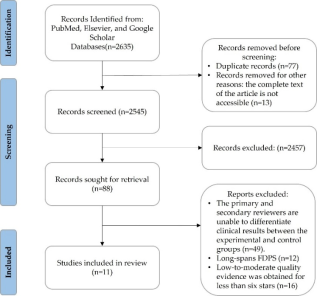
This study utilized the PRISMA 2020 framework alongside the Newcastle-Ottawa Scale (NOS) assessment tool during the screening process to conduct a systematic review of the fracture rates of zirconia (ZrO2) ceramic crowns in clinical practice. The primary objective was to investigate the factors influencing to the failure of zirconia ceramic crowns. The literature search employed targeted keywords including veneered fixed dental prostheses, zirconia, and all-ceramic single crowns. Inclusion criteria encompassed randomized controlled trials (RCTs) and cohort studies with a minimum follow-up duration of three years and at least 20 cases. Non-clinical reports and those exclusively addressing long-span fixed dental prostheses were excluded from the analysis. Of the eleven high-quality reports selected, only three reported crown fracture rates consistent with the clinically recommended threshold of 4.4%. To mitigate fractures in ZrO2 ceramic crowns used in dental restorations, precision is essential in both research and clinical practice. Multiple factors influence fracture incidence in fixed dental prostheses, including ceramic material thickness, connector dimensions, pontic span, type of cementation, and ceramic surface treatment. Preventative strategies focus on reducing occlusal overload by narrowing the occlusal table, decreasing cusp inclination, modifying load direction, minimizing non-axial forces, and selecting lighter occlusal contacts. Additionally, the integration of screw access channels and mechanical circulation in implant-supported prostheses may lower average fracture loads. Lastly, ensuring the precise alignment of the screw access channel at the center of the occlusal surface is critical to avoid off-center occlusal contacts during subsequent evaluations and measurements.
| Published in | International Journal of Dental Medicine (Volume 12, Issue 1) |
| DOI | 10.11648/j.ijdm.20261201.11 |
| Page(s) | 1-14 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
PRISMA 2020, Newcastle–Ottawa Scale, Fracture Rates, Fixed Dental Prostheses (FDPs), Zirconia (ZrO2), All-ceramic Single Crown, Endocrown
Article Resources | Selection | Comparability of cohorts on the basis of the design or analysis 1) | Outcome | Total Score | |||||
|---|---|---|---|---|---|---|---|---|---|
Representativeness of the exposed cohort | Selection of the non exposed cohort | Ascertainment of exposure | Demonstration that outcome of interest was not present at start of study | a) study controls * b) study controls for any additional factor | Assessment of outcome | Was follow-up long enough for outcomes to occur (≥ 3years) | Adequacy of follow up of cohorts | ||
Esquivel-pshaw et al. [3 3] | | | | - | | | | | 8 |
Sailer et al. [3 4] | | | | | | | | | 9 |
Nicolaisen et al. [3 5] | | | | | | | | | 9 |
Naenni et al. [ 36] | | | | | | | | | 9 |
Esquivel-Upshaw et al. [ 37] | | | | - | | | | | 8 |
Pelaez et al. [3 1] | | | | - | | | | | 8 |
Gardell et al. [2 4] | | | | | | | | | 9 |
Sulaiman et al. [ 38] | | | | | - | | | | 7 |
De Angelis et al. [ 37] | | | | | | | | | 9 |
Monaco et al. [4 0] | | | | | - | | | | 7 |
Güncü et al. [4 1] | | | | | | | | | 9 |
Authors and year of article publication | First control factor or other control factors |
|---|---|
Esquivel-Upshaw et al. [3 3] (2020) | (1) Control veneer ceramic thickness, connector radius of curvature, and connector height. (2) The absence of active caries, periodontal disease, or the depth of periodontal pockets should not exceed 4 mm. (3) The participant exhibits a deficiency of at least three teeth in the posterior region. |
Sailer et al. [3 4] (2018) | (1) The participant does not have periodontal disease and shows no apparent signs of bruxism. (2) The same treatment procedures are used for both types of FDPs after the clinical procedures. for metal–ceramic reconstructions. |
