Abstract
Introduction: Prostate cancer is a leading malignancy among men, with radiotherapy (RT) serving as a cornerstone of curative treatment. The precision of external beam radiotherapy (EBRT) is challenged by prostate motion caused by bladder and rectal filling variations, leading to inter- and intra-fraction positional uncertainties. Advanced image-guided radiotherapy (IGRT) and motion management technologies can mitigate these uncertainties; however, their implementation in low- and middle-income countries (LMICs) such as India remains inconsistent due to infrastructure, training, and resource limitations. Radiation therapists (RTTs) play a critical role in accurate patient setup, imaging, and on-treatment verification, yet their perspectives on motion management in prostate radiotherapy are underrepresented in literature. This study aimed to evaluate current RTT practices, challenges, and training needs in India. Materials and Methods: A descriptive, cross-sectional, questionnaire-based survey was conducted over 60 days among RTTs treating prostate cancer with EBRT in India. The online survey, developed through literature review and expert consultation, included 15 mandatory questions across seven domains: demographics, institutional profiles, clinical load, techniques in use, workflow impact, technical challenges, and training preferences. Purposive sampling recruited participants via professional networks, email, and social media. Responses from 202 RTTs were analyzed using descriptive statistics in Microsoft Excel. Results: Daily cone-beam computed tomography (CBCT) was the most widely adopted motion management method (84.7%), followed by respiratory position management (15.8%), surface-guided radiotherapy (15.8%), and real-time tracking (9.4%). Notably, 40.6% reported no dedicated motion management technique. The most common challenges were inconsistent bladder/rectum filling (64.4%), time constraints (34.2%), patient discomfort (24.3%), and technology limitations (14.9%). Motion management increased setup times by 6-15 minutes in 49.5% of cases, with 16.3% of RTTs reporting reduced patient throughput. While 66.9% agreed that current strategies reduce setup uncertainties, responses revealed variability in practice and technology access. Training needs were substantial, with workshops (55.4%), SOP/guideline updates (46.5%), and online modules (34.2%) most preferred. Private institutions accounted for 81.2% of responses, reflecting disparities between urban and rural access to technology. Conclusions: This nationwide survey highlights widespread adoption of CBCT-based IGRT in Indian prostate cancer radiotherapy but also reveals significant gaps in advanced motion tracking, workflow optimization, and standardized patient preparation protocols. Addressing these limitations through national guidelines, equitable technology distribution, and RTT-focused education is essential for consistent, high-quality motion management. Investment in training, patient education, and infrastructure will be critical to bridging practice variability and improving treatment precision across diverse healthcare settings.
|
Published in
|
Journal of Cancer Treatment and Research (Volume 13, Issue 3)
|
|
DOI
|
10.11648/j.jctr.20251303.15
|
|
Page(s)
|
72-82 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2025. Published by Science Publishing Group
|
Keywords
Prostate Cancer Radiotherapy, Motion Management, Indian Radiation Therapists, Image-guided Radiotherapy, Intrafraction Monitoring, Nationwide Survey
1. Introduction
Prostate cancer remains one of the most frequently diagnosed malignancies among men worldwide, with its incidence steadily increasing in developing countries such as India
. Radiotherapy plays a pivotal role in the definitive management of localized and locally advanced prostate cancer, offering both curative intent and organ preservation
| [2] | Dearnaley D, Syndikus I, Mossop H, Khoo V, Birtle A, Bloomfield D, et al. Conventional versus hypofractionated high-dose intensity-modulated radiotherapy for prostate cancer: 5-year outcomes of the randomised, non-inferiority, phase 3 CHHiP trial. Lancet Oncol. 2016; 17(8): 1047-60. https://doi.org/10.1016/S1470-2045(16)30102-4 |
[2]
. The clinical success of external beam radiotherapy (EBRT), however, is highly dependent on the precision of dose delivery. This precision is often compromised by the natural movement of the prostate gland during and between treatment sessions
. The displacement of the prostate is largely driven by physiological fluctuations in bladder and rectal filling, leading to inter-fractional and intra-fractional positional uncertainties
| [4] | de Muinck Keizer DM, Kerkmeijer LGW, Willigenburg T. Daily online plan adaptation for prostate cancer using MRI-guided radiotherapy: Dosimetric benefits and treatment time analysis. Radiotherapy Oncol. 2019; 140: 244-9. |
[4]
. Studies have shown a tendency for the prostate to shift posteriorly and inferiorly following initial setup, primarily due to variations in bladder and rectal distension. Moreover, intra-fraction motion can occur unpredictably and varies between patients and treatment fractions, making real-time monitoring crucial for minimizing geometric and dosimetric errors
| [5] | Byrne TE. A review of prostate motion with considerations for the treatment of prostate cancer. Med Dosim. 2005; 30(3): 155-61. https://doi.org/10.1016/j.meddos.2005.03.005 |
| [6] | Lovelock DM, Messineo AP, Cox BW, Kollmeier MA, Zelefsky MJ. Continuous monitoring and intrafraction target position correction during treatment improves target coverage for patients undergoing SBRT prostate therapy. Int J Radiat Oncol Biol Phys. 2015; 91(3): 588-94. https://doi.org/10.1016/j.ijrobp.2014.10.049 |
| [7] | Ballhausen H, Reiner M, Kantz S, Belka C, Söhn M. The random walk model of intrafraction movement. Phys Med Biol. 2013; 58(7): 2413-27. https://doi.org/10.1088/0031-9155/58/7/2413 |
| [8] | Ten Haken RK, Forman JD, Heimburger DK, Gerhardsson A, McShan DL, Perez-Tamayo C, et al. Treatment planning issues related to prostate movement in response to differential filling of the rectum and bladder. Int J Radiat Oncol Biol Phys. 1991; 20(6): 1317-24. https://doi.org/10.1016/0360-3016(91)90244-x |
| [9] | Sengupta C, Skouboe S, Ravkilde T, Poulsen PR, Nguyen DT, Greer PB, et al. The dosimetric error due to uncorrected tumor rotation during real-time adaptive prostate stereotactic body radiation therapy. Med Phys. 2023; 50(1): 20-9. https://doi.org/10.1002/mp.16094 |
| [10] | Sihono DSK, Ehmann M, Heitmann S, von Swietochowski S, Grimm M, Boda-Heggemann J, Lohr F, Wenz F, Wertz H. Determination of intrafraction prostate motion during external beam radiation therapy with a transperineal 4-dimensional ultrasound real-time tracking system. Int J Radiat Oncol Biol Phys. 2018 May 1; 101(1): 136-43. https://doi.org/10.1016/j.ijrobp.2018.01.040 |
[5-10]
.
