Angiofibroma is a benign but very aggressive tumor due to its tendency for local invasion. It is composed of myofibroblasts and vasogenic elements, making it a highly vascularized tumor. The oropharyngeal angiofibroma is an atypical angiofibroma in terms of location and symptoms. The general objective of our study was to examine the diagnostic and therapeutic characteristics of an angiofibroma with an exceptional location at the base of the tongue through a case observation accompanied by a literature review. This involves a 13-year-old patient who consulted for solid dysphagia. The onset would date back to 2 years after his admission, marked by the progressive installation of a ronchopathy associated with a feeling of a foreign body in the throat, and firm rhinophonia. This clinical picture prompted traditional treatments based on fumigations, which were unsuccessful. The evolution was marked after 3 months by the addition of solid dysphagia and dyspnea in the supine position. Faced with this clinical picture, they decided to consult us for management. The physical examination revealed a budding mass at the base of the tongue with vascular hyperemia that is mobile during tongue prostration and swallowing, with contact and palpation showing no bleeding or pulsation. A nasofibroscopy objectively showed a submucosal lesion budding at the base of the tongue, mobile during swallowing, extending towards the posterior pharyngeal wall and narrowing the oropharyngeal canal. A computed tomography scan with contrast injection suggested a hyperdense tissue mass, well-circumscribed, developing at the expense of the base of the tongue with significant obstruction of the oropharyngeal tract. The histopathological examination of the operative sample after complete transoral surgical excision under general anesthesia was in favor of an angiofibroma rearranged from the base of the language. The patient was lost to follow-up for 2 years due to financial difficulties as all the medical expenses were borne by the patient without any assistance or health insurance.
| Published in | Clinical Medicine Research (Volume 14, Issue 5) |
| DOI | 10.11648/j.cmr.20251405.14 |
| Page(s) | 187-193 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Angiofibroma, Tumor, Benign, Oropharynx, Mali
PATHOLOGIES | Clinics | TDM | Histology | References |
|---|---|---|---|---|
Angiofibroma | Dysphagia, severe dyspnea, firm rhinolalia, bronchopathy, and miscarriages, An emerging mass at the base of the tongue, hyperemic, vascular, mobile, without bleeding or pulsation. | A hyperdensity of tissue at the expense of the base of the tongue, with regular contours and significant obstruction of the oropharyngeal pathway. | The examined samples were the site of a proliferation consisting of vascular septa associated with a fascicular proliferation of fibroblasts. In some places, the tumor is infiltrated with lymphoplasmacytes. | Our article |
Cysts | Snoring, without true dyspnea, a rounded, firm regular swelling forming a bulge covered with normal mucosa. | Median mass syndrome coming into contact with the hyoid bone, a liquid density and a capsule. | Cystic cavity bordered by a richly vascularized fibrous wall containing slightly eosinophilic hematic serosity punctuated by inflammatory elements and histiocytes. | Guerina; N. [23] |
Lipomas | Lipomas generally appear deep in the soft tissues, rarely located under the mucosa; a yellowish color is visible through the stretched mucosa, which also contains some telangiectasias. | A negative fat density with sharp, generally homogeneous contours and without contrast uptake. | Presents adipose cells. With a few exceptions, they are surrounded by a fibrous capsule, or they are at least clearly delineated from the surrounding tissue, on which they generally rest with a wide non-pedunculated (sessile) base. | Bassetti, R., and al. [24] |
