. 2010 May; 57(5): 804-14.
. Several studies observed a progressive prevalence of ED as a man ages
[1]
Hatzimouratidis K, Amar E, Eardley I, Giuliano F, Hatzichristou D, Montorsi F, Vardi Y, Wespes E; European Association of Urology. Guidelines on male sexual dysfunction: erectile dysfunction and premature ejaculation. Eur Urol. 2010 May; 57(5): 804-14.
Morant S, Bloomfield G, Vats V, Chapple C. Increased sexual dysfunction in men with storage and voiding lower urinary tract symptoms. J Sex Med. 2009 Apr; 6(4): 1103-1110.
. ED affects marital harmony and is a significant cause of crisis. Most medical management are basically for palliation and can have serious side effect. The medical therapy sometimes used in the management of bladder outlet obstruction (BOO) also affect sexual function
[4]
Klotz T, Mathers MJ, Braun M, Bloch W, Engelmann U. Effectiveness of oral L-arginine in first-line treatment of erectile dysfunction in a controlled crossover study. Urol Int. 1999; 63(4): 220-3.
International prostate symptom score (IPSS) is a tool that evaluates the severity of lower urinary tract symptoms (LUTS) caused by prostate enlargement. National Institute of Health and Clinical Excellence guidelines classified lower urinary tract symptoms as consisting of storage, voiding and post-micturition symptoms. This symptoms basically affects the urinary tract in patients who suffers from bladder outlet obstruction
[5]
NICE clinical guidelines 97. Lower urinary tract symptoms. Management of lower urinary tract symptoms in men.
. Post-micturition dribbling majorly suggests urethral disease which is not part of the parameters assessed by IPSS
[6]
Kenenna Obiatuegwu, Terkaa Atim, Sadiq Abu et al. Correlation between the Severity of Erectile Dysfunction and Prostate Size in Patients with Benign Prostatic Enlargement. Afr J Urol 27, 31 (2021),
. IPSS is a self-administered, valid and reliable tool for assessing the LUTS caused by prostate enlargement. It comprises of 4 voiding and 3 storage items. The voiding symptoms are incomplete emptying, intermittency, weak stream and straining. The storage symptoms are frequency, urgency and nocturia. Each symptom is score from 0-5 giving a minimum total score of 0 and maximum total score of 35 points.A total symptom score of 0-7 is mild, 8-19 is moderate and 20-35 is severe
[6]
Kenenna Obiatuegwu, Terkaa Atim, Sadiq Abu et al. Correlation between the Severity of Erectile Dysfunction and Prostate Size in Patients with Benign Prostatic Enlargement. Afr J Urol 27, 31 (2021),
Yeboah E. D. The Prostate Gland. In: Badoe E. A, Archampong E. Q, J. T Da Rocha-Afodu: Principles and Practice of Surgery Including Pathology in the Tropics. Ch. 47, 4th edition: Assemblies of God Literature Center Ltd, 2009; 920-924.
[6, 7]
. Quality of life (QoL) responses ranges from ‘delighted’ ‘pleased’, ‘mostly satisfied’, ‘mixed (both equally satisfied and dissatisfied’, ‘mostly dissatisfied’, ‘unhappy’, ‘terrible’. It is scored from 0 to 6
[8]
Thomas A. M, Roger S. K, Herbert L. Evaluation and Nonsurgical Management of Benign Prostatic Hyperplasia. In: Campbell-Walsh Urology, Louis R. K, Alan W. P, Andrew C. N and Craig A. P. Ch. 92, 10th edition: Elsevier Saunder, 2012; 2611-2654.
[8]
. IIEF-5 is an abridged validated questionnaire used in ascertaining the severity of ED. Parameters assessed includes erectile function, orgasmic function, sexual desire, intercourse satisfaction and overall satisfaction. Score ranges from severe (5-7), moderate (8-11), mild to moderate (12-16), mild (17-21), and no ED (22-25)
[9]
Rosen RC. Evaluation of the patient with erectile dysfunction: history, questionnaires, and physical examination. Endocrine. 2004 Mar-Apr; 23(2-3): 107-11.
Bladder outlet obstruction present with storage and voiding LUTS which may impact on sexual function and performance
[10]
Kirby M, Chapple C, Jackson G, Eardley I, Edwards D, Hackett G, Ralph D, Rees J, Speakman M, Spinks J, Wylie K. Erectile dysfunction and lower urinary tract symptoms: a consensus on the importance of co-diagnosis. Int J Clin Pract. 2013 Jul; 67(7): 606-18.
. Ikuerowo et al observed a positive link between ED and IPSS probably due to the voiding lower urinary symptoms with a prevalence rate of ED at over 70%
[12]
Ikuerowo SO, Akindiji YO, Akinoso OA, Akinlusi FM, Esho JO. Association between erectile dysfunction and lower urinary tract symptoms due to benign prostatic hyperplasia in Nigerian men. Urol Int. 2008; 80(3): 296-9.
