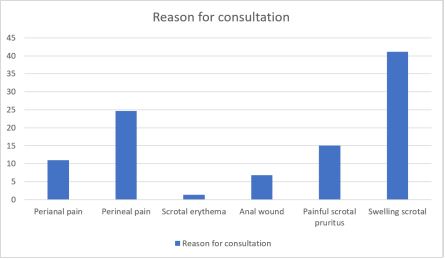
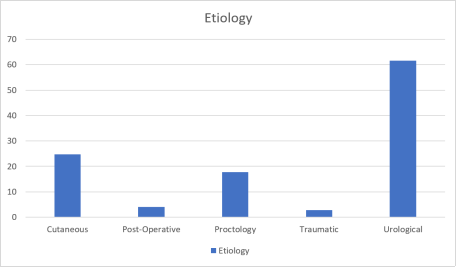
Intoduction: The aim of our study was to identify the factors that determine the vital and functional prognosis of patients with gangrene of the external genitalia. Patients and Methods: Our study is retrospective and descriptive. It concerned all patients treated for Gangrene of the external genitalia (GOGE) in the Urology Department of the Cocody University Hospital over a period of 13 years. Results: Among the 3244 patients consulted for a surgical pathology, 73 (2.25%) had a GOGE. The mean age of patients was 48.81 years with extremes of 19 and 74 years. The majority of patients were male. The main reasons for consultation were scrotal swelling (41.1%) and perineal pain. More than half (53.1%) consulted between 8 and 15 days. Gangrene mainly affected the scrotum, perineum, and in some cases, the penis and pelvis. Diabetes was the most common risk factor (50.68%), followed by alcoholism (23.29%) and acute kidney injury (15.07%). Urological causes were the most common with more than half of the cases (61.64%). All patients underwent surgical debridement. Triple broad-spectrum antibiotic therapy combining a 3rd generation cephalosporin, an Imidazole and an Aminoside was initiated in the majority of cases (93.15%). Nearly half of the patients were treated the day after their admission. The cure rate was 89.04%, with a mortality rate of 6.85%. Major erectile dysfunction and dysuria were found in 35.61% and 34.25% of patients, respectively. Conclusion: Early therapeutic management, well-codified treatment and a multidisciplinary care pathway could improve patients' prognostic factors. Our study suggests that patients surviving after gangrene of the external genitalia show a marked and continuous impairment in their overall urological and sexual quality of life.
| Published in | International Journal of Clinical Urology (Volume 9, Issue 2) |
| DOI | 10.11648/j.ijcu.20250902.22 |
| Page(s) | 180-186 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Gangrene, Prognosis, Genitals
TIME LIMIT FOR CONSULTATION | NUMDER (n) | PERCENTAGES (%) |
|---|---|---|
The first 7 days | 25 | 34,25 |
Between 8 and 15 days | 39 | 53,42 |
After 15 days | 9 | 12,33 |
Total | 73 | 100,00 |
SEATS | NUMBER (n) | PERCENTAGES (%) |
|---|---|---|
Not Successful | 4 | 5,48 |
Penis | 1 | 1,37 |
Penis + Scrotum | 10 | 13,70 |
Penis+Perineum+Scrotum+Pelvis | 3 | 4,11 |
Perineum | 9 | 12,33 |
Perineum + scrotum | 24 | 32,88 |
Scrotum | 22 | 30,14 |
Total | 73 | 100,00 |
RISK FACTORS | STAFF (n) | PERCENTAGES (%) |
|---|---|---|
HIV ((human immunodeficiency virus) | 2 | 2,74 |
Diabetes | 37 | 50,68 |
Obesity | 1 | 1,37 |
AKI (acute kidney injury) | 11 | 15,07 |
Malnutrition | 1 | 1,37 |
Alcoholism | 17 | 23,29 |
Drug | 1 | 1,37 |
Poor Hygiene | 8 | 10,96 |
Tobacco | 15 | 20,55 |
GOGE | Gangrene of the External Genitalia |
| [1] | Eke N (2000). Fournier's gangrene: a review of 1,726 cases. Br J Surg 87: 718-28. |
| [2] | Jeong HJ, ParkSC, SEO IY, Rim JS (2005) Prognostic factors in Fournier's gangrene. Int J Urol 12: 1041-1044. |
| [3] | Tahmaz L, Erdemir F, Tahmaz L, Kibar Y et al. (2006) Fournier's gangrene: report of thirty-three cases and a review of literature. Int J Urol 13: 960-67. |
| [4] | Mehl AA, Filho DCN, Mantovani LM, Grippal MM, Berger, Krauss D and Ly. Management of fournier's gangrene: experience of a univertity hospital of Curitiba. Rev armneck CIR 2010; 37: p 435-41. |
