Eosinophilic esophagitis (EoE) is a chronic, immune-mediated inflammatory condition that primarily affects the esophagus, characterized by the infiltration of eosinophils into the esophageal mucosa. This condition leads to symptoms of esophageal dysfunction, including dysphagia (difficulty swallowing), food impaction, and substernal pain. EoE is commonly associated with other atopic diseases such as asthma, allergic rhinitis, and eczema, and it predominantly affects young men with a history of atopy. Although it can occur in both children and adults, EoE is often underdiagnosed due to its subtle or nonspecific symptoms and its overlap with other gastrointestinal disorders. Rarely, EoE can present with severe complications, such as spontaneous esophageal perforation, known as Boerhaave’s syndrome, which is a life-threatening emergency. A typical diagnostic approach for EoE includes esophageal biopsies, which reveal significant eosinophilic infiltration, and endoscopic findings that may show structural changes such as strictures or rings in the esophagus. In some cases, the strictures can be severe, leading to difficulty swallowing and even food impaction. We present the case of a 36-year-old man from Addis Ababa, Ethiopia, who had been experiencing persistent substernal pain and dysphagia for eight years. His symptoms gradually worsened over time, prompting further investigation. Endoscopic examination revealed a severe lower esophageal stricture located approximately 35 cm from the incisors, and esophageal biopsies confirmed the presence of significant eosinophilic infiltration, consistent with a diagnosis of EoE. This case highlights the importance of considering EoE in patients with chronic dysphagia and substernal pain, especially those with a history of atopic conditions, and emphasizes the need for timely diagnosis and management to prevent complications.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Isolated eosinophilic infiltration in the esophageal mucosa is a defining feature of eosinophilic esophagitis (EoE). It rarely happened to adults and was mostly diagnosed in children. However, EoE has been rising quickly in adults lately, with a 3:1 male-to-female ratio with the majority of cases occurring in males
[1]
Clayton F, Peterson K. Eosinophilic Esophagitis. Gastrointest Endosc Clin N Am [Internet]. 2018 Jan [cited 2025 Mar 1]; 28(1): 1-14. Available from:
. For patients and healthcare systems, the rising incidence of eosinophilic esophagitis (EoE) poses a significant burden
[11]
Lucendo AJ, Santander C, Savarino E, Guagnozzi D, Pérez-Martínez I, Perelló A, et al. EoE CONNECT, the European Registry of Clinical, Environmental, and Genetic Determinants in Eosinophilic Esophagitis: rationale, design, and study protocol of a large-scale epidemiological study in Europe. Ther Adv Gastroenterol [Internet]. 2022 Jan [cited 2025 Mar 1]; 15: 17562848221074204. Available from:
The cause of EoE is not well understood. However, there is proof that EoE and other atopic illnesses are associated. Other atopic conditions include food allergies, atopic dermatitis, allergic rhinitis, and asthma affect up to 60% of people with EoE. Since there is substantial evidence of a family history of atopic disorders, there may be a genetic component in addition to the relationship with these conditions
[2]
Kiely K. Eosinophilic Esophagitis: A Case Study of a 12-Year-Old Boy. J Pediatr Health Care [Internet]. 2017 Sep 1 [cited 2025 Feb 27]; 31(5): 618-22. Available from:
Age has a significant impact on the variety of clinical manifestations of EoE. Nonspecific symptoms in young children include vomiting, stomach pain, and feeding issues such as prolonged mealtimes and underdevelopment. Food impaction and dysphagia are common in adults and adolescents
