Rhabdomyosarcomas (RMS) are malignant tumors derived embryonically from the mesenchymal tissue that form from the skeletal muscles. It is the most common soft tissue sarcoma in pediatrics. The embryonal mesenchymal subtype is the most common and is often diagnosed in the first decade of life. Treatment of RMS is multimodal including systemic chemotherapy, surgery and radiotherapy. In sub-Saharan Africa, data in pediatric cancers, and on RMS in particular, are rare and limited generaly to case reports. This case aims to report a bladder embryonal rhabdomyosarcoma in a 19-month-old child boy who is diagnosed post mortem. It was referred to the pediatric emergency department for sudden painful complete inability to urinate. On clinical examination, an acute urine retention was diagnosed and transurethral catherisation was established with resultant drainnage of hematic urine. Hemodynamic parameters were unstable, with oxygen saturation at 91%. A painless well-fixed mass of solid appearance was palpable at the hypogastric. Laboratory exams showed an impaired renal function with metabolic acidosis. Urine culture and sensitivity testing revealed a urinary tract infection that isolated klebsiella pneumonia. Emergency ultrasonography of the urinary tract, showed a large, heterogeneous, multilobulated intravesical vegetative mass measuring 60.85 x 35.34 x 42.2mm, responsible of a bilateral stage VI ureterohydronephrosis. Abdominal-pelvic MRI showed a vegetative postero-basal tissue mass invading the entire bladder trigone and classified T3bN0Mx. Bilateral nephrostomy was performed the following day with a medical resuscitation, and antibiotherapy adapted to renal function, was installed. A cystoscopy was performed under general anaesthesia showed a large bladder mass filling almost the entire bladder lumen. The biopsy was done using a monopolar resector. The post-operative event was marked by a cardiorespiratory arrest with failure of all reanimation maneuvers occurred. The histological results the biopsy showed a sarcomatous proliferation of small round or spindle-shaped fusiformed cells with hyperchromatic nuclei and little cytoplasm. Mitotic activity was high. Immunohistochemical analysis showed desmin and myoginin, confirming the diagnosis of embryonal-type rhabdomyosarcoma classified as TNM stage II and ISRG IV.
| Published in | International Journal of Clinical Oncology and Cancer Research (Volume 11, Issue 1) |
| DOI | 10.11648/j.ijcocr.20261101.12 |
| Page(s) | 15-21 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Bladder Cancer, Rhabdomyosarcoma, Embryonal Subtype, Onco-pediatrics
Constants | Values/ Units |
|---|---|
Body temperature | 36.5 ° C |
Blood pressure | 120/ 100mmHg |
Heart Rate | 120 Bpm |
Respiratory Rate | 20 Cpm |
Diuresis | 200 Cc/ 24H |
Capillary Dextro | 1.17 g/dL |
Saturation of 02 | 91% |
Head circumference | 48 cm |
Height | 86 cm |
Weight | 9450 g |
Constants | Values / Units |
|---|---|
Hemoglobin level | 7.1 g/dL |
hematocrit | 20.7% |
Creatinine level | 43.8 mg/L |
Blood urea | 1.17 g/L |
Kalemia | 4 mEq/l |
Natremia | 115 mEq/l |
Blood pH | 6.98 |
pCO2 | 29mmHg |
pO2 | 62mmHg |
Bicarbonate (HCO3) | 7mmol/L |
Hight bases | -23.4mmol/L |
RMS | Rhabdomyosarcomas |
MRI | Magnetic Resonance Imagery |
TNM | Tumor Node and Metastasis |
GU | Genitourinary |
ISRG | Intergroup Rhabdomyosarcoma Study |
HPD | Hospital Principal of Dakar |
CT | Computed Tomography |
FDG -PET | Fluorodeoxy-D-Glucose Positron Emission Tomography |
EFS | Event Free Survival |
PET-CT | Positron Emission Tomography-Computed Tomography |
| [1] | Leaphart C, Rodeberg D: Pediatric surgical oncology: management of rhabdomyosarcoma. Surg Oncol. 2007; 16(3): 173–85. |