Nicolaisen et al. [3 5] (2016) | (1) The need to replace the second molar or the first molar. (2) Medium to large dental fillings in teeth neighboring edentulous areas. (3) The vertical dimensions of the treatment site allow for a 2 mm reduction in bite while maintaining a height of 4 mm. (4) Bleeding should not occur during periodontal probing, and the depth of periodontal pockets should not exceed 4 mm. |
Naenni et al. [ 36] (2015) | (1) The participants were periodontally healthy, as indicated by plaque indices and bleeding on probing below 20%. (2) There are no apparent signs or symptoms of bruxism or clenching. (3) The abutment teeth is in need of reconstruction. (4) Inadequate remaining tooth structure. |
Esquivel-Upshaw et al. [ 37] (2014) | (1) The absence of active caries, periodontal disease, or the depth of periodontal pockets should not exceed 4 mm. (2) The participant exhibits a deficiency of at least three teeth in the posterior region. (3) The presence of sufficient bone height (>6 mm) and width in the intended implant sites is essential. (4) The interocclusal distance should be sufficient to accommodate the prosthesis, with a minimum of 6 mm. (5) The combined thickness of the core framework and veneer ceramic is 2.0 mm. |
Pelaez et al. [3 1] (2012) | (1) There is no high incidence of dental caries, no active periodontal disease, and no bruxism. (2) Vital abutments or abutments with sufficient endodontic treatment; the abutments had not been previously fitted with crowns. (3) Abutments free of periodontal disease, exhibiting no evidence of bone resorption or periapical pathology. (4) The occlusion is stable, and the dentition in the opposing arch is natural. |
Gardell et al. [2 4] (2021) | (1) Absence of high caries activity or active destructive periodontal disease. (2) There is no documented history of recurrent fractures in dental fillings or other restorations. (3) The tooth was prepared with an occlusal reduction of 1.5 to 2.0 mm, an axial reduction of 1.5 mm, and a cervical shape featuring a 120° chamfer with a depth of 1.0 mm. |
Sulaiman et al. [ 38] (2020) | - |
De Angelis et al. [ 39] (2020) | (1) Participants must be edentulous for at least 4 months and aged over 18 years. (2) The full-mouth bleeding score is less than 15%. (3) Absence of temporomandibular disorders, bruxism, clenching, or periodontal disease. (4) Non-alcoholism and smoking fewer than 10 cigarettes per day. (5) The software sets the tightness of interproximal and occlusal contacts at 25 μm. |
Monaco et al. [4 0] (2017) | - |
Güncü et al. [4 1] (2016) | (1) Loss of upper or lower premolar or molar in one quadrant, with a need for crown fabrication for the symmetrical vital or devital tooth in the same jaw. (2) There are no contraindications for implant treatment. (3) Low caries prevalence and natural dentition of opposing teeth. (4) There is no evidence of active bone resorption, furcation involvement, or periapical pathology. (5) The ZrO2 framework should have a thickness of at least 0.5 mm, while the veneer thickness layer should range from 1.0 to 2.0 mm. |
First author | No. failures of experimental group (E) | Sample size of experimental group | Chipping or fracture rate (%) | No. failures of control group (C) | Sample size of control group | Chipping or fracture rate (%) | Materials and usage of dental crowns |
|---|---|---|---|---|---|---|---|
Esquivel [3 3] | 16 | 65 | 24.6 | 11 | 64 | 17.2 | E- IPS ZirPress on IPS e.max ZirCAD / Veneered FDP C-PdAuAg alloy on IPS INLine POM/ Veneered FDP |
Sailer [3 4] | 11 | 29 | 37.9 | 8 | 24 | 33.3 | E- Cercon-Ceram-S on Ceron /Veneered FDP C- Duceram-Plus on gold-alloy /Veneered FDP |
Nicolaisen [3 5] | 5 | 17 | 29.4 | 3 | 17 | 17.6 | E- Vita VM9 on BeCe® CAD Zirkon+/ Veneered FDP C- Vita VM13 on AuPt Alloy /Veneered FDP |
