Emphysematous cystitis (EC) is a rare form of urinary tract infection characterized by the spontaneous formation of air which is floated in the bladder and/or bladder wall. The sometimes severe prognosis depends on the delay in management. We describe the case of a patient followed for multiple myeloma undergoing chemotherapy who presented with emphysematous cystitis in this context of immunosuppression, with a narrative review of the literature. A 77-year-old woman patient with multiple myeloma in the palliative stage of chemotherapy was brought to the emergency room by her family for unusual asthenia and diffuse pain that had been developing for 72 hours. The interview did not reveal any lower urinary tract symptoms or fever. The biological assessment revealed a biological inflammatory syndrome with a C-Reactiv Protein of 300 mg/l and hyperleukocytosis of 14,000 elements /mm3. The urine dipstick was positive for leukocytes and nitrites. In view of this major biological inflammatory syndrome with no real clinical urinary point of call, a thoraco-abdomino-pelvic CT scan without injection of contrast medium was carried out as a matter of urgency and revealed the presence of air bubbles in the bladder wall and the underlying soft tissues. Treatment consisted of trans-urethral bladder catheterisation and double antibiotic therapy with amiklin and imipenem. Cytobacteriological examination of the urine revealed quinolone-sensitive Escherichia coli at day 4, leading to a switch from TIENAM to ofloxacin for 14 days. A follow-up CT scan at day 7 showed regression of aerial infiltration of the bladder wall and extra-vesical aerial images. Emphysematous cystitis is a rare form of acute inflammation of the bladder mucosa and underlying muscularis. The clinical picture of emphysematous cystitis is often aspecific. The prognosis depends on the early diagnosis and the quality of the management, i.e. bladder drainage and broad-spectrum probabilistic antibiotic therapy.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Emphysematous Cystitis (EC) is a rare form of lower urinary tract infection, characterized by gas formation in the bladder wall and/or bladder lumen. It is an infection secondary to aerobic and anaerobic bacterial proliferation in the bladder
[1]
Egawa S, Utsunomiya T, Uchida T, et al. Emphysematous pyelo-nephritis, ureteritis, and cystitis in a diabetic patient. Urol Int 1994; 52: 176-8.
may also be associated with emphysematous cystitis. Prognosis is sometimes dismal, worsened by delays in diagnosis and management.
We present the case of a 77-year-old female patient, under chemotherapy for multiple myeloma, diagnosed with emphysematous cystitis in a context of immunosuppression. We also reviewed the litterature concerning the clinical presentation, diagnosis, and management of emphysematous cystitis.
2. Case Presentation
2.1. Patient Information
We hereby present the case of a 77-year-old female patient, under chemotherapy for multiple myeloma, brought by her family to the Emergency Department of the Centre Hospitalier de Martigues, Martigues, France, for a 3-day-history of unusual fatigue and diffuse body aches. The patient denies any fever, or any respiratory, gastro-intestinal, or urinary tract symptoms.
2.2. Clinical Findings
On physical examination, the patient was oriented, afebrile, and hemodynamically stable. Cardiorespiratory examination was normal, and the abdomen was non-distended, soft, and non-tender, with no palpable masses or hernias. There was no abdominal wall, perineal, or inner thigh crepitus.
2.3. Diagnostic Assessment
Her blood tests revealed an elevated C-Reactive Protein at 300 mg/L, leucocytosis with 14000 white blood cells/mm3, and a normal serum creatinine level with a normal glyceaemia level. Urine dipstick test was positive for leucocytes and nitrites. A chest-abdomen-pelvis CT-scan without IV contrast was then ordered to look for an infectious etiology, and showed multiple air pockets in the bladder wall and in the soft tissues of the perineum and inner thighs. Therefore, the diagnosis of emphysematous cystitis, with extension into the adjacent soft tissues was made.
2.4. Therapeutic
After consulting the urology team, treatment was initiated, and consisted of bladder drainage with an indwelling transurethral bladder catheter, and broad-spectrum empiric intravenous antibiotics with Imipenem 500 mg every 8 hours and 2 doses of Amikacin 15mg/Kg.
