Abstract
Background: Chronic vulvar discomfort (CVD) affects up to 28% of women but remains diagnostically challenging due to overlapping symptoms and limited application of structured sensory profiling. Objective: To delineate qualitative sensory profiles in women with vulvar dermatoses and vulvodynia, identify dominant pain descriptors, and explore internal sensory hierarchies using comparative statistical methods. Methods: A total of 328 women were enrolled in the prospective DATRIV study. All participants underwent structured pain assessment, Three-Rings Vulvoscopy (TRIV), and targeted vulvar biopsy with histopathologic confirmation. Pain descriptors were categorized according to putative neurophysiological mechanisms (C-fiber vs. A-delta fiber input). Statistical analyses included frequency comparisons, co-occurrence matrices, and data visualization through heatmaps and radar plots. Results: Dull pain was nearly universal (>98%). In vulvar dermatoses, itching (96.2%) and stinging (77.4%) predominated, reflecting C-fiber-mediated pruriceptive pathways. In contrast, vulvodynia demonstrated a significantly higher prevalence of sharp pain, particularly stabbing (45.5%) and knife-like sensations (54.5%), indicating A-delta fiber hyperexcitability. Heatmap analysis revealed distinct internal sensory hierarchies: clustering of pruritic descriptors in dermatoses and a more heterogeneous, dispersed pattern in vulvodynia. Conclusion: Women with chronic vulvar discomfort display distinct sensory phenotypes that align with underlying neurophysiological mechanisms. Sensory profiling distinguishes between inflammatory C-fiber–mediated and neuropathic A-delta–mediated patterns, as well as mixed profiles reflecting contributions from both fiber types, and non-specific or minimal input lacking clear descriptor dominance. Notably, a subset of patients with histologically confirmed dermatoses also displayed A-delta–dominant features, suggesting overlapping neuropathic components. These findings indicate that vulvodynia and vulvar dermatoses may represent interconnected conditions along a shared pathophysiological continuum, where untreated or prolonged vulvodynia may evolve toward inflammatory dermatoses. Recognizing these trajectories may enhance diagnostic precision and support personalized, mechanism-based therapeutic strategies.
|
Published in
|
Journal of Gynecology and Obstetrics (Volume 13, Issue 5)
|
|
DOI
|
10.11648/j.jgo.20251305.14
|
|
Page(s)
|
103-116 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2025. Published by Science Publishing Group
|
Keywords
Chronic Vulvar Discomfort, Vulvodynia, Vulvar Dermatosis, Pain, Dull Pain, Sharp Pain, Sensory Phenotyping, A-delta Phenotype, C-fiber Phenotype, DATRIV Study
1. Introduction
Chronic vulvar discomfort (CVD) represents a highly prevalent yet underrecognized pain syndrome in women’s health, characterized by complex and heterogeneous symptoms. It encompasses a spectrum of persistent or recurrent vulvar sensations—including pain, burning, stinging, soreness, itching, and hypersensitivity—that may present with or without visible pathology. These symptoms occur in both primary conditions such as vulvodynia and in secondary forms including vulvar dermatoses like lichen sclerosus or lichen planus.
Epidemiologic studies estimate that 8–16% of women experience persistent vulvar pain during their lifetime, with up to 28% reporting at least one chronic vulvar symptom in cross-sectional surveys
| [1] | Harlow BL, Stewart EG. A population-based assessment of chronic unexplained vulvar pain: have we underestimated the prevalence of vulvodynia? J Am Med Womens Assoc. 2003; 58(2): 82–88. PMID 12744420 |
| [2] | Reed BD, Harlow SD, Sen A, Legocki LJ, Edwards RM, Arato N, Haefner HK. Prevalence and demographic characteristics of vulvodynia in a population-based sample. Am J Obstet Gynecol. 2012; 206: 170. e1–9. PMID 21963307; https://doi.org/10.1016/j.ajog.2011.08.021 |
| [3] | Arnold LD, Bachmann GA, Rosen R, Kelly S, Rhoads GG. Vulvodynia: characteristics and associations with comorbidities and quality of life. Obstet Gynecol. 2006; 107: 617–624. PMID 16507933; https://doi.org/10.1097/01.AOG.0000199951.26822.27 |
[1-3]
. The prevalence of clinically defined vulvodynia ranges from 8% to 12%, yet the majority of cases remain undiagnosed. Vulvar dermatoses are also frequently associated with pain, with up to 50% of affected women reporting discomfort
| [4] | Goldstein AT, Marinoff SC, Christopher K, Srodon M. Prevalence of vulvar lichen sclerosus in a general gynecology practice. J Reprod Med. 2005; 50 (7): 477–480. PMID 16130842 |
| [5] | Powell J, Wojnarowska F. Lichen sclerosus. Lancet. 1999; 353: 1777–1783. PMID: 10348006; https://doi.org/10.1016/S0140-6736(98)08228-2 |
[4, 5]
. Despite this burden, clinical evaluation remains imprecise. Many patients are treated symptomatically, without an etiologic classification or understanding of underlying mechanisms, resulting in diagnostic delays and reduced quality of life.