Naenni [ 36] | 8 | 18 | 44.4 | 4 | 18 | 22.2 | E- IPS e.max ZirPress on IPS e.max ZirCAD / Veneered FDP C- (1) IPS e.max Ceram ZirLiner, (2) IPS e.max Ceram Margin, (3) IPS e.max Ceram Dentin, (4) Enamel on IPS e.max ZirCAD/ Veneed FDP |
Esquivel [ 37] | 6 | 41 | 14.6 | 7 | 48 | 14.6 | E- IPS ZirPress on IPS e.max ZirCAD / Veneered FDP C- PdAuAg alloy on IPS INLine POM / Veneered FDP |
Pelaez [3 1] | 2 | 20 | 10.0 | 0 | 20 | 0.0 | E- Lava Ceram on Lava/ Veneered FDP C- Vita VM13 on CoCr alloy/Veneered FDP |
Gardell* [2 4] | 0 | 29 | 0.0 | 0 | 30 | 0.0 | T- IPS e.max Ceram on IPS e.max CAD / posterior crown C- Lava 3M / posterior crown |
Sulaiman* [ 38] | 416 | 77411 | 0.54 | 849 | 30036 | 2.83 | E-ZrO2 / monolithic single crown C-ZrO2 on ZrO2 / layered single crown |
Sulaiman* [ 38] | 320 | 16437 | 1.95 | 252 | 13060 | 1.93 | E-ZrO2 / monolithic FDP C-ZrO2 on ZrO2 / layered FDP |
Sulaiman* [ 38] | 72 | 5854 | 1.23 | 433 | 20712 | 2.09 | E-ZrO2 / monolithic anterior restoration C-ZrO2 on ZrO2 / layered anterior restoration |
Sulaiman* [ 38] | 664 | 87994 | 0.75 | 668 | 22384 | 2.98 | E-ZrO2 / monolithic posterior restoration C-ZrO2 on ZrO2 / layered posterior restoration |
De Angelis* [ 39] | 0 | 19 | 0.0 | 0 | 19 | 0.0 | E-IPS e.max CAD/ implant-supported monolithic single crown C-inCoris TZI/ implant-supported monolithic single crown |
Monaco [4 0] | 2 | 40 | 5.0 | 3 | 45 | 6.7 | E- PoM on d.SIGN 91/veneered single crown C-ZirPress on ZirCad/veneered single crown |
Güncü [4 1] | 2 | 24 | 8.3 | 1 | 24 | 4.2 | E-Vita VM9 on Lava/implant-supported crown C- Vita VM9 on Lava/nature tooth-supported crown |
PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
NOS | Newcastle-Ottawa Scale |
RCTs | Randomized Controlled Trials |
FDPs | Fixed Dental Prostheses |
ZrO2 | Zirconium Dioxide |
CEREC | Chairside Economical Restoration of Esthetic Ceramics |
Y-TZP | Yttria-Stabilized Tetragonal Zirconia Polycrystal |
CASP | Critical Appraisal Skills Programme |
CEBM | Oxford Centre for Evidence-Based Medicine |
SIGN 50 | Scottish Intercollegiate Guidelines Network |
JBI | Joanna Briggs Institute |
CC | Ceramic–Ceramic |
MC | Metal–Ceramic |
E | Number Failures of Experimental Group |
C | Number Failures of Control Group |
TZI | Translucent Zirconia Ceramic Blocks for inLab |
CAD | Computer-Aided Design |
| [1] | Munn, Z., et al., Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol, 2018. 18(1): p. 143. |
| [2] | Page, M. J., et al., The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ, 2021. 372: p. n71. |
| [3] | Tawfik, G. M., et al., A step by step guide for conducting a systematic review and meta-analysis with simulation data. Trop Med Health, 2019. 47: p. 46. |
| [4] | Norris, J. M., et al., A Modified Newcastle-Ottawa Scale for Assessment of Study Quality in Genetic Urological Research. Eur Urol, 2021. 79(3): p. 325-326. |
| [5] | Wells, G., et al., The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. 2009, Ottawa Hospital Research Institute. |
| [6] | Xu, A., et al., Peri-Implantitis in Relation to Titanium Corrosion: Current Status and Future Perspectives. Journal of Bio- and Tribo-Corrosion, 2022. 8(2): p. 46. |
| [7] | Smith, B. G. and J. E. Cardwell, One visit ceramic restorations made at the chairside: the CEREC machine. Restorative Dent, 1989. 5(3): p. 60-5. |
| [8] | Bona, A. D., O. E. Pecho, and R. Alessandretti, Zirconia as a Dental Biomaterial. Materials (Basel), 2015. 8(8): p. 4978-4991. |
| [9] | Larsson, C. and P. Vult von Steyern, Five-year follow-up of implant-supported Y-TZP and ZTA fixed dental prostheses. A randomized, prospective clinical trial comparing two different material systems. Int J Prosthodont, 2010. 23(6): p. 555-61. |
| [10] | Zhang, Y., I. Sailer, and B. R. Lawn, Fatigue of dental ceramics. J Dent, 2013. 41(12): p. 1135-47. |
| [11] | CASP. Establishment Of CASP. 2023; Available from: |
| [12] | CASP. Critical Appraisal Checklists. 2023; Available from: |
| [13] | CEMB. Our history. 2023; Available from: |