[3]
Ikobah JM, Ikwuagwu E, Ukpabio I, Ugbem T, Okechukwu OC, Ekanem E. Eosinophilic oesophagitis in a Nigerian adolescent: a case report. Pan Afr Med J [Internet]. 2024 Jan 4 [cited 2025 Feb 27]; 47(3). Available from:
Frontiers | Eosinophilic esophagitis improved by the discontinuation of sublingual immunotherapy for aeroallergens: a case report [Internet]. [cited 2025 Feb 27]. Available from:
In order to diagnose EoE, a clinicopathological diagnosis, esophageal symptoms such as dysphagia with endoscopic rings, furrows, stricture, crepe paper mucosa, concurrent atopic conditions, and eosinophils on histology with more than 15 eosinophils/high-power field must be present. Additionally, non-EoE disorders, such as Crohn's disease, hypereosinophilic syndrome, gastroesophageal reflux disease, connective tissue disease, infection, drug hypersensitivity, or Crohn's disease, must be evaluated
[4]
Eosinophilic esophagitis presenting with spontaneous esophageal rupture: a case report | Journal of Medical Case Reports | Full Text [Internet]. [cited 2025 Feb 27]. Available from:
Even though some individuals have seen spontaneous remission, EoE is most likely a chronic illness that requires treatment to avoid consequences
[2]
Kiely K. Eosinophilic Esophagitis: A Case Study of a 12-Year-Old Boy. J Pediatr Health Care [Internet]. 2017 Sep 1 [cited 2025 Feb 27]; 31(5): 618-22. Available from:
Esophageal stricture, food impaction, perforation, and malnourishment are among the complications that can arise from eosinophilic esophagitis, although cancer is not one of them. Patients with esophageal eosinophilia have been linked to a variety of concomitant disorders, such as Crohn's disease, celiac disease, and connective tissue diseases
[5]
Furuta GT, Katzka DA. Eosinophilic Esophagitis. N Engl J Med [Internet]. 2015 Oct 22 [cited 2025 Feb 27]; 373(17): 1640-8. Available from:
A 36-year-old man from Addis Ababa, Ethiopia, came to the gastrointestinal clinic after experiencing substernal pain and dysphagia for eight years. He had no prior history of allergies or atopic disorder in his family. There were no skin lesions found, and the physical examination was uneventful. The results of the CBC, liver function test, renal function test, and ultrasound were all unremarkable.
2.2. Diagnostic Workup
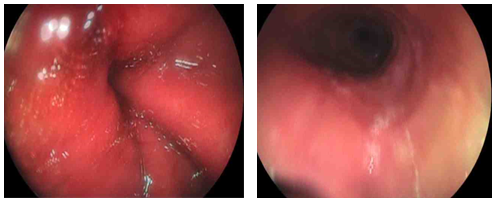
Esophagogastroduodenoscopy (EGD) revealed a normal oropharynx, and the upper esophageal sphincter (UES) was intubated without difficulty. Examination of the esophagus showed feline esophagus features, including multiple ring-like lesions, mucosal hyperemia, furrowing, and patchy whitish areas suggestive of eosinophilic abscesses. A tight esophageal stricture was identified in the lower esophagus, approximately 35 cm from the incisors. Although the scope initially required manipulation to pass through, further dilation was performed using a 15 mm bougie, resulting in a clear mucosal tear. Following dilation, the scope advanced easily into the stomach. The gastric mucosa, including the fundus, body, antrum, and cardia, appeared normal, with no evidence of masses, ulcers, or erosions. We took specimens at the lower and mid esophagus, respectively, under suspecting EoE.
Figure 1. Shows multiple rings in the proximal to mid esophagus, giving it the appearance of a trachea. Small whitish papules are also visible, representing eosinophilic abscesses.
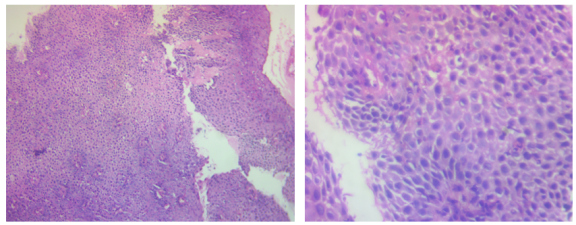
Based on the clinical, endoscopic and histological findings, the patient was diagnosed as EoE. And we confirmed the result by biopsies.
Figure 2. Stratified squamous epithelium with mild edema. Multiple intra epithelial eosinophilic are seen.