2.5. Follow-up and Outcome
Clinical evolution was favourable, with absence of fever, and lack of cutaneous signs of soft tissue infection and crepitus, and a decrease in inflammatory markers on subsequent blood tests. Antibiotic treatment was deescalated to Ofloxacin 200 mg every 12 hours on day 4, after urine culture came positive for sensitive Escherichia coli. Antibiotics were continued for a total of 21 days. A follow-up CT-scan done on day 7 of antibiotic treatment showed a marked regression of bladder wall and soft tissue pneumatosis.
3. Discussion
EC is a rare clinical entity characterized by air pockets in the bladder wall secondary to bacterial fermentation
[7]
Quint HJ, Drach GW, Rappaport WD, Hoffmann CJ. Emphysematous cystitis: a review of the spectrum of disease. J Urol. 1992 Jan; 147(1): 134-7.
. The first case of pneumaturia was reported by E. L. Keyes in 1882, and H. Bailey described emphysematous cystitis on animal and Human autopsy specimens in 1961
[8]
Keyes EL. Pneumaturia. Med News. 1882; 14: 675-8.
[8]
. Two hundred and fifty-seven cases were later reported in the literature between 1963 and 2013
[2]
Grupper M, Kravtsov A, Potasman I. Emphysematous cystitis: illustrative casereport and review of literature. Medicine 2007; 86(1): 47-53.
Many pathophysiologic hypotheses exist to explain the development of emphysematous cystitis. In diabetic patients, urinary stasis secondary to neurogenic bladder dysfunction, may favor bacterial proliferation in the bladder. The glucose present in the urine serves as a substrate for the bacteria to produce carbon dioxide. The fermentation capacity of these bacteria accounts for their role in the development of emphysematous cystitis. The fact that emphysematous cystitis may develop in non-diabetic patients may be explained by the fact that lactose and albumin in the urine may also be used as fermentation substrates by gas-producing bacteria. This carbon dioxide production may lead to an increase in intravesical pressure and subsequent bladder wall infracts, which constitute a proper medium for bacterial proliferation due to decreased tissue oxygenation, therefore creating a vicious cycle
[12]
Yang WH, Shen NC. Gas forming infection of the urinary tract: an investigation of fermentation as a mechanism. J Urol 1990; 143: 960-4.
. Other micro-organisms, namely facultative anaerobic bacteria like Enterobacter and Proteus mirablilis, or strictly anaerobic organisms like Clostridium perfringens, may also be encountered. Rare cases of emphysematous cystitis caused by Candida albicans have also been reported
[13]
Bartkowski DP, Lanesky JR. Emphysematous prostatis and cystitis secondary to Candida albicans. J Urol 1988; 139: 1063-5.
Clinical presentation of EC is highly variable and often atypical regardless of the severity of inflammation, as was the case for our patient, and this is responsible for the delay in diagnosis. Abdominal pain, which is found in 80% of cases, is the most common presenting symptom, followed by irritative voiding symptoms (dysuria, burning, urgency) in 50% of cases. Pneumaturia is found in 7 to 10% of cases
[2]
Grupper M, Kravtsov A, Potasman I. Emphysematous cystitis: illustrative casereport and review of literature. Medicine 2007; 86(1): 47-53.
. According to Thomas et al, patients were asymptomatic and diagnosed on abdominal imaging done for other purposes, in 7% of cases. Others may even present in septic shock.
Therefore, because of its highly variable, and non-specific clinical presentation, the diagnosis of emphysematous cystitis remains a radiological one, with an increasing prevalence over the last decades, as a consequence of improvements in imaging quality and access
[11]
Thomas AA, Lane BR, Thomas AZ et al (2007) Emphysematous cystitis: a review of 135 cases. BJU international, 100: 17-20.
Abdomen-pelvis CT-scan is the imaging study of choice to confirm the diagnosis (by showing gas pockets in the bladder wall and/or lumen), to assess the severity and extension of the disease process, and to look for concomitant upper urinary tract involvement. It also allows to rule out other causes of pneumaturia, such as fistulas between the bladder and the vagina or the bladder and the bowel
[14]
Grayson DE, Abbott RM, Levy AD, Sherman PM. Emphysematous infections of the abdomen and pelvis: a pictorial review. Radiographics 2002; 22: 543-61.