| [5] | Sarkis P, Farran F, Khoury R. Gangène de Fournier: revue de la littérature actuelle, The surgeon 2009. Volume 19.2: p75-84. |
| [6] | Mougougou A, Essola L, Ndang Ngou Milama S, Ngomas JF, Papa Iebama P, Mbethé D, Bissiriou I, Angué Obiang M, Didja DB, Massandé Mouyendi J. Gangen of the external genitalia: epidemiological, diagnostic and therapeutic aspects. Journal of Central African Surgery (RECAC) volume 3, number 17 December 2019. P32-34. |
| [7] | Dekou A, Konan PG, Vodi C, Kramo N, Fofana A, Tchetche G, Ouegnin GA, Manzan K. Gangrene of the external genitalia: epidemiology, competitive morbidity and prognosis. ABM 2014 Volume 19, N3: p61-67. |
| [8] | Diallo MS, Coulibaly MT, Cissé D, Berthé HJG, Diarra A, Tembély A. Epidemiological, clinical and therapeutic aspects of Fournier's gangrene in the urology department of the Point-G University Hospital in Bamako (Mali). Rev Mali infect microbiol 2019, tome 14, p 01-05. |
| [9] | Czymek R, Hildebrand P, Kleeman M, et al (2009) New insights into the epidemiology and etiology of Fournier's gangrene: a review of 33 patients. Infection 37: 306-12. |
| [10] | Sehmi S, Osaghae S (2011) Type II diabetes mellitus, new presentation manifesting as Fournier's gangrene. JRSM Short Rep2: 51. |
| [11] | Jeong H. J., Park Sc., Seo Iy., Rim Js. Fournier's gangrene. Int. J. Urol., 2005, 12: 1. |
| [12] | Adama Toutou Diallo. FOURNIER'S GANGRENE: CLINICAL AND THERAPEUTIC STUDY IN THE <> SURGERY DEPARTMENT OF THE POINT G UNIVERSITY HOSPITAL. Th Med Bamako 2007 n°78.07M78. |
| [13] | Nouhoum Dicko. THE MANAGEMENT OF FOURNIER'S GANGRENE IN THE UROLOGY DEPARTMENT OF THE POINT G UNIVERSITY HOSPITAL. ABOUT 36 CASES. Th Med Bamako, 2015. No. 122. 15m122. |
| [14] | Bah I, Diallo A. B and Coll. Problem of the management of gangrene of the external genitalia in the urology-andrology department of the University Hospital of Conakry URO ANDRO-Volume 1- Num 1 December 2023. |
| [15] | Fall B. and Coll. Gangrene of the external genitalia: about 102 cases. Andrology 2009, 19, 45-9. |
| [16] | Jaime Ruiz-Tovar, Luis Cordoba, José Manuel Devesa. Prognostic factors in Fournier gangrene, Asian Journal of Surgery 2012. p: 35-41. |
| [17] | K. Borki, Ait Ali, And Coll. gangrene perineo-scrotal: about 60 cases e – memoirs of the National Academy of Surgery 2002, 1(4): 49-54 on the net 19-04-2005. |
| [18] |
Kokaina S. Gangrene of the external genitalia: clinical, diagnostic, therapeutic and evolutionary aspects in the urology department of the Gabriel Toure University Hospital. Thesis University of Science, Technology and Technology of Bamako. 2021. Available at:
https://www.bibliosante.ml/bitstream/handle/123456789/4652/21M28.pdf ?sequence=1&isAllowed=y |
| [19] | Boyer A, Vagas F, Fournier's gangrene: emergencies 2011, 53: 601-08. |
| [20] | Morua A. G et al. Fournier's gangrene: our experience in 5 years, bibliographic. Review and assessment of the fournier's gangrene severity index, Archivos Espanoles de Urologia 2009; 62 (7): 532- 540. |
| [21] | Hubert J, Fournier G, Mangin P, Punga-Maole M (1995) Gangrene of the external genitalia. Prog Urol 5: 911-24. |
| [22] | De Jong Z, Anaya Y, Pontonnier F, et l (1995) Evolution and treatment of eight patients with Fournier's perineoscrotal gangrene. Ann Urol 26: 364-7. |
| [23] | Kuo C, Wang W, Lee C, Liu C, Tseng H. Fournier's gangrene: ten-year experience in a medical center in northern Taiwan J Microbiol Immunol Infect 2007; 40(6): 500-6. |
| [24] | El Moussaoui A, Boutaleb R, Joual A, El Mrini M, Meziane F, Benjelloun S. perineoscrotal gangrene: analysis of forty-nine cases. Ann Urol 1994; Rev. 28: 142-7. |