.Tadanafil administered in low doses may be useful and possibly counter the adverse effect of 5 alpha reductase inhibitors like dutasteride and finasteride considering that ED is one of the major side effect reported with the used of these drugs
[6]
Kenenna Obiatuegwu, Terkaa Atim, Sadiq Abu et al. Correlation between the Severity of Erectile Dysfunction and Prostate Size in Patients with Benign Prostatic Enlargement. Afr J Urol 27, 31 (2021),
. Worsening voiding lower urinary tract symptoms due BOO/prostate enlargement is seen as the possible cause of ED in men above 40
[13]
Glina S, Santana A. W, Azank F et al. Lower urinary tract symptoms and erectile dysfunction are highly prevalent in ageing men. BJU Int. 2006; 97(4): 763-765.
Nasir A. R, Zehn A. A, Abbas F et al. The correction between International Prostate Symptom Score and sexual health inventory in men with lower urinary tract symptoms. Int. Urol. Nephrol. 2001; 43(3): 625-629.
[13, 14]
.
This study is focused in establishing the link between the ED assessed with IIEF-5 and lower urinary tract symptoms assessed with IPSS in patients with bladder outlet obstruction. Perhaps the outcome may support other studies that observed similar trend/positive link between ED and BOO.
2. Methodology
This was a prospective study. Patients with storage and voiding LUTS were randomly recruited and assessed for the presence of ED. IPSS and IIEF-5 were used to objectively determine the symptom severity and those that fulfilled the enrolling criteria were included in the study.
2.1. Inclusion Criteria
1) Male patients with bladder outlet obstruction presenting with lower urinary tract symptoms.
2) All consenting patients.
2.2. Exclusion Criteria
1) Male patients with other causes of lower urinary tract symptoms like locally advanced prostate malignancy and urethral stricture.
2) Male patients with neurogenic bladder and risk factors.
3) Male patients with chronic back pain.
4) Male patients on medications that affect erectile function including psycho-tropics, anti-androgens, hypoglycemic drugs and anti-hypertensives.
5) Male patients with history of major pelvic injury including pelvic fracture urethral distraction defect.
6) Male patients on urethral catheter.
Patients with BOO who fulfilled the enrolling criteria were included in the study. We obtained an informed consent and approval for the study were obtained from the ethical committee of the hospital. Two globally recognized questionnaires (IPSS and IIEF-5) were used to objectively evaluate the bothersome nature LUTS and severity of ED. A proforma was specifically designed to record the biodata as well as other relevant information.
Completely filled questionnaires/proforma were collated and data obtained were analyzed using Statistical Package for the Social Sciences (SPSS) version 21.0 and p-values < 0.05 was referred to be statistically relevant. Statistical tools including chi square and student’s paired T test were employed to compare outcome appropriately. Relationship between IIEF-5 and IPSS was compared using the Pearson’s correlation. Results are represented in charts and tables.
3. Results
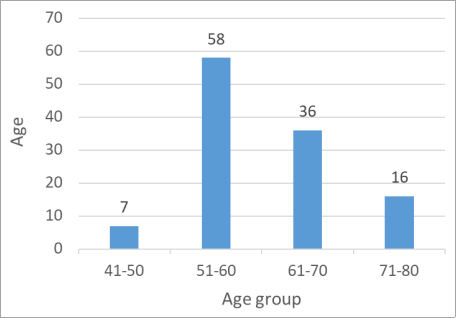
One hundred and seventeen patients with bladder outlet obstruction were recruited in this study. The patients were between 43 to 75 years with majority of the patient falling between the age ranges of 51-70. Only 7 patients were below 50 years as shown in figure 1.
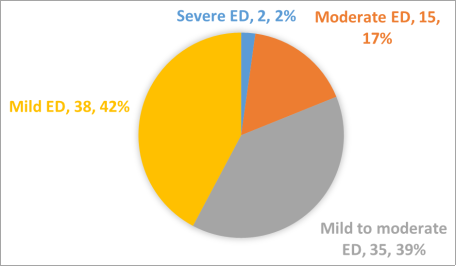
Ninety patients (77%) had varying degree of ED/IIEF-5 while 23% had normal IIEF-5 score. Amongst the 90 patients that abnormal IIEF-5 score, 2.2% had severe IIEF-5 score, 17% had moderate IIEF-5 score, 39% had mild to moderate ED/IIEF-5 score while 42% observed mild ED/IIEF-5 score as shown in figure 2.
Figure 2. Distribution of Patients with ED based on IIEF-5 score.
Mean age of patients with severe IIEF-5 score was 64 ± 7.07 and that of moderate IIEF-5 score, mild to moderate IIEF-5 score, mild IIEF-5 score and normal IIEF-5 score were 64, 64.62, 60 and 58 respectively. The comparison between the severity of IIEF-5 and mean age is as represented in table 1.
Table 1. Mean age versus severity of IIEF-5.