| [14] | Burns, P. B., R. J. Rohrich, and K. C. Chung, The levels of evidence and their role in evidence-based medicine. Plast Reconstr Surg, 2011. 128(1): p. 305-310. |
| [15] | Fearns, N., et al., User testing of a Scottish Intercollegiate Guideline Network public guideline for the parents of children with autism. BMC Health Serv Res, 2022. 22(1): p. 77. |
| [16] | NHS. Scottish Intercollegiate Guidelines Network: A guideline developers' handbook (SIGB 50). 2011; Available from: |
| [17] | JBI. JBI EBP Database Guide. 2023. |
| [18] | Jadad, A. R., et al., Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials, 1996. 17(1): p. 1-12. |
| [19] | Oremus, M., et al., Interrater reliability of the modified Jadad quality scale for systematic reviews of Alzheimer's disease drug trials. Dement Geriatr Cogn Disord, 2001. 12(3): p. 232-6. |
| [20] | Hempel, S., et al., AHRQ Methods for Effective Health Care, in Empirical Evidence of Associations Between Trial Quality and Effect Size. 2011, Agency for Healthcare Research and Quality (US): Rockville (MD). |
| [21] | Dhima, M., et al., Practice-based clinical evaluation of ceramic single crowns after at least five years. J Prosthet Dent, 2014. 111(2): p. 124-30. |
| [22] | Pjetursson, B. E., et al., A systematic review of the survival and complication rates of implant-supported fixed dental prostheses (FDPs) after a mean observation period of at least 5 years. Clin Oral Implants Res, 2012. 23 Suppl 6: p. 22-38. |
| [23] | Wang, X., et al., A systematic review of all-ceramic crowns: clinical fracture rates in relation to restored tooth type. Int J Prosthodont, 2012. 25(5): p. 441-50. |
| [24] | Gardell, E., C. Larsson, and P. V. von Steyern, Translucent Zirconium Dioxide and Lithium Disilicate: A 3-Year Follow-up of a Prospective, Practice-Based Randomized Controlled Trial on Posterior Monolithic Crowns. Int J Prosthodont, 2021. 34(2): p. 163-172. |
| [25] | Laass, A., et al., Randomized Controlled Clinical Trial of All-Ceramic Single-Tooth Implant Reconstructions Using Modified Zirconia Abutments: Results at 5 Years After Loading. Int J Periodontics Restorative Dent, 2019. 39(1): p. 17-27. |
| [26] | Matta, R. E., et al., Ten-year clinical performance of zirconia posterior fixed partial dentures. J Oral Rehabil, 2022. 49(1): p. 71-80. |
| [27] | Scherrer, S. S., et al., Incidence of fractures and lifetime predictions of all-ceramic crown systems using censored data. Am J Dent, 2001. 14(2): p. 72-80. |
| [28] | Alenezi, A. and S. Aloqayli, Technical complications with tooth-supported fixed dental prostheses (FDPs) of different span lengths: an up to 15-year retrospective study. BMC Oral Health, 2023. 23(1): p. 393. |
| [29] | Schmitter, M., et al., Clinical performance of long-span zirconia frameworks for fixed dental prostheses: 5-year results. J Oral Rehabil, 2012. 39(7): p. 552-7. |
| [30] | Spitznagel, F. A., et al., Clinical outcomes of all-ceramic single crowns and fixed dental prostheses supported by ceramic implants: A systematic review and meta-analyses. Clin Oral Implants Res, 2022. 33(1): p. 1-20. |
| [31] | Pelaez, J., et al., A four-year prospective clinical evaluation of zirconia and metal-ceramic posterior fixed dental prostheses. Int J Prosthodont, 2012. 25(5): p. 451-8. |
| [32] | Konstantinidis, I. K., et al., Prospective evaluation of zirconia based tooth- and implant-supported fixed dental prostheses: 3-year results. J Dent, 2015. 43(1): p. 87-93. |
| [33] | Esquivel-Upshaw, J. F., et al., Factors influencing the survival of implant-supported ceramic-ceramic prostheses: A randomized, controlled clinical trial. J Dent, 2020. 103s: p. 100017. |
| [34] | Sailer, I., et al., 10-year randomized trial (RCT) of zirconia-ceramic and metal-ceramic fixed dental prostheses. J Dent, 2018. 76: p. 32-39. |
| [35] | Nicolaisen, M. H., et al., Comparison of Metal-Ceramic and All-Ceramic Three-Unit Posterior Fixed Dental Prostheses: A 3-Year Randomized Clinical Trial. Int J Prosthodont, 2016. 29(3): p. 259-64. |