2.3. Treatment and Follow up
The patient underwent two sessions of endoscopic dilation, which resulted in a gradual improvement in his dysphagia and overall symptoms. Following the procedure, he was prescribed Fluticasone propionate as part of his ongoing management. A follow-up appointment was scheduled for one month to assess his progress and response to treatment.
3. Discussion
Eosinophilic esophagitis (EoE) is a long-term inflammatory disease that can lead to fibrotic remodeling and esophageal dysfunction
[13]
Johnson J, Dellon E, McCoy AN, Sun S, Jensen ET, Fodor AA, et al. Lack of association of the esophageal microbiome in adults with eosinophilic esophagitis compared with non-EoE controls. J Gastrointestin Liver Dis [Internet]. 2021 Mar 12 [cited 2025 Mar 1]; 30(1): 17-24. Available from:
. Due to its fast increasing incidence and prevalence, EoE has been a major source of esophageal morbidity within the last 20 years
[6]
Dowling PJ, Neuhaus H, Polk BI. The Role of the Environment in Eosinophilic Esophagitis. Clin Rev Allergy Immunol [Internet]. 2019 Dec [cited 2025 Mar 1]; 57(3): 330-9. Available from:
Since EoE was first identified as a distinct disease entity only 20 years ago, its incidence and prevalence have significantly increased. When EoE was initially identified in the 1990s, the disease incidence was only thought to be 0.4 instances per 100,000 year. Although there are currently differing estimates of disease incidence and prevalence, they are commonly stated as being approximately 10 cases per 100,000 year and 50-100 cases per 100,000
[7]
Jensen ET, Dellon ES. Environmental factors and eosinophilic esophagitis. J Allergy Clin Immunol [Internet]. 2018 Jul [cited 2025 Mar 1]; 142(1): 32-40. Available from:
It is unclear whether this represents heightened awareness and increased testing or a true escalation in incidence
[8]
D. Villalta, A.M. Baragiotta. Volume eosinophilic esophagitis from case report 310allasp1.pdf [Internet]. 2008 Nov [cited 2025 Feb 27]. Available from:
Most studies on eosinophilic esophagitis (EoE) in Africa are limited to case reports, resulting in a lack of comprehensive data on its overall prevalence across the continent but it still considered rare in Africa. Limited access to endoscopy and low awareness of EoE contribute to the likelihood that many cases remain undiagnosed
[3]
Ikobah JM, Ikwuagwu E, Ukpabio I, Ugbem T, Okechukwu OC, Ekanem E. Eosinophilic oesophagitis in a Nigerian adolescent: a case report. Pan Afr Med J [Internet]. 2024 Jan 4 [cited 2025 Feb 27]; 47(3). Available from:
EoE affects all age groups and is more common in adult males compared with adult females. Symptoms may be present for up to 4.5 years prior to the diagnosis
[9]
Sarah E, Jill O, Joseph V. Case 13: Eosinophilic Esophagitis [Internet]. Graphic 70915. UpToDate, 2023 [cited 2025 Feb 27]. Available from:
The exact pathophysiology of EoE is unknown. It is an allergy condition that is triggered by environmental and food allergens via both IgE- and non-IgE-mediated pathways. Age has a significant impact on the variety of clinical symptoms of EoE
[3]
Ikobah JM, Ikwuagwu E, Ukpabio I, Ugbem T, Okechukwu OC, Ekanem E. Eosinophilic oesophagitis in a Nigerian adolescent: a case report. Pan Afr Med J [Internet]. 2024 Jan 4 [cited 2025 Feb 27]; 47(3). Available from:
For our patients, the most prevalent symptom is dysphagia to solid meals. Up to 50% of individuals with EoE had a history of acute esophageal food impaction. EoE patients learn to adjust for dysphagia symptoms by chewing repeatedly, avoiding particular foods, eating slowly, and imbibing (drinking liquids with meals)
[9]
Sarah E, Jill O, Joseph V. Case 13: Eosinophilic Esophagitis [Internet]. Graphic 70915. UpToDate, 2023 [cited 2025 Feb 27]. Available from:
Clinical symptoms such as vomiting, abdominal pain, dysphagia, food impactions, odynophagia, and chest pain
