Abstract
Post-dural puncture headache (PDPH) is a common complication following spinal anaesthesia, characterised by a postural headache that worsens on standing and improves when supine, with an incidence ranging from 1% to 30% depending on patient and procedural factors. It results primarily from cerebrospinal fluid leakage at the dural puncture site, leading to decreased intracranial pressure, compensatory cerebral vasodilation, and traction on pain-sensitive structures. Despite preventive measures such as atraumatic needles and minimising puncture attempts, PDPH remains clinically significant, prompting interest in pharmacological strategies. Vitamin C, owing to its antioxidant, vasomodulatory, and collagen synthesis–enhancing properties, may support dural healing and regulate cerebral vascular tone, thereby reducing PDPH risk. This prospective, randomised, double-blind, placebo-controlled study evaluated the effect of perioperative vitamin C supplementation on PDPH in 120 ASA I–II patients (18–60 years) undergoing elective lower abdominal or lower limb surgeries under spinal anesthesia. Participants were allocated into two groups: Group V received oral vitamin C (1 g preoperatively and 1 g 12 hours postoperatively), while Group P received placebo. Spinal anesthesia was administered using a 25G Quincke needle with 0.5% hyperbaric bupivacaine. The primary outcome was PDPH incidence within five postoperative days, while secondary outcomes included severity (VAS), onset time, duration, safety, and hemodynamic stability. Baseline characteristics were comparable between groups. The incidence of PDPH was significantly lower in the vitamin C group (10%) compared to the placebo group (21.7%) (p = 0.04). Severity was also reduced (VAS 3.2 ± 1.0 vs 4.6 ± 1.2; p < 0.01), and duration was shorter (2.4 ± 0.8 vs 3.5 ± 1.1 days; p = 0.03). However, the time of onset showed no significant difference (30 ± 5 vs 28 ± 6 hours; p = 0.22). No adverse effects were observed. In conclusion, perioperative vitamin C supplementation significantly reduces the incidence, severity, and duration of PDPH without affecting onset time, offering a safe, cost-effective, and practical adjunct for improving postoperative outcomes and patient comfort following spinal anesthesia.
Keywords
PDPH, Vitamin C, Spinal Anaesthesia, Antioxidant Therapy, Randomised Controlled Trial
1. Introduction
Post-dural puncture headache (PDPH) is a well-recognised complication of neuraxial anaesthesia and continues to pose a significant clinical challenge despite advances in anaesthetic techniques
| [1] | Turnbull DK, Shepherd DB. Post-dural puncture headache: pathogenesis, prevention and treatment. Br J Anaesth 2003; 91(5): 718–729. |
| [2] | Bezov D, Lipton RB, Ashina S. Post-dural puncture headache: Part I—Diagnosis, epidemiology, etiology, and pathophysiology. Headache. 2010; 50(7): 1144–1152. |
[1, 2]
. It is typically characterised by a postural headache that worsens upon sitting or standing and improves when the patient lies down, often accompanied by nausea, vomiting, neck stiffness, photophobia, and auditory disturbances
| [2] | Bezov D, Lipton RB, Ashina S. Post-dural puncture headache: Part I—Diagnosis, epidemiology, etiology, and pathophysiology. Headache. 2010; 50(7): 1144–1152. |
| [3] | Ahmed SV, Jayawarna C, Jude E. Post lumbar puncture headache: diagnosis and management. BMJ. 2006; 333(7563): 365–369. |
[2, 3]
. PDPH not only causes considerable patient discomfort but can also delay mobilisation, prolong hospital stay, and negatively impact overall patient satisfaction
| [1] | Turnbull DK, Shepherd DB. Post-dural puncture headache: pathogenesis, prevention and treatment. Br J Anaesth 2003; 91(5): 718–729. |
| [4] | Vallejo MC. Postdural puncture headache: current perspectives. Curr Opin Anaesthesiol. 2017; 30(3): 372–378. |
[1, 4]
. The incidence of PDPH varies widely, ranging from less than 1% to as high as 30%, depending on several factors such as age, gender, body mass index, needle size and design, and the number of dural puncture attempts
| [2] | Bezov D, Lipton RB, Ashina S. Post-dural puncture headache: Part I—Diagnosis, epidemiology, etiology, and pathophysiology. Headache. 2010; 50(7): 1144–1152. |
| [4] | Vallejo MC. Postdural puncture headache: current perspectives. Curr Opin Anaesthesiol. 2017; 30(3): 372–378. |
[2, 4]
. Younger patients, females, and those undergoing procedures with larger or cutting needles are at higher risk