To mitigate such uncertainties, various motion management techniques have been adopted
| [11] | Brennan S, Burleson S, Kostrzewa C, Godoy Scripes P, Subashi E, Zhang Z, et al. SBRT focal dose intensification using an MR-Linac adaptive planning for intermediate-risk prostate cancer: An analysis of the dosimetric impact of intra-fractional organ changes. Radiotherapy Oncol. 2023; 179: 109441. https://doi.org/10.1016/j.radonc.2022.109441 |
| [12] | Rose C, Ebert MA, Mukwada G, Skorska M, Gill S. Intrafraction motion during CyberKnife® prostate SBRT: Impact of imaging frequency and patient factors. Phys Eng Sci Med. 2023. https://doi.org/10.1007/s13246-023-01242-7 |
[11, 12]
. In linear accelerator-based treatment settings, kilovoltage (kV) planar imaging and volumetric CBCT, often used in conjunction with fiducial markers, remain standard practices
| [13] | Kron T, Thomas J, Fox C, Thompson A, Owen R, Herschtal A, et al. Intra-fraction prostate displacement in radiotherapy estimated from pre- and post-treatment imaging of patients with implanted fiducial markers. Radiother Oncol. 2010; 95(2): 191-7. https://doi.org/10.1016/j.radonc.2010.01.010 |
| [14] | Gladwish A, Pang G, Cheung P, D’Alimonte L, Deabreu A, Loblaw A. Prostatic displacement during extreme hypofractionated radiotherapy using volumetric modulated arc therapy (VMAT). Radiation Oncol. 2014; 9: 262. https://doi.org/10.1186/s13014-014-0262-y |
[13, 14]
. These imaging techniques help detect positional deviations of more than 5 mm, which could otherwise result in geographic miss and unintentional irradiation of adjacent organs-at-risk (OARs), including the rectum and bladder
| [15] | Mutanga TF, de Boer HCJ, van der Wielen GJ, Hoogeman MS, Incrocci L, Heijmen BJM. Margin evaluation in the presence of deformation, rotation, and translation in prostate and entire seminal vesicle irradiation with daily marker-based setup corrections. Int J Radiat Oncol Biol Phys. 2011 Nov 15; 81(4): 1160-7. https://doi.org/10.1016/j.ijrobp.2010.09.013 |
[15]
. With the evolution of high-precision techniques such as Intensity-Modulated Radiation Therapy (IMRT) and Stereotactic Body Radiation Therapy (SBRT), motion management has become even more critical
| [16] | Tree AC, Alexander EJ, Van As NJ, Dearnaley DP, Khoo V, et al. Biological dose escalation and hypofractionation: what is there to be gained and how will it best be done? Clin Oncol (R Coll Radiol). 2013 Aug; 25(8): 483-98. https://doi.org/10.1016/j.clon.2013.05.003 |
[16]
. Technologies including image-guided radiotherapy (IGRT), surface-guided radiation therapy (SGRT), electromagnetic transponders, and real-time tracking systems have shown potential in enhancing targeting precision and minimizing treatment margins
| [17] | Nguyen KA, Peñagaricano JA, McCulloch W. Advances in prostate cancer motion management. Med Dosim. 2020; 45(2): 150-7. |
| [18] | Van der Heide UA, Kotte ANTJ, Dehnad H, Hofman P, Lagenijk JJW, van Vulpen M, et al. Analysis of fiducial marker-based position verification in the external beam radiotherapy of patients with prostate cancer. Radiother Oncol. 2007 Jan; 82(1): 38-45. https://doi.org/10.1016/j.radonc.2006.11.002 |
[17, 18]
. Despite these advancements, access and implementation remain inconsistent, especially in low- and middle-income countries like India, where limitations in equipment, training, and staffing often create practice variability
| [19] | Harris EJ, Freeman N, Perks J. A national survey of IGRT practice in the UK. Br J Radiol. 2017; 90(1071): 20160666. https://doi.org/10.1259/bjr.20160666 |
| [20] | Gupta T, Laskar S, Agarwal JP, Budrukkar A. Indian perspective of quality and access in cancer radiotherapy. J Cancer Policy. 2020; 24: 100235. |
[19, 20]
. A core radiation oncology team consists of Radiation oncologists (RO), Medical Physicists (MP) and Radiation therapists (RTT) among other staff. Radiation therapists (RTT), who are responsible for patient setup, imaging, and on-treatment verification, play a key role in ensuring motion management accuracy
| [21] | Radiation Therapy Advisory Group. National framework for radiation therapists’ advanced practice. Radiation Therapist Practice Report, Cancer Council Australia. 2018. |
[21]
. However, their practical experiences and operational challenges are underreported in the literature
| [22] | Fischer-Valuck BW, Henke LE, Green OL, Kashani R, Yang D, Olsen JR, et al. Clinical implementation of MR-guided pelvic radiotherapy: Feasibility and workflow considerations. Pract Radiat Oncol. 2017; 7(6): 373-81. https://doi.org/10.1016/j.adro.2017.05.006 |
| [23] | Paulino AC, Johnstone PAS, Calley CS. The evolving role of the radiation therapist in modern radiotherapy delivery. J Appl Clin Med Phys. 2019; 20(1): 9-17. https://doi.org/10.1002/acm2.12540 |
[22, 23]
.
This study aims to evaluate current practices, challenges, and training needs of Indian RTTs in prostate motion management to inform future policy, practice standardization, and education.
2. Materials and Methods
2.1. Study Design
This research was conducted as a descriptive, cross-sectional, questionnaire-based survey study aimed at exploring current practices, challenges, and perceived effectiveness of motion management techniques used by RTTs in the definitive radiotherapy treatment of prostate cancer across India for a duration of sixty days. The conceptual framework was built upon a need to document applications of motion mitigation strategies, levels of expertise, and systemic barriers within Indian radiation oncology facilities. The methodology was designed to ensure structured data collection from practicing RTT professionals, using quantitative and qualitative inputs via a structured online questionnaire.
2.2. Development of the Survey
The survey questionnaires were developed using Google Forms and consisted of a total of 15 structured questions, are presented in
Table S1. The formulation of these questions was formed by a comprehensive literature review on motion management in prostate radiotherapy, along with expert consultations involving clinical oncologists, medical physicists, and senior radiation therapists. The survey questions were categorized into the seven following major sections.
1) Demographics and Institutional Profiles
2) Clinical Load and Techniques in Use
3) Time Impact and Workflow Efficiency
4) Common Technical Challenges
5) Setup and Imaging Issues
6) Perception of Motion Management Effectiveness
7) Training and Support Needs
All questions were marked as mandatory to ensure completeness of each response and to minimize missing data during analysis. The questionnaire comprised multiple-choice, Likert-scale, and checkbox-style responses, as well as a few short-answer questions to gather contextual qualitative insights. A comprehensive summary of the entire question bank can be found in
Table S1.
2.3. Target Population and Inclusion Criteria
The target population for this study included RTTs currently practicing in India, with experience in the treatment of prostate cancer using external beam radiotherapy.
2.4. Sampling Method
A non-probability purposive sampling technique was employed to recruit participants. The survey link was distributed electronically through professional networks, email lists, national radiation therapy whatsapp groups, and social media platforms such as LinkedIn. The link remained open for responses for a period of sixty days, ensuring sufficient time for dissemination and participation. During the recruitment phase, the invitation clearly stated the objective of the study, voluntary nature of participation, assurance of confidentiality, and the estimated time commitment (5 minutes).
2.5. Data Collection and Management
Responses were collected anonymously via Google Forms and were automatically compiled into a secure spreadsheet in real-time. Upon closure of the form, all raw data were reviewed for completeness and consistency. In total, 202 complete and validated responses were obtained. No partial submissions were included in the final analysis, as the survey platform enforced completion of all required fields.
2.6. Data Analysis
Data analysis was conducted using Microsoft Excel. Descriptive statistics such as frequencies, percentages, and measures of central tendency were used to summarize responses. Multiple-response and checkbox data were tallied to reflect the percentage of therapists endorsing each category.
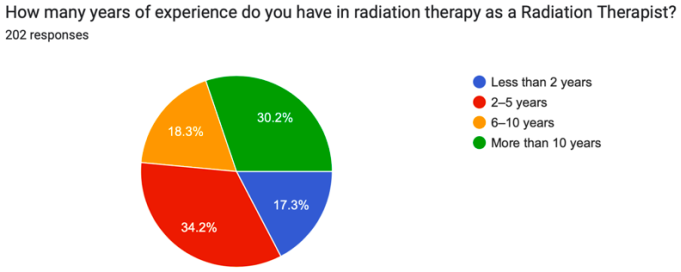
Figure 1. Years of professional experience among radiation therapists (n = 202). The majority reported 2–5 years (34.5%) and over 10 years (30.2%) of experience, with fewer indicating less than 1 year or 6–10 years in the field.