IIEF-5 score
Frequency
Mean age
Standard deviation
Severe
2
64
7.07
Moderate
15
64
7.26
Mild to moderate
35
64
7.40
Mild
38
60
7.05
Normal
27
58
5.16
P value = 0.01
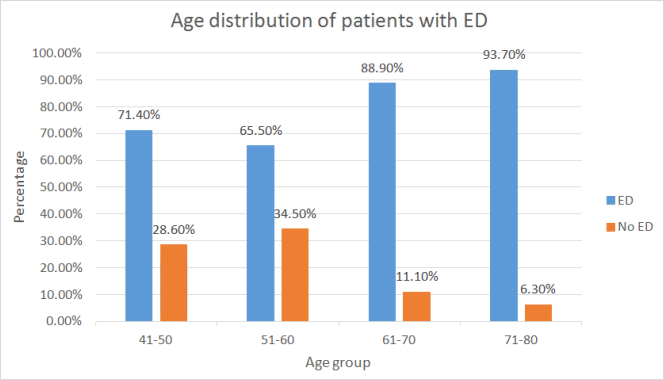
The patients who had normal IIEF-5 score were between 54-60 years. Seven patients were between 41-50 years and over seventy percent (71.4%) had ED. 65.5% of patients between 51-60 years had abnormal IIEF-5 score while 88.9% and 93.7% of patients between 61-70 and 71-80 years respectively had abnormal IIEF-5 as depicted in figure 3 below.
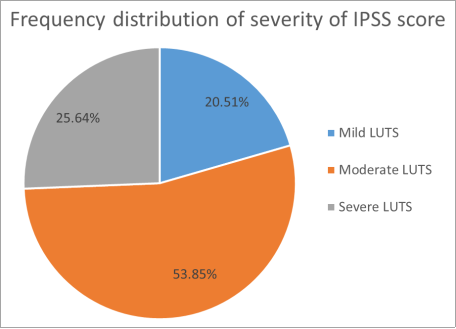
Figure 4. Frequency distribution of the severity of LUTS.
Severity of IIEF-5 was compared with the severity of IPSS. Patients with severe IIEF-5 score had a higher mean IPSS of 23 while patients with normal IIEF-5 score had the lowest mean IPSS of 13 as shown in table 2. The P-value was 0.21.
Table 2. Correlation between IIEF-5 and mean IPSS.
IIEF-5 score
Frequency
Mean IPSS score
Standard deviation
Severe
2
23
12.73
Moderate
15
18
9.20
Mild to moderate
35
15
7.46
Mild
38
14.
7.08
Normal
27
13
8.05
P -value = 0.21.
4. Discussion
Erectile dysfunction (ED) is the persistent inability to achieve and maintain erection sufficient for satisfactory penetrative sexual experience
[1]
Hatzimouratidis K, Amar E, Eardley I, Giuliano F, Hatzichristou D, Montorsi F, Vardi Y, Wespes E; European Association of Urology. Guidelines on male sexual dysfunction: erectile dysfunction and premature ejaculation. Eur Urol. 2010 May; 57(5): 804-14.
. Sexual health is an aspect of human existence that has significant impacts on quality of life (QoL)
[6]
Kenenna Obiatuegwu, Terkaa Atim, Sadiq Abu et al. Correlation between the Severity of Erectile Dysfunction and Prostate Size in Patients with Benign Prostatic Enlargement. Afr J Urol 27, 31 (2021),
. Prevalence of erectile dysfunction is age dependent. Several studies observed a higher prevalence rate in males greater than 70 years compared to younger adults
[2]
Rosen RC, Giuliano F, Carson CC. Sexual dysfunction and lower urinary tract symptoms (LUTS) associated with benign prostatic hyperplasia (BPH). Eur Urol. 2005 Jun; 47(6): 824-37.
Morant S, Bloomfield G, Vats V, Chapple C. Increased sexual dysfunction in men with storage and voiding lower urinary tract symptoms. J Sex Med. 2009 Apr; 6(4): 1103-1110.
. This is in keeping with our observation which showed a progressive trend in the prevalence of ED with increasing age. We also observed a high prevalence of ED in this study. This increased prevalence observed in our study may be due to concomitant existence of BOO as we excluded all other risk of ED prior to enrolling the patients. The age range of the patients in our study was 43-75 years with majority falling between 51-70 years. While we acknowledge that there may still be other factors responsible for the ED observed in this age group which we inadvertently did not exclude, we excluded documented likely risk factors of ED amongst this age group like hypertension, diabetes mellitus etc.
[6]
Kenenna Obiatuegwu, Terkaa Atim, Sadiq Abu et al. Correlation between the Severity of Erectile Dysfunction and Prostate Size in Patients with Benign Prostatic Enlargement. Afr J Urol 27, 31 (2021),
. More so, the increase in the severity of ED observed with aging in this study was statistically significant (P value of 0.001) as noted in several studies
[2]
Rosen RC, Giuliano F, Carson CC. Sexual dysfunction and lower urinary tract symptoms (LUTS) associated with benign prostatic hyperplasia (BPH). Eur Urol. 2005 Jun; 47(6): 824-37.
Morant S, Bloomfield G, Vats V, Chapple C. Increased sexual dysfunction in men with storage and voiding lower urinary tract symptoms. J Sex Med. 2009 Apr; 6(4): 1103-1110.