| [2] | Bezov D, Lipton RB, Ashina S. Post-dural puncture headache: Part I—Diagnosis, epidemiology, etiology, and pathophysiology. Headache. 2010; 50(7): 1144–1152. |
[2]
. The underlying pathophysiology of PDPH is primarily related to persistent leakage of cerebrospinal fluid (CSF) through the dural puncture site, leading to decreased intracranial pressure, traction on pain-sensitive intracranial structures, and compensatory cerebral vasodilation
| [1] | Turnbull DK, Shepherd DB. Post-dural puncture headache: pathogenesis, prevention and treatment. Br J Anaesth 2003; 91(5): 718–729. |
| [3] | Ahmed SV, Jayawarna C, Jude E. Post lumbar puncture headache: diagnosis and management. BMJ. 2006; 333(7563): 365–369. |
[1, 3]
. Various strategies have been proposed to prevent PDPH, including the use of smaller gauge or atraumatic (pencil-point) needles and minimising multiple puncture attempts
| [5] | Arevalo-Rodriguez I, Muñoz L, Godoy-Casasbuenas N, et al. Needle gauge and tip design for preventing post-dural puncture headache. Cochrane Database Syst Rev. 2017; 4: CD010807. |
[5]
. Conservative measures such as adequate hydration and bed rest have also been recommended, although evidence supporting their effectiveness remains inconclusive
| [6] | Arevalo-Rodriguez I, Ciapponi A, Munoz L, et al. Posture and fluids for preventing post-dural puncture headache. Cochrane Database Syst Rev. 2016; 3: CD009199. |
[6]
. Pharmacological interventions such as caffeine and theophylline, as well as invasive techniques like epidural blood patch, have shown varying degrees of success but are not universally effective and may be associated with additional risks
| [1] | Turnbull DK, Shepherd DB. Post-dural puncture headache: pathogenesis, prevention and treatment. Br J Anaesth 2003; 91(5): 718–729. |
| [3] | Ahmed SV, Jayawarna C, Jude E. Post lumbar puncture headache: diagnosis and management. BMJ. 2006; 333(7563): 365–369. |
[1, 3]
. Spinal anaesthesia remains a widely used and effective technique, but complications such as PDPH necessitate ongoing research into safer and more effective preventive strategies
| [10] | Rawal N. Current issues in spinal anesthesia. Eur J Anaesthesiol. 2005; 22(3): 161–162. |
[10]
. In recent years, attention has turned toward the role of oxidative stress and endothelial dysfunction in the development of PDPH. It is hypothesised that CSF loss and intracranial hypotension may trigger biochemical pathways involving reactive oxygen species and altered nitric oxide-mediated vascular responses, leading to cerebral vasodilation and pain
| [2] | Bezov D, Lipton RB, Ashina S. Post-dural puncture headache: Part I—Diagnosis, epidemiology, etiology, and pathophysiology. Headache. 2010; 50(7): 1144–1152. |
| [4] | Vallejo MC. Postdural puncture headache: current perspectives. Curr Opin Anaesthesiol. 2017; 30(3): 372–378. |
[2, 4]
. Vitamin C (ascorbic acid) is a well-known antioxidant with multiple physiological roles, including free radical scavenging, enhancement of endothelial function, and promotion of collagen synthesis
| [7] | Carr AC, Maggini S. Vitamin C and immune function. Nutrients. 2017; 9(11): 1211. |
| [9] | Padayatty SJ, Levine M. Vitamin C: the known and the unknown. Nutrients. 2016; 8(11): 709. |
[7, 9]
. It also plays a significant role in immune function and tissue repair processes
| [7] | Carr AC, Maggini S. Vitamin C and immune function. Nutrients. 2017; 9(11): 1211. |
| [8] | Hemilä H, Chalker E. Vitamin C and infections: a review of the evidence. Nutrients. 2013; 5(11): 4393–4426. |
[7, 8]
. By stabilising vascular tone and supporting dural healing, vitamin C may help mitigate the effects of CSF leakage and facilitate faster recovery
| [9] | Padayatty SJ, Levine M. Vitamin C: the known and the unknown. Nutrients. 2016; 8(11): 709. |
[9]
. Additionally, its influence on nitric oxide pathways may reduce cerebral vasodilation, thereby potentially decreasing the incidence and severity of PDPH
| [9] | Padayatty SJ, Levine M. Vitamin C: the known and the unknown. Nutrients. 2016; 8(11): 709. |
[9]
. Vitamin C is inexpensive, widely available, and has an excellent safety profile, making it an attractive candidate for routine prophylactic use. However, there is limited clinical evidence evaluating its effectiveness in the prevention of PDPH. Therefore, this study was designed to assess the role of vitamin C supplementation in reducing the incidence, severity, and duration of PDPH following spinal anaesthesia.