Fibrous tumor | Dysarthria, dysphonia, dysphagia, bleeding and/or diagnosis may be present, with a well-defined, rounded, smooth, pale submucosal nodular mass. | Shows a hypodense area in the center and an increased fixation of the CT at the periphery. | Numerous thin-walled vessels often made of deer antler associated with a proliferation of spindle-shaped cells with hypercellular and hypocellular areas. | Betsalel, AD. [25] |
AF | Angiofibroma |
JNA | Juvenile Nasopharyngeal Angiofibroma |
ENA | Extra-nasopharyngeal Angiofibroma |
ATCD | Medical History |
MRI | Magnetic Resonance Imaging |
CT | Computed Tomography |
WHO | World Health Organization |
| [1] | Euswas, C. A result of sublabial transnasomaxillary approach to nasopharyngeal angiofibroma: a retrospective study. J Med Assoc Thai. 1999, 82: 234-41. |
| [2] | Celik, B., Erisen, L., Saraydaroglu, O., Coskun, H. Atypical angiofibromas: report of four cases. Int J Pediatric Otorhinolaryngol. 2005; 69: 415-421. |
| [3] | Butugan, O. Angiofibroma Juvenil - Aspectos Atuais Terapêuticos. À Brandão LG, Ferraz AR. Cirurgie de Cabeça et Pescoço. Brésil: Editora Roca. 1989; 2: 415-20. |
| [4] | Luiz, AC., Ricardo., RSL Tiago., AS, Fava. Nasopharyngeal angiofibroma: literature review. Revista Brasileira de Otorrinolaryngologia-English edition. 2003; 69: 394 to 403. |
| [5] | Macri, A., Tanner, LS. Cutaneous Angiofibroma. Stat Pearls; Treasure Island: StatPearls Publishing; 2020. disponible PubMed Jan-PMID: 35015466. |
| [6] | Ahmad, MD., Ramesh, R., Bestoun, H. Endoscopic Surgery of juvenile angiofibroma: First published online Asian Journal of surgery. January 10, 2017 Chapter pp 131–145. |
| [7] | Neel HB 3rd, Whicker JH, Devine KD, Weiland LH. Juvenile angiofibroma. Review of 120 cases. Am J Surg. 1973; 126: 547–56. |
| [8] | Sivanandan, R., Fee, WE. Tumeurs bénignes et malignes du nasopharynx. Dans: Cummings CW, Flint PW, Harker LA, et al. Éditeurs. Cummings otolaryngology head and neck surgery, ed 4. Philadelphie: Elsevier Mosby; 2005; 1669-84. |
| [9] | Liu, ZF., Wang, DH., Sun, XC., Wang, JJ., Hu, L., Dal, PD. The site of origin and expansion pathways of juvenile nasopharyngeal angiofibroma (JNA). Int. J Pediatr Otorhinolaryngol. 2011; 75(9): 1088-92. |
| [10] | Beeden, AG., Alexandre, FW. An unusual pharyngeal tumor. J Laryngol Otol. 1971; 85: 733-735. |
| [11] | Ganakalyan, B., Vikas, G µ1., Utkal, P. M., Ashwani, T. Extra nasopharyngeal angiofibroma from oropharynx: clinic report. Affiliations Developer. |
| [12] | Lloyd, G., Howard, D., Phelps, P., Cheesman, A. Angiofibrome juvénile: les leçons de 20 ans d’imagerie moderne. J Laryngol Otol 1999; 113: 127-33. |
| [13] | Mohamed, M., Fakiri, El., Youssef, R., F, Zahra Abdala et al. Voluminous laryngeal Schwannoma Treated with Endoscopic Laser Approach. Turk Arch Otorhinolaryngol. 2020; 58(1): 52-5. |
| [14] | Shwettal, M., Madhu, P., Saurabh, V., Sumeet, A., Joyson, X., Manu, M., Abhishek. Atypical extranasopharyngeal angiofibroma in an unusual location: posterior pillar of tonsils (oropharynx). European Journal of Clinical and Experimental Medicine. 2020, 49-53. |
| [15] | Matar, N., M, Remacle. Tumeurs bénignes de l’oropharynx. EMC (Elsevier Masson SAS), Oto-Rhino-Laryngologie. 2015; 10(3): 20-700-A-10. |
| [16] | Freihofer, HP., BjörkG, JE., Kuijpers-Jagtman, AM. Timing of facial osteotomies. A consensus conferences. Oral Surg Oral Med Oral Pathol. 1994; 78: 432–6. |
| [17] | Nicolai, P., Villaret, AB., Farina, D., et al. Endoscopic surgery for juvenile angiofibroma: critical review of indications after 46 cases. Am J Rhinol Allergy. 2010; 24: e67–72. |
| [18] | Makek, MS., Andrews, JC., Fisch, U. Transformation of nasopharyngeal angiofibroma. The Laryngoscope 99 (10). 1989: 1088-1092. |
| [19] | Antonelli, AR., Cappiello, J., Donajo, CA., Lorenzo, D., Nicolai, P., Orlandini, B. Diagnosis, staging, and treatment of juvenile nasopharyngeal angiofibroma. The Laryngoscope 1987; 97: 1319-25. |
| [20] | Gullane, PJ., Davidson, J., O’dwyer, T., Forte, F. Juvenile angiofibrosis: a literature review and case series report. The Laryngoscope 1992; 102: 928-33. |
| [21] | Fagan, JJ., Snyderman, CH., Carrau, RL., Janecka, IP. Nasopharyngeal angiofibromas: choice of surgical approach. Head Neck 1997; 19: 391-9. |