Kenenna Obiatuegwu, Terkaa Atim, Sadiq Abu et al. Correlation between the Severity of Erectile Dysfunction and Prostate Size in Patients with Benign Prostatic Enlargement. Afr J Urol 27, 31 (2021),
Ikuerowo SO, Akindiji YO, Akinoso OA, Akinlusi FM, Esho JO. Association between erectile dysfunction and lower urinary tract symptoms due to benign prostatic hyperplasia in Nigerian men. Urol Int. 2008; 80(3): 296-9.
Nasir A. R, Zehn A. A, Abbas F et al. The correction between International Prostate Symptom Score and sexual health inventory in men with lower urinary tract symptoms. Int. Urol. Nephrol. 2001; 43(3): 625-629.
[2, 3, 6, 12, 14]
.
BOO is a common clinical presentation observed in older men above 50 years
[13]
Glina S, Santana A. W, Azank F et al. Lower urinary tract symptoms and erectile dysfunction are highly prevalent in ageing men. BJU Int. 2006; 97(4): 763-765.
Ponholzer A, Temml C, Obermayr R, Madersbacher S. Association between lower urinary tract symptoms and erectile dysfunction. Urology. 2004 Oct; 64(4): 772-6.
. This group of adults commonly report varying forms and severity of sexual dysfunction particularly ED prompting possible link between ED and LUTS/IPSS. Obiatuegwu et al reported a direct relationship between the severity of ED and prostate volume with 76.9% of men with BOO due to symptomatic BPE experiencing diverse severity of ED and displeased with their QoL and sexual performance. This is also in keeping with our findings which observed that men with BOO and moderate/severe IPSS experienced significant progressive severity of ED. This study is not focused on the specific etiology of BOO such as BPE as reported by Obiatuegwu et al as we only considered the general relationship between ED and the severity of IPSS irrespective of the etiology
[1]
Hatzimouratidis K, Amar E, Eardley I, Giuliano F, Hatzichristou D, Montorsi F, Vardi Y, Wespes E; European Association of Urology. Guidelines on male sexual dysfunction: erectile dysfunction and premature ejaculation. Eur Urol. 2010 May; 57(5): 804-14.
Sak et al noted a causative link between BOO/LUTS and sexual dysfunction
[16]
Sak SC, Hussain Z, Johnston C, Eardley I: What is the relationship between male sexual function and lower urinary tract symptoms?Eur Urol 200 4; 46: 482–487.
. This index study observed an exponential relationship between the severity of ED assessed using IIEF-5 and the severity of BOO/LUTS assessed with IPSS. We noted that the severity of ED worsened as the IPSS progressed exponentially with patients with severe IPSS ≥ 20 had the worst sexual experience compared with patient with mild IPSS. This further confirms a direct correlation between the severity of ED and IPSS.
Kirby et al reported LUTS as a strong indicator of ED with an odd ratio for erection problems of 8.90 (95.0%)
[10]
Kirby M, Chapple C, Jackson G, Eardley I, Edwards D, Hackett G, Ralph D, Rees J, Speakman M, Spinks J, Wylie K. Erectile dysfunction and lower urinary tract symptoms: a consensus on the importance of co-diagnosis. Int J Clin Pract. 2013 Jul; 67(7): 606-18.
.Other studies also noted that men with moderate (IPSS= 8-19) or severe (IPSS ≥20) LUTS increased every 10 years with commensurate decline in erectile function
[11]
Schiff JD, Mulhall JP. The link between LUTS and ED: clinical and basic science evidence. J Androl. 2004 Jul-Aug; 25(4): 470-8.
Nasir A. R, Zehn A. A, Abbas F et al. The correction between International Prostate Symptom Score and sexual health inventory in men with lower urinary tract symptoms. Int. Urol. Nephrol. 2001; 43(3): 625-629.
[11, 14]
. This is in keeping with our observation that found a direct relationship between ED, IPSS and aging. Ikuerowo et al also reported a positive link between ED and BPE/LUTS probably due to the voiding lower urinary symptoms from prostate enlargement with a very high prevalence of ED as IPSS worsened
[12]
Ikuerowo SO, Akindiji YO, Akinoso OA, Akinlusi FM, Esho JO. Association between erectile dysfunction and lower urinary tract symptoms due to benign prostatic hyperplasia in Nigerian men. Urol Int. 2008; 80(3): 296-9.
. While we observed similar trend, our study was not focused on any specific category of lower urinary symptoms responsible for the decline in sexual function. However, we noted worsening ED in patients with worsening IPSS.
ED has been observed by many studies to have a direct relationship with IPSS
[6]
Kenenna Obiatuegwu, Terkaa Atim, Sadiq Abu et al. Correlation between the Severity of Erectile Dysfunction and Prostate Size in Patients with Benign Prostatic Enlargement. Afr J Urol 27, 31 (2021),
Ikuerowo SO, Akindiji YO, Akinoso OA, Akinlusi FM, Esho JO. Association between erectile dysfunction and lower urinary tract symptoms due to benign prostatic hyperplasia in Nigerian men. Urol Int. 2008; 80(3): 296-9.