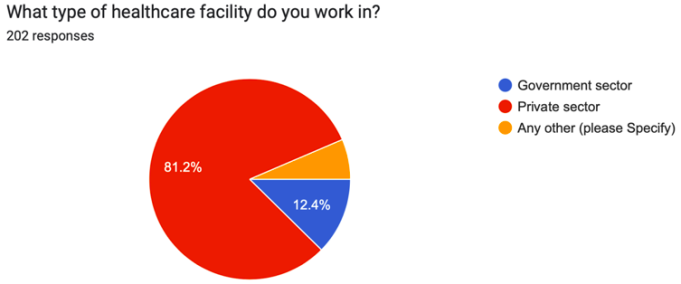
Figure 2. Type of healthcare facility where respondents are employed (n = 202). Most (81.2%) work in private sector institutions, while only 18.8% are affiliated with government hospitals.
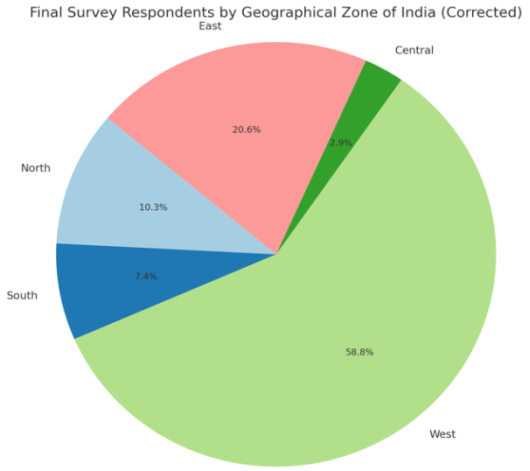
Figure 3. Geographical distribution of survey respondents (n = 202), categorized by Indian zones. The West region contributed the highest number of responses (38.8%), followed by East (20.3%), North (19.3%), South (14.4%), and Central (7.2%).
3. Results
Demographics and Institutional Profiles: A total of 202 radiation therapists (RTTs) from a wide range of clinical settings across India participated in the survey, aiming to capture current practices and perspectives in definitive prostate cancer motion management. Demographic and institutional characteristics, corresponding to Questions 1-4, are presented in
Table S1.A substantial proportion of participants reported over 10 years of clinical experience (34.2%), followed by 2-5 years (30.2%), 6-10 years (18.3%), and less than 2 years (17.3%), indicating a well-distributed respondent profile with strong representation from mid-career and senior RTTs (
Figure 1).
Regarding workplace type, the majority (81.2%) were employed in private healthcare institutions, with 12.4% from government hospitals, and the remainder from charitable or other settings (
Figure 2). Geographic representation spanned over 40 cities, including metropolitan hubs (e.g., Mumbai, Delhi, Kolkata) and smaller regional centers (e.g., Silchar, Bhuj), suggesting considerable diversity in clinical exposure and infrastructure. This breadth of representation reflects varying access to technology, training, and motion management protocols across urban and semi-urban regions (
Figure 3). An aggregated summary is provided in
Table S2.
Clinical Load and Techniques in Use: Responses to Questions 5-7 evaluated institutional patient volume and technique utilization. As shown in
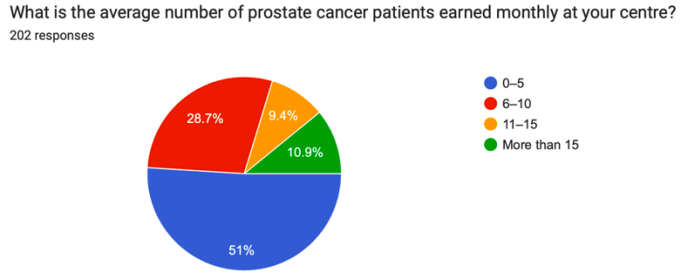
Table S3, 51% of respondents indicated their centers treat more than 15 prostate cancer patients per month, while 9.4% treat fewer than 5 patients/month. These findings illustrate a wide variation in patient load, with many centers managing a high clinical throughput, potentially influencing imaging strategies and motion verification practices (
Figure 4).
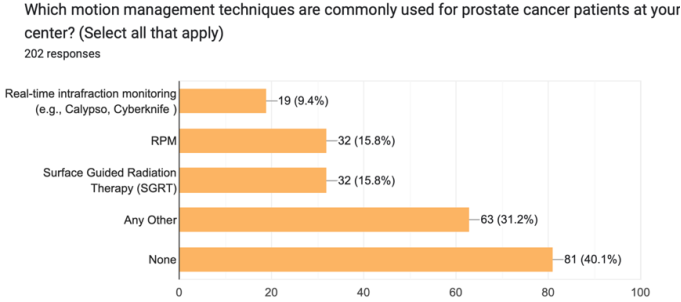
In terms of motion management techniques, the most commonly reported approach was daily CBCT (30.7%), followed by RPM and SGRT (15.8% each), and real-time tracking (9.4%). Alarmingly, 40.6% of respondents indicated that no specific motion management technique was employed (
Figure 5). These findings highlight a growing reliance on image-guided radiotherapy (IGRT) practices while also pointing to the underutilization of advanced real-time motion tracking systems, likely due to infrastructural or training constraints.
Time Impact and Workflow Efficiency: Questions 8-10 assessed the impact of motion management on imaging frequency, treatment time, and workflow disruptions, summarized in
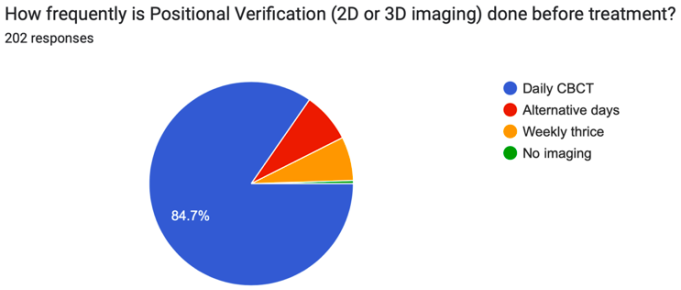
Table S4. An overwhelming majority (84.7%) reported the use of daily CBCT for setup verification, with only a minority practicing alternate-day (8%) or thrice-weekly imaging (6%). A small subset indicated no imaging prior to treatment, raising concerns regarding motion uncertainty (
Figure 6).
Figure 4. Monthly caseload of prostate cancer patients treated across surveyed centres (n = 202). Over half (51.9%) reported managing 0–5 patients monthly, while 28.7% managed 6–10 patients. A smaller proportion handled higher volumes (11–15 and ≥15 patients).
Figure 5. Motion management techniques employed for prostate cancer radiotherapy across centres (n = 202). Surface Guided Radiation Therapy (SGRT) and rectal filling/bladder control were the most commonly used techniques. A minority reported use of daily motion management with fiducial markers or transperineal ultrasound.
Figure 6. Distribution of daily imaging frequencies for treatment among participating centres (n = 202). The majority (84.7%) reported daily Cone Beam CT (CBCT), followed by imaging on alternate days (red), weekly (orange), and other intervals.