2. Materials and Methods
2.1. Study Design and Setting
This prospective, randomised, double-blind, placebo-controlled study was conducted at SKIMS HOSPITAL SOURA. Written informed consent was obtained from all participants prior to inclusion in the study.
2.2. Sample Size and Population
A total of 120 patients aged 18–60 years, belonging to ASA physical status I–II and scheduled for elective lower abdominal or lower limb surgeries under spinal anaesthesia, were enrolled and equally divided into two groups (n = 60 each).
Inclusion Criteria:
1) Age 18–60 years
2) ASA I–II
3) Elective surgery under spinal anesthesia
Exclusion Criteria:
1) History of migraine or chronic headache
2) Coagulopathy
3) Infection at puncture site
4) Renal disease or history of renal stones
5) Allergy to study drug
6) Multiple dural puncture attempts
2.3. Randomisation and Blinding
Participants were randomly allocated using a computer-generated sequence into two groups. The study was double-blinded, with both patients and outcome assessors unaware of group allocation.
2.4. Intervention
Group V (Vitamin C): Received oral Vitamin C 1 g one hour before surgery and 1 g 12 hours postoperatively.
Group P (Placebo): Received identical placebo tablets at the same time intervals.
2.5. Anaesthetic Technique
All patients were preloaded with intravenous crystalloid solution prior to the procedure. Standard monitoring, including electrocardiography, non-invasive blood pressure, and pulse oximetry, was applied. Under strict aseptic precautions, spinal anaesthesia was performed in the sitting position at the L3–L4 or L4–L5 interspace using a 25G Quincke needle. After confirming free flow of cerebrospinal fluid, 3 ml of 0.5% hyperbaric bupivacaine was administered intrathecally. Patients were then positioned supine immediately. Hemodynamic parameters were monitored throughout the procedure, and any episodes of hypotension or bradycardia were managed according to standard institutional protocols.
2.6. Outcome Measures
Primary Outcome:
Incidence of post-dural puncture headache (PDPH) within 5 days
Secondary Outcomes:
1) Severity of headache using Visual Analog Scale (VAS)
2) Time of onset
3) Duration of headache
2.7. Statistical Analysis
Data were analysed using statistical software. Continuous variables were expressed as mean ± standard deviation and compared using Student’s t-test. Categorical variables were analyzed using the Chi-square test. A p-value < 0.05 was considered statistically significant.
3. Result
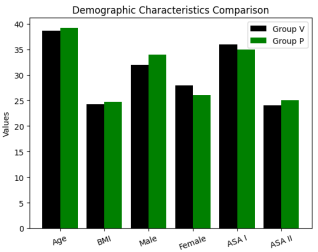
Figure 1. Demographic Characteristics.
Table 1. Demographic Characteristics.
Variable | Group V (n=60) | Group P (n=60) |
Age (years) | 38.6 ± 9.5 | 39.2 ± 10.1 |
Gender (M/F) | 32/28 | 34/26 |
BMI (kg/m²) | 24.3 ± 2.5 | 24.7 ± 2.8 |
ASA I/II | 36/24 | 35/25 |
There was no statistically significant difference in age, gender distribution, BMI, or ASA status between the two groups (p > 0.05).
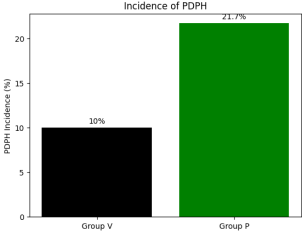
Table 2. Primary Outcome – Incidence of PDPH.