| [36] | Naenni, N., et al., A randomized controlled clinical trial of 3-unit posterior zirconia-ceramic fixed dental prostheses (FDP) with layered or pressed veneering ceramics: 3-year results. J Dent, 2015. 43(11): p. 1365-70. |
| [37] | Esquivel-Upshaw, J. F., et al., Fracture analysis of randomized implant-supported fixed dental prostheses. J Dent, 2014. 42(10): p. 1335-42. |
| [38] | Sulaiman, T. A., et al., Fracture rate of 188695 lithium disilicate and zirconia ceramic restorations after up to 7.5 years of clinical service: A dental laboratory survey. J Prosthet Dent, 2020. 123(6): p. 807-810. |
| [39] | De Angelis, P., et al., Monolithic CAD-CAM lithium disilicate versus monolithic CAD-CAM zirconia for single implant-supported posterior crowns using a digital workflow: A 3-year cross-sectional retrospective study. J Prosthet Dent, 2020. 123(2): p. 252-256. |
| [40] | Monaco, C., et al., Zirconia-based versus metal-based single crowns veneered with overpressing ceramic for restoration of posterior endodontically treated teeth: 5-year results of a randomized controlled clinical study. J Dent, 2017. 65: p. 56-63. |
| [41] | Güncü, M. B., et al., Comparison of implant versus tooth-supported zirconia-based single crowns in a split-mouth design: a 4-year clinical follow-up study. Clin Oral Investig, 2016. 20(9): p. 2467-2473. |
| [42] | Sulaiman, T. A., A. J. Delgado, and T. E. Donovan, Survival rate of lithium disilicate restorations at 4 years: A retrospective study. J Prosthet Dent, 2015. 114(3): p. 364-6. |
| [43] | Schärer, P., All-ceramic crown systems: clinical research versus observation in supporting claims. Signature, 1996: p. 1. |
| [44] | Mallmann, F., et al., Effect of screw-access hole and mechanical cycling on fracture load of 3-unit implant-supported fixed dental prostheses. J Prosthet Dent, 2018. 119(1): p. 124-131. |
APA Style
Chang, H. C., Chiu, G. S. C., Lan, T. H. (2026). A Clinical Assessment of Fracture Incidence in Zirconia Ceramic Crowns: A Systematic Review and Evaluation of Influencing Factors. International Journal of Dental Medicine, 12(1), 1-14. https://doi.org/10.11648/j.ijdm.20261201.11
ACS Style
Chang, H. C.; Chiu, G. S. C.; Lan, T. H. A Clinical Assessment of Fracture Incidence in Zirconia Ceramic Crowns: A Systematic Review and Evaluation of Influencing Factors. Int. J. Dent. Med. 2026, 12(1), 1-14. doi: 10.11648/j.ijdm.20261201.11
AMA Style
Chang HC, Chiu GSC, Lan TH. A Clinical Assessment of Fracture Incidence in Zirconia Ceramic Crowns: A Systematic Review and Evaluation of Influencing Factors. Int J Dent Med. 2026;12(1):1-14. doi: 10.11648/j.ijdm.20261201.11
@article{10.11648/j.ijdm.20261201.11,
author = {Han Chao Chang and Grace S. C. Chiu and Ting Hsun Lan},
title = {A Clinical Assessment of Fracture Incidence in Zirconia Ceramic Crowns: A Systematic Review and Evaluation of Influencing Factors},
journal = {International Journal of Dental Medicine},
volume = {12},
number = {1},
pages = {1-14},
doi = {10.11648/j.ijdm.20261201.11},
url = {https://doi.org/10.11648/j.ijdm.20261201.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijdm.20261201.11},
abstract = {This study utilized the PRISMA 2020 framework alongside the Newcastle-Ottawa Scale (NOS) assessment tool during the screening process to conduct a systematic review of the fracture rates of zirconia (ZrO2) ceramic crowns in clinical practice. The primary objective was to investigate the factors influencing to the failure of zirconia ceramic crowns. The literature search employed targeted keywords including veneered fixed dental prostheses, zirconia, and all-ceramic single crowns. Inclusion criteria encompassed randomized controlled trials (RCTs) and cohort studies with a minimum follow-up duration of three years and at least 20 cases. Non-clinical reports and those