The review study investigates the possibility of using hydrocortisone and thymoquinone together as a medical cream to treat inflammatory skin diseases such as acne, eczema, and psoriasis. The well-known anti-inflammatory actions of hydrocortisone are enhanced by the anti-inflammatory, antioxidant, and wound-healing qualities of thymoquinone, which is derived from Nigella sativa seeds. There is a noticeable lack of prescription creams with these substances, indicating a market gap, even though skin problems are chronic and there are treatment alternatives available. The review highlights the advantages of creams as the recommended dose form because of their ease of use, quick absorption, and patient choice. It also mentions the growing popularity of herbal and natural skincare products, which is consistent with thymoquinone's potential. In order to meet the unmet requirements of patients with dermatological conditions and progress pharmacotherapy in this area, the study recommends the creation and evaluation of a thymoquinone and hydrocortisone cream.
| Published in | Journal of Diseases and Medicinal Plants (Volume 11, Issue 3) |
| DOI | 10.11648/j.jdmp.20251103.12 |
| Page(s) | 90-112 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Anti-inflammatory Properties, Topical Drug Delivery System, Health Related Quality of Life, Chronic Inflammatory Skin Disease
Layers of epidermis | Characteristics | Reference |
|---|---|---|
Stratum corneum | Made up of 15–30 layers of corneocytes, also known as squames, which are keratinocytes. These keratinocytes are deceased. They have a high keratin content, which gives the skin, hair, and nails an impermeable layer. The body is constantly losing this layer. The process of skin cell migration from the stratum basale replaces shed cells. The length of this procedure varies depending on age and certain medical issues, but it usually takes 30 days. | [8] |
Stratum lucidum | Is made up of two or three layers of inactive keratinocytes. It is possible to shave it off or puncture it unknowingly. Only thick skin regions, such as the palms of hands and the soles of feet, exhibit it. Found in calluses. | |
Stratum granulosum | The largest concentration of free nerve terminals extending from the dermis is found in this layer. Unencapsulated dendrites that emerge from a sensory neuron are known as free nerve ends. They are the most prevalent nerve endings in the skin and send sensory data regarding temperature changes, gentle contact, and painful stimuli. They are less susceptible, nevertheless, to sudden variations in stimulus. | [9] |
Stratum spinosum | Includes lymphocytes and Langerhans cells, which are crucial components of the immune system. | |
Stratum basale | The sole layer that continuously divides to create new cells. In the stratum basale, keratinocytes are continuously created and ascend through the layers to the outermost layer. In the skin, keratinocytes are the predominant cell type. Because they are structural cells and carry out vital immunological tasks, they are essential to wound healing. Additionally, melanocytes are generated in the basale layer. Melanin, which they generate, is a factor in skin tone. There are roughly equal numbers of melanocytes in humans. Thus, the quantity of melanin that these melanocytes create in reaction to their surroundings determines the color of skin. Merkel cells, which are capable of combining neuronal and endocrine functions, are also present in this layer. Hormones and neurotransmitters generated locally can be synthesized and stored by them. They convey nociceptive signals and operate as mechanoreceptors for light and selective tactile perception, but not for harsh touch or vibration. | [10] |
Layers of dermis | Characteristics | References |
|---|---|---|
Papillary layer | Interconnects with the skin's surface. This layer's ridges are what create our own fingerprints. Have fibroblasts, which are in charge of producing proteins, elastin, and collagen. Skin gains strength and flexibility from these properties. Have mast cells, which are crucial for the inflammatory response and the production of clots because they generate the chemicals histamine and heparin. Includes macrophages, which are important for the defense system, wound healing, and defense against cancer, hair growth and salt balance. Phagocytosis, in which phagocyte, a kind of white blood cell, engulfs and digests foreign cells and eliminates dead cells, is how they are recognized for eliminating foreign invaders. Contains leukocytes, which are essential to the inflammatory reaction that occurs after a skin injury. Leukocytes are necessary for both proper wound healing and infection clearance. | [12] |
Reticular layer | Situated halfway between the hypodermis, or subcutaneous layer, and the papillary layer. Collagen, blood arteries, nerve endings, T-cells, hair follicles, and glands are its constituent parts. Stem cells found in follicles of hair generate keratinocytes, which eventually develop into hair. They provide epithelial cells for closure of wounds, which is an important part of their involvement in wound healing-lymphocytes are in charge of eliminating infections and cancerous cells. Itching, touch, pressure, vibration, pain, and warmth are all sensed by nerves in the dermis. Damage to or exposure of nerves can cause pain from injuries that penetrate into the dermis. | [13] |
Disease | Diagnosis | Treatment | Reference |