Outcome | Group V | Group P | p-value |
PDPH (n, %) | 6 (10%) | 13 (21.7%) | 0.04 |
Figure 2. Primary Outcome – Incidence of PDPH.
The incidence of post-dural puncture headache (PDPH) was observed in 6 out of 60 patients (10%) in Group V (vitamin C group), compared to 13 out of 60 patients (21.7%) in Group P (placebo group). This demonstrates a notable reduction of approximately 11.7% in the incidence of PDPH among patients receiving vitamin c. Statistical analysis revealed that this difference was statistically significant (p = 0.04), indicating that the reduction in PDPH incidence is unlikely due to chance.
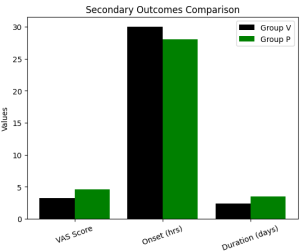
Figure 3. Secondary Outcomes.
Table 3. Secondary Outcomes.
Parameter | Group V | Group P | p-value |
VAS Score | 3.2 ± 1.0 | 4.6 ± 1.2 | <0.01 |
Onset (hours) | 30 ± 5 | 28 ± 6 | 0.22 |
Duration (days) | 2.4 ± 0.8 | 3.5 ± 1.1 | 0.03 |
The severity of post-dural puncture headache, assessed using the Visual Analogue Scale (VAS), was significantly lower in Group V (3.2 ± 1.0) compared to Group P (4.6 ± 1.2), indicating better pain control in patients receiving Vitamin C. This difference was highly statistically significant (p < 0.01). The time of onset of PDPH was comparable between the two groups, with Group V showing onset at 30 ± 5 hours and Group P at 28 ± 6 hours. This difference was not statistically significant (p = 0.22), suggesting that vitamin C does not influence the timing of headache onset. However, the duration of PDPH was significantly shorter in Group V (2.4 ± 0.8 days) compared to Group P (3.5 ± 1.1 days), with a statistically significant difference (p = 0.03).
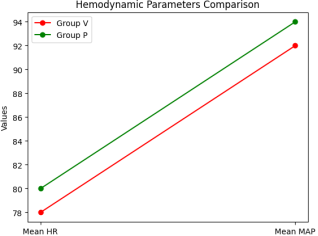
Figure 4. Hemodynamic Parameters.
Table 4. Hemodynamic Parameters.
Parameter | Group V | Group P | p-value |
Mean HR (bpm) | 78 ± 8 | 80 ± 7 | 0.18 |
Mean MAP (mmHg) | 92 ± 6 | 94 ± 7 | 0.21 |
The mean heart rate (HR) in Group V was 78 ± 8 bpm, compared to 80 ± 7 bpm in Group P. This difference was not statistically significant (p = 0.18). Similarly, the mean arterial pressure (MAP) was 92 ± 6 mmHg in Group V and 94 ± 7 mmHg in Group P, with no statistically significant difference (p = 0.21). These findings indicate that both groups maintained comparable hemodynamic stability throughout the study period.
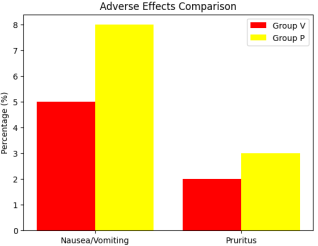
Table 5. Adverse Effects.
Complication | Group V | Group P | p-value |
Nausea/Vomiting | 5% | 8% | 0.52 |
Pruritus | 2% | 3% | 0.65 |
Others | Nil | Nil | — |
Figure 5. Adverse Effects.
The incidence of adverse effects was low in both groups. Nausea and vomiting were observed in 5% of patients in Group V compared to 8% in Group P, while pruritus occurred in 2% of patients in Group V and 3% in Group P. Although the frequency of these complications was slightly higher in the placebo group, the differences were not statistically significant (nausea/vomiting: p = 0.52, pruritus: p = 0.65). Importantly, no other adverse effects were reported in either group, and the majority of patients remained complication-free.