| [22] | Eftekharian, A., Samiei, F., Rakhshan, M. Angifibroma of oropharyngeal origin. Shahid Beheshti University of Medical Sciences, Tehran-Iran. 2008; 24(2): 319-320. |
| [23] | Guerina; N. Un kyste thyréoglosse de la base de langue. Lettre d’oto-rhino-laryngologie et de chirurgie cervico-faciale - n°236 - Octobre 1998. |
| [24] | Bassetti, R., Patrick Tomasetti, P., Johannes Kuttenberger, J. Lipome intraoral de la base de la langue. SWISS DENTAL JOURNAL SSO VOL 125 6 P 2015. |
| [25] | Betsalel, AD. La tumeur fibreuse solitaire de la C B un défi diagnostique. Hal open Sciences du Vivant q-bio. 2023. Dumas-04501579. |
APA Style
Mariam, T., Ibrahim, D., Tata, T., Oumar, K., Aissata, O., et al. (2025). An Unusual Case of Angiofibroma at the Base of the Tongue in a Male Child. Clinical Medicine Research, 14(5), 187-193. https://doi.org/10.11648/j.cmr.20251405.14
ACS Style
Mariam, T.; Ibrahim, D.; Tata, T.; Oumar, K.; Aissata, O., et al. An Unusual Case of Angiofibroma at the Base of the Tongue in a Male Child. Clin. Med. Res. 2025, 14(5), 187-193. doi: 10.11648/j.cmr.20251405.14
AMA Style
Mariam T, Ibrahim D, Tata T, Oumar K, Aissata O, et al. An Unusual Case of Angiofibroma at the Base of the Tongue in a Male Child. Clin Med Res. 2025;14(5):187-193. doi: 10.11648/j.cmr.20251405.14
@article{10.11648/j.cmr.20251405.14,
author = {Tangara Mariam and Dicko Ibrahim and Toure Tata and Konate Oumar and Ouane Aissata and Coulibaly Assitan Kole and Konate Moussa and Keita Moussa Bourama and Berthe Ismael and Simpara Gaoussou and Cisse Naouma and Traore Nouhoum and Konate N'faly and Diarra Kassim and Kone Fatogoma Issa and Guindo Boubacary and Soumaoro Siaka and Singare Kadidiatou and Keita Mohamed Amadou},
title = {An Unusual Case of Angiofibroma at the Base of the Tongue in a Male Child
},
journal = {Clinical Medicine Research},
volume = {14},
number = {5},
pages = {187-193},
doi = {10.11648/j.cmr.20251405.14},
url = {https://doi.org/10.11648/j.cmr.20251405.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cmr.20251405.14},
abstract = {Angiofibroma is a benign but very aggressive tumor due to its tendency for local invasion. It is composed of myofibroblasts and vasogenic elements, making it a highly vascularized tumor. The oropharyngeal angiofibroma is an atypical angiofibroma in terms of location and symptoms. The general objective of our study was to examine the diagnostic and therapeutic characteristics of an angiofibroma with an exceptional location at the base of the tongue through a case observation accompanied by a literature review. This involves a 13-year-old patient who consulted for solid dysphagia. The onset would date back to 2 years after his admission, marked by the progressive installation of a ronchopathy associated with a feeling of a foreign body in the throat, and firm rhinophonia. This clinical picture prompted traditional treatments based on fumigations, which were unsuccessful. The evolution was marked after 3 months by the addition of solid dysphagia and dyspnea in the supine position. Faced with this clinical picture, they decided to consult us for management. The physical examination revealed a budding mass at the base of the tongue with vascular hyperemia that is mobile during tongue prostration and swallowing, with contact and palpation showing no bleeding or pulsation. A nasofibroscopy objectively showed a submucosal lesion budding at the base of the tongue, mobile during swallowing, extending towards the posterior pharyngeal wall and narrowing the oropharyngeal canal. A computed tomography scan with contrast injection suggested a hyperdense tissue mass, well-circumscribed, developing at the expense of the base of the tongue with significant obstruction of the oropharyngeal tract. The histopathological examination of the operative sample after complete transoral surgical excision under general anesthesia was in favor of an angiofibroma rearranged from the base of the language. The patient was lost to follow-up for 2 years due to financial difficulties as all the medical expenses were borne by the patient without any assistance or health insurance.