A core challenge in evaluating CVD is the subjectivity and heterogeneity of the pain experience. Vulvodynia—the most common diagnosis in this spectrum—is often misattributed to infectious, inflammatory, or psychogenic causes, particularly in early stages
| [6] | Bornstein J, et al. 2015 ISSVD, ISSWSH and IPPS consensus terminology and classification of persistent vulvar pain and vulvodynia. J Low Genit Tract Dis. 2016; 20: 126–130. PMID 27008217; https://doi.org/10.1097/LGT.0000000000000190 |
| [7] | Bohm-Starke N, Ramsay KW, Lytsy P, Nordgren B, Sjöberg I, Moberg K, Flink I. Treatment of provoked vulvodynia: a systematic review. J Sex Med. 2022; 19(5): 789-808. PMID: 35331660; https://doi.org/10.1016/j.jsxm.2022.02.008 |
[6, 7]
. Traditional diagnostic approaches often focus on visible findings or rely solely on pain intensity scales, which, while quantifying severity, do not capture the modality-specific nature of pain. This gap underscores the need for tools that assess the quality—not just the intensity—of pain
| [8] | Dworkin RH, Turk DC, Farrar JT, Haythornthwaite JA, Jensen MP, Katz NP, et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain. 2005; 113: 9–19. PMID 15621359; https://doi.org/10.1016/j.pain.2004.09.012 |
[8]
.
Pain quality refers to the specific sensory character of a patient’s experience, such as burning, stabbing, stinging, or aching. These descriptors reflect distinct neurophysiological pathways and types of nociceptive input. Studies in other chronic pain syndromes have shown that pain quality correlates with specific nerve fiber activation and clinical phenotypes, offering valuable diagnostic and therapeutic insights
. However, in vulvar pain, structured sensory profiling remains largely underutilized.
The International Society for the Study of Vulvovaginal Disease (ISSVD) has acknowledged this limitation by incorporating pain descriptors into its standardized vulvodynia questionnaire, including terms such as burning, rawness, stinging, and itching
| [6] | Bornstein J, et al. 2015 ISSVD, ISSWSH and IPPS consensus terminology and classification of persistent vulvar pain and vulvodynia. J Low Genit Tract Dis. 2016; 20: 126–130. PMID 27008217; https://doi.org/10.1097/LGT.0000000000000190 |
| [11] | ISSVD Vulvodynia Pattern Questionnaire. Available at: Clinical Protocols: ISSVD |
[6, 11]
. This implicitly recognizes that sensory descriptors may reflect different neurophysiological mechanisms. Yet few studies have examined the interrelationships among these descriptors or how their distributions vary across diagnostic groups. Recent efforts to unify terminology, such as the multisocietal consensus of the International Society for the Study of Vulvovaginal Disease (ISSVD), the International Society for the Study of Women’s Sexual Health (ISSWSH), and the International Pelvic Pain Society (IPPS) on descriptors of vulvodynia, have provided an essential framework, but have not addressed hierarchical relationships or fiber-specific mechanisms
| [6] | Bornstein J, et al. 2015 ISSVD, ISSWSH and IPPS consensus terminology and classification of persistent vulvar pain and vulvodynia. J Low Genit Tract Dis. 2016; 20: 126–130. PMID 27008217; https://doi.org/10.1097/LGT.0000000000000190 |
| [12] | Bornstein J, Goldstein AT, Stockdale CK, Bergeron S, Pukall C, Zolnoun D, Coady D. Descriptors of vulvodynia: a multisocietal definition and consensus statement. J Low Genit Tract Dis. 2019; 23: 161-163. PMID: 30768446; https://doi.org/10.1097/LGT.0000000000000461 |
[6, 12]
.
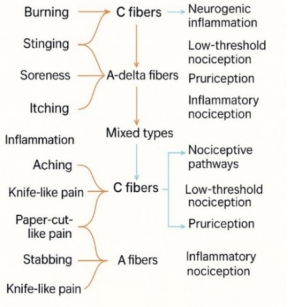
Figure 1. Sensory Profiling of Vulvar Pain. Flowchart representing sensory profiling of vulvar pain based on descriptor-fiber-pathway associations. Burning and itching are linked to C-fiber activity, stinging to A-delta fibers, and tenderness to mixed fiber input. Neurogenic inflammation, pruriception, nerve hyperexcitability, and nociceptive pathways are associated mechanisms.