4. Discussion
The present study evaluated the role of Vitamin C in the prevention of post-dural puncture headache (PDPH) following spinal anaesthesia. The findings demonstrate that vitamin C supplementation significantly reduces the incidence, severity, and duration of PDPH without affecting its onset or hemodynamic stability, and without increasing adverse effects. The incidence of PDPH in this study was significantly lower in the vitamin C group (10%) compared to the placebo group (21.7%) (p = 0.04). This reduction suggests a beneficial role of vitamin C in mitigating the development of PDPH. The pathophysiology of PDPH is primarily attributed to cerebrospinal fluid (CSF) leakage leading to intracranial hypotension and compensatory cerebral vasodilation. Vitamin C, being a potent antioxidant, may counteract oxidative stress and stabilise endothelial function, thereby reducing vasodilation and associated headache. In addition to reducing incidence, vitamin C also significantly decreased the severity of PDPH, as reflected by lower VAS scores (3.2 ± 1.0 vs 4.6 ± 1.2, p < 0.01). This finding indicates that even when PDPH occurs, its clinical impact is less pronounced in patients receiving vitamin C. The antioxidant properties of vitamin C may modulate nociceptive pathways and inflammatory responses, thereby attenuating pain perception. Furthermore, the duration of PDPH was significantly shorter in the vitamin C group (2.4 ± 0.8 days) compared to the placebo group (3.5 ± 1.1 days) (p = 0.03). This suggests that vitamin C may facilitate faster recovery, possibly by promoting collagen synthesis and enhancing tissue repair at the dural puncture site, thereby reducing the duration of CSF leakage. However, no significant difference was observed in the onset of PDPH between the two groups (p = 0.22), indicating that vitamin C does not influence the initial development timeline of headache. This finding suggests that while vitamin C may not prevent the immediate physiological consequences of dural puncture, it plays a role in modulating subsequent processes that influence severity and recovery. Hemodynamic parameters, including heart rate and mean arterial pressure, were comparable between the two groups, with no statistically significant differences (p > 0.05). This indicates that vitamin C does not adversely affect cardiovascular stability, making it a safe adjunct in the perioperative period. The incidence of adverse effects was low and similar in both groups. Nausea, vomiting, and pruritus were slightly more frequent in the placebo group, but the differences were not statistically significant. Importantly, no serious complications were observed, further supporting the safety profile of vitamin C. The findings of this study are consistent with emerging evidence suggesting a role for antioxidant therapy in managing PDPH. While traditional preventive strategies focus on mechanical factors such as needle type and technique, pharmacological approaches like vitamin C supplementation offer a simple, cost-effective, and non-invasive alternative. Despite these promising results, certain limitations must be acknowledged. This was a single-centre study with a relatively modest sample size. Additionally, biochemical markers of oxidative stress were not assessed, which could have provided further insight into the underlying mechanisms. Future multicentric studies with larger sample sizes and mechanistic evaluations are recommended to validate these findings. In conclusion, vitamin C supplementation appears to be an effective and safe strategy for reducing the incidence, severity, and duration of PDPH. Its incorporation into routine perioperative protocols may improve patient comfort and enhance recovery following spinal anaesthesia.
5. Conclusion
The present study demonstrates that perioperative supplementation with Vitamin C is an effective strategy for reducing the burden of post-dural puncture headache (PDPH) following spinal anaesthesia. Patients who received vitamin C showed a significantly lower incidence of PDPH compared to the placebo group. In addition, both the severity and duration of headache were markedly reduced, indicating not only a preventive but also a therapeutic benefit. Importantly, vitamin C did not influence the time of onset of PDPH, suggesting that while it may not prevent the initial physiological effects of dural puncture, it plays a significant role in modulating subsequent clinical outcomes. Hemodynamic parameters remained stable and comparable between the two groups, and no increase in adverse effects was observed, confirming its safety in the perioperative setting. Given its antioxidant properties, low cost, ease of administration, and excellent safety profile, vitamin C represents a practical and accessible adjunct in PDPH prevention. Incorporating vitamin C supplementation into routine anaesthetic practice may enhance patient comfort, facilitate faster recovery, and reduce healthcare burden. Further large-scale studies are recommended to validate these findings and establish standardized protocols.