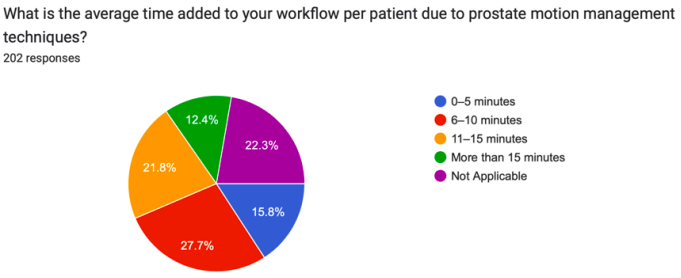
Figure 7. Average additional time per patient added to the workflow due to prostate motion management techniques (n = 202). The most common response was 6–10 minutes (27.7%), followed by more than 15 minutes (22.3%), 11–15 minutes (21.8%), 0–5 minutes (15.8%), and not applicable (12.4%). This reflects the clinical time burden introduced by motion management strategies in prostate radiotherapy.
When asked about additional time required per patient, 27.7% estimated 6-10 minutes, while 21.8% reported 11-15 minutes. Notably, 22.3% marked this question as not applicable, suggesting non-implementation or minimal workflow impact (
Figure 7). In total, 65.3% of respondents acknowledged increased treatment time, underscoring the need for workflow optimization.
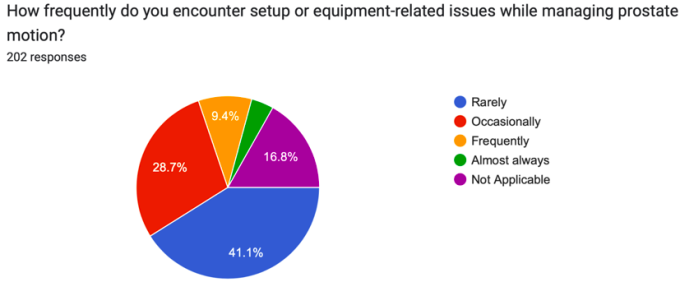
Regarding operational challenges, 41.1% reported equipment or setup-related issues rarely, while 28.7% encountered them occasionally, and 9.4% frequently. Only 4% reported such issues consistently, indicating general stability with room for technical refinement (
Figure 8).
Figure 8. Frequency of setup or equipment-related issues encountered while managing prostate motion (n = 202). The majority reported encountering such issues rarely (41.1%), followed by occasionally (28.7%), frequently (16.8%), not applicable (9.4%), and almost always (4.0%). These findings highlight variability in technological and procedural challenges.
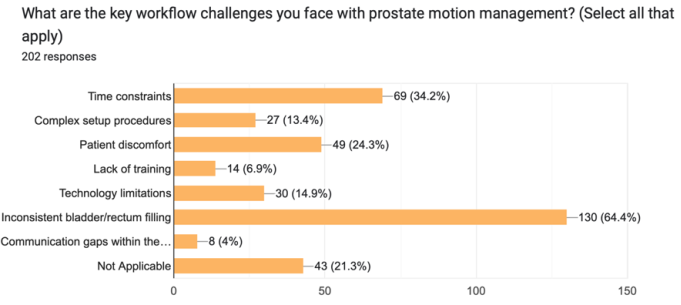
Figure 9. Workflow challenges encountered in prostate motion management (n = 202). Inconsistent bladder or rectum filling was most reported (64.1%), followed by time constraints (34.5%) and patient discomfort (34.3%). Other concerns included technology limitations and staff workload.
Common Technical Challenges: Questions 11 and 12 focused on common technical challenges and RTT perceptions of motion management effectiveness, as detailed in
Table S5.
The most frequently reported challenge was inconsistent bladder/rectum filling (64.4%), followed by time constraints (34.2%), patient discomfort (24.3%), and technology limitations (14.9%). Less frequently cited issues included complex setup (13.4%), lack of training (6.9%), and communication barriers (4%) (
Figure 9). These findings emphasize the need for robust patient preparation protocols and streamlined workflows.
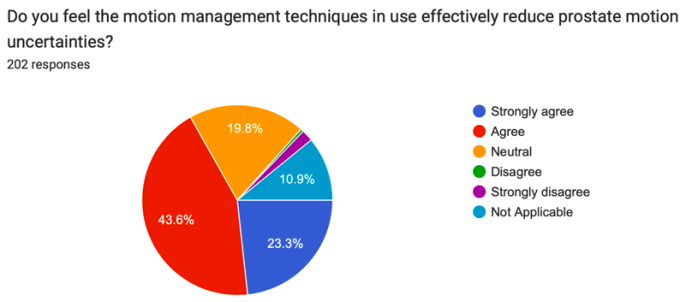
Regarding perceived effectiveness, 43.6% of RTTs agreed and 23.3% strongly agreed that current motion management techniques reduce prostate motion uncertainties. Only a small fraction disagreed (1.5%) or strongly disagreed (0.5%). Approximately 19.8% remained neutral, and 10.9% marked “not applicable,” indicating varying degrees of exposure and confidence (
Figure 10).
Figure 10. Perceptions of the effectiveness of motion management techniques in reducing prostate motion uncertainties (n = 202). Responses varied by centre and technique applied.
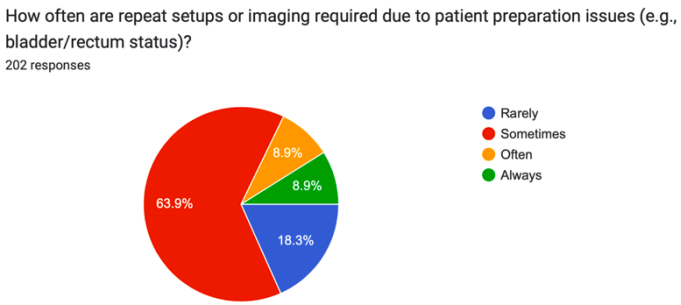
Figure 11. Frequency of repeat setup or imaging necessitated by patient preparation issues (n = 202). Most respondents (69.8%) experienced such issues “sometimes,” while 18.3% experienced them “rarely.” Equal proportions (6.9%) reported “often” or “always.
Setup and Imaging Issues: Question 13 examined the frequency of repeat setups due to inadequate patient preparation (
Table S1,
Figure 11). A significant portion (63.9%) reported that such occurrences happen “sometimes”, while 18.3% indicated “rarely”. Alarmingly, 17.8% of respondents reported frequent or constant repeat setups, highlighting the need for enhanced patient education and standardized bladder/bowel protocols.
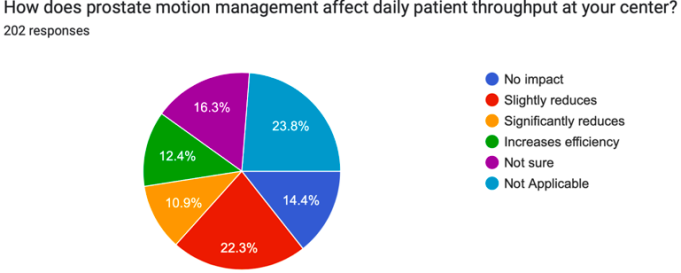
Figure 12. Impact of prostate motion management on daily patient throughput (n = 202). Responses were varied, with 33.9% indicating no impact, 22.3% reporting slight reductions, and 14.4% reporting no impact. A smaller proportion noted significant reductions (10.9%) or moderate effects (12.4%).