|---|---|---|---|
Fungal infections | |||
Tinea capitis | The most definite test is a culture of lesion scrapings, however quicker findings can be obtained with a potassium hydroxide (KOH) preparation. | The majority of patients have instances that are resistant to treatment, thus systemic antifungal drugs such as terbinafine or other "cidal” antifungal medications like fluconazole, or ketoconazole, itraconazole should be used. Selenium sulfide added to shampoo is advised as an adjunctive treatment. | [44, 45] |
Tinea corporis | For circumscribed lesions, topical therapy twice daily with a cidal antifungal drug is useful. Examples of such agents are oxiconazole, ciclopirox, naftifine, and terbinafine (or more than one of these). Systemic antifungal treatment should be used to treat more diffuse inflammatory disorders. | [46] | |
Viral infections | |||
Herpes simplex | The most reliable test, a culture of lesion scrapings, can take several days to complete. Results from a Tzanck smear that detects large cells infected with herpes may be obtained more quickly and precisely. | An oral antiviral drug, such valacyclovir, can be used to treat new, active lesions in order to reduce the length of the infection and lower the risk of transmission. | [47, 48] |
Molluscum contagiosum | The diagnosis is made using microscopic examination and clinical data. | Although other anecdotal treatments have been proposed, it is advised to physically destroy the lesions with a sharp curette. | [49, 50] |
Bacterial infections | |||
Impetigo | The history and distinctive look of the lesions are the main factors used in the diagnosis of bacterial infections. Any dubious lesions should yield specimens for culture and antibiotic susceptibility testing. | Treatment for all bacterial infections will depend on the culture and sensitivity of the suspicious lesions. Impetigo has been successfully treated with external fusidic acid (Fucidin H; Leo Pharma, Ballerup, Denmark), mupirocin (Bactroban; GSK, Middlesex, United Kingdom), and retapamulin (Altabax; GSK, Middlesex, United Kingdom). | [51, 52] |
Folliculitis/furuncles/carbuncles | Treatment for all bacterial infections depends on the culture and sensitivity of the suspicious lesions. | [53, 54] | |
Methicillin-resistant Staphylococcus aureus (MRSA) | The history and distinctive look of the lesions are the main factors used in the diagnosis of bacterial infections. i. MRSA is to be included in the differential diagnosis of any possible Staphylococcus lesion. ii. "Spider bite” reported to have been taken seriously as a potential indicator of community-associated MRSA (CA-MRSA). iii. Any suspicious lesions should yield specimens for culture and antimicrobial susceptibility testing. | It is critical to identify and send athletes with questionable lesions. i. Athletes who exhibit questionable lesions ought to be kept apart from their teammates. Local susceptibility data must be used to guide antibiotic treatment decisions, which must be made case-by-case. | [55, 56] |
Topical therapy | Systemic therapy (non-biological) | Systemic therapy (biological) | Cytokine inhibitors | Reference |
|---|---|---|---|---|
vitamin D analogues | Vitamin D and its analogue | Monoclonal antibodies | Guselkumab | [58] |
Coal tar | Acitretin | IgG-fusion proteins | Tildrakizumab | |
Dithranol | Etretinate (vitamin A derivative) | Tumor necrosis factor alpha | Ustekinumab | |
Retinoid tazarotene | Pro inflammatory cytokines | Brodalumab | ||
Corticosteroids (tacalcitol or calcitriol) | Ixekizumab | |||
Desoximetasone | Secukinumab |
Treatment | Reason of use | Research | Reference |
|---|---|---|---|
Retinoid | Microcomedone is the major target for acne therapy. Retinoid therapy when used topically acts on follicular keratinocytes to prevent excess blockage of cornification and follicle. Additionally, it could decrease the cytokine synthesis that fuels inflammation. Inflammatory lesions and Comedones are reduced by forty to seventy percent with this kind of therapy. | Analyzing five multicenter randomized investigator-blind studies including nine hundred patients, it was shown that 0.1% adapalene gel was more effective than tretinoin 0.025% gel, however it leds to less irritation. | [61] [62] |
Topical Anti-microbials | Topical antimicrobials including antibiotics and benzoyl peroxide are effective to treat inflammatory disorders. Benzoyl peroxide, having bactericidal action, prevents P. acnes from becoming resistant to antibiotic therapy. It also has modest anti-inflammatory and comedolytic properties. Many topical preparations ranging in potency from 2.5% to 10.0% are available. | Erythromycin and clindamycin have been shown in several randomized controlled studies to decrease inflammatory lesions by 46% to 70% when applied topically. Most of the time, these drugs are well tolerated. | [63] [64] |
Oral anti-biotics | 250–500 mg of tetracycline twice a day 50–200 mg of minocycline each day 100–200 mg of doxycycline each day 500 mg of erythromycin twice a day 80/400 mg or 160/800 mg of trimethoprim/sulfamethoxazole 4 times a day | After using oral antibiotics for at least six weeks, a response is typically observed. The antibiotics may be progressively stopped and only topical treatment continued if control is maintained for a number of months. Because there is a chance of resistance building, systemic antibiotics shouldn't be used to treat minor cases of acne. | [65] [66] |