},
year = {2025}
}
TY - JOUR T1 - An Unusual Case of Angiofibroma at the Base of the Tongue in a Male Child AU - Tangara Mariam AU - Dicko Ibrahim AU - Toure Tata AU - Konate Oumar AU - Ouane Aissata AU - Coulibaly Assitan Kole AU - Konate Moussa AU - Keita Moussa Bourama AU - Berthe Ismael AU - Simpara Gaoussou AU - Cisse Naouma AU - Traore Nouhoum AU - Konate N'faly AU - Diarra Kassim AU - Kone Fatogoma Issa AU - Guindo Boubacary AU - Soumaoro Siaka AU - Singare Kadidiatou AU - Keita Mohamed Amadou Y1 - 2025/10/09 PY - 2025 N1 - https://doi.org/10.11648/j.cmr.20251405.14 DO - 10.11648/j.cmr.20251405.14 T2 - Clinical Medicine Research JF - Clinical Medicine Research JO - Clinical Medicine Research SP - 187 EP - 193 PB - Science Publishing Group SN - 2326-9057 UR - https://doi.org/10.11648/j.cmr.20251405.14 AB - Angiofibroma is a benign but very aggressive tumor due to its tendency for local invasion. It is composed of myofibroblasts and vasogenic elements, making it a highly vascularized tumor. The oropharyngeal angiofibroma is an atypical angiofibroma in terms of location and symptoms. The general objective of our study was to examine the diagnostic and therapeutic characteristics of an angiofibroma with an exceptional location at the base of the tongue through a case observation accompanied by a literature review. This involves a 13-year-old patient who consulted for solid dysphagia. The onset would date back to 2 years after his admission, marked by the progressive installation of a ronchopathy associated with a feeling of a foreign body in the throat, and firm rhinophonia. This clinical picture prompted traditional treatments based on fumigations, which were unsuccessful. The evolution was marked after 3 months by the addition of solid dysphagia and dyspnea in the supine position. Faced with this clinical picture, they decided to consult us for management. The physical examination revealed a budding mass at the base of the tongue with vascular hyperemia that is mobile during tongue prostration and swallowing, with contact and palpation showing no bleeding or pulsation. A nasofibroscopy objectively showed a submucosal lesion budding at the base of the tongue, mobile during swallowing, extending towards the posterior pharyngeal wall and narrowing the oropharyngeal canal. A computed tomography scan with contrast injection suggested a hyperdense tissue mass, well-circumscribed, developing at the expense of the base of the tongue with significant obstruction of the oropharyngeal tract. The histopathological examination of the operative sample after complete transoral surgical excision under general anesthesia was in favor of an angiofibroma rearranged from the base of the language. The patient was lost to follow-up for 2 years due to financial difficulties as all the medical expenses were borne by the patient without any assistance or health insurance. VL - 14 IS - 5 ER -
Department of ENT and Head and Neck Surgery, Mother-Child Hospital Naomi Harris, Kayes, Mali
Faculty of Medicine and Odontostomatology, University of Sciences, Techniques and Technologies of Bamako, Bamako, Mali
Department of ENT and Head and Neck Surgery, Main Medical Center of the Air Force, Bamako, Mali
Department of ENT and Head and Neck Surgery, Gabriel Toure University Hospital, Bamako, Mali
Department of ENT and Head and Neck Surgery, Gabriel Toure University Hospital, Bamako, Mali
Department of ENT and Head and Neck Surgery, Gabriel Toure University Hospital, Bamako, Mali
Department of ENT and Head and Neck Surgery, Gabriel Toure University Hospital, Bamako, Mali; Faculty of Medicine and Odontostomatology, University of Sciences, Techniques and Technologies of Bamako, Bamako, Mali
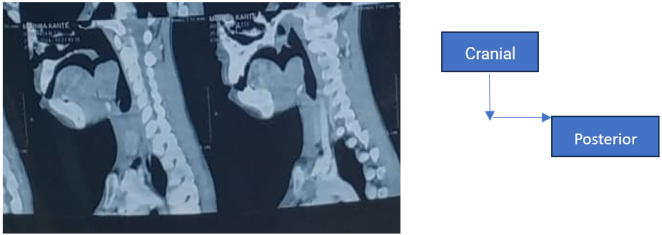
Figure 1. Sagittal section with PC injection suggesting a large expansile tissue process, well-defined developing at the base of the tongue with significant obstruction of the oropharyngeal passage appearing benign.