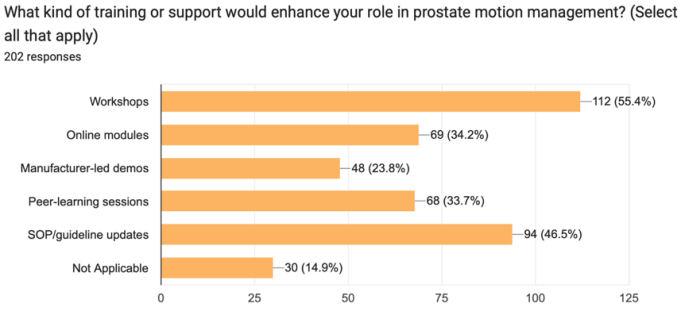
Figure 13. Preferred types of training or support identified by respondents (n = 202) to enhance proficiency in prostate motion management. Workshop-based learning was most preferred (35.6%), followed by SOP/guideline updates (31.6%), online modules (27.3%), and manufacturer-led demos (23.8%). Multiple responses were allowed.
Perception of Motion Management Effectiveness: In Question 14, RTTs assessed the impact of motion management on daily treatment throughput. While 23.8%marked this as “Not Applicable”, 22.3% indicated a slight reduction, and 10.9% reported a significant reduction. Interestingly, 12.4% believed it increased workflow efficiency, while 14.4% saw no impact. The diversity in responses (
Figure 12) likely reflects heterogeneity in institutional resources, staff training, and workflow design.
Training and Support Needs: The final section (Q15) addressed training and support needs, with results displayed in
Table S6 and (
Figure 13). The most preferred mode of support was workshops (55.4%), followed by SOP/guideline updates (46.5%), online modules (34.2%), peer-learning sessions (33.7%), and manufacturer-led demonstrations (23.8%). Only 14.9% of RTTs found these options not applicable, indicating widespread interest in structured training.
These findings underline a significant demand for continuous professional development, hands-on learning, and regular updates to institutional protocols to support effective prostate motion management.
4. Discussion
The mobility of the prostate gland, influenced by bladder and rectal filling, anatomical variability, and internal organ motion, continues to present a major challenge in achieving precision during radiotherapy for prostate cancer. This nationwide survey of 202 Indian radiation therapists (RTTs) provides valuable insights into the current clinical landscape, highlighting trends in motion management techniques, associated workflow challenges, and training needs, particularly in resource-diverse healthcare environments.
Daily cone-beam computed tomography (CBCT) was reported as the most widely adopted motion verification method, with 84.7% of RTTs utilizing it routinely. This is in alignment with international guidelines and literature supporting the routine use of CBCT for enhancing setup accuracy and reducing geographic miss in prostate radiotherapy
| [24] | Frank SJ, Dong L, Gillin M, Kuban DA, Lee AK, Cheung R, et al. IGRT in prostate cancer: evolution and outcomes. Radiother Oncol. 2014; 111(1): 43-50. |
| [25] | Bell LJ, Cox J, Eade T, Rinks M, Kneebone A. The impact of rectal and bladder variability on target coverage during post-prostatectomy intensity-modulated radiotherapy. Radiotherapy and Oncology. 2014 Feb;110(2):245-50. https://doi.org/10.1016/j.radonc.2013.10.042 |
[24, 25]
. Studies have demonstrated that daily image guidance improves treatment precision and contributes to better target localization and reduced margins, especially in the context of interfraction motion
| [26] | Kupelian P, Willoughby T, Mahadevan A, Djemil T, Weinstein G, Jani S, et al. Image-guided hypofractionated radiotherapy: outcomes for localized prostate cancer. J Clin Oncol. 2007; 25(31): 5305-10. https://doi.org/10.1016/j.ijrobp.2006.10.026. |
[26]
.
However, the adoption of more advanced motion management technologies such as real-time intrafraction monitoring systems (e.g., electromagnetic transponders like Calypso) remains limited, reported by fewer than 10% of respondents. Similar trends were noted in international surveys, particularly in low- and middle-income countries (LMICs), where cost, maintenance, and training requirements act as significant barriers
| [27] | Thondykandy R, Saseendran V, Chandran P, Ramesh V, Pillai S, Krishnan S, et al. Challenges in implementing IGRT in low-resource settings: A South Asian perspective. Clin Oncol (R Coll Radiol). 2020; 32(10): e162-9. |
| [28] | Jaffray DA, Siewerdsen JH, Wong JW, Martinez AA. Real-time tumor tracking: Current status and future directions. Semin Radiat Oncol. 2009; 19(1): 77-86. |
[27, 28]
. Likewise, surface-guided radiation therapy (SGRT) and respiratory gating were adopted in fewer than 16% of Indian centers surveyed. While respiratory motion has a limited impact on prostate position, the low uptake of these technologies could also reflect infrastructural limitations and prioritization of CBCT-based solutions, as seen in other resource-constrained settings
.
The survey also sheds light on workflow implications associated with motion management. Approximately 65% of RTTs reported additional setup times ranging from 6 to 15 minutes. These findings are consistent with international reports indicating that advanced motion verification methods can lead to increased treatment time and operational strain
| [30] | Verma V, Simone CB, Kruser TJ, Lin C, Shah C, Chang JY. Time and resource implications of advanced IGRT in prostate cancer. Pract Radiat Oncol. 2016; 6(6): e271-80. |
[30]
. Notably, 16.3% of participants reported reduced patient throughput, highlighting the balance between precision and efficiency that departments must navigate. This reinforces the need for optimized imaging protocols, automation, and effective scheduling to maintain clinical throughput without compromising treatment quality.
Inconsistent bladder and rectal filling emerged as the most common challenge (64.4%), echoing evidence that prostate position can vary significantly due to internal organ motion and gas-induced displacement
| [31] | Söhn M, Alber M, Yan D, Ludewig P, Nüsslin F. Variability in bladder and rectum filling and its impact on prostate position. Radiother Oncol. 2010; 95(1): 48-53. |
[31]
. Such anatomical inconsistencies have been shown to compromise reproducibility, particularly when image guidance is inconsistently applied or when patient preparation protocols are lacking. Over 70% of respondents reported the need for repeat imaging or setup, underscoring the critical role of standardized bowel and bladder protocols, patient education, and pre-treatment bladder volume checks
| [32] | Van Herk M, Remeijer P, Rasch C, Lebesque JV. The probability of correct target dosage: Dose-population histograms for deriving treatment margins in radiotherapy. International Journal of Radiation Oncology, Biology, Physics.2000; 47(4): 1121-1135. https://doi.org/10.1016/S0360-3016(00)00518-6 |
[32]
.
Despite these efforts, only 43.6% of RTTs agreed that current motion management strategies are effective in reducing setup uncertainties, while over 30% remained neutral or disagreed. This divergence in perception may be attributed to inconsistent institutional protocols, limited access to advanced technology, and inadequate staff training. Similar gaps in confidence and variability in practice have been reported in other European and Asia-Pacific RTT surveys
| [33] | Svensson H, Nilsson K, Gunnlaugsson A, Håkansson U, Hjelstuen M, Muren LP, et al. Variability in motion management techniques among European RTTs. Tech Innov Patient Support Radiat Oncol. 2021; 17: 55-61. |
| [34] | Yoshimura R, Nakamura M, Yamada M, Fuji H, Haga A, Shibata T, et al. Motion management strategies in Asian radiotherapy centers: a survey report. Asia Pac J Clin Oncol. 2020; 16(2): e40-6. |
[33, 34]
.