Hormonal agents | Regardless of the underlying hormonal imbalances, hormonal medications are the second line of therapy for acne. Clinical studies have demonstrated the potential benefits of estrogen-containing oral contraceptives. All formulations are thought to work similarly well, lowering free testosterone levels by boosting sex-hormone-binding globulin. The patient's tolerance and any adverse effects should be taken into consideration while selecting a combination oral contraceptive. | The combination of thirty-five microgram ethinylestradiol and three milligram drospirenone led to a 63% decrease in acne lesions in a randomized controlled research with 128 women, whereas the combination of 35 μg ethinylestradiol and 2 mg cyproterone acetate generated a 59% reduction. Antiandrogen medicine needs to be used for a minimum of three to six months in order to show significant results. | [67] [68] |
Isotretinoin | Isotretinoin affects every mechanism that causes acne; it also has anti-inflammatory qualities and corrects abnormal follicular keratinization. Additionally, it prevents P. acnes from colonizing and lowers sebum production by 70%. Isotretinoin is used for a number of conditions, including severe nodulocystic acne, scarring disease, and less than fifty percent effectiveness with oral antibiotics or hormonal therapies after 4 months. | In a 10-year follow-up research including 88 patients, it was discovered that individuals who had cumulatively received isotretinoin between 120 and 150 mg/kg (30%) had a considerably reduced probability of recurrence than patients who had received less than 120 mg/kg (82%). | [69] [70] |
Treatment | Drugs | Reference |
|---|---|---|
Topical | Creams with antibacterial or antifungal properties, lotions containing calamine, creams with corticosteroids to reduce inflammation, and anti-itch creams with hydrocortisone to relieve itching. Immunomodulators, agents that alter the immune system | [71] |
Oral | Oral antibiotics and antifungal pills are taken for bacterial infections, while generic antihistamines are provided for some allergic responses. | |
Medicinal plants | Flowers of the marigold and chamomile plants, calendula and matricaria, are often used to soothe skin irritation and conditions including dermatitis and eczema. Herbs such as yarrow, aloe vera, witch hazel, and evening primrose oil are also used to treat skin irritation. Herbs with anti-inflammatory properties include purple coneflower sage leaf, ribwort plantain leaf/herb, fenugreek seed, and St. John's wort. | |
Alternatives | diet, oil massage, and cold press |
Drug or combination of pharmaceutical agents | Mechanism of action | Result | Reference |
|---|---|---|---|
Nigella sativa, methotrexate and their combination | An imbalance between the oxidant and anti-oxidant systems is seen in psoriasis. There is antioxidant action in Nigella sativa. In addition to oxidative stress, methotrexate can also inhibit T-cell activation; reduce cell proliferation, and antagonistic effects on folate. | Methotrexate alone has a greater effect than nigella sativa alone, but the combination had the biggest impact. | [128] |
Nigellia sativa | Patients are happier with the ointment since they find its nice aroma and the fact that it doesn't ruin or stain clothing. As with other recipes for ointments, when applied topically, oil in ointment distributes active components straight into the lesion at the application site than other routes of delivery. In fifty percent (50%) of the instances, the crude powder in the form of capsules (500 mg three times daily) improved the psoriatic lesion. Compared to therapy with either the ointment or the combination, the beginning of effect was delayed. Patients did not enjoy capsules because most of them thought that topical treatments, as opposed to oral ones, were a superior way to treat skin conditions like psoriasis. | Nigella sativa has antipsoriatic properties, and the optimum results are achieved when the ointment and oral dosage form are combined. | [129] |
Thymoquinone | Thymoquinone has anti-oxidant, pro-apoptotic, chemoprevention, anti-inflammatory action. | Through a variety of mechanisms of action, thymoquinone has shown therapeutic benefits in the treatment of inflammation and cancer. Research indicates that this substance has strong anti-free radical and superoxide radical scavenging properties while securing the properties of several antioxidant enzymes, including glutathione-S-transferase, catalase, and glutathione peroxidase. | [130] |
Thymoquinone | Its anti-inflammatory and anti-oxidant actions are produced via activating cyclooxygenase-2 (COX2), phosphatidylinositol 3-kinase/protein kinase B (PI3K/AKT), nuclear factor erythroid 2–related factor 2 (Nrf2), and nuclear factor kappa–light-chain–enhancer of activated B (NF-Kβ). | Has been demonstrated to lower various pro-inflammatory cytokines and ROS. | [131] |
Thymoquinone | Nigella sativa is a widely used plant for medicinal properties having a rich cultural and religious past in Unani, Ayurvedic, Chinese, and Arabic medicine. Alkaloids, saponins, thymoquinone, and alpha-hederin are some of the naturally occurring bioactive chemicals that provide N. sativa its many health advantages, which include bronchodilator, diuretic, antihypertensive, antidiabetic, and analgesic properties. Moreover, N. sativa demonstrates antibacterial, reducing inflammatory, and antineoplastic activity, which make it a strong therapeutic choice for the treatment of skin conditions. | The application of N. sativa extract having antibacterial, anticancer, antioxidant, and reducing inflammatory response in the treatment of dermatological disorders, is backed by a large body of scientific research. | [132] |