| [25] | Czymek R, Kujath P, Bruch HP, Pfeiffer D, Nebrig M, Seehofer D, et al, Treatment, outcome and quality of life after Fournier's gangrene: a multicentre study. Colorectal Dis 2013; 15(12): 1529-36. |
APA Style
Kouame, B., Kramo, F. N., Coulibaly, I., Drabo, A., Armand, T. K. W. (2025). Gangrene of the External Genitalia: Vital and Functional Prognosis in the Urology Department of the Cocody University Hospital from 2010 to 2022. International Journal of Clinical Urology, 9(2), 180-186. https://doi.org/10.11648/j.ijcu.20250902.22
ACS Style
Kouame, B.; Kramo, F. N.; Coulibaly, I.; Drabo, A.; Armand, T. K. W. Gangrene of the External Genitalia: Vital and Functional Prognosis in the Urology Department of the Cocody University Hospital from 2010 to 2022. Int. J. Clin. Urol. 2025, 9(2), 180-186. doi: 10.11648/j.ijcu.20250902.22
AMA Style
Kouame B, Kramo FN, Coulibaly I, Drabo A, Armand TKW. Gangrene of the External Genitalia: Vital and Functional Prognosis in the Urology Department of the Cocody University Hospital from 2010 to 2022. Int J Clin Urol. 2025;9(2):180-186. doi: 10.11648/j.ijcu.20250902.22
@article{10.11648/j.ijcu.20250902.22 ,
author = {Benjamin Kouame and Felicite Nykan Kramo and Issoufou Coulibaly and Ali Drabo and Tano Kouamé William Armand},
title = {Gangrene of the External Genitalia: Vital and Functional Prognosis in the Urology Department of the Cocody University Hospital from 2010 to 2022
},
journal = {International Journal of Clinical Urology},
volume = {9},
number = {2},
pages = {180-186},
doi = {10.11648/j.ijcu.20250902.22 },
url = {https://doi.org/10.11648/j.ijcu.20250902.22 },
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcu.20250902.22 },
abstract = {Intoduction: The aim of our study was to identify the factors that determine the vital and functional prognosis of patients with gangrene of the external genitalia. Patients and Methods: Our study is retrospective and descriptive. It concerned all patients treated for Gangrene of the external genitalia (GOGE) in the Urology Department of the Cocody University Hospital over a period of 13 years. Results: Among the 3244 patients consulted for a surgical pathology, 73 (2.25%) had a GOGE. The mean age of patients was 48.81 years with extremes of 19 and 74 years. The majority of patients were male. The main reasons for consultation were scrotal swelling (41.1%) and perineal pain. More than half (53.1%) consulted between 8 and 15 days. Gangrene mainly affected the scrotum, perineum, and in some cases, the penis and pelvis. Diabetes was the most common risk factor (50.68%), followed by alcoholism (23.29%) and acute kidney injury (15.07%). Urological causes were the most common with more than half of the cases (61.64%). All patients underwent surgical debridement. Triple broad-spectrum antibiotic therapy combining a 3rd generation cephalosporin, an Imidazole and an Aminoside was initiated in the majority of cases (93.15%). Nearly half of the patients were treated the day after their admission. The cure rate was 89.04%, with a mortality rate of 6.85%. Major erectile dysfunction and dysuria were found in 35.61% and 34.25% of patients, respectively. Conclusion: Early therapeutic management, well-codified treatment and a multidisciplinary care pathway could improve patients' prognostic factors. Our study suggests that patients surviving after gangrene of the external genitalia show a marked and continuous impairment in their overall urological and sexual quality of life.