. We noted that patients with severe ED had a higher mean IPSS of 23 while patients with no ED had the lowest mean IPSS of 13. This findings are in keeping with several studies showing significant link between IPSS and erectile dysfunction in older men globally
[17]
Rosen R, Altwein J, Boyle P, Kirby RS, Lukacs B, Meuleman E, O'Leary MP, Puppo P, Robertson C, Giuliano F. Lower urinary tract symptoms and male sexual dysfunction: the multinational survey of the aging male (MSAM-7). Eur Urol. 2003 Dec; 44(6): 637-49.
. Sexual function and LUTS may be affected by changes in smooth muscle tone as seen in patients with BOO/LUTS due to BPE. The growth of these tissues around the transitional zone of the prostate may cause a mechanical obstruction with consequent increased urethral resistance and with worsening IPSS. This may have contributed to the direct link between the severity of IIEF-5 score and IPSS observed in our study
[12]
Ikuerowo SO, Akindiji YO, Akinoso OA, Akinlusi FM, Esho JO. Association between erectile dysfunction and lower urinary tract symptoms due to benign prostatic hyperplasia in Nigerian men. Urol Int. 2008; 80(3): 296-9.
Nasir A. R, Zehn A. A, Abbas F et al. The correction between International Prostate Symptom Score and sexual health inventory in men with lower urinary tract symptoms. Int. Urol. Nephrol. 2001; 43(3): 625-629.
[12, 14]
.
Preservation and restoration of sexual function cannot be over emphasized in the management of patients with bothersome lower urinary tract symptoms
[6]
Kenenna Obiatuegwu, Terkaa Atim, Sadiq Abu et al. Correlation between the Severity of Erectile Dysfunction and Prostate Size in Patients with Benign Prostatic Enlargement. Afr J Urol 27, 31 (2021),
. This was clearly observed in our study as the prevalence of ED increased in men with moderate and severe IPSS which translates to bothersome LUTS. The QoL of the patients in these category may improve on low dose tadanafil. Sexual and urinary functions has a direct impact on QoL and varies in different patients. A patient with severe IPSS may be satisfied with his sexual function and performance while another patient with mild IPSS may experience the worse erectile function
[6]
Kenenna Obiatuegwu, Terkaa Atim, Sadiq Abu et al. Correlation between the Severity of Erectile Dysfunction and Prostate Size in Patients with Benign Prostatic Enlargement. Afr J Urol 27, 31 (2021),
This study confirms a direct relationship between ED and the severity of LUTS/IPSS. There was a direct link between ED and IPSS. The exact nature of this relationship and the specific LUTS responsible for decline in sexual function will require a more comprehensive study to identify. Administering daily low dose tadalafil may improve the QoL and sexual performance in patients with bothersome LUTS.
6. Limitation
Our small sample size may not be a true representation of facts. More research on severity of IIEF-5 and IPSS with a larger sample size and involving multiple centers will further strengthen our verdict.
Abbreviations
ED
Erectile Dysfunction
BPE
Benign Prostatic Enlargement
LUTS
Lower Urinary Tract Symptoms
IPSS
International Prostate Symptoms Score
IIEF-5
International Index of Erectile Function
QoL
Quality of Life
SPSS
Statistical Package for the Social Sciences
Ethical Clearance
Ethical clearance was obtained from the hospital ethical committee.
Funding
This article was funded by the authors.
Data Availability Statement
All data are in the archive of the hospital record department and readily accessible.
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
Hatzimouratidis K, Amar E, Eardley I, Giuliano F, Hatzichristou D, Montorsi F, Vardi Y, Wespes E; European Association of Urology. Guidelines on male sexual dysfunction: erectile dysfunction and premature ejaculation. Eur Urol. 2010 May; 57(5): 804-14.
Morant S, Bloomfield G, Vats V, Chapple C. Increased sexual dysfunction in men with storage and voiding lower urinary tract symptoms. J Sex Med. 2009 Apr; 6(4): 1103-1110.
Klotz T, Mathers MJ, Braun M, Bloch W, Engelmann U. Effectiveness of oral L-arginine in first-line treatment of erectile dysfunction in a controlled crossover study. Urol Int. 1999; 63(4): 220-3.
Kenenna Obiatuegwu, Terkaa Atim, Sadiq Abu et al. Correlation between the Severity of Erectile Dysfunction and Prostate Size in Patients with Benign Prostatic Enlargement. Afr J Urol 27, 31 (2021),
Yeboah E. D. The Prostate Gland. In: Badoe E. A, Archampong E. Q, J. T Da Rocha-Afodu: Principles and Practice of Surgery Including Pathology in the Tropics. Ch. 47, 4th edition: Assemblies of God Literature Center Ltd, 2009; 920-924.