[14]
Busing JD, Buendia M, Choksi Y, Hiremath G, Das SR. Microbiome in Eosinophilic Esophagitis—Metagenomic, Metatranscriptomic, and Metabolomic Changes: A Systematic Review. Front Physiol [Internet]. 2021 Sep 10 [cited 2025 Mar 1]; 12: 731034. Available from:
, endoscopic findings such as stacked circular rings, linear furrows, white specks (eosinophil microabscesses), and strictures, as well as histology demonstrating eosinophilic infiltration at the esophageal mucosa (≥ 15 eosinophilis per high power field), nonresponsiveness to high-dose proton pump inhibitors, and ruling out other causes of dysphagia, are used to diagnose EoE
[9]
Sarah E, Jill O, Joseph V. Case 13: Eosinophilic Esophagitis [Internet]. Graphic 70915. UpToDate, 2023 [cited 2025 Feb 27]. Available from:
Kim NI, Jo Y, Ahn SB, Son BK, Kim SH, Park YS, et al. A Case of Eosinophilic Esophagitis With Food Hypersensitivity. J Neurogastroenterol Motil [Internet]. 2010 Jul [cited 2025 Feb 27]; 16(3): 315-8. Available from:
Our patient experienced dysphagia and substernal discomfort for eight years. An upper endoscopy revealed the presence of circular rings along the esophageal mucosa, accompanied by white specks, both characteristic endoscopic findings of eosinophilic esophagitis (EoE). To confirm the diagnosis, a biopsy was performed, which reveals squamous epithelium exhibiting basal cell hyperplasia and intercellular edema. Notably, there is an infiltration of intraepithelial eosinophils, with a density of approximately 20 eosinophils per high-power field (HPF). No evidence of ulceration is observed, and there are no histological features suggestive of dysplasia. These findings are consistent with eosinophilic esophagitis and support the clinical diagnosis.
Based on these clinical, endoscopic, and histopathological findings, the patient was diagnosed with EoE.
EoE is treated with medication (such as corticosteroids) and nutrition. EoE recurs in over 90% of patients once therapy is finished, despite the fact that systemic or topical steroids successfully reduce clinical symptoms
[11]
Lucendo AJ, Santander C, Savarino E, Guagnozzi D, Pérez-Martínez I, Perelló A, et al. EoE CONNECT, the European Registry of Clinical, Environmental, and Genetic Determinants in Eosinophilic Esophagitis: rationale, design, and study protocol of a large-scale epidemiological study in Europe. Ther Adv Gastroenterol [Internet]. 2022 Jan [cited 2025 Mar 1]; 15: 17562848221074204. Available from:
In therapies of EoE, there can be a discrepancy between a patient's symptoms and their histopathological findings, necessitating repeated evaluations to monitor disease activity accurately. Consequently, short-term treatment aims to relieve symptoms, reduce inflammation and restore normal esophageal function. These goals can be achieved through three main therapeutic approaches: dietary modifications, pharmacologic treatment, and esophageal dilation. Whenever feasible, a multidisciplinary team including a gastroenterologist, allergist, and nutritionist should be involved in managing the condition to ensure comprehensive care
[5]
Furuta GT, Katzka DA. Eosinophilic Esophagitis. N Engl J Med [Internet]. 2015 Oct 22 [cited 2025 Feb 27]; 373(17): 1640-8. Available from:
To our patient to address his symptoms he underwent two endoscopic dilation procedures which resulted in a gradual improvement in his dysphagia and overall symptoms. In addition to the endoscopic treatment, the patient was prescribed Fluticasone propionate as part of his ongoing management.
The patient has been scheduled for a follow-up appointment in one month to monitor his progress and ensure that the symptoms do not recur. This follow-up is crucial to assess the long-term effectiveness of the treatment and to determine if any additional interventions, such as further dilations or adjustments to medication, are necessary.