From a neurophysiological standpoint, pain quality reflects the activation of specific sensory afferents. Thinly myelinated A-delta fibers mediate sharp, fast-onset sensations such as stabbing and knife-like pain, often linked to mechanical stimuli and peripheral nerve hyperexcitability
. These fibers have small receptive fields and conduct at speeds of 5–30 m/s. In contrast, unmyelinated C fibers transmit slower, diffuse sensations such as burning, aching, and itching—sensations typically associated with neurogenic inflammation, pruritus, or deeper tissue involvement
. Polymodal C fibers can also integrate chemical, mechanical, and thermal input, contributing to complex sensations such as irritation. Under conditions of central sensitization, even A-beta fibers may be recruited, leading to tactile allodynia and hypersensitivity
.
Recent literature underscores the relevance of this distinction. Central sensitization in vulvodynia has been associated with more severe pain symptoms across multiple domains and poorer treatment response, highlighting the clinical importance of qualitative descriptors
| [20] | Rubal L, Pereira A, Calles Sastre L, Perez Cejuela BA, Herrero Gamiz S, et al. Managing vulvodynia with central sensitization: challenges and strategies. J Clin Med. 2023; 12(11): 3851. PMID: 37298046; https://doi.org/10.3390/jcm12113851 |
[20]
. Unique inflammatory profiles have also been identified in painful compared with non-painful vulvar sites, suggesting that pain quality reflects not only fiber type but also local immune activation
| [21] | Falsetta ML. Editorial: Vulvodynia and beyond: innate immune sensing, microbes, inflammation, and chronic pain. Front Cell Infect Microbiol. 2023; 13: 1338659. PMID: 38145051; https://doi.org/10.3389/fcimb.2023.1338659 |
[21]
. Furthermore, a recent scoping review emphasized persistent diagnostic gaps and the need for novel approaches to symptom classification in vulvodynia research
| [22] | Lountzi A, Abhyankar P, Durand H. A scoping review of vulvodynia research: diagnosis, treatment, and care experiences. Womens Health (Lond). 2025; 17: 17455057251345946. PMID: 40525542; https://doi.org/10.1177/17455057251345946 |
[22]
.
Figure 1 provides a conceptual model linking qualitative descriptors to sensory fiber types and their associated mechanisms. Burning and aching are mediated by C fibers; stabbing and knife-like pain by A-delta fibers; tenderness and irritation involve mixed input
. These associations serve as the foundation for the sensory phenotyping used in the present study. Consequently, profiling these qualities could help differentiate between predominantly inflammatory, neuropathic, or dysfunctional pain types—a classification increasingly used in pain medicine
| [23] | Bornstein S, Bornstein J. [THE NEW CONSENSUS TERMINOLOGY OF CHRONICVULVAR PAIN AND VULVODYNIA]. Harefuah. 2019; 158(12): 812-816. Hebrew. PMID: 31823537. |
[23]
.
The DATRIV study (Diagnostic Accuracy of the Three Rings Vulvoscopy) was initiated to address diagnostic uncertainty in CVD. As a prospective experimental investigation, its primary aim was to evaluate the diagnostic accuracy of a novel Three Rings Vulvoscopy (TRIV) method against histopathological confirmation
| [24] | Harni V, Babic D, Hadzavdic S, Barisic D. Diagnostic accuracy of the Vulvoscopy Index for detection of vulvar dermatosis (DATRIV study, Part 1). J Gynecol Obstet. 2022; 10(1): 39-47. https://doi.org/10.11648/j.jgo.20221001.16 |
| [25] | Harni V, Babic D, Hadzavdic S, Barisic D. Clinical value of the N-S-P scheme for detection of vulvar dermatosis (DATRIV study, Part 2). J Gynecol Obstet. 2022; 10(3): 159-166. https://doi.org/10.11648/j.jgo.20221003.11 |
[24, 25]
.
Beyond this primary objective, the study generated important secondary outcomes. It demonstrated that vulvodynia is not an “invisible” disorder but is associated with characteristic nonspecific lesions whose type and distribution can be systematically localized across the three vulvar rings. In addition, sensory profiling of vulvar pain was pre-specified as a secondary outcome measure. This substudy used the same cohort to investigate whether qualitative pain descriptors—analyzed in relation to clinical findings and histology—could reveal distinct fiber-specific mechanisms differentiating vulvodynia from vulvar dermatoses.
The aim of the present analysis was therefore to construct qualitative sensory profiles of vulvar pain and to examine whether the distribution and internal hierarchy of pain descriptors reflect neurophysiological differentiation between the two conditions.