[8]
Thomas A. M, Roger S. K, Herbert L. Evaluation and Nonsurgical Management of Benign Prostatic Hyperplasia. In: Campbell-Walsh Urology, Louis R. K, Alan W. P, Andrew C. N and Craig A. P. Ch. 92, 10th edition: Elsevier Saunder, 2012; 2611-2654.
[9]
Rosen RC. Evaluation of the patient with erectile dysfunction: history, questionnaires, and physical examination. Endocrine. 2004 Mar-Apr; 23(2-3): 107-11.
Kirby M, Chapple C, Jackson G, Eardley I, Edwards D, Hackett G, Ralph D, Rees J, Speakman M, Spinks J, Wylie K. Erectile dysfunction and lower urinary tract symptoms: a consensus on the importance of co-diagnosis. Int J Clin Pract. 2013 Jul; 67(7): 606-18.
Ikuerowo SO, Akindiji YO, Akinoso OA, Akinlusi FM, Esho JO. Association between erectile dysfunction and lower urinary tract symptoms due to benign prostatic hyperplasia in Nigerian men. Urol Int. 2008; 80(3): 296-9.
Glina S, Santana A. W, Azank F et al. Lower urinary tract symptoms and erectile dysfunction are highly prevalent in ageing men. BJU Int. 2006; 97(4): 763-765.
Nasir A. R, Zehn A. A, Abbas F et al. The correction between International Prostate Symptom Score and sexual health inventory in men with lower urinary tract symptoms. Int. Urol. Nephrol. 2001; 43(3): 625-629.
[15]
Ponholzer A, Temml C, Obermayr R, Madersbacher S. Association between lower urinary tract symptoms and erectile dysfunction. Urology. 2004 Oct; 64(4): 772-6.
Sak SC, Hussain Z, Johnston C, Eardley I: What is the relationship between male sexual function and lower urinary tract symptoms?Eur Urol 200 4; 46: 482–487.
Rosen R, Altwein J, Boyle P, Kirby RS, Lukacs B, Meuleman E, O'Leary MP, Puppo P, Robertson C, Giuliano F. Lower urinary tract symptoms and male sexual dysfunction: the multinational survey of the aging male (MSAM-7). Eur Urol. 2003 Dec; 44(6): 637-49.
Kenenna, O., Felix, M., Ernest, A., Vivian, M. (2025). Relationship Between Erectile Dysfunction and International Prostate Symptom Score. Clinical Medicine Research, 14(5), 181-186. https://doi.org/10.11648/j.cmr.20251405.13
Kenenna, O.; Felix, M.; Ernest, A.; Vivian, M. Relationship Between Erectile Dysfunction and International Prostate Symptom Score. Clin. Med. Res.2025, 14(5), 181-186. doi: 10.11648/j.cmr.20251405.13
Kenenna O, Felix M, Ernest A, Vivian M. Relationship Between Erectile Dysfunction and International Prostate Symptom Score. Clin Med Res. 2025;14(5):181-186. doi: 10.11648/j.cmr.20251405.13
@article{10.11648/j.cmr.20251405.13,
author = {Obiatuegwu Kenenna and Magnus Felix and Aniede Ernest and Magnus Vivian},
title = {Relationship Between Erectile Dysfunction and International Prostate Symptom Score
},
journal = {Clinical Medicine Research},
volume = {14},
number = {5},
pages = {181-186},
doi = {10.11648/j.cmr.20251405.13},
url = {https://doi.org/10.11648/j.cmr.20251405.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cmr.20251405.13},
abstract = {Introduction: Erectile dysfunction (ED) refers to inability to achieve and sustain erection sufficient for satisfactory penetrative sexual experience. Lower Urinary Tract Symptoms (LUTS) includes storage, voiding and post-micturition symptoms due to bladder outlet obstruction. LUTS may be a risk factor for ED. Objectively, international prostate symptoms score (IPSS) is an essential tool for assessing the bothersome nature of lower urinary tract symptoms while the abridged version of international index of erectile function (IIEF-5) is objectively useful in assessing ED. This study is focused on establishing the relationship between severity of ED and IPSS in patients with bladder outlet obstruction (BOO) caused by prostate enlargement. Methodology: By simple random sampling, patients presenting in clinic with bladder outlet obstruction not due to urethral stricture were evaluated for ED. Two questionnaires (IIEF-5 and IPSS) and a specially designed proforma were administered to all the patients who met the criteria for inclusion. The questionnaires objectively evaluated the ED and severity of LUTS respectively. The data obtained were analyzed using Statistical Package for Social Sciences (SPSS) version 21.0. P-value of Results: One hundred and seventeen male patients with bladder outlet obstruction were enrolled in this study. Ninety patients (77%) varying severity of IIEF-5 score while twenty-seven patients (23%) normal IIEF-5 score. Mean age of patients with severe IIEF-5 score was 64 while the mean age of patients with moderate IIEF-5 score, mild to moderate IIEF-5 score, mild IIEF-5 score and normal IIEF-5 score were 64, 65, 60 and 58 respectively. Over seventy one percent (71.4%) of patients between 41-50 years had varying degree of ED based on IIEF-5 score. 65% of patients between the age range of 51-60 abnormal IIEF-5 score while 89% and 94% of patients between the age range of 61-70 and 71-80 respectively varying degree of ED. Patients with severe IIEF-5 score had the highest mean IPSS of 23 while patients with normal IIEF-5 score had the lowest mean IPSS. The P-value (0.21) was not significant. Conclusion: This study shows that IIEF-5/ED has a direct relationship with IPSS. There was a positive link between ED/IIEF-5 and IPSS/LUTS. This may also be part of the rationale for administering low dose tadalafil to improve sexual performance in patients with bladder outlet obstruction.