Thymoquinone | Prior to receiving Nigella Sativa oil, the majority of teenagers with acne vulgaris had serious skin integrity issues. Adolescents with acne vulgaris experienced minor skin integrity disorder following the treatments. | Adolescents with acne vulgaris who receive Nigella Sativa oil administration show improvement in skin integrity. | [133] |
Name of product | Dosage form |
|---|---|
Mother tincture | Tincture containing thymoquinone |
Thymolum | Tincture |
Al hawang cream | Cream |
Black seed miracle skin repair | Cream |
Planta elcaptain (elcaptain ointment with black seed ) | Ointment |
Black cumin containing 2-2.4% thymoquinone | Suspension for allergy symptoms |
Constituent | Activity | Mechanism of action | Reference |
|---|---|---|---|
Thymoquinone | Anti-inflammatory and anti-oxidant | Prevent COX2 inhibiting prostaglandins from being expressed. Reduces certain pro-inflammatory regulators such as interleukin 6 (IL-6), interleukin 1 beta (IL-1β), tumor necrosis factor (TNFα), prostaglandin E2 PGE (2), and interferon γ (IFNγ). | [12 4] |
Hydrocortisone | Anti-inflammatory and anti-itch agent | Exert biological effects by binding to the glucocorticoid receptor. Glucocorticoid receptor complex is formed, DNA binding site of receptor exposed and absence of inflammatory response occurs because of alterations in translation and transcription of proteins. | [129 ] |
cp | Centipoise |
cm | Centimeter |
HLB | Hydrophilic Lipophilic Balance |
SC | Stratum Corneum |
O/W | Oil in Water Emulsion |
W/O | Water in Oil Emulsion |
O/W/O | Oil in Water in Oil Emulsion |
W/O/W | Water in Oil in Water Type Emulsion |
FDA | Food and Drug Authority |
RPM | Revolution Per Minute |
TQ | Thymoquinone |
HC | Hydrocortisone |
COX2 | Cyclooxygenase |
N. sativa | Nigella Sativa |
g | Gram |
| [1] | M. D, "Surfactant Science and Technology, VCH Publishers,” p. 209-247, 1992. |
| [2] | P. A. Kolarsick, "Anatomy and Physiology of the Skin". |
| [3] | N. D. Bikiaris, "Preparation and Investigation of the SPF and Antioxidant Properties of O/W and W/O Emulsions Containing Vitamins A, C and E for Cosmetic Applications,” MDPI, 2023. |
| [4] | " Skin Anatomy, Physiology, and Healing Process ". |
| [5] | D. Palmer, "Skin Anatomy, Physiology, and Healing.” Physiotherapy Wound Care Programme. Plus. 2022. |
| [6] | L. D. L. N. Piipponen M, “The immune functions of keratinocytes in skin wound healing.” International journal of molecular sciences. 21 1 2020. |
| [7] | M. S. Abraham J, “Merkel cells: a collective review of current concepts.” International Journal of Applied and Basic Medical Research, 2019. |
| [8] | R. a. Wilson, “Anatomy and Physiology in Health and Illness". |
| [9] | "Matsui, T. (2023). Epidermal barrier development via corneoptosis: a unique form of cell death in stratum granulosum cells. Journal of Developmental Biology, 11(4), 43. |
| [10] | Y. T. W. J. S. J. B. D. Soliman AM, “Isolation of Skin Leukocytes Uncovers Phagocyte Inflammatory Responses During Induction and Resolution of Cutaneous Inflammation in Fish.” Frontiers in Immunology. 2021. |
| [11] | C. Lalita, "Creams: A Review on Classification, Preparation Methods, Evaluation and its Applications,” Journal of Drug Delivery and Therapeutics, 2020. |
| [12] | H. RJ, "The global burden of skin disease in 2010: an analysis of the prevalence and impact of skin conditions.” 2014. |
| [13] | F. A. Wagener, “Targeting the redox balance in inflammatory skin conditions,” 2013. |
| [14] | A. Rendon, "Psoriasis Pathogenesis and Treatment,” national library of medicine, 2019. |
| [15] | S. H. Ibrahim, "Systemic Immune Inflammatory Index Is Associated with Pustular Psoriasis: A Single Center Retrospective Study,” Journal of Cosmetics, Dermatological Sciences and Applications, vol. 12, 2022. |
| [16] | A. Rendon, "Psoriasis Pathogenesis and Treatment,” international journal of molecular science, 2019. |
| [17] | C. Albanesi, "Immunology of Psoriasis,” science direct, 2019. |
| [18] | A. W. Armstrong, "Psoriasis Prevalence in Adults in the United States,” JAMA dermatology, 2021. |
| [19] | N. Kanda, "Nutrition and Psoriasis,” MDPI, 2020. |
| [20] | G. Egawa and K. Kabashima, “Barrier dysfunction in the skin allergy." |
| [21] | C. palmer, A. Irvine, A. Terron-Kwiatkowski, Y. Zhao, H. Liao, S. Lee, D. Goudie, A. Sandilands, L. Campbell, F. Smith and e. al. "Common loss-of-function variants of the epidermal barrier protein filaggrin are a major predisposing factor for atopic dermatitis.” 2006. |
| [22] | J. thyssen and S. Kezic, "Causes of epidermal filaggrin reduction and their role in the pathogenesis of atopic dermatitis.” 2014. |
| [23] | S. Nakajima, T. Nomura, J. Common and K. Kabashima, "Insights into atopic dermatitis gained from genetically defined mouse models.” 2019. |
| [24] | A. Otsuka, M. Tanioka, Y. Nakagawa, T. Honda, A. Ikoma, Y. Miyachi and K. Kabashima, “Effects of cyclosporine on pruritus and serum IL-31 levels in patients with atopic dermatitis.” 2011. |
| [25] | L. Beck, D. Thaçi, J. Hamilton, N. Graham, T. Bieber, R. Rocklin, J. Ming, H. Ren, R. Kao, E. Simpson and e. a. Dupilumab, “Treatment in Adults with Moderate-to-Severe Atopic Dermatitis.” 2014. |