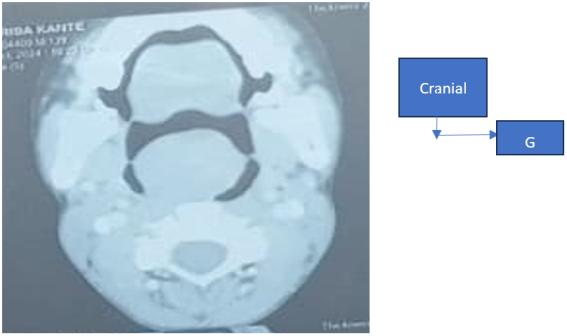
Figure 2. Axial section with PC injection suggesting tissue hyperdensity at the expense of the base of the tongue, with regular contours and significant obstruction of the oropharyngeal pathway.
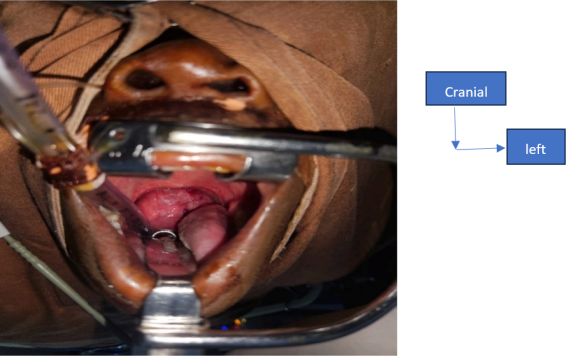
Figure 3. Exposure of the tumor in the oropharynx during surgery.

Figure 4. Image of the surgical site after complete excision.
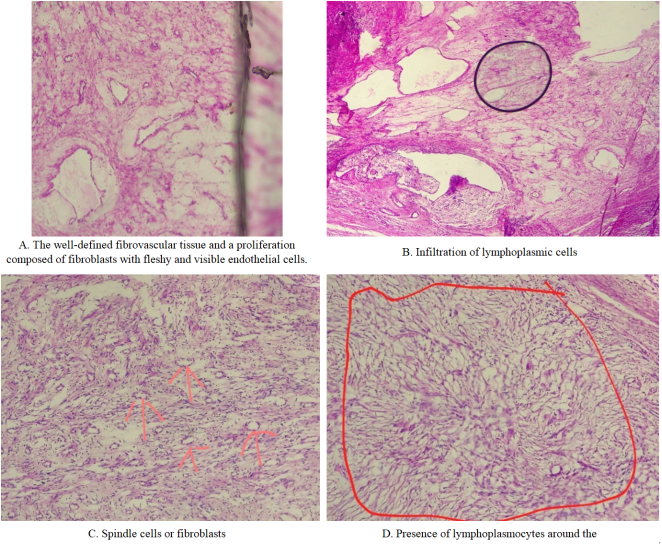
Figure 5. Histological images.

Figure 6. Nasofibroscopic image of the base of the tongue J15 postoperatively.
Information