| [2] | Castle JT, Levy BE, Allison DB, Rodeberg DA, Rellinger EJ. Pediatric Rhabdomyosarcomas of the Genitourinary Tract. Cancers (Basel). 2023 May 22; 15(10): 2864. |
| [3] | Joshi D, Anderson JR, Paidas C, Breneman J, Parham DM, Crist W. Age is an independent prognostic factor in rhabdomyosarcoma: a report from the soft tissue sarcoma committee of the Children’s Oncology Group. Pediatr Blood Cancer. 2004; 42(1): 64–73. |
| [4] | Ferrer FA, Isakoff M, Koyle MA. Bladder/prostate rhabdomyosarcoma: past, present and future. J Urol. 2006; 176(4): 1283–91. |
| [5] | Rodeberg DA, Anderson JR, Arndt CA, et al. Comparison of outcomes based on treatment algorithms for rhabdomyosarcoma of the bladder/prostate: combined results from the Children’s Oncology Group, German Cooperative Soft Tissue Sarcoma Study, Italian Cooperative Group, and International Society of Pediatric Oncology Malignant Mesenchymal Tumors Committee. Int J Cancer. 2011; 128(5): 1232-1239. |
| [6] | Fuchs J, Paulsen F, Bleif M et al. Conservative surgery with combined high dose rate brachytherapy for patients suffering from genitourinary and perianal rhabdomyosarcoma. Radiother Oncol (2016), |
| [7] | Tembely A, Diakite ML, Berthe HJG, et al. Vesical rhabdomyosarcoma: a case study from the Urology Department at Point G University Hospital. Mali Med. 2010; 25(3): 49–52. |
| [8] | Arndt C, Rodeberg D, Breitfeld PP, et al. Does bladder preservation (as a surgical principle) lead to retaining bladder function in bladder/prostate rhabdomyosarcoma? Results from intergroup rhabdomyosarcoma study iv. J Urol. 2004 Jun; 171(6 Pt 1): 2396-403. |
| [9] | Dasgupta R, Rodeberg DA. Update on rhabdomyosarcoma. Semin Pediatr Surg. 2012 Feb; 21(1): 68-78. |
| [10] | Buszek SM, Ludmir EB, Grosshans DR, et al. Patterns of failure and toxicity profile following proton beam therapy for pediatric bladder and prostate rhabdomyosarcoma. Pediatr Blood Cancer. 2019 Nov; 66(11): e27952. |
| [11] | Choi J. H., Ro J. Y. The 2020 WHO Classification of Tumors of Bone: An Updated Review. Adv. Anat. Pathol. 2021; 28: 119–138. |
| [12] | Li J, Thompson TD, Miller JW, et al. Cancer incidence among children and adolescents in the United States, 2001-2003. Pediatrics. 2008 Jun; 121(6): e1470-7. |
| [13] | Pastore G, Peris-Bonet R, Carli M, et al. Childhood soft tissue sarcomas incidence and survival in European children (1978-1997): report from the Automated Childhood Cancer Information System project. Eur J Cancer. 2006 Sep; 42(13): 2136-49. |
| [14] | Stefan C, Bray F, Ferlay J, et al. Cancer of childhood in sub-Saharan Africa. Ecancermedicalscience. 2017 Jul 28; 11: 755. |
| [15] | Saltzman AF, Cost NG. Current Treatment of Pediatric Bladder and Prostate Rhabdomyosarcoma. Curr Urol Rep. 2018 Feb 22; 19(1): 11. |
| [16] | Mbeutcha A, Lucca I, Mathieu R, et al. Current Status of Urinary Biomarkers for Detection and Surveillance of Bladder Cancer. Urol Clin North Am. 2016 Feb; 43(1): 47-62. |
| [17] | Harel M, Ferrer FA, Shapiro LH, Makari JH. Future directions in risk stratification and therapy for advanced pediatric genitourinary rhabdomyosarcoma. Urol Oncol. 2016 Feb; 34(2): 103-15. |
| [18] | Norman G, Fayter D, Lewis-Light K, et al. An emerging evidence base for PET-CT in the management of childhood rhabdomyosarcoma: systematic review. BMJ Open. 2015 Jan 8; 5(1): e006030. |
| [19] | Denes FT, Duarte RJ, Cristófani LM, et al. Pediatric genitourinary oncology. Front Pediatr. 2013 Dec 16; 1: 48. |
| [20] | Malempati S, Hawkins DS. Rhabdomyosarcoma: review of the Children's Oncology Group (COG) Soft-Tissue Sarcoma Committee experience and rationale for current COG studies. Pediatr Blood Cancer. 2012 Jul 15; 59(1): 5-10. |
APA Style