. An abdominal x-ray may show a curvilinear radiolucency delineating the bladder wall, with or without intraluminal air. Diagnosis may be suspected on ultrasound, with hyperechoic islets and acoustic shadows in the thickened bladder wall, with or without intraluminal polypoid islets. However, abdominal x-rays and ultrasound are not recommended for the diagnosis of emphysematous cystitis
[2]
Grupper M, Kravtsov A, Potasman I. Emphysematous cystitis: illustrative casereport and review of literature. Medicine 2007; 86(1): 47-53.
The main factors that determine prognosis are timely diagnosis and treatment. Delayed diagnosis and/or treatment may lead to extension into the ureters or renal parenchyma.
The main complications of EC are necrotizing cystitis, emphysematous pyelonephritis, septicemia, and subcutaneous emphysema
. In our case, the clinical presentation was that of an emphysematous cystitis with extension into adjacent soft tissues.
Management of EC is three-fold, with empiric road-spectrum double intravenous antibiotic treatment which is then tailored according to the antibiogram, bladder drainage and bladder rest using an indwelling bladder catheter, and tight glycemic control in diabetic patients. In severe cases, such as those with renal involvement, bladder necrosis, or bladder rupture, or in patients with poor response to conservative therapy, surgical intervention, with partial cystectomy, or even cystectomy and debridement, is indicated
[16]
Barkia A1, Larbi N, Mnif A, Chebil M, Ayed M. Emphysematous cystitis: apropos of 2 cases. Prog Urol 1997 Jun; 7(3): 468-70.
[16]
.
Outcomes are usually favourable following medical treatment, marked by a decrease in inflammatory markers and tissue pneumatosis, as was the case in our patient.
There is no consensus concerning treatment duration, which varies between 3 and 6 weeks in the literature
Bailey H. Cystitis emphysematosa: 19 cases with intraluminal and interstitial collections of gas. Am J Roentgenol Radium Ther Nucl Med. 1961; 86: 850-62.
[10]
Amano M, Shimizu T (2014) Emphysematous cystitis: a review of the literature. Internal Medicine, 53: 79-82.
, and prognosis depends on timely diagnosis and treatment.
4. Conclusion
Emphysematous cystitis is a rare form inflammation of the bladder mucosa and underlying musculosa. The clinical presentation is often non-specific, and diagnosis relies on urgent abdomen-pelvis CT-scan. Prognosis depends on early diagnosis and treatment initiation with bladder drainage and empiric, broad-spectrm IV antibiotics.
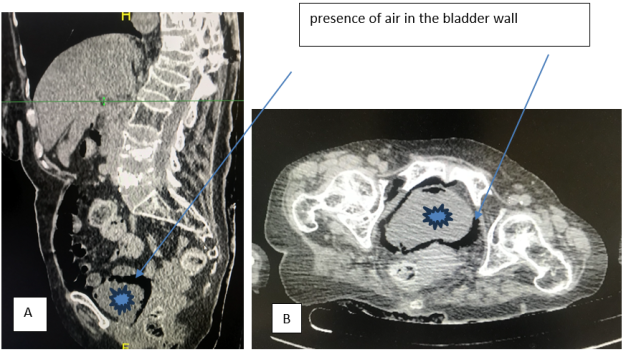
Figure 1. Emphysematous Cystitis. A: Sagittal section and B: Axial section of an abdomen-pelvis CT-scan without IV contrast. Presence of air pockets in the bladder wall, bladder lumen, and extravesical soft tissues, suggestive of emphysematous cystitis (bladder ).
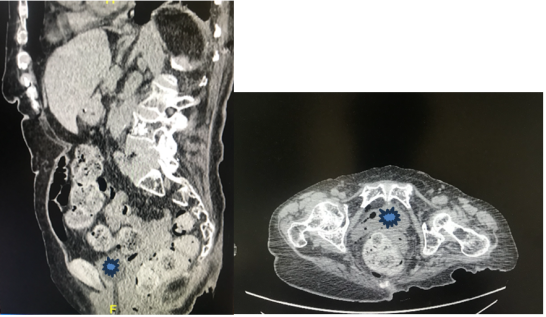
Figure 2. Emphysematous cystitis: A and B. Frontal and horizontal section of non-injected abdominal-pelvic CT scan. Progressive control at day 7 of an emphysematous cystitis marked by a regression of the aerial infiltration of the bladder wall as well as of the extra bladder aerial images (bladder ).