A widely recognized treatment for eosinophilic esophagitis, especially in older teens and adults, is esophageal dilatation to relieve esophageal constriction. A analysis of multiple large series has revealed perforation rates of less than 1% (3 of 992 dilations), despite previous studies indicating a high risk of dilation-related problems in patients with eosinophilic esophagitis. It is anticipated that 75% of patients with eosinophilic esophagitis would experience chest pain following the surgery, hence dilatation should be done gradually over several sessions. Dilation does not cure the underlying inflammatory condition, but it effectively treats the luminal narrowing that might exacerbate eosinophilic esophagitis
[5]
Furuta GT, Katzka DA. Eosinophilic Esophagitis. N Engl J Med [Internet]. 2015 Oct 22 [cited 2025 Feb 27]; 373(17): 1640-8. Available from:
Improvement in symptoms following treatment for eosinophilic esophagitis is not reliably indicator of histologic remission, as patient-reported symptoms often do not correlate with underlying histologic activity. Therefore, to confirm histologic remission, a follow-up endoscopy with biopsy should be performed at least 6 to 16 weeks after starting treatment
[3]
Ikobah JM, Ikwuagwu E, Ukpabio I, Ugbem T, Okechukwu OC, Ekanem E. Eosinophilic oesophagitis in a Nigerian adolescent: a case report. Pan Afr Med J [Internet]. 2024 Jan 4 [cited 2025 Feb 27]; 47(3). Available from:
EoE is often misdiagnosed as GERD due to symptom overlap; however, it is primarily an immune-mediated disorder that requires distinct management. EoE should be considered in patients with unexplained dysphagia and esophageal strictures and requires a multidisciplinary approach, incorporating allergists, gastroenterologists, and dietitians to tailor therapy based on disease severity. Timely recognition and appropriate management can significantly improve outcomes and quality of life. Future research should focus on optimizing therapeutic strategies and improving patient outcomes through earlier recognition and intervention.
Abbreviations
EGD
Esophagogastroduodenoscopy
EoE
Eosinophilic Oesophagitis
GERD
Gastroesophageal Reflux Disease
UES
Upper Esophageal Sphincter
Author Contributions
Yohannes Birhanu: Conceptualization, Validation.
Yonas Bekuretsion: Investigation.
Henok Seife: Supervision, Validation.
Bethelhem Zerfu Tefera: Writing original draft, Writing review & editing.
Acknowledgments
We would like to acknowledge the patient for providing us consent to share his history as a case report and Lancet general hospital for evaluating the case and giving us ethical clearance.
Availability of Data and Materials
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Ethical Clearance
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Funding
No specific grant was obtained for this case report from any funding agency.
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
Clayton F, Peterson K. Eosinophilic Esophagitis. Gastrointest Endosc Clin N Am [Internet]. 2018 Jan [cited 2025 Mar 1]; 28(1): 1-14. Available from:
Kiely K. Eosinophilic Esophagitis: A Case Study of a 12-Year-Old Boy. J Pediatr Health Care [Internet]. 2017 Sep 1 [cited 2025 Feb 27]; 31(5): 618-22. Available from:
Ikobah JM, Ikwuagwu E, Ukpabio I, Ugbem T, Okechukwu OC, Ekanem E. Eosinophilic oesophagitis in a Nigerian adolescent: a case report. Pan Afr Med J [Internet]. 2024 Jan 4 [cited 2025 Feb 27]; 47(3). Available from:
Eosinophilic esophagitis presenting with spontaneous esophageal rupture: a case report | Journal of Medical Case Reports | Full Text [Internet]. [cited 2025 Feb 27]. Available from:
Dowling PJ, Neuhaus H, Polk BI. The Role of the Environment in Eosinophilic Esophagitis. Clin Rev Allergy Immunol [Internet]. 2019 Dec [cited 2025 Mar 1]; 57(3): 330-9. Available from:
D. Villalta, A.M. Baragiotta. Volume eosinophilic esophagitis from case report 310allasp1.pdf [Internet]. 2008 Nov [cited 2025 Feb 27]. Available from:
Kim NI, Jo Y, Ahn SB, Son BK, Kim SH, Park YS, et al. A Case of Eosinophilic Esophagitis With Food Hypersensitivity. J Neurogastroenterol Motil [Internet]. 2010 Jul [cited 2025 Feb 27]; 16(3): 315-8. Available from:
Lucendo AJ, Santander C, Savarino E, Guagnozzi D, Pérez-Martínez I, Perelló A, et al. EoE CONNECT, the European Registry of Clinical, Environmental, and Genetic Determinants in Eosinophilic Esophagitis: rationale, design, and study protocol of a large-scale epidemiological study in Europe. Ther Adv Gastroenterol [Internet]. 2022 Jan [cited 2025 Mar 1]; 15: 17562848221074204. Available from:
Frontiers | Eosinophilic esophagitis improved by the discontinuation of sublingual immunotherapy for aeroallergens: a case report [Internet]. [cited 2025 Feb 27]. Available from:
Johnson J, Dellon E, McCoy AN, Sun S, Jensen ET, Fodor AA, et al. Lack of association of the esophageal microbiome in adults with eosinophilic esophagitis compared with non-EoE controls. J Gastrointestin Liver Dis [Internet]. 2021 Mar 12 [cited 2025 Mar 1]; 30(1): 17-24. Available from:
Busing JD, Buendia M, Choksi Y, Hiremath G, Das SR. Microbiome in Eosinophilic Esophagitis—Metagenomic, Metatranscriptomic, and Metabolomic Changes: A Systematic Review. Front Physiol [Internet]. 2021 Sep 10 [cited 2025 Mar 1]; 12: 731034. Available from:
Birhanu, Y., Bekuretsion, Y., Seife, H., Tefera, B. Z. (2025). Eosinophilic Esophagitis with Long-standing Dysphagia. International Journal of Medical Case Reports, 4(2), 37-41. https://doi.org/10.11648/j.ijmcr.20250402.13
Birhanu, Y.; Bekuretsion, Y.; Seife, H.; Tefera, B. Z. Eosinophilic Esophagitis with Long-standing Dysphagia. Int. J. Med. Case Rep.2025, 4(2), 37-41. doi: 10.11648/j.ijmcr.20250402.13
Birhanu Y, Bekuretsion Y, Seife H, Tefera BZ. Eosinophilic Esophagitis with Long-standing Dysphagia. Int J Med Case Rep. 2025;4(2):37-41. doi: 10.11648/j.ijmcr.20250402.13
@article{10.11648/j.ijmcr.20250402.13,
author = {Yohannes Birhanu and Yonas Bekuretsion and Henok Seife and Bethelhem Zerfu Tefera},
title = {Eosinophilic Esophagitis with Long-standing Dysphagia
},
journal = {International Journal of Medical Case Reports},
volume = {4},
number = {2},
pages = {37-41},
doi = {10.11648/j.ijmcr.20250402.13},
url = {https://doi.org/10.11648/j.ijmcr.20250402.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijmcr.20250402.13},
abstract = {Eosinophilic esophagitis (EoE) is a chronic, immune-mediated inflammatory condition that primarily affects the esophagus, characterized by the infiltration of eosinophils into the esophageal mucosa. This condition leads to symptoms of esophageal dysfunction, including dysphagia (difficulty swallowing), food impaction, and substernal pain. EoE is commonly associated with other atopic diseases such as asthma, allergic rhinitis, and eczema, and it predominantly affects young men with a history of atopy. Although it can occur in both children and adults, EoE is often underdiagnosed due to its subtle or nonspecific symptoms and its overlap with other gastrointestinal disorders. Rarely, EoE can present with severe complications, such as spontaneous esophageal perforation, known as Boerhaave’s syndrome, which is a life-threatening emergency. A typical diagnostic approach for EoE includes esophageal biopsies, which reveal significant eosinophilic infiltration, and endoscopic findings that may show structural changes such as strictures or rings in the esophagus. In some cases, the strictures can be severe, leading to difficulty swallowing and even food impaction. We present the case of a 36-year-old man from Addis Ababa, Ethiopia, who had been experiencing persistent substernal pain and dysphagia for eight years. His symptoms gradually worsened over time, prompting further investigation. Endoscopic examination revealed a severe lower esophageal stricture located approximately 35 cm from the incisors, and esophageal biopsies confirmed the presence of significant eosinophilic infiltration, consistent with a diagnosis of EoE. This case highlights the importance of considering EoE in patients with chronic dysphagia and substernal pain, especially those with a history of atopic conditions, and emphasizes the need for timely diagnosis and management to prevent complications.