| [26] | Y. Tokura, “Extrinsic and intrinsic types of atopic dermatitis.” 2010. |
| [27] | H. Yamaguchi, N. Hirasawa, S. Asakawa, K. Okita and Y. Tokura, "Intrinsic atopic dermatitis shows high serum nickel concentration.” 2015. |
| [28] | V. Frings, D. Müller, G. Storz, A. Rossi, H. Sennefelder, C. Adam, M. Goebeler, F. Groeber-Becker and M. Schmidt, “Improved metal allergen reactivity of artificial skin models by integration of Toll-like receptor 4-positive cells.” 2019. |
| [29] | Y. Sawada, T. Honda, S. Hanakawa, S. Nakamizo, T. Murata, Y. Ueharaguchi-Tanada, S. Ono, W. Amano, S. Nakajima, G. Egawa and e. al. "Resolvin E1 inhibits dendritic cell migration in the skin and attenuates contact hypersensitivity responses.” 2015. |
| [30] | Y. Natsuaki, G. Egawa, S. Nakamizo, S. Ono, S. Hanakawa, T. Okada, N. Kusuba, A. Otsuka, A. Kitoh, T. Honda and e. al, "Perivascular leukocyte clusters are essential for efficient activation of effector T cells in the skin.” 2014. |
| [31] | T. Honda, G. Egawa, S. Grabbe and K. Kabashima, “Update of Immune Events in the Murine Contact Hypersensitivity Model: Toward the Understanding of Allergic Contact Dermatitis.” 2013. |
| [32] | L. Parrish, "Psoriasis: symptoms, treatments and its impact on quality of life,” british journal of community nursing, vol. 17, 2013. |
| [33] | P. R, "Global epidemiology of psoriasis: a systematic review of incidence and prevalence.” journal of investigative dermatology, 2012. |
| [34] | A. Egeberg, "Prevalence and characteristics of psoriasis in Denmark: findings from the Danish skin cohort,” BMJ journals, vol. 9. |
| [35] | A. M. Dessie, "Prevalence of Skin Disease and Its Associated Factors Among Primary Schoolchildren: A Cross-Sectional Study from a Northern Ethiopian Town,” pub med, 2022. |
| [36] | R. Hay, "Disease Control Priorities in Developing Countries.” pub med. |
| [37] | A. C. Nicolescu, "Prevalence and Characteristics of Psoriasis in Romania-First Study in Overall Population,” PUB MED, 2021. |
| [38] | D. W. Pleacher MD, "Cutaneous fungal and viral infections in athelets,” 2007. |
| [39] | B. RS. "Skin problems in athletics.” 2002. |
| [40] | M. D. B. M. Kohl TD, "Comparison of topical and oral treatments for tinea gladiatorum.” 1999. |
| [41] | J. R. W. K. e. Fitzpatrick TB, “Cutaneous Fungal infections,” 1997. |
| [42] | A. BB. "New strategies for the diagnosis, treatment, and prevention of herpes simplex in contact sports.” 2004. |
| [43] | B. R. Rogers M, "Diseases of the skin.” 1998. |
| [44] | O. D. Ross GL, "Combination topical treatment of molluscum contagiosum with cantharidin and imiquimod 5% in children: a case series of 16 patients.” 2001. |
| [45] | A. BB. "Sports dermatology.” 2001. |
| [46] | V. A. Koning S, "interventions for impetigo,” 2004. |
| [47] | Chayavichitsilp, P., Buckwalter, J. V., Krakowski, A. C., & Friedlander, S. F. (2009). Herpes simplex. Pediatrics in review, 30(4), 119-130. |
| [48] | L. FD. "Staphylococcus aureus infections.” 1998. |
| [49] | M. M. H. C. Rihn JA, "Community-acquired methicillinresistant Staphylococcus aureus: an emerging problem in the athletic population,” 2005. |
| [50] | G. S. K. S. E.-G. E. L. E. Postier RG, "results of a multicenter, randomized, open-label efficacy and safety study of two doses of tigecycline for complicated skin and skin-structure infections in hospitalized patients,” 2006. |
| [51] | "Hartman-Adams, H., Banvard, C., & Juckett, G. (2014). Impetigo: diagnosis and treatment. American family physician, 90(4), 229-235. |
| [52] | K. D. L. J. e. a. Strauss JS, "Guidelines of care for acne vulgaris management.” 2007. |
| [53] | Dawson, A. L., & Dellavalle, R. P. (2013). Acne vulgaris. Bmj, 346. |
| [54] | S. J. Haider A, "Treatment of acne vulgaris.” JAMA, 2004. |
| [55] | P. M. L. C. e. a. Cunliffe WJ, “A comparison of the efficacy and tolerability of adapalene 0.1% gel vs tretinoin 0.025% gel in patients with acne vulgaris: a meta analysis of five randomized trials.” 1998. |
| [56] | N. J. C. W. Hughes BR, “A double-blind evaluation of topical isotretinoin 0.05%, benzoyl peroxide gel 5% and placebo in patients with acne.” 1992. |
| [57] | J. K. A. P. P. e. a. Mills OH, "Comparing 2.5%, 5%, and 10% benzoyl peroxide on inflammatory acne vulgaris,” 1986. |
| [58] | N. C. Oprica C, "European surveillance study on the antibiotic susceptibility of Propionibacterium acnes.” 2005. |
| [59] | C. J. H. K. e. a. Eady EA, “Erythromycin resistant propionibacteria in antibiotic treated acne patients: association with treatment failure.” 1989. |
| [60] | A. W. Z. H. e. a. Worret I, "Acne resolution rates: results of a single-blind, randomized, controlled, parallel phase III trial with EE/CMA (Belara) and EE/LNG (Microgynon).” 2001. |
| [61] | "ACOG practice bulletin no. 110: noncontraceptive uses of hormonal contraceptives.” 2010. |
| [62] | W. SE. "Comprehensive dermatologic drug therapy.” 2007. |
| [63] | D. C. Hull PR, "Isotretinoin use and subsequent depression and suicide.” 2003. |
| [64] | M. Kort, "inflammatory skin diseases treatment,” skin disease and skin care, vol. 6, 2021. |
| [65] | B. R. Hunt M. J, "A comparative study of gluconolactone versus benzoyl peroxide in the treatment of acne,” 1992. |
| [66] | H. C. U. R. McGuffin M, "Botanical Safety Handbook.” 1997. |
| [67] | B. M. R. "Alternative medicine and dermatology.” 1998. |
| [68] | H. G. Swords G, "Composition of Australian tea tree oil.” 1978. |