},
year = {2025}
}
TY - JOUR
T1 - Relationship Between Erectile Dysfunction and International Prostate Symptom Score
AU - Obiatuegwu Kenenna
AU - Magnus Felix
AU - Aniede Ernest
AU - Magnus Vivian
Y1 - 2025/09/26
PY - 2025
N1 - https://doi.org/10.11648/j.cmr.20251405.13
DO - 10.11648/j.cmr.20251405.13
T2 - Clinical Medicine Research
JF - Clinical Medicine Research
JO - Clinical Medicine Research
SP - 181
EP - 186
PB - Science Publishing Group
SN - 2326-9057
UR - https://doi.org/10.11648/j.cmr.20251405.13
AB - Introduction: Erectile dysfunction (ED) refers to inability to achieve and sustain erection sufficient for satisfactory penetrative sexual experience. Lower Urinary Tract Symptoms (LUTS) includes storage, voiding and post-micturition symptoms due to bladder outlet obstruction. LUTS may be a risk factor for ED. Objectively, international prostate symptoms score (IPSS) is an essential tool for assessing the bothersome nature of lower urinary tract symptoms while the abridged version of international index of erectile function (IIEF-5) is objectively useful in assessing ED. This study is focused on establishing the relationship between severity of ED and IPSS in patients with bladder outlet obstruction (BOO) caused by prostate enlargement. Methodology: By simple random sampling, patients presenting in clinic with bladder outlet obstruction not due to urethral stricture were evaluated for ED. Two questionnaires (IIEF-5 and IPSS) and a specially designed proforma were administered to all the patients who met the criteria for inclusion. The questionnaires objectively evaluated the ED and severity of LUTS respectively. The data obtained were analyzed using Statistical Package for Social Sciences (SPSS) version 21.0. P-value of Results: One hundred and seventeen male patients with bladder outlet obstruction were enrolled in this study. Ninety patients (77%) varying severity of IIEF-5 score while twenty-seven patients (23%) normal IIEF-5 score. Mean age of patients with severe IIEF-5 score was 64 while the mean age of patients with moderate IIEF-5 score, mild to moderate IIEF-5 score, mild IIEF-5 score and normal IIEF-5 score were 64, 65, 60 and 58 respectively. Over seventy one percent (71.4%) of patients between 41-50 years had varying degree of ED based on IIEF-5 score. 65% of patients between the age range of 51-60 abnormal IIEF-5 score while 89% and 94% of patients between the age range of 61-70 and 71-80 respectively varying degree of ED. Patients with severe IIEF-5 score had the highest mean IPSS of 23 while patients with normal IIEF-5 score had the lowest mean IPSS. The P-value (0.21) was not significant. Conclusion: This study shows that IIEF-5/ED has a direct relationship with IPSS. There was a positive link between ED/IIEF-5 and IPSS/LUTS. This may also be part of the rationale for administering low dose tadalafil to improve sexual performance in patients with bladder outlet obstruction.