},
year = {2025}
}
TY - JOUR
T1 - Eosinophilic Esophagitis with Long-standing Dysphagia
AU - Yohannes Birhanu
AU - Yonas Bekuretsion
AU - Henok Seife
AU - Bethelhem Zerfu Tefera
Y1 - 2025/06/30
PY - 2025
N1 - https://doi.org/10.11648/j.ijmcr.20250402.13
DO - 10.11648/j.ijmcr.20250402.13
T2 - International Journal of Medical Case Reports
JF - International Journal of Medical Case Reports
JO - International Journal of Medical Case Reports
SP - 37
EP - 41
PB - Science Publishing Group
SN - 2994-7049
UR - https://doi.org/10.11648/j.ijmcr.20250402.13
AB - Eosinophilic esophagitis (EoE) is a chronic, immune-mediated inflammatory condition that primarily affects the esophagus, characterized by the infiltration of eosinophils into the esophageal mucosa. This condition leads to symptoms of esophageal dysfunction, including dysphagia (difficulty swallowing), food impaction, and substernal pain. EoE is commonly associated with other atopic diseases such as asthma, allergic rhinitis, and eczema, and it predominantly affects young men with a history of atopy. Although it can occur in both children and adults, EoE is often underdiagnosed due to its subtle or nonspecific symptoms and its overlap with other gastrointestinal disorders. Rarely, EoE can present with severe complications, such as spontaneous esophageal perforation, known as Boerhaave’s syndrome, which is a life-threatening emergency. A typical diagnostic approach for EoE includes esophageal biopsies, which reveal significant eosinophilic infiltration, and endoscopic findings that may show structural changes such as strictures or rings in the esophagus. In some cases, the strictures can be severe, leading to difficulty swallowing and even food impaction. We present the case of a 36-year-old man from Addis Ababa, Ethiopia, who had been experiencing persistent substernal pain and dysphagia for eight years. His symptoms gradually worsened over time, prompting further investigation. Endoscopic examination revealed a severe lower esophageal stricture located approximately 35 cm from the incisors, and esophageal biopsies confirmed the presence of significant eosinophilic infiltration, consistent with a diagnosis of EoE. This case highlights the importance of considering EoE in patients with chronic dysphagia and substernal pain, especially those with a history of atopic conditions, and emphasizes the need for timely diagnosis and management to prevent complications.
VL - 4
IS - 2
ER -
Birhanu, Y., Bekuretsion, Y., Seife, H., Tefera, B. Z. (2025). Eosinophilic Esophagitis with Long-standing Dysphagia. International Journal of Medical Case Reports, 4(2), 37-41. https://doi.org/10.11648/j.ijmcr.20250402.13
Birhanu, Y.; Bekuretsion, Y.; Seife, H.; Tefera, B. Z. Eosinophilic Esophagitis with Long-standing Dysphagia. Int. J. Med. Case Rep.2025, 4(2), 37-41. doi: 10.11648/j.ijmcr.20250402.13
Birhanu Y, Bekuretsion Y, Seife H, Tefera BZ. Eosinophilic Esophagitis with Long-standing Dysphagia. Int J Med Case Rep. 2025;4(2):37-41. doi: 10.11648/j.ijmcr.20250402.13
@article{10.11648/j.ijmcr.20250402.13,
author = {Yohannes Birhanu and Yonas Bekuretsion and Henok Seife and Bethelhem Zerfu Tefera},
title = {Eosinophilic Esophagitis with Long-standing Dysphagia
},
journal = {International Journal of Medical Case Reports},
volume = {4},
number = {2},
pages = {37-41},
doi = {10.11648/j.ijmcr.20250402.13},
url = {https://doi.org/10.11648/j.ijmcr.20250402.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijmcr.20250402.13},