| [69] | F. P. S. E. Peirce A, “The American Pharmaceutical Association Practical Guide to Natural Medicines,” 1999. |
| [70] | R. J. H. M. Hausen B. M, "Degradation products of monoterpenes aresensitizing agents in tea tree oil.” 1999. |
| [71] | F. T. “Medical Economics Co.; PDR for Herbal Medicines.” 2000. |
| [72] | A. K. Yarnell E, "Herbal medicine for acne vulgaris.” 2006. |
| [73] | G. J. H. T. R. R. Blumenthal M, "The Complete German Commission E Monographs: Therapeutic Guide to Herbal Medicine,” 1998. |
| [74] | W. M. Bisset N. G, “Herbal Drugs and Phytopharmaceuticals.” 2001. |
| [75] | S. T. M. I. P. H. H. Lyss G, "an anti-inflammatory sesquiterpene lactone from arnica, selectively inhibits transcription factor NF-κB.” 1997. |
| [76] | 77D. A. Brown D. J, "Phytotherapeutic approaches to common dermatological conditions.” 1998. |
| [77] | S. M. R. M. H. A. W. B. G. G. Atherton D. J, "Treatment of atopic eczema with traditional Chinese medicinal plants.” 1992. |
| [78] | A. D. Sheehan M. P, “A controlled trial of traditional Chinese medicinal plants in widespread non-exudative atopic eczema.” 1992. |
| [79] | G.-B. R. "Toxicity of Chinese herbal remedies,” 1992. |
| [80] | W. B. R. M. A. D. B. J. Latchman Y, “The efficacy of traditional Chinese herbal therapy in atopic eczema.” 1994. |
| [81] | L. P. C. L. B. P. W. E. Fung A. Y, “A controlled trial of traditional Chinese herbal medicine in Chinese patients with recalcitrant atopic dermatitis.” 1999. |
| [82] | H. K. L. P. e. a. Chan B. C, "Traditional Chinese medicine for atopic eczema:PentaHerbs formula suppresses inflammatory mediators release from mast cells.” 2008. |
| [83] | L. H. K. S. e. a. Kim E. C, “The bark of Betula platyphylla var. japonica inhibits the developmentof atopic dermatitis-like skin lesions in NC/Nga mice.” 2008. |
| [84] | L. R. A. "Comparison of jewelweed and steroid in the treatment of poison ivy contact dermatitis.” 1958. |
| [85] | R. R. Guin J. D, “Jewelweed treatment of poison ivy dermatitis.” 1980. |
| [86] | B. N. M. J. J. Long D, "Treatment of poison ivy/oak allergic contact dermatitis with an extract of jewelweed.” 1997. |
| [87] | S.-K. M. H. H. L. P. S. M. Korting H. C, "Anti-inflammatory activity of hamamelis distillate applied topically to the skin.” 1993. |
| [88] | D. S. L. J. A. Ledezma E, "Efficacy of ajoene, an organosulphur derived from garlic, in the short-term therapy of tinea pedis.” 1996. |
| [89] | B. M. F. "Bacteriostatic activity of some Australian essential oils.” 1979. |
| [90] | A. P. B. R. Tong M. M, “Tea tree oil in the treatment of tinea pedis.” 1992. |
| [91] | N. D. A. J. Buck D. S, “Comparison of two topical preparations for the treatment of onychomycosis: Melaleuca alternifolia (tea tree) oil and clotrimazole.” 1994. |
| [92] | G. N. L. J. Faoagali J, “Does tea tree oil have a place in the topical treatment of burns?,” 1997. |
| [93] | S. I. “Antifungal activity of the extracts from Galla rhois against Candida albicans.” 2007. |
| [94] | A. S. H. A. A. S. A. S. A. M. Syed T. A, "Management of psoriais with aloe vera extract in a hydrophilic cream: A placebo-controlled, double-blind study.” 1996. |
| [95] | P. L. R. M. e. a. Bernstein J. E, "Effects of topically applied capsaicin on moderate and severe psoriasis vulgaris.” 1986. |
| [96] | B. B. S. V. e. a. Ellis C. N, "A double-blind evaluation of topical capsaicin in pruritic psoriasis.” 1993. |
| [97] | F. S. R. S. R. D. E. M. C. A. Fleischer A. B, “Alternative therapies commonly used within a population of patients with psoriasis,” 1996. |
| [98] | J. P. "Use of alternative medicine by patients with atopic dermatitis and psoriasis.” 1990. |
| [99] | N. S. K. "Topical traditional Chinese medicine.” 1998. |
| [100] | G. J. Zhang H, "Progress of experimental study on treatment of psoriasis by Chinese medicinal monomer and single or compound recipe in Chinese material medica.” 2007. |
| [101] | C. T. P. "Uses of turmeric in dentistry,” 2009. |
| [102] | S. M. H. J. H. M. Heng M. C, “Drug-induces suppression of phosphorylase kinase activity correlates with resolution of psoriasis as assessed by clinical, histological and immuno- histochemical parameters.” 2000. |
| [103] | P. K. T. Y. Aziz H. A, "Solubility of core materials in aqueous polymeric solution effect on microencapsulation of curcumin.” 2007. |
| [104] | M. Z. Ahmad, "Nanoscale Topical Pharmacotherapy in Management of Psoriasis: Contemporary Research and Scope,” MPDI, 2023. |
| [105] | P. Negi, "Thymoquinone-loaded lipid vesicles: a promising nanomedicine for psoriasis,” NIH, 2019. |
| [106] | F. Shad, "The role of thymoquinone, a major constituent of Nigella sativa, in the treatment of inflammatory and infectious diseases.” 2021. |
| [107] | A. M. Yousuf, "Thymoquinone in autoimmune diseases: Therapeutic potential and molecular mechanisms,” Biomedicine and Pharmacotherapy, 2021. |
| [108] | A. Kmail, "How Thymoquinone from Nigella sativa Accelerates Wound Healing through Multiple Mechanisms and Targets,” MPDI, 2023. |
| [109] | E. Niculet, "Influence of phytochemicals in induced psoriasis (Review),” NCBI, 2020. |
| [110] | K. Reich, "The concept of psoriasis as a systemic inflammation: implications for disease management,” JEADV, 2012. |
| [111] | R. Saraceno, "A European perspective on the challenges of managing psoriasis,” PUB MED, 2006. |
| [112] | S. R. Feldman, "The Challenge of Managing Psoriasis: Unmet Medical Needs and Stakeholder Perspectives,” PUB MED, 2016. |