A prominent outcome of this survey is the identified demand for structured training and support. Over half of respondents (55.4%) expressed a preference for hands-on workshops, with additional interest in SOP/guideline updates (46.5%) and peer-learning platforms (33.7%). These findings are in line with international recommendations from ESTRO and other professional bodies, which emphasize the need for continuous education, interprofessional collaboration, and the development of RTT-led protocols
| [35] | Coffey M, Leech M, Poole C, Vaandering A, Verellen D, Borras JM. The changing role of RTTs: ESTRO’s vision and strategy. Radiother Oncol. 2016; 119(1): 1-4. |
| [36] | Dwyer L, Barten D, Forde E, Sharma DS, van Dyk S. Training needs for RTTs in IGRT implementation: A global perspective. Radiography. 2019; 25(4): e102-9. |
[35, 36]
. The expressed interest in manufacturer-led demonstrations also reflects a knowledge gap in the clinical implementation of emerging technologies, indicating the necessity for greater industry-academic collaboration. The majority of responses originated from private sector institutions (81.2%), pointing toward unequal access to technological advancements across public and rural centers. While the geographic diversity of responses-from both metropolitan and smaller cities-illustrates the expanding reach of radiotherapy in India, it also highlights variations in infrastructure, training exposure, and practice uniformity. This uneven landscape is consistent with global surveys showing disparities in radiotherapy access and quality between urban and rural regions
| [37] | Datta NR, Samiei M, Bodis S. Access to radiotherapy in low- and middle-income countries. Lancet Oncol. 2014; 15(11): e495-503. |
[37]
.
In conclusion, this study highlights the progress made in adopting IGRT practices such as CBCT in Indian radiotherapy centers, while also drawing attention to ongoing challenges in training, standardization, and technology integration. Addressing these issues through national guidelines, investment in infrastructure, and RTT-specific education initiatives is essential to ensuring high-quality, patient-centred prostate cancer treatment across all healthcare settings.
5. Conclusion
This survey highlights a crucial point in the changing dynamics of prostate cancer motion management within radiation oncology. Despite significant advancements in the adoption of IGRT, there are still important deficiencies in advanced motion tracking, workflow optimization, and staff training. The findings indicate an increasing recognition among radiation therapists of the necessity for accurate, patient-specific, and resource-sensitive motion management protocols. Future initiatives should focus on the creation of national guidelines, centralized training resources, and improved access to affordable technology to guarantee fair and effective treatment for prostate cancer in diverse clinical environments.
Theory and Calculation
This research utilized descriptive statistics to evaluate survey responses regarding prostate motion management among Indian RTTs. Although dosimetric calculations were not conducted, the study assessed percentage distributions and the impact on workflow. This methodology underscored existing practices, challenges, and training requirements, establishing a foundational framework for future research and the standardization of protocols.
Ethics Statement
As the survey involved no patient data or clinical intervention and focused on professional practices, formal IRB approval was waived. However, participants were assured of complete anonymity, and no identifiable personal or institutional data were collected beyond professional characteristics.
Limitations of the Study
There was a lack of external validation regarding institutional practices or treatment logs. The findings provide important foundational insights into existing practices and perceived challenges related to motion management in prostate cancer radiotherapy within India.
Abbreviations
CBCT | Cone-beam Computed Tomography |
EBRT | External Beam Radiotherapy |
IGRT | Image-guided Radiation Therapy |
IMRT | Intensity-modulated Radiation Therapy |
SBRT | Stereotactic Body Radiation Therapy |
RTT | Radiation Therapist |
SGRT | Surface-guided Radiation Therapy |
RPM | Respiratory Position Management |
SOP | Standard Operating Procedure |
kV | Kilovoltage |
IRB | Institutional Review Board |
VMAT | Volumetric Modulated Arc Therapy |
MR-Linac | Magnetic Resonance Linear Accelerator |
Acknowledgments
We sincerely thank all the survey respondents, as well as the team of Radiation Therapy Technologists (RTTs), physicists, and oncologists, for their invaluable contributions and support in this study.
Author Contributions
Subrata Roy: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing
Kaustav Talapatra: Investigation, Project administration, Supervision, Validation, Writing – review & editing
Ajinkya Gupte: Formal Analysis, Investigation, Resources, Software, Visualization, Writing – review & editing
Unmesh Mukherjee: Investigation, Methodology, Resources, Software
Anand Parab: Investigation, Visualization, Writing – review & editing
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of Generative AI in Scientific Writing
This study was conducted without the use of AI-assisted technology in the design, data collection, analysis, or interpretation of the results. All aspects of the research were carried out through traditional scientific methods and human expertise.
Data Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Rawla P. Epidemiology of prostate cancer. World J Oncol. 2019; 10(2): 63-89.
https://doi.org/10.14740/wjon1191
|
| [2] |
Dearnaley D, Syndikus I, Mossop H, Khoo V, Birtle A, Bloomfield D, et al. Conventional versus hypofractionated high-dose intensity-modulated radiotherapy for prostate cancer: 5-year outcomes of the randomised, non-inferiority, phase 3 CHHiP trial. Lancet Oncol. 2016; 17(8): 1047-60.
https://doi.org/10.1016/S1470-2045(16)30102-4
|
| [3] |
Langen KM, Jones DT. Organ motion and its management. Int J Radiat Oncol Biol Phys. 2001; 50(1): 265-78.
https://doi.org/10.1016/s0360-3016(01)01453-5
|
| [4] |
de Muinck Keizer DM, Kerkmeijer LGW, Willigenburg T. Daily online plan adaptation for prostate cancer using MRI-guided radiotherapy: Dosimetric benefits and treatment time analysis. Radiotherapy Oncol. 2019; 140: 244-9.
|
| [5] |
Byrne TE. A review of prostate motion with considerations for the treatment of prostate cancer. Med Dosim. 2005; 30(3): 155-61.
https://doi.org/10.1016/j.meddos.2005.03.005
|
| [6] |
Lovelock DM, Messineo AP, Cox BW, Kollmeier MA, Zelefsky MJ. Continuous monitoring and intrafraction target position correction during treatment improves target coverage for patients undergoing SBRT prostate therapy. Int J Radiat Oncol Biol Phys. 2015; 91(3): 588-94.
https://doi.org/10.1016/j.ijrobp.2014.10.049
|
| [7] |
Ballhausen H, Reiner M, Kantz S, Belka C, Söhn M. The random walk model of intrafraction movement. Phys Med Biol. 2013; 58(7): 2413-27.
https://doi.org/10.1088/0031-9155/58/7/2413
|
| [8] |
Ten Haken RK, Forman JD, Heimburger DK, Gerhardsson A, McShan DL, Perez-Tamayo C, et al. Treatment planning issues related to prostate movement in response to differential filling of the rectum and bladder. Int J Radiat Oncol Biol Phys. 1991; 20(6): 1317-24.
https://doi.org/10.1016/0360-3016(91)90244-x
|
| [9] |
Sengupta C, Skouboe S, Ravkilde T, Poulsen PR, Nguyen DT, Greer PB, et al. The dosimetric error due to uncorrected tumor rotation during real-time adaptive prostate stereotactic body radiation therapy. Med Phys. 2023; 50(1): 20-9.
https://doi.org/10.1002/mp.16094
|
| [10] |
Sihono DSK, Ehmann M, Heitmann S, von Swietochowski S, Grimm M, Boda-Heggemann J, Lohr F, Wenz F, Wertz H. Determination of intrafraction prostate motion during external beam radiation therapy with a transperineal 4-dimensional ultrasound real-time tracking system. Int J Radiat Oncol Biol Phys. 2018 May 1; 101(1): 136-43.
https://doi.org/10.1016/j.ijrobp.2018.01.040
|
| [11] |
Brennan S, Burleson S, Kostrzewa C, Godoy Scripes P, Subashi E, Zhang Z, et al. SBRT focal dose intensification using an MR-Linac adaptive planning for intermediate-risk prostate cancer: An analysis of the dosimetric impact of intra-fractional organ changes. Radiotherapy Oncol. 2023; 179: 109441.