abstract = {Eosinophilic esophagitis (EoE) is a chronic, immune-mediated inflammatory condition that primarily affects the esophagus, characterized by the infiltration of eosinophils into the esophageal mucosa. This condition leads to symptoms of esophageal dysfunction, including dysphagia (difficulty swallowing), food impaction, and substernal pain. EoE is commonly associated with other atopic diseases such as asthma, allergic rhinitis, and eczema, and it predominantly affects young men with a history of atopy. Although it can occur in both children and adults, EoE is often underdiagnosed due to its subtle or nonspecific symptoms and its overlap with other gastrointestinal disorders. Rarely, EoE can present with severe complications, such as spontaneous esophageal perforation, known as Boerhaave’s syndrome, which is a life-threatening emergency. A typical diagnostic approach for EoE includes esophageal biopsies, which reveal significant eosinophilic infiltration, and endoscopic findings that may show structural changes such as strictures or rings in the esophagus. In some cases, the strictures can be severe, leading to difficulty swallowing and even food impaction. We present the case of a 36-year-old man from Addis Ababa, Ethiopia, who had been experiencing persistent substernal pain and dysphagia for eight years. His symptoms gradually worsened over time, prompting further investigation. Endoscopic examination revealed a severe lower esophageal stricture located approximately 35 cm from the incisors, and esophageal biopsies confirmed the presence of significant eosinophilic infiltration, consistent with a diagnosis of EoE. This case highlights the importance of considering EoE in patients with chronic dysphagia and substernal pain, especially those with a history of atopic conditions, and emphasizes the need for timely diagnosis and management to prevent complications.
},
year = {2025}
}
TY - JOUR
T1 - Eosinophilic Esophagitis with Long-standing Dysphagia
AU - Yohannes Birhanu
AU - Yonas Bekuretsion
AU - Henok Seife
AU - Bethelhem Zerfu Tefera
Y1 - 2025/06/30
PY - 2025
N1 - https://doi.org/10.11648/j.ijmcr.20250402.13
DO - 10.11648/j.ijmcr.20250402.13
T2 - International Journal of Medical Case Reports
JF - International Journal of Medical Case Reports
JO - International Journal of Medical Case Reports
SP - 37
EP - 41
PB - Science Publishing Group
SN - 2994-7049
UR - https://doi.org/10.11648/j.ijmcr.20250402.13
AB - Eosinophilic esophagitis (EoE) is a chronic, immune-mediated inflammatory condition that primarily affects the esophagus, characterized by the infiltration of eosinophils into the esophageal mucosa. This condition leads to symptoms of esophageal dysfunction, including dysphagia (difficulty swallowing), food impaction, and substernal pain. EoE is commonly associated with other atopic diseases such as asthma, allergic rhinitis, and eczema, and it predominantly affects young men with a history of atopy. Although it can occur in both children and adults, EoE is often underdiagnosed due to its subtle or nonspecific symptoms and its overlap with other gastrointestinal disorders. Rarely, EoE can present with severe complications, such as spontaneous esophageal perforation, known as Boerhaave’s syndrome, which is a life-threatening emergency. A typical diagnostic approach for EoE includes esophageal biopsies, which reveal significant eosinophilic infiltration, and endoscopic findings that may show structural changes such as strictures or rings in the esophagus. In some cases, the strictures can be severe, leading to difficulty swallowing and even food impaction. We present the case of a 36-year-old man from Addis Ababa, Ethiopia, who had been experiencing persistent substernal pain and dysphagia for eight years. His symptoms gradually worsened over time, prompting further investigation. Endoscopic examination revealed a severe lower esophageal stricture located approximately 35 cm from the incisors, and esophageal biopsies confirmed the presence of significant eosinophilic infiltration, consistent with a diagnosis of EoE. This case highlights the importance of considering EoE in patients with chronic dysphagia and substernal pain, especially those with a history of atopic conditions, and emphasizes the need for timely diagnosis and management to prevent complications.
VL - 4
IS - 2
ER -