exclusively addressing long-span fixed dental prostheses were excluded from the analysis. Of the eleven high-quality reports selected, only three reported crown fracture rates consistent with the clinically recommended threshold of 4.4%. To mitigate fractures in ZrO2 ceramic crowns used in dental restorations, precision is essential in both research and clinical practice. Multiple factors influence fracture incidence in fixed dental prostheses, including ceramic material thickness, connector dimensions, pontic span, type of cementation, and ceramic surface treatment. Preventative strategies focus on reducing occlusal overload by narrowing the occlusal table, decreasing cusp inclination, modifying load direction, minimizing non-axial forces, and selecting lighter occlusal contacts. Additionally, the integration of screw access channels and mechanical circulation in implant-supported prostheses may lower average fracture loads. Lastly, ensuring the precise alignment of the screw access channel at the center of the occlusal surface is critical to avoid off-center occlusal contacts during subsequent evaluations and measurements.},
year = {2026}
}
TY - JOUR T1 - A Clinical Assessment of Fracture Incidence in Zirconia Ceramic Crowns: A Systematic Review and Evaluation of Influencing Factors AU - Han Chao Chang AU - Grace S. C. Chiu AU - Ting Hsun Lan Y1 - 2026/01/27 PY - 2026 N1 - https://doi.org/10.11648/j.ijdm.20261201.11 DO - 10.11648/j.ijdm.20261201.11 T2 - International Journal of Dental Medicine JF - International Journal of Dental Medicine JO - International Journal of Dental Medicine SP - 1 EP - 14 PB - Science Publishing Group SN - 2472-1387 UR - https://doi.org/10.11648/j.ijdm.20261201.11 AB - This study utilized the PRISMA 2020 framework alongside the Newcastle-Ottawa Scale (NOS) assessment tool during the screening process to conduct a systematic review of the fracture rates of zirconia (ZrO2) ceramic crowns in clinical practice. The primary objective was to investigate the factors influencing to the failure of zirconia ceramic crowns. The literature search employed targeted keywords including veneered fixed dental prostheses, zirconia, and all-ceramic single crowns. Inclusion criteria encompassed randomized controlled trials (RCTs) and cohort studies with a minimum follow-up duration of three years and at least 20 cases. Non-clinical reports and those exclusively addressing long-span fixed dental prostheses were excluded from the analysis. Of the eleven high-quality reports selected, only three reported crown fracture rates consistent with the clinically recommended threshold of 4.4%. To mitigate fractures in ZrO2 ceramic crowns used in dental restorations, precision is essential in both research and clinical practice. Multiple factors influence fracture incidence in fixed dental prostheses, including ceramic material thickness, connector dimensions, pontic span, type of cementation, and ceramic surface treatment. Preventative strategies focus on reducing occlusal overload by narrowing the occlusal table, decreasing cusp inclination, modifying load direction, minimizing non-axial forces, and selecting lighter occlusal contacts. Additionally, the integration of screw access channels and mechanical circulation in implant-supported prostheses may lower average fracture loads. Lastly, ensuring the precise alignment of the screw access channel at the center of the occlusal surface is critical to avoid off-center occlusal contacts during subsequent evaluations and measurements. VL - 12 IS - 1 ER -
National Center for Instrumentation Research, National Institutes of Applied Research, Hsinchu, Taiwan
Beethoven Orthodontic Center, Hsinchu, Taiwan
School of Dentistry, College of Dental Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan;Division of Prosthodontics, Department of Dentistry, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan
Information