https://doi.org/10.1016/j.radonc.2022.109441
|
| [12] |
Rose C, Ebert MA, Mukwada G, Skorska M, Gill S. Intrafraction motion during CyberKnife® prostate SBRT: Impact of imaging frequency and patient factors. Phys Eng Sci Med. 2023.
https://doi.org/10.1007/s13246-023-01242-7
|
| [13] |
Kron T, Thomas J, Fox C, Thompson A, Owen R, Herschtal A, et al. Intra-fraction prostate displacement in radiotherapy estimated from pre- and post-treatment imaging of patients with implanted fiducial markers. Radiother Oncol. 2010; 95(2): 191-7.
https://doi.org/10.1016/j.radonc.2010.01.010
|
| [14] |
Gladwish A, Pang G, Cheung P, D’Alimonte L, Deabreu A, Loblaw A. Prostatic displacement during extreme hypofractionated radiotherapy using volumetric modulated arc therapy (VMAT). Radiation Oncol. 2014; 9: 262.
https://doi.org/10.1186/s13014-014-0262-y
|
| [15] |
Mutanga TF, de Boer HCJ, van der Wielen GJ, Hoogeman MS, Incrocci L, Heijmen BJM. Margin evaluation in the presence of deformation, rotation, and translation in prostate and entire seminal vesicle irradiation with daily marker-based setup corrections. Int J Radiat Oncol Biol Phys. 2011 Nov 15; 81(4): 1160-7.
https://doi.org/10.1016/j.ijrobp.2010.09.013
|
| [16] |
Tree AC, Alexander EJ, Van As NJ, Dearnaley DP, Khoo V, et al. Biological dose escalation and hypofractionation: what is there to be gained and how will it best be done? Clin Oncol (R Coll Radiol). 2013 Aug; 25(8): 483-98.
https://doi.org/10.1016/j.clon.2013.05.003
|
| [17] |
Nguyen KA, Peñagaricano JA, McCulloch W. Advances in prostate cancer motion management. Med Dosim. 2020; 45(2): 150-7.
|
| [18] |
Van der Heide UA, Kotte ANTJ, Dehnad H, Hofman P, Lagenijk JJW, van Vulpen M, et al. Analysis of fiducial marker-based position verification in the external beam radiotherapy of patients with prostate cancer. Radiother Oncol. 2007 Jan; 82(1): 38-45.
https://doi.org/10.1016/j.radonc.2006.11.002
|
| [19] |
Harris EJ, Freeman N, Perks J. A national survey of IGRT practice in the UK. Br J Radiol. 2017; 90(1071): 20160666.
https://doi.org/10.1259/bjr.20160666
|
| [20] |
Gupta T, Laskar S, Agarwal JP, Budrukkar A. Indian perspective of quality and access in cancer radiotherapy. J Cancer Policy. 2020; 24: 100235.
|
| [21] |
Radiation Therapy Advisory Group. National framework for radiation therapists’ advanced practice. Radiation Therapist Practice Report, Cancer Council Australia. 2018.
|
| [22] |
Fischer-Valuck BW, Henke LE, Green OL, Kashani R, Yang D, Olsen JR, et al. Clinical implementation of MR-guided pelvic radiotherapy: Feasibility and workflow considerations. Pract Radiat Oncol. 2017; 7(6): 373-81.
https://doi.org/10.1016/j.adro.2017.05.006
|
| [23] |
Paulino AC, Johnstone PAS, Calley CS. The evolving role of the radiation therapist in modern radiotherapy delivery. J Appl Clin Med Phys. 2019; 20(1): 9-17.
https://doi.org/10.1002/acm2.12540
|
| [24] |
Frank SJ, Dong L, Gillin M, Kuban DA, Lee AK, Cheung R, et al. IGRT in prostate cancer: evolution and outcomes. Radiother Oncol. 2014; 111(1): 43-50.
|
| [25] |
Bell LJ, Cox J, Eade T, Rinks M, Kneebone A. The impact of rectal and bladder variability on target coverage during post-prostatectomy intensity-modulated radiotherapy. Radiotherapy and Oncology. 2014 Feb;110(2):245-50.
https://doi.org/10.1016/j.radonc.2013.10.042
|
| [26] |
Kupelian P, Willoughby T, Mahadevan A, Djemil T, Weinstein G, Jani S, et al. Image-guided hypofractionated radiotherapy: outcomes for localized prostate cancer. J Clin Oncol. 2007; 25(31): 5305-10.
https://doi.org/10.1016/j.ijrobp.2006.10.026.
|
| [27] |
Thondykandy R, Saseendran V, Chandran P, Ramesh V, Pillai S, Krishnan S, et al. Challenges in implementing IGRT in low-resource settings: A South Asian perspective. Clin Oncol (R Coll Radiol). 2020; 32(10): e162-9.
|
| [28] |
Jaffray DA, Siewerdsen JH, Wong JW, Martinez AA. Real-time tumor tracking: Current status and future directions. Semin Radiat Oncol. 2009; 19(1): 77-86.
|
| [29] |
Hoogeman MS, van Herk M, de Bois J, Lebesque JV. Strategies to reduce intrafraction motion in prostate radiotherapy. Int J Radiat Oncol Biol Phys. 2008; 71(2): 619-25,
https://doi.org/10.1016/j.radonc.2004.12.010
|
| [30] |
Verma V, Simone CB, Kruser TJ, Lin C, Shah C, Chang JY. Time and resource implications of advanced IGRT in prostate cancer. Pract Radiat Oncol. 2016; 6(6): e271-80.
|
| [31] |
Söhn M, Alber M, Yan D, Ludewig P, Nüsslin F. Variability in bladder and rectum filling and its impact on prostate position. Radiother Oncol. 2010; 95(1): 48-53.
|
| [32] |
Van Herk M, Remeijer P, Rasch C, Lebesque JV. The probability of correct target dosage: Dose-population histograms for deriving treatment margins in radiotherapy. International Journal of Radiation Oncology, Biology, Physics.2000; 47(4): 1121-1135.
https://doi.org/10.1016/S0360-3016(00)00518-6
|
| [33] |
Svensson H, Nilsson K, Gunnlaugsson A, Håkansson U, Hjelstuen M, Muren LP, et al. Variability in motion management techniques among European RTTs. Tech Innov Patient Support Radiat Oncol. 2021; 17: 55-61.
|
| [34] |
Yoshimura R, Nakamura M, Yamada M, Fuji H, Haga A, Shibata T, et al. Motion management strategies in Asian radiotherapy centers: a survey report. Asia Pac J Clin Oncol. 2020; 16(2): e40-6.
|
| [35] |
Coffey M, Leech M, Poole C, Vaandering A, Verellen D, Borras JM. The changing role of RTTs: ESTRO’s vision and strategy. Radiother Oncol. 2016; 119(1): 1-4.
|
| [36] |
Dwyer L, Barten D, Forde E, Sharma DS, van Dyk S. Training needs for RTTs in IGRT implementation: A global perspective. Radiography. 2019; 25(4): e102-9.
|
| [37] |
Datta NR, Samiei M, Bodis S. Access to radiotherapy in low- and middle-income countries. Lancet Oncol. 2014; 15(11): e495-503.