Bailey H. Cystitis emphysematosa: 19 cases with intraluminal and interstitial collections of gas. Am J Roentgenol Radium Ther Nucl Med. 1961; 86: 850-62.
[10]
Amano M, Shimizu T (2014) Emphysematous cystitis: a review of the literature. Internal Medicine, 53: 79-82.
Ye, O. D., Tadrist, A., Pare, A., Elkhoury, E., Dicrocco, E., et al. (2026). Unusual Presentation of Emphysematous Cystitis: A Case Report and Review of the Literature. International Journal of Clinical Urology, 10(1), 48-52. https://doi.org/10.11648/j.ijcu.20261001.19
Ye, O. D.; Tadrist, A.; Pare, A.; Elkhoury, E.; Dicrocco, E., et al. Unusual Presentation of Emphysematous Cystitis: A Case Report and Review of the Literature. Int. J. Clin. Urol.2026, 10(1), 48-52. doi: 10.11648/j.ijcu.20261001.19
Ye OD, Tadrist A, Pare A, Elkhoury E, Dicrocco E, et al. Unusual Presentation of Emphysematous Cystitis: A Case Report and Review of the Literature. Int J Clin Urol. 2026;10(1):48-52. doi: 10.11648/j.ijcu.20261001.19
@article{10.11648/j.ijcu.20261001.19,
author = {Ouienababo Delphine Ye and Abel Tadrist and Abdoul-Karim Pare and Eliane Elkhoury and Eugenie Dicrocco and Sinaly Soare and Adama Ouattara and Harry Toledano},
title = {Unusual Presentation of Emphysematous Cystitis: A Case Report and Review of the Literature},
journal = {International Journal of Clinical Urology},
volume = {10},
number = {1},
pages = {48-52},
doi = {10.11648/j.ijcu.20261001.19},
url = {https://doi.org/10.11648/j.ijcu.20261001.19},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcu.20261001.19},
abstract = {Emphysematous cystitis (EC) is a rare form of urinary tract infection characterized by the spontaneous formation of air which is floated in the bladder and/or bladder wall. The sometimes severe prognosis depends on the delay in management. We describe the case of a patient followed for multiple myeloma undergoing chemotherapy who presented with emphysematous cystitis in this context of immunosuppression, with a narrative review of the literature. A 77-year-old woman patient with multiple myeloma in the palliative stage of chemotherapy was brought to the emergency room by her family for unusual asthenia and diffuse pain that had been developing for 72 hours. The interview did not reveal any lower urinary tract symptoms or fever. The biological assessment revealed a biological inflammatory syndrome with a C-Reactiv Protein of 300 mg/l and hyperleukocytosis of 14,000 elements /mm3. The urine dipstick was positive for leukocytes and nitrites. In view of this major biological inflammatory syndrome with no real clinical urinary point of call, a thoraco-abdomino-pelvic CT scan without injection of contrast medium was carried out as a matter of urgency and revealed the presence of air bubbles in the bladder wall and the underlying soft tissues. Treatment consisted of trans-urethral bladder catheterisation and double antibiotic therapy with amiklin and imipenem. Cytobacteriological examination of the urine revealed quinolone-sensitive Escherichia coli at day 4, leading to a switch from TIENAM to ofloxacin for 14 days. A follow-up CT scan at day 7 showed regression of aerial infiltration of the bladder wall and extra-vesical aerial images. Emphysematous cystitis is a rare form of acute inflammation of the bladder mucosa and underlying muscularis. The clinical picture of emphysematous cystitis is often aspecific. The prognosis depends on the early diagnosis and the quality of the management, i.e. bladder drainage and broad-spectrum probabilistic antibiotic therapy.},
year = {2026}
}
TY - JOUR
T1 - Unusual Presentation of Emphysematous Cystitis: A Case Report and Review of the Literature
AU - Ouienababo Delphine Ye
AU - Abel Tadrist
AU - Abdoul-Karim Pare
AU - Eliane Elkhoury
AU - Eugenie Dicrocco
AU - Sinaly Soare
AU - Adama Ouattara
AU - Harry Toledano
Y1 - 2026/03/26
PY - 2026
N1 - https://doi.org/10.11648/j.ijcu.20261001.19
DO - 10.11648/j.ijcu.20261001.19
T2 - International Journal of Clinical Urology
JF - International Journal of Clinical Urology