Abbreviations
CSF | Cerebrospinal Fluid |
PDPH | Post-Dural Puncture Headache |
VAS | Visual Analogue Scale |
ASA | American Society of Anesthesiologists |
HR | Heart Rate |
MAP | Mean Arterial Pressure |
Author Contributions
Burhan ul Khursheed: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing
Tahzeeb Sheikh: Data curation, Methodology
Jasir Yousuf: Data curation, Methodology
Anshu: Investigation, Methodology, Project administration
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Turnbull DK, Shepherd DB. Post-dural puncture headache: pathogenesis, prevention and treatment. Br J Anaesth 2003; 91(5): 718–729.
|
| [2] |
Bezov D, Lipton RB, Ashina S. Post-dural puncture headache: Part I—Diagnosis, epidemiology, etiology, and pathophysiology. Headache. 2010; 50(7): 1144–1152.
|
| [3] |
Ahmed SV, Jayawarna C, Jude E. Post lumbar puncture headache: diagnosis and management. BMJ. 2006; 333(7563): 365–369.
|
| [4] |
Vallejo MC. Postdural puncture headache: current perspectives. Curr Opin Anaesthesiol. 2017; 30(3): 372–378.
|
| [5] |
Arevalo-Rodriguez I, Muñoz L, Godoy-Casasbuenas N, et al. Needle gauge and tip design for preventing post-dural puncture headache. Cochrane Database Syst Rev. 2017; 4: CD010807.
|
| [6] |
Arevalo-Rodriguez I, Ciapponi A, Munoz L, et al. Posture and fluids for preventing post-dural puncture headache. Cochrane Database Syst Rev. 2016; 3: CD009199.
|
| [7] |
Carr AC, Maggini S. Vitamin C and immune function. Nutrients. 2017; 9(11): 1211.
|
| [8] |
Hemilä H, Chalker E. Vitamin C and infections: a review of the evidence. Nutrients. 2013; 5(11): 4393–4426.
|
| [9] |
Padayatty SJ, Levine M. Vitamin C: the known and the unknown. Nutrients. 2016; 8(11): 709.
|
| [10] |
Rawal N. Current issues in spinal anesthesia. Eur J Anaesthesiol. 2005; 22(3): 161–162.
|
Cite This Article
-
APA Style
Khursheed, B. U., Sheikh, T., Yousuf, J., Anshu. (2026). Role of Vitamin C Supplementation in the Prevention of Post-Dural Puncture Headache: A Randomized Controlled Trial. International Journal of Anesthesia and Clinical Medicine, 14(1), 92-97. https://doi.org/10.11648/j.ijacm.20261401.24
 Copy
|
Copy
|
 Download
Download
ACS Style
Khursheed, B. U.; Sheikh, T.; Yousuf, J.; Anshu. Role of Vitamin C Supplementation in the Prevention of Post-Dural Puncture Headache: A Randomized Controlled Trial. Int. J. Anesth. Clin. Med. 2026, 14(1), 92-97. doi: 10.11648/j.ijacm.20261401.24
Copy
|
Download
AMA Style
Khursheed BU, Sheikh T, Yousuf J, Anshu. Role of Vitamin C Supplementation in the Prevention of Post-Dural Puncture Headache: A Randomized Controlled Trial. Int J Anesth Clin Med. 2026;14(1):92-97. doi: 10.11648/j.ijacm.20261401.24
Copy
|
Download
-
@article{10.11648/j.ijacm.20261401.24,
author = {Burhan ul Khursheed and Tahzeeb Sheikh and Jasir Yousuf and Anshu},
title = {Role of Vitamin C Supplementation in the Prevention of Post-Dural Puncture Headache: A Randomized Controlled Trial},
journal = {International Journal of Anesthesia and Clinical Medicine},
volume = {14},
number = {1},
pages = {92-97},
doi = {10.11648/j.ijacm.20261401.24},
url = {https://doi.org/10.11648/j.ijacm.20261401.24},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijacm.20261401.24},
abstract = {Post-dural puncture headache (PDPH) is a common complication following spinal anaesthesia, characterised by a postural headache that worsens on standing and improves when supine, with an incidence ranging from 1% to 30% depending on patient and procedural factors. It results primarily from cerebrospinal fluid leakage at the dural puncture site, leading to decreased intracranial pressure, compensatory cerebral vasodilation, and traction on pain-sensitive structures. Despite preventive measures such as atraumatic needles and minimising puncture attempts, PDPH remains clinically significant, prompting interest in pharmacological strategies. Vitamin C, owing to its antioxidant, vasomodulatory, and collagen synthesis–enhancing properties, may support dural healing and regulate cerebral vascular tone, thereby reducing PDPH risk. This prospective, randomised, double-blind, placebo-controlled study evaluated the effect of perioperative vitamin C supplementation on PDPH in 120 ASA I–II patients (18–60 years) undergoing elective lower abdominal or lower limb surgeries under spinal anesthesia. Participants were allocated into two groups: Group V received oral vitamin C (1 g preoperatively and 1 g 12 hours postoperatively), while Group P received placebo. Spinal anesthesia was administered using a 25G Quincke needle with 0.5% hyperbaric bupivacaine. The primary outcome was PDPH incidence within five postoperative days, while secondary outcomes included severity (VAS), onset time, duration, safety, and hemodynamic stability. Baseline characteristics were comparable between groups. The incidence of PDPH was significantly lower in the vitamin C group (10%) compared to the placebo group (21.7%) (p = 0.04). Severity was also reduced (VAS 3.2 ± 1.0 vs 4.6 ± 1.2; p < 0.01), and duration was shorter (2.4 ± 0.8 vs 3.5 ± 1.1 days; p = 0.03). However, the time of onset showed no significant difference (30 ± 5 vs 28 ± 6 hours; p = 0.22). No adverse effects were observed. In conclusion, perioperative vitamin C supplementation significantly reduces the incidence, severity, and duration of PDPH without affecting onset time, offering a safe, cost-effective, and practical adjunct for improving postoperative outcomes and patient comfort following spinal anesthesia.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Role of Vitamin C Supplementation in the Prevention of Post-Dural Puncture Headache: A Randomized Controlled Trial
AU - Burhan ul Khursheed
AU - Tahzeeb Sheikh
AU - Jasir Yousuf
AU - Anshu
Y1 - 2026/04/16
PY - 2026
N1 - https://doi.org/10.11648/j.ijacm.20261401.24
DO - 10.11648/j.ijacm.20261401.24
T2 - International Journal of Anesthesia and Clinical Medicine
JF - International Journal of Anesthesia and Clinical Medicine
JO - International Journal of Anesthesia and Clinical Medicine
SP - 92
EP - 97
PB - Science Publishing Group
SN - 2997-2698
UR - https://doi.org/10.11648/j.ijacm.20261401.24
AB - Post-dural puncture headache (PDPH) is a common complication following spinal anaesthesia, characterised by a postural headache that worsens on standing and improves when supine, with an incidence ranging from 1% to 30% depending on patient and procedural factors. It results primarily from cerebrospinal fluid leakage at the dural puncture site, leading to decreased intracranial pressure, compensatory cerebral vasodilation, and traction on pain-sensitive structures. Despite preventive measures such as atraumatic needles and minimising puncture attempts, PDPH remains clinically significant, prompting interest in pharmacological strategies. Vitamin C, owing to its antioxidant, vasomodulatory, and collagen synthesis–enhancing properties, may support dural healing and regulate cerebral vascular tone, thereby reducing PDPH risk. This prospective, randomised, double-blind, placebo-controlled study evaluated the effect of perioperative vitamin C supplementation on PDPH in 120 ASA I–II patients (18–60 years) undergoing elective lower abdominal or lower limb surgeries under spinal anesthesia. Participants were allocated into two groups: Group V received oral vitamin C (1 g preoperatively and 1 g 12 hours postoperatively), while Group P received placebo. Spinal anesthesia was administered using a 25G Quincke needle with 0.5% hyperbaric bupivacaine. The primary outcome was PDPH incidence within five postoperative days, while secondary outcomes included severity (VAS), onset time, duration, safety, and hemodynamic stability. Baseline characteristics were comparable between groups. The incidence of PDPH was significantly lower in the vitamin C group (10%) compared to the placebo group (21.7%) (p = 0.04). Severity was also reduced (VAS 3.2 ± 1.0 vs 4.6 ± 1.2; p < 0.01), and duration was shorter (2.4 ± 0.8 vs 3.5 ± 1.1 days; p = 0.03). However, the time of onset showed no significant difference (30 ± 5 vs 28 ± 6 hours; p = 0.22). No adverse effects were observed. In conclusion, perioperative vitamin C supplementation significantly reduces the incidence, severity, and duration of PDPH without affecting onset time, offering a safe, cost-effective, and practical adjunct for improving postoperative outcomes and patient comfort following spinal anesthesia.
VL - 14
IS - 1
ER -
Copy
|
Download