| [113] | C. REID, "Psoriasis and Treatment: Past, Present and Future Aspects,” PUB MED, 2020. |
| [114] | A. Reich, "Speed of clinical improvement in the real-world setting from patient-reported Psoriasis Symptoms and Signs Diary: Secondary outcomes from the Psoriasis Study of Health Outcomes through 12weeks,” JEADV, 2023. |
| [115] | U. Mrowietz, "Psoriasis: to treat or to manage?,” wiley online library, 2014. |
| [116] | P. Rider, "Biologics for Targeting Inflammatory Cytokines, Clinical Uses, and Limitations,” international journal of cell biology, 2016. |
| [117] | K. F. Shad, "The role of thymoquinone, a major constituent of Nigella sativa, in the treatment of inflammatory and infectious diseases,” Clinical and Experimental Pharmacology and Physiology, 2021. |
| [118] | H. Shaterzadeh-Yazdi, "Immunomodulatory and Anti-inflammatory Effects of Thymoquinone,” NIH, 2018. |
| [119] | Y.-J. Surh, "Cancer chemoprevention with dietary phytochemicals,” PUB MED, 2003. |
| [120] | M. Y. Shahani, "Effect of Nigella sativa extract oil on granulation tissue in cutaneous wound: An experimental study in a rabbit model,” Research gate, 2013. |
| [121] | M. R. A. Rahman, "Evaluation of Wound Closure Activity of Nigella sativa, Melastoma malabathricum, Pluchea indica, and Piper sarmentosum Extracts on Scratched Monolayer of Human Gingival Fibroblasts,” Evidence-Based Complementary and Alternative Medicine, 2014. |
| [122] | y. liu, "The Role of Thymoquinone in Inflammatory Response in Chronic Diseases,” 2022. |
| [123] | S. C. McNeill, "Local Enhanced Topical Delivery (LETD) of Drugs: Does It Truly Exist?,” springer link, vol. 9, 1992. |
| [124] | A. Kaur, "Nanoemulsion loaded gel for topical co-delivery of clobitasol propionate and calcipotriol in psoriasis,” pub med, 2017. |
| [125] | M. Pradhan, "Novel colloidal carriers for psoriasis: current issues, mechanistic insight and novel delivery approaches,” pub med, 2013. |
| [126] | K. Mohsin, "Design of Lipid-Based Formulations for Oral Administration of Poorly Water-Soluble Drug Fenofibrate: Effects of Digestion,” PUB MED, 2012. |
| [127] | C. E. Umeyor, "Formulation of gentamicin as surface modified self-nanoemulsifying formulations (SNEFs) improves its anti-pneumococcal activity,” European Journal of Nanomedicine, 2016. |
| [128] | M. Alwadei, "Novel oral dosage regimen based on self-nanoemulsifying drug delivery systems for codelivery of phytochemicals – Curcumin and thymoquinone,” Saudi Pharmaceutical Journal, vol. 27, no. 6, 2019. |
| [129] | K. Khatoon, "Novel nanoemulsion gel containing triple natural bio-actives combination of curcumin, thymoquinone, and resveratrol improves psoriasis therapy: in vitro and in vivo studies,” 2020. |
| [130] | W. J. De Groot A. C, "Contact allergy to tea tree oil. Contact Dermatitis.” 1993. |
| [131] | E. C. "Tea tree oil poisoning.” 1993. |
| [132] | F. Zangeneh, "Psoriasis — Types, Causes and Medication,” 2013. |
| [133] | N. Michael Traub, "Psoriasis – Pathophysiology, Conventional, and Alternative Approaches to Treatment,” 2007. |
| [134] | P. Zhang, "The roles of T cells in psoriasis,” 2023. |
| [135] | X. J, "Advances in the Application of Natural Products and the Novel Drug Delivery Systems for Psoriasis.” europe pmc, 2021. |
| [136] | C. Blome, "Patient-relevant treatment goals in psoriasis,” research gate, 2016. |
| [137] | J. C. D. Res. "A study of clinical profile and quality of life in patients with scabies at a rural tertiary care Centre,” 2016. |
| [138] | K. C, "Global skin disease morbidity and mortality: an update from the global burden of disease study 2013,” 2017. |
| [139] | F. A. Wagener, "Targeting the redox balance in inflammatory skin conditions,” 2013. |
| [140] | Gupta, L., & Aggarwal, A. (2017). Inflammation in Psoriasis and Psoriatic Arthritis. In Psoriasis and Psoriatic Arthritis (pp. 35-44). CRC Press. |
| [141] | A. Ragheb, "The Protective Effect of Thymoquinone, an Anti-Oxidant and Anti-Inflammatory Agent, Against Renal Injury," saudi journal of kidney disease and transplantation, 2009. |
| [142] | S. Darakhshan, "Thymoquinone and its therapeutic potentials," science direct, 2015. |
| [143] | H. Shaterzadeh-Yazdi, "Immunomodulatory and Anti-inflammatory Effects of Thymoquinone," NIH, 2018. |
| [144] | Z. Kohandel, "Anti-inflammatory effects of thymoquinone and its protective effects against several diseases," science direct, 2021. |
| [145] | A. B. Mehta, "Topical corticosteroids in dermatology," indian journal of dermatology, venereology and leprology, 2016. |
APA Style
Hamid, F., Hamid, A. (2025). Exploring the Potential of Thymoquinone and Hydrocortisone Cream for Inflammatory Skin Conditions: A Review Article. Journal of Diseases and Medicinal Plants, 11(3), 90-112. https://doi.org/10.11648/j.jdmp.20251103.12
ACS Style
Hamid, F.; Hamid, A. Exploring the Potential of Thymoquinone and Hydrocortisone Cream for Inflammatory Skin Conditions: A Review Article. J. Dis. Med. Plants 2025, 11(3), 90-112. doi: 10.11648/j.jdmp.20251103.12
@article{10.11648/j.jdmp.20251103.12,
author = {Faizan Hamid and Ayesha Hamid},
title = {Exploring the Potential of Thymoquinone and Hydrocortisone Cream for Inflammatory Skin Conditions: A Review Article
},
journal = {Journal of Diseases and Medicinal Plants},
volume = {11},
number = {3},
pages = {90-112},
doi = {10.11648/j.jdmp.20251103.12},
url = {https://doi.org/10.11648/j.jdmp.20251103.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.jdmp.20251103.12},