JO - International Journal of Clinical Urology
SP - 48
EP - 52
PB - Science Publishing Group
SN - 2640-1355
UR - https://doi.org/10.11648/j.ijcu.20261001.19
AB - Emphysematous cystitis (EC) is a rare form of urinary tract infection characterized by the spontaneous formation of air which is floated in the bladder and/or bladder wall. The sometimes severe prognosis depends on the delay in management. We describe the case of a patient followed for multiple myeloma undergoing chemotherapy who presented with emphysematous cystitis in this context of immunosuppression, with a narrative review of the literature. A 77-year-old woman patient with multiple myeloma in the palliative stage of chemotherapy was brought to the emergency room by her family for unusual asthenia and diffuse pain that had been developing for 72 hours. The interview did not reveal any lower urinary tract symptoms or fever. The biological assessment revealed a biological inflammatory syndrome with a C-Reactiv Protein of 300 mg/l and hyperleukocytosis of 14,000 elements /mm3. The urine dipstick was positive for leukocytes and nitrites. In view of this major biological inflammatory syndrome with no real clinical urinary point of call, a thoraco-abdomino-pelvic CT scan without injection of contrast medium was carried out as a matter of urgency and revealed the presence of air bubbles in the bladder wall and the underlying soft tissues. Treatment consisted of trans-urethral bladder catheterisation and double antibiotic therapy with amiklin and imipenem. Cytobacteriological examination of the urine revealed quinolone-sensitive Escherichia coli at day 4, leading to a switch from TIENAM to ofloxacin for 14 days. A follow-up CT scan at day 7 showed regression of aerial infiltration of the bladder wall and extra-vesical aerial images. Emphysematous cystitis is a rare form of acute inflammation of the bladder mucosa and underlying muscularis. The clinical picture of emphysematous cystitis is often aspecific. The prognosis depends on the early diagnosis and the quality of the management, i.e. bladder drainage and broad-spectrum probabilistic antibiotic therapy.
VL - 10
IS - 1
ER -
Ye, O. D., Tadrist, A., Pare, A., Elkhoury, E., Dicrocco, E., et al. (2026). Unusual Presentation of Emphysematous Cystitis: A Case Report and Review of the Literature. International Journal of Clinical Urology, 10(1), 48-52. https://doi.org/10.11648/j.ijcu.20261001.19
Ye, O. D.; Tadrist, A.; Pare, A.; Elkhoury, E.; Dicrocco, E., et al. Unusual Presentation of Emphysematous Cystitis: A Case Report and Review of the Literature. Int. J. Clin. Urol.2026, 10(1), 48-52. doi: 10.11648/j.ijcu.20261001.19
Ye OD, Tadrist A, Pare A, Elkhoury E, Dicrocco E, et al. Unusual Presentation of Emphysematous Cystitis: A Case Report and Review of the Literature. Int J Clin Urol. 2026;10(1):48-52. doi: 10.11648/j.ijcu.20261001.19
@article{10.11648/j.ijcu.20261001.19,
author = {Ouienababo Delphine Ye and Abel Tadrist and Abdoul-Karim Pare and Eliane Elkhoury and Eugenie Dicrocco and Sinaly Soare and Adama Ouattara and Harry Toledano},
title = {Unusual Presentation of Emphysematous Cystitis: A Case Report and Review of the Literature},
journal = {International Journal of Clinical Urology},
volume = {10},
number = {1},
pages = {48-52},
doi = {10.11648/j.ijcu.20261001.19},
url = {https://doi.org/10.11648/j.ijcu.20261001.19},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcu.20261001.19},