Thiapato, F. S., Mbene, F., Bintou, D. R. F., Hamidou, K. K., Souleymane, S. E. H., et al. (2026). A Pediatric Case of Embryonal Rhabdomyosarcoma of the Bladder: A Case Report and Literature Review. International Journal of Clinical Oncology and Cancer Research, 11(1), 15-21. https://doi.org/10.11648/j.ijcocr.20261101.12
ACS Style
Thiapato, F. S.; Mbene, F.; Bintou, D. R. F.; Hamidou, K. K.; Souleymane, S. E. H., et al. A Pediatric Case of Embryonal Rhabdomyosarcoma of the Bladder: A Case Report and Literature Review. Int. J. Clin. Oncol. Cancer Res. 2026, 11(1), 15-21. doi: 10.11648/j.ijcocr.20261101.12
@article{10.11648/j.ijcocr.20261101.12,
author = {Faye Samba Thiapato and Fall Mbene and Diop Rama Fatou Bintou and Kikalulu Kiambote Hamidou and Sarr El Hadji Souleymane and Seck Aita and Dembele Mamadou and Diatta Marie Noel and Ndiaye Abdoulaye},
title = {A Pediatric Case of Embryonal Rhabdomyosarcoma of the Bladder: A Case Report and Literature Review},
journal = {International Journal of Clinical Oncology and Cancer Research},
volume = {11},
number = {1},
pages = {15-21},
doi = {10.11648/j.ijcocr.20261101.12},
url = {https://doi.org/10.11648/j.ijcocr.20261101.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcocr.20261101.12},
abstract = {Rhabdomyosarcomas (RMS) are malignant tumors derived embryonically from the mesenchymal tissue that form from the skeletal muscles. It is the most common soft tissue sarcoma in pediatrics. The embryonal mesenchymal subtype is the most common and is often diagnosed in the first decade of life. Treatment of RMS is multimodal including systemic chemotherapy, surgery and radiotherapy. In sub-Saharan Africa, data in pediatric cancers, and on RMS in particular, are rare and limited generaly to case reports. This case aims to report a bladder embryonal rhabdomyosarcoma in a 19-month-old child boy who is diagnosed post mortem. It was referred to the pediatric emergency department for sudden painful complete inability to urinate. On clinical examination, an acute urine retention was diagnosed and transurethral catherisation was established with resultant drainnage of hematic urine. Hemodynamic parameters were unstable, with oxygen saturation at 91%. A painless well-fixed mass of solid appearance was palpable at the hypogastric. Laboratory exams showed an impaired renal function with metabolic acidosis. Urine culture and sensitivity testing revealed a urinary tract infection that isolated klebsiella pneumonia. Emergency ultrasonography of the urinary tract, showed a large, heterogeneous, multilobulated intravesical vegetative mass measuring 60.85 x 35.34 x 42.2mm, responsible of a bilateral stage VI ureterohydronephrosis. Abdominal-pelvic MRI showed a vegetative postero-basal tissue mass invading the entire bladder trigone and classified T3bN0Mx. Bilateral nephrostomy was performed the following day with a medical resuscitation, and antibiotherapy adapted to renal function, was installed. A cystoscopy was performed under general anaesthesia showed a large bladder mass filling almost the entire bladder lumen. The biopsy was done using a monopolar resector. The post-operative event was marked by a cardiorespiratory arrest with failure of all reanimation maneuvers occurred. The histological results the biopsy showed a sarcomatous proliferation of small round or spindle-shaped fusiformed cells with hyperchromatic nuclei and little cytoplasm. Mitotic activity was high. Immunohistochemical analysis showed desmin and myoginin, confirming the diagnosis of embryonal-type rhabdomyosarcoma classified as TNM stage II and ISRG IV.},
year = {2026}
}