abstract = {The review study investigates the possibility of using hydrocortisone and thymoquinone together as a medical cream to treat inflammatory skin diseases such as acne, eczema, and psoriasis. The well-known anti-inflammatory actions of hydrocortisone are enhanced by the anti-inflammatory, antioxidant, and wound-healing qualities of thymoquinone, which is derived from Nigella sativa seeds. There is a noticeable lack of prescription creams with these substances, indicating a market gap, even though skin problems are chronic and there are treatment alternatives available. The review highlights the advantages of creams as the recommended dose form because of their ease of use, quick absorption, and patient choice. It also mentions the growing popularity of herbal and natural skincare products, which is consistent with thymoquinone's potential. In order to meet the unmet requirements of patients with dermatological conditions and progress pharmacotherapy in this area, the study recommends the creation and evaluation of a thymoquinone and hydrocortisone cream.},
year = {2025}
}
TY - JOUR T1 - Exploring the Potential of Thymoquinone and Hydrocortisone Cream for Inflammatory Skin Conditions: A Review Article AU - Faizan Hamid AU - Ayesha Hamid Y1 - 2025/08/25 PY - 2025 N1 - https://doi.org/10.11648/j.jdmp.20251103.12 DO - 10.11648/j.jdmp.20251103.12 T2 - Journal of Diseases and Medicinal Plants JF - Journal of Diseases and Medicinal Plants JO - Journal of Diseases and Medicinal Plants SP - 90 EP - 112 PB - Science Publishing Group SN - 2469-8210 UR - https://doi.org/10.11648/j.jdmp.20251103.12 AB - The review study investigates the possibility of using hydrocortisone and thymoquinone together as a medical cream to treat inflammatory skin diseases such as acne, eczema, and psoriasis. The well-known anti-inflammatory actions of hydrocortisone are enhanced by the anti-inflammatory, antioxidant, and wound-healing qualities of thymoquinone, which is derived from Nigella sativa seeds. There is a noticeable lack of prescription creams with these substances, indicating a market gap, even though skin problems are chronic and there are treatment alternatives available. The review highlights the advantages of creams as the recommended dose form because of their ease of use, quick absorption, and patient choice. It also mentions the growing popularity of herbal and natural skincare products, which is consistent with thymoquinone's potential. In order to meet the unmet requirements of patients with dermatological conditions and progress pharmacotherapy in this area, the study recommends the creation and evaluation of a thymoquinone and hydrocortisone cream. VL - 11 IS - 3 ER -
HITEC Institute of Medical Sciences, Islamabad, Pakistan
Biography: Faizan Hamid, a dedicated medical professional, completed his MBBS from HITECH, Pakistan and is a registered medical practitioner with Pakistan. Furthermore, he holds registration with the General Medical Council (GMC) in the United Kingdom, solidifying his expertise as a doctor. Currently serving as a medical officer, Faizan is actively engaged in advancing healthcare and combating diseases. His current re-search endeavors are focused on the development and characterization of thymoquinone and hydrocortisone cream to address inflammatory skin conditions effectively. Through this research, Faizan aims to unlock the therapeutic potential of these compounds for patients grappling with various skin ailments, particularly focusing on alleviating the burdens of conditions like psoriasis. Faizan Hamid's commitment to en-hancing healthcare and his specialized research in dermatology showcase his passion for making a tangible difference in the lives of those suffering from skin disorders.

Faculty of Pharmaceutical Sciences, University of Punjab, Lahore, Pakistan
Biography: Ayesha Hamid is a dedicated pharmacist who completed her Doctor of Pharmacy degree from the University of Central Pun-jab, Lahore, Pakistan. She is currently pursuing an MPhil in Pharmacology at Punjab University, where she continues to expand her expertise in the field of pharmacological sciences. Ayesha's professional journey as a pharmacist is marked by her commitment to advancing healthcare through research and innovation. Her current research focuses on the development and characterization of a thymoquinone and hydrocortisone cream for treating inflammatory skin conditions. Through this work, she aims to explore the therapeutic potential of these compounds and contribute to the field of dermatological treatments. Ayesha's academic achievements and professional experience reflect her passion for improving patient care and her dedication to finding innovative solutions to health challenges.

Figure 1. Advantages of topical drug delivery system.
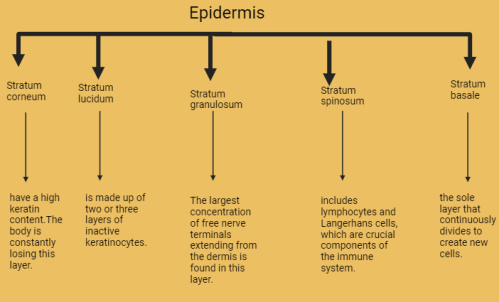
Figure 2. General characteristics of epidermis.
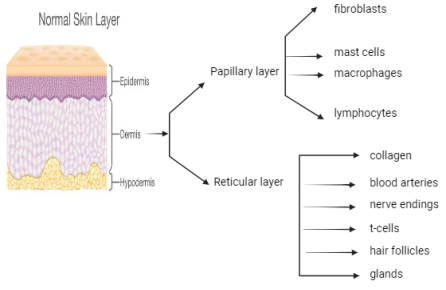
Figure 3. General characteristics of dermis.
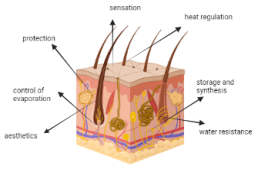
Figure 4. Functions of skin.
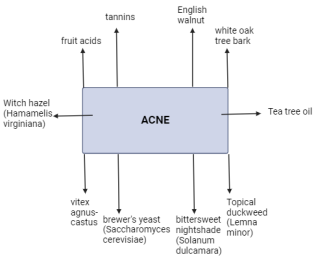
Figure 5. Herbal treatment of acne.
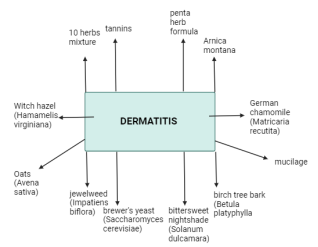
Figure 6. Herbal treatment of dermatitis.
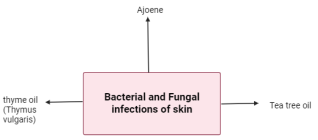
Figure 7. Herbal treatment of bacterial and fungal skin conditions.
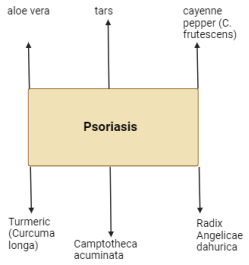
Figure 8. Herbal treatment of psoriasis.
Information