abstract = {Emphysematous cystitis (EC) is a rare form of urinary tract infection characterized by the spontaneous formation of air which is floated in the bladder and/or bladder wall. The sometimes severe prognosis depends on the delay in management. We describe the case of a patient followed for multiple myeloma undergoing chemotherapy who presented with emphysematous cystitis in this context of immunosuppression, with a narrative review of the literature. A 77-year-old woman patient with multiple myeloma in the palliative stage of chemotherapy was brought to the emergency room by her family for unusual asthenia and diffuse pain that had been developing for 72 hours. The interview did not reveal any lower urinary tract symptoms or fever. The biological assessment revealed a biological inflammatory syndrome with a C-Reactiv Protein of 300 mg/l and hyperleukocytosis of 14,000 elements /mm3. The urine dipstick was positive for leukocytes and nitrites. In view of this major biological inflammatory syndrome with no real clinical urinary point of call, a thoraco-abdomino-pelvic CT scan without injection of contrast medium was carried out as a matter of urgency and revealed the presence of air bubbles in the bladder wall and the underlying soft tissues. Treatment consisted of trans-urethral bladder catheterisation and double antibiotic therapy with amiklin and imipenem. Cytobacteriological examination of the urine revealed quinolone-sensitive Escherichia coli at day 4, leading to a switch from TIENAM to ofloxacin for 14 days. A follow-up CT scan at day 7 showed regression of aerial infiltration of the bladder wall and extra-vesical aerial images. Emphysematous cystitis is a rare form of acute inflammation of the bladder mucosa and underlying muscularis. The clinical picture of emphysematous cystitis is often aspecific. The prognosis depends on the early diagnosis and the quality of the management, i.e. bladder drainage and broad-spectrum probabilistic antibiotic therapy.},
year = {2026}
}
TY - JOUR
T1 - Unusual Presentation of Emphysematous Cystitis: A Case Report and Review of the Literature
AU - Ouienababo Delphine Ye
AU - Abel Tadrist
AU - Abdoul-Karim Pare
AU - Eliane Elkhoury
AU - Eugenie Dicrocco
AU - Sinaly Soare
AU - Adama Ouattara
AU - Harry Toledano
Y1 - 2026/03/26
PY - 2026
N1 - https://doi.org/10.11648/j.ijcu.20261001.19
DO - 10.11648/j.ijcu.20261001.19
T2 - International Journal of Clinical Urology
JF - International Journal of Clinical Urology
JO - International Journal of Clinical Urology
SP - 48
EP - 52
PB - Science Publishing Group
SN - 2640-1355
UR - https://doi.org/10.11648/j.ijcu.20261001.19
AB - Emphysematous cystitis (EC) is a rare form of urinary tract infection characterized by the spontaneous formation of air which is floated in the bladder and/or bladder wall. The sometimes severe prognosis depends on the delay in management. We describe the case of a patient followed for multiple myeloma undergoing chemotherapy who presented with emphysematous cystitis in this context of immunosuppression, with a narrative review of the literature. A 77-year-old woman patient with multiple myeloma in the palliative stage of chemotherapy was brought to the emergency room by her family for unusual asthenia and diffuse pain that had been developing for 72 hours. The interview did not reveal any lower urinary tract symptoms or fever. The biological assessment revealed a biological inflammatory syndrome with a C-Reactiv Protein of 300 mg/l and hyperleukocytosis of 14,000 elements /mm3. The urine dipstick was positive for leukocytes and nitrites. In view of this major biological inflammatory syndrome with no real clinical urinary point of call, a thoraco-abdomino-pelvic CT scan without injection of contrast medium was carried out as a matter of urgency and revealed the presence of air bubbles in the bladder wall and the underlying soft tissues. Treatment consisted of trans-urethral bladder catheterisation and double antibiotic therapy with amiklin and imipenem. Cytobacteriological examination of the urine revealed quinolone-sensitive Escherichia coli at day 4, leading to a switch from TIENAM to ofloxacin for 14 days. A follow-up CT scan at day 7 showed regression of aerial infiltration of the bladder wall and extra-vesical aerial images. Emphysematous cystitis is a rare form of acute inflammation of the bladder mucosa and underlying muscularis. The clinical picture of emphysematous cystitis is often aspecific. The prognosis depends on the early diagnosis and the quality of the management, i.e. bladder drainage and broad-spectrum probabilistic antibiotic therapy.
VL - 10
IS - 1
ER -