VL - 14
IS - 5
ER -
Kenenna, O., Felix, M., Ernest, A., Vivian, M. (2025). Relationship Between Erectile Dysfunction and International Prostate Symptom Score. Clinical Medicine Research, 14(5), 181-186. https://doi.org/10.11648/j.cmr.20251405.13
Kenenna, O.; Felix, M.; Ernest, A.; Vivian, M. Relationship Between Erectile Dysfunction and International Prostate Symptom Score. Clin. Med. Res.2025, 14(5), 181-186. doi: 10.11648/j.cmr.20251405.13
Kenenna O, Felix M, Ernest A, Vivian M. Relationship Between Erectile Dysfunction and International Prostate Symptom Score. Clin Med Res. 2025;14(5):181-186. doi: 10.11648/j.cmr.20251405.13
@article{10.11648/j.cmr.20251405.13,
author = {Obiatuegwu Kenenna and Magnus Felix and Aniede Ernest and Magnus Vivian},
title = {Relationship Between Erectile Dysfunction and International Prostate Symptom Score
},
journal = {Clinical Medicine Research},
volume = {14},
number = {5},
pages = {181-186},
doi = {10.11648/j.cmr.20251405.13},
url = {https://doi.org/10.11648/j.cmr.20251405.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cmr.20251405.13},
abstract = {Introduction: Erectile dysfunction (ED) refers to inability to achieve and sustain erection sufficient for satisfactory penetrative sexual experience. Lower Urinary Tract Symptoms (LUTS) includes storage, voiding and post-micturition symptoms due to bladder outlet obstruction. LUTS may be a risk factor for ED. Objectively, international prostate symptoms score (IPSS) is an essential tool for assessing the bothersome nature of lower urinary tract symptoms while the abridged version of international index of erectile function (IIEF-5) is objectively useful in assessing ED. This study is focused on establishing the relationship between severity of ED and IPSS in patients with bladder outlet obstruction (BOO) caused by prostate enlargement. Methodology: By simple random sampling, patients presenting in clinic with bladder outlet obstruction not due to urethral stricture were evaluated for ED. Two questionnaires (IIEF-5 and IPSS) and a specially designed proforma were administered to all the patients who met the criteria for inclusion. The questionnaires objectively evaluated the ED and severity of LUTS respectively. The data obtained were analyzed using Statistical Package for Social Sciences (SPSS) version 21.0. P-value of Results: One hundred and seventeen male patients with bladder outlet obstruction were enrolled in this study. Ninety patients (77%) varying severity of IIEF-5 score while twenty-seven patients (23%) normal IIEF-5 score. Mean age of patients with severe IIEF-5 score was 64 while the mean age of patients with moderate IIEF-5 score, mild to moderate IIEF-5 score, mild IIEF-5 score and normal IIEF-5 score were 64, 65, 60 and 58 respectively. Over seventy one percent (71.4%) of patients between 41-50 years had varying degree of ED based on IIEF-5 score. 65% of patients between the age range of 51-60 abnormal IIEF-5 score while 89% and 94% of patients between the age range of 61-70 and 71-80 respectively varying degree of ED. Patients with severe IIEF-5 score had the highest mean IPSS of 23 while patients with normal IIEF-5 score had the lowest mean IPSS. The P-value (0.21) was not significant. Conclusion: This study shows that IIEF-5/ED has a direct relationship with IPSS. There was a positive link between ED/IIEF-5 and IPSS/LUTS. This may also be part of the rationale for administering low dose tadalafil to improve sexual performance in patients with bladder outlet obstruction.
},
year = {2025}
}
TY - JOUR
T1 - Relationship Between Erectile Dysfunction and International Prostate Symptom Score
AU - Obiatuegwu Kenenna
AU - Magnus Felix
AU - Aniede Ernest
AU - Magnus Vivian
Y1 - 2025/09/26
PY - 2025
N1 - https://doi.org/10.11648/j.cmr.20251405.13
DO - 10.11648/j.cmr.20251405.13
T2 - Clinical Medicine Research
JF - Clinical Medicine Research
JO - Clinical Medicine Research
SP - 181
EP - 186
PB - Science Publishing Group
SN - 2326-9057
UR - https://doi.org/10.11648/j.cmr.20251405.13
AB - Introduction: Erectile dysfunction (ED) refers to inability to achieve and sustain erection sufficient for satisfactory penetrative sexual experience. Lower Urinary Tract Symptoms (LUTS) includes storage, voiding and post-micturition symptoms due to bladder outlet obstruction. LUTS may be a risk factor for ED. Objectively, international prostate symptoms score (IPSS) is an essential tool for assessing the bothersome nature of lower urinary tract symptoms while the abridged version of international index of erectile function (IIEF-5) is objectively useful in assessing ED. This study is focused on establishing the relationship between severity of ED and IPSS in patients with bladder outlet obstruction (BOO) caused by prostate enlargement. Methodology: By simple random sampling, patients presenting in clinic with bladder outlet obstruction not due to urethral stricture were evaluated for ED. Two questionnaires (IIEF-5 and IPSS) and a specially designed proforma were administered to all the patients who met the criteria for inclusion. The questionnaires objectively evaluated the ED and severity of LUTS respectively. The data obtained were analyzed using Statistical Package for Social Sciences (SPSS) version 21.0. P-value of Results: One hundred and seventeen male patients with bladder outlet obstruction were enrolled in this study. Ninety patients (77%) varying severity of IIEF-5 score while twenty-seven patients (23%) normal IIEF-5 score. Mean age of patients with severe IIEF-5 score was 64 while the mean age of patients with moderate IIEF-5 score, mild to moderate IIEF-5 score, mild IIEF-5 score and normal IIEF-5 score were 64, 65, 60 and 58 respectively. Over seventy one percent (71.4%) of patients between 41-50 years had varying degree of ED based on IIEF-5 score. 65% of patients between the age range of 51-60 abnormal IIEF-5 score while 89% and 94% of patients between the age range of 61-70 and 71-80 respectively varying degree of ED. Patients with severe IIEF-5 score had the highest mean IPSS of 23 while patients with normal IIEF-5 score had the lowest mean IPSS. The P-value (0.21) was not significant. Conclusion: This study shows that IIEF-5/ED has a direct relationship with IPSS. There was a positive link between ED/IIEF-5 and IPSS/LUTS. This may also be part of the rationale for administering low dose tadalafil to improve sexual performance in patients with bladder outlet obstruction.
VL - 14
IS - 5
ER -