},
year = {2025}
}
TY - JOUR T1 - Gangrene of the External Genitalia: Vital and Functional Prognosis in the Urology Department of the Cocody University Hospital from 2010 to 2022 AU - Benjamin Kouame AU - Felicite Nykan Kramo AU - Issoufou Coulibaly AU - Ali Drabo AU - Tano Kouamé William Armand Y1 - 2025/10/31 PY - 2025 N1 - https://doi.org/10.11648/j.ijcu.20250902.22 DO - 10.11648/j.ijcu.20250902.22 T2 - International Journal of Clinical Urology JF - International Journal of Clinical Urology JO - International Journal of Clinical Urology SP - 180 EP - 186 PB - Science Publishing Group SN - 2640-1355 UR - https://doi.org/10.11648/j.ijcu.20250902.22 AB - Intoduction: The aim of our study was to identify the factors that determine the vital and functional prognosis of patients with gangrene of the external genitalia. Patients and Methods: Our study is retrospective and descriptive. It concerned all patients treated for Gangrene of the external genitalia (GOGE) in the Urology Department of the Cocody University Hospital over a period of 13 years. Results: Among the 3244 patients consulted for a surgical pathology, 73 (2.25%) had a GOGE. The mean age of patients was 48.81 years with extremes of 19 and 74 years. The majority of patients were male. The main reasons for consultation were scrotal swelling (41.1%) and perineal pain. More than half (53.1%) consulted between 8 and 15 days. Gangrene mainly affected the scrotum, perineum, and in some cases, the penis and pelvis. Diabetes was the most common risk factor (50.68%), followed by alcoholism (23.29%) and acute kidney injury (15.07%). Urological causes were the most common with more than half of the cases (61.64%). All patients underwent surgical debridement. Triple broad-spectrum antibiotic therapy combining a 3rd generation cephalosporin, an Imidazole and an Aminoside was initiated in the majority of cases (93.15%). Nearly half of the patients were treated the day after their admission. The cure rate was 89.04%, with a mortality rate of 6.85%. Major erectile dysfunction and dysuria were found in 35.61% and 34.25% of patients, respectively. Conclusion: Early therapeutic management, well-codified treatment and a multidisciplinary care pathway could improve patients' prognostic factors. Our study suggests that patients surviving after gangrene of the external genitalia show a marked and continuous impairment in their overall urological and sexual quality of life. VL - 9 IS - 2 ER -
Urology Department, The University Hospital Center (CHU), Cocody-Abidjan, Côte d'Ivoire
Urology Department, The University Hospital Center (CHU), Cocody-Abidjan, Côte d'Ivoire
Urology Department, The University Hospital Center (CHU), Cocody-Abidjan, Côte d'Ivoire
Urology Department, The University Hospital Center (CHU), Cocody-Abidjan, Côte d'Ivoire
Urology Department, The University Hospital Center (CHU), Cocody-Abidjan, Côte d'Ivoire
Information