TY - JOUR T1 - A Pediatric Case of Embryonal Rhabdomyosarcoma of the Bladder: A Case Report and Literature Review AU - Faye Samba Thiapato AU - Fall Mbene AU - Diop Rama Fatou Bintou AU - Kikalulu Kiambote Hamidou AU - Sarr El Hadji Souleymane AU - Seck Aita AU - Dembele Mamadou AU - Diatta Marie Noel AU - Ndiaye Abdoulaye Y1 - 2026/01/23 PY - 2026 N1 - https://doi.org/10.11648/j.ijcocr.20261101.12 DO - 10.11648/j.ijcocr.20261101.12 T2 - International Journal of Clinical Oncology and Cancer Research JF - International Journal of Clinical Oncology and Cancer Research JO - International Journal of Clinical Oncology and Cancer Research SP - 15 EP - 21 PB - Science Publishing Group SN - 2578-9511 UR - https://doi.org/10.11648/j.ijcocr.20261101.12 AB - Rhabdomyosarcomas (RMS) are malignant tumors derived embryonically from the mesenchymal tissue that form from the skeletal muscles. It is the most common soft tissue sarcoma in pediatrics. The embryonal mesenchymal subtype is the most common and is often diagnosed in the first decade of life. Treatment of RMS is multimodal including systemic chemotherapy, surgery and radiotherapy. In sub-Saharan Africa, data in pediatric cancers, and on RMS in particular, are rare and limited generaly to case reports. This case aims to report a bladder embryonal rhabdomyosarcoma in a 19-month-old child boy who is diagnosed post mortem. It was referred to the pediatric emergency department for sudden painful complete inability to urinate. On clinical examination, an acute urine retention was diagnosed and transurethral catherisation was established with resultant drainnage of hematic urine. Hemodynamic parameters were unstable, with oxygen saturation at 91%. A painless well-fixed mass of solid appearance was palpable at the hypogastric. Laboratory exams showed an impaired renal function with metabolic acidosis. Urine culture and sensitivity testing revealed a urinary tract infection that isolated klebsiella pneumonia. Emergency ultrasonography of the urinary tract, showed a large, heterogeneous, multilobulated intravesical vegetative mass measuring 60.85 x 35.34 x 42.2mm, responsible of a bilateral stage VI ureterohydronephrosis. Abdominal-pelvic MRI showed a vegetative postero-basal tissue mass invading the entire bladder trigone and classified T3bN0Mx. Bilateral nephrostomy was performed the following day with a medical resuscitation, and antibiotherapy adapted to renal function, was installed. A cystoscopy was performed under general anaesthesia showed a large bladder mass filling almost the entire bladder lumen. The biopsy was done using a monopolar resector. The post-operative event was marked by a cardiorespiratory arrest with failure of all reanimation maneuvers occurred. The histological results the biopsy showed a sarcomatous proliferation of small round or spindle-shaped fusiformed cells with hyperchromatic nuclei and little cytoplasm. Mitotic activity was high. Immunohistochemical analysis showed desmin and myoginin, confirming the diagnosis of embryonal-type rhabdomyosarcoma classified as TNM stage II and ISRG IV. VL - 11 IS - 1 ER -
Urology Departement, Principal Main Hospital of Dakar, Dakar, Senegal
Urology Departement, Principal Main Hospital of Dakar, Dakar, Senegal
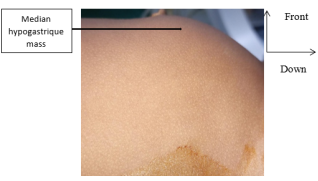
Figure 1. Hypogastric mass [IMAGE_HPD].
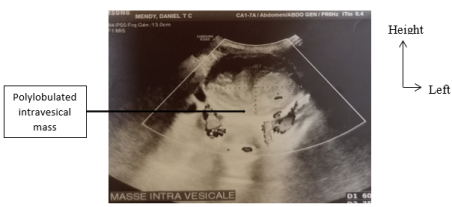
Figure 2. Bladder mass seen on echography [IMAGE_HPD].
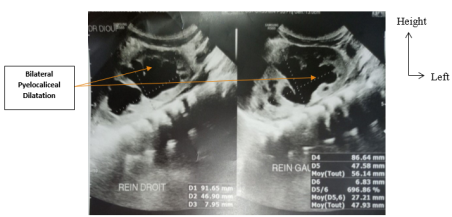
Figure 3. Bilateral Pyelocaliceal Dilatation on echography [Image HPD].
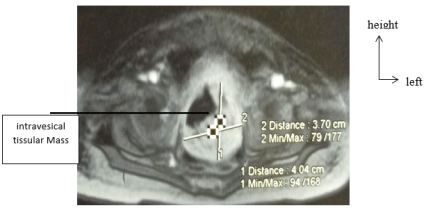
Figure 4. Intravesical aspect of the mass seen at MRI [IMAGE_HPD].
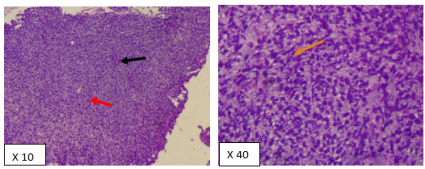
Figure 5. Microscopic Aspect of ERMS [IMAGE_HPD].
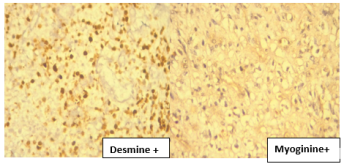
Figure 6. Immunohistochemical reactions of Desmine and Myoginine (X40) [IMAGE_HPD].
Information