|
Cite This Article
-
APA Style
Roy, S., Talapatra, K., Gupte, A., Mukherjee, U., Parab, A. (2025). Radiation Therapists Perspectives on Motion Management in Definitive Prostate Cancer Radiotherapy: Insights from Indian Clinical Practice. Journal of Cancer Treatment and Research, 13(3), 72-82. https://doi.org/10.11648/j.jctr.20251303.15
 Copy
|
Copy
|
 Download
Download
ACS Style
Roy, S.; Talapatra, K.; Gupte, A.; Mukherjee, U.; Parab, A. Radiation Therapists Perspectives on Motion Management in Definitive Prostate Cancer Radiotherapy: Insights from Indian Clinical Practice. J. Cancer Treat. Res. 2025, 13(3), 72-82. doi: 10.11648/j.jctr.20251303.15
Copy
|
Download
AMA Style
Roy S, Talapatra K, Gupte A, Mukherjee U, Parab A. Radiation Therapists Perspectives on Motion Management in Definitive Prostate Cancer Radiotherapy: Insights from Indian Clinical Practice. J Cancer Treat Res. 2025;13(3):72-82. doi: 10.11648/j.jctr.20251303.15
Copy
|
Download
-
@article{10.11648/j.jctr.20251303.15,
author = {Subrata Roy and Kaustav Talapatra and Ajinkya Gupte and Unmesh Mukherjee and Anand Parab},
title = {Radiation Therapists Perspectives on Motion Management in Definitive Prostate Cancer Radiotherapy: Insights from Indian Clinical Practice
},
journal = {Journal of Cancer Treatment and Research},
volume = {13},
number = {3},
pages = {72-82},
doi = {10.11648/j.jctr.20251303.15},
url = {https://doi.org/10.11648/j.jctr.20251303.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.jctr.20251303.15},
abstract = {Introduction: Prostate cancer is a leading malignancy among men, with radiotherapy (RT) serving as a cornerstone of curative treatment. The precision of external beam radiotherapy (EBRT) is challenged by prostate motion caused by bladder and rectal filling variations, leading to inter- and intra-fraction positional uncertainties. Advanced image-guided radiotherapy (IGRT) and motion management technologies can mitigate these uncertainties; however, their implementation in low- and middle-income countries (LMICs) such as India remains inconsistent due to infrastructure, training, and resource limitations. Radiation therapists (RTTs) play a critical role in accurate patient setup, imaging, and on-treatment verification, yet their perspectives on motion management in prostate radiotherapy are underrepresented in literature. This study aimed to evaluate current RTT practices, challenges, and training needs in India. Materials and Methods: A descriptive, cross-sectional, questionnaire-based survey was conducted over 60 days among RTTs treating prostate cancer with EBRT in India. The online survey, developed through literature review and expert consultation, included 15 mandatory questions across seven domains: demographics, institutional profiles, clinical load, techniques in use, workflow impact, technical challenges, and training preferences. Purposive sampling recruited participants via professional networks, email, and social media. Responses from 202 RTTs were analyzed using descriptive statistics in Microsoft Excel. Results: Daily cone-beam computed tomography (CBCT) was the most widely adopted motion management method (84.7%), followed by respiratory position management (15.8%), surface-guided radiotherapy (15.8%), and real-time tracking (9.4%). Notably, 40.6% reported no dedicated motion management technique. The most common challenges were inconsistent bladder/rectum filling (64.4%), time constraints (34.2%), patient discomfort (24.3%), and technology limitations (14.9%). Motion management increased setup times by 6-15 minutes in 49.5% of cases, with 16.3% of RTTs reporting reduced patient throughput. While 66.9% agreed that current strategies reduce setup uncertainties, responses revealed variability in practice and technology access. Training needs were substantial, with workshops (55.4%), SOP/guideline updates (46.5%), and online modules (34.2%) most preferred. Private institutions accounted for 81.2% of responses, reflecting disparities between urban and rural access to technology. Conclusions: This nationwide survey highlights widespread adoption of CBCT-based IGRT in Indian prostate cancer radiotherapy but also reveals significant gaps in advanced motion tracking, workflow optimization, and standardized patient preparation protocols. Addressing these limitations through national guidelines, equitable technology distribution, and RTT-focused education is essential for consistent, high-quality motion management. Investment in training, patient education, and infrastructure will be critical to bridging practice variability and improving treatment precision across diverse healthcare settings.
},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Radiation Therapists Perspectives on Motion Management in Definitive Prostate Cancer Radiotherapy: Insights from Indian Clinical Practice
AU - Subrata Roy
AU - Kaustav Talapatra
AU - Ajinkya Gupte
AU - Unmesh Mukherjee
AU - Anand Parab
Y1 - 2025/09/23
PY - 2025
N1 - https://doi.org/10.11648/j.jctr.20251303.15
DO - 10.11648/j.jctr.20251303.15
T2 - Journal of Cancer Treatment and Research
JF - Journal of Cancer Treatment and Research
JO - Journal of Cancer Treatment and Research
SP - 72
EP - 82
PB - Science Publishing Group
SN - 2376-7790
UR - https://doi.org/10.11648/j.jctr.20251303.15
AB - Introduction: Prostate cancer is a leading malignancy among men, with radiotherapy (RT) serving as a cornerstone of curative treatment. The precision of external beam radiotherapy (EBRT) is challenged by prostate motion caused by bladder and rectal filling variations, leading to inter- and intra-fraction positional uncertainties. Advanced image-guided radiotherapy (IGRT) and motion management technologies can mitigate these uncertainties; however, their implementation in low- and middle-income countries (LMICs) such as India remains inconsistent due to infrastructure, training, and resource limitations. Radiation therapists (RTTs) play a critical role in accurate patient setup, imaging, and on-treatment verification, yet their perspectives on motion management in prostate radiotherapy are underrepresented in literature. This study aimed to evaluate current RTT practices, challenges, and training needs in India. Materials and Methods: A descriptive, cross-sectional, questionnaire-based survey was conducted over 60 days among RTTs treating prostate cancer with EBRT in India. The online survey, developed through literature review and expert consultation, included 15 mandatory questions across seven domains: demographics, institutional profiles, clinical load, techniques in use, workflow impact, technical challenges, and training preferences. Purposive sampling recruited participants via professional networks, email, and social media. Responses from 202 RTTs were analyzed using descriptive statistics in Microsoft Excel. Results: Daily cone-beam computed tomography (CBCT) was the most widely adopted motion management method (84.7%), followed by respiratory position management (15.8%), surface-guided radiotherapy (15.8%), and real-time tracking (9.4%). Notably, 40.6% reported no dedicated motion management technique. The most common challenges were inconsistent bladder/rectum filling (64.4%), time constraints (34.2%), patient discomfort (24.3%), and technology limitations (14.9%). Motion management increased setup times by 6-15 minutes in 49.5% of cases, with 16.3% of RTTs reporting reduced patient throughput. While 66.9% agreed that current strategies reduce setup uncertainties, responses revealed variability in practice and technology access. Training needs were substantial, with workshops (55.4%), SOP/guideline updates (46.5%), and online modules (34.2%) most preferred. Private institutions accounted for 81.2% of responses, reflecting disparities between urban and rural access to technology. Conclusions: This nationwide survey highlights widespread adoption of CBCT-based IGRT in Indian prostate cancer radiotherapy but also reveals significant gaps in advanced motion tracking, workflow optimization, and standardized patient preparation protocols. Addressing these limitations through national guidelines, equitable technology distribution, and RTT-focused education is essential for consistent, high-quality motion management. Investment in training, patient education, and infrastructure will be critical to bridging practice variability and improving treatment precision across diverse healthcare settings.
VL - 13
IS - 3
ER -
Copy
|
Download