2. Methods
2.1. Study Design and Population
This analysis is a sub-study of the DATRIV project (Diagnostic Accuracy of Three Rings Vulvoscopy), a prospective experimental investigation with diagnostic intervention conducted at the Polyclinic Harni in Zagreb, Croatia, from December 1, 2011, to December 31, 2016. The study's primary objective was to improve diagnostic precision in women with chronic vulvar discomfort using a novel vulvoscopy technique, TRIV
| [24] | Harni V, Babic D, Hadzavdic S, Barisic D. Diagnostic accuracy of the Vulvoscopy Index for detection of vulvar dermatosis (DATRIV study, Part 1). J Gynecol Obstet. 2022; 10(1): 39-47. https://doi.org/10.11648/j.jgo.20221001.16 |
| [25] | Harni V, Babic D, Hadzavdic S, Barisic D. Clinical value of the N-S-P scheme for detection of vulvar dermatosis (DATRIV study, Part 2). J Gynecol Obstet. 2022; 10(3): 159-166. https://doi.org/10.11648/j.jgo.20221003.11 |
[24, 25]
. In addition to its diagnostic focus, the study incorporated sensory phenotyping as a predefined secondary objective, designed to capture the spectrum of pain profiles and to provide insight into their clinical and histopathological correlates.
A total of 328 women aged 18 to 75 years were enrolled. Symptomatic participants were recruited from the specialized vulvoscopy section, whereas asymptomatic women were enrolled from the aesthetic gynecology unit. The latter group consisted of patients scheduled for elective vulvar procedures who voluntarily consented to donate tissue samples for further analysis after being fully informed about the purpose of the study. Participants were stratified into four diagnostic categories based on clinical history, gynecologic examination, vulvoscopic findings, and responses to the ISSVD Vulvodynia Pattern Questionnaire. Asymptomatic women were subdivided into those with normal vulvar appearance and those with nonspecific vulvar changes. Symptomatic patients with vulvar symptoms persisting for more than three months were classified as having either primary vulvar pain (vulvodynia) or secondary pain associated with histologically confirmed vulvar dermatoses. The diagnosis of vulvodynia was based on the 2015 ISSVD consensus criteria, while dermatoses were confirmed by biopsy where clinically indicated
| [6] | Bornstein J, et al. 2015 ISSVD, ISSWSH and IPPS consensus terminology and classification of persistent vulvar pain and vulvodynia. J Low Genit Tract Dis. 2016; 20: 126–130. PMID 27008217; https://doi.org/10.1097/LGT.0000000000000190 |
[6]
.
Exclusion criteria included active vulvovaginal infection, gynecologic or dermatologic malignancy, incomplete data, or deviation from the study protocol. All participants underwent a structured pain assessment, standardized gynecological examination, complete TRIV vulvoscopy, and biopsy with histopathologic analysis. Vulvar biopsies were part of routine clinical care in symptomatic women, while asymptomatic participants were recruited from those undergoing elective labiaplasty.
2.2. Pain Assessment and Semantic Descriptor Profiling
Pain quality was assessed using a standardized sensory pain questionnaire developed specifically for the DATRIV study, adapted from the ISSVD Vulvodynia Pattern Questionnaire
| [11] | ISSVD Vulvodynia Pattern Questionnaire. Available at: Clinical Protocols: ISSVD |
[11]
. Participants selected the descriptors that best characterized their symptoms over the preceding four weeks.
Each descriptor was mapped to a corresponding sensory fiber type and its presumed neurophysiological mechanism, based on current pain physiology literature
| [10] | Backonja MM, Krause SJ. Neuropathic pain questionnaire – short form. Clin J Pain. 2003; 19(5): 315-316. PMID: 12966257; https://doi.org/10.1097/00002508-200309000-00005 |
| [13] | Treede RD, Mayer RA, Raja N, Campbell N. Peripheral and central mechanisms of cutaneous hyperalgesia. Prog Neurobiol. 1992; 38(4): 397-421. PMID: 1574584; https://doi.org/10.1016/0301-0082(92)90027-C |
| [16] | Schmelz M. Itch and pain. Neurosci Biobehav Rev. 2010; 34: 171–176. PMID: 19146873; https://doi.org/10.1016/j.neubiorev.2008.12.004 |
| [17] | Ikoma A, Steinhoff M, Ständer S, Yosipovitch G. The neurobiology of itch. Nat Rev Neurosci. 2006; 7: 535-547. PMID: 16791143; https://doi.org/10.1038/nrn1950 |
| [20] | Rubal L, Pereira A, Calles Sastre L, Perez Cejuela BA, Herrero Gamiz S, et al. Managing vulvodynia with central sensitization: challenges and strategies. J Clin Med. 2023; 12(11): 3851. PMID: 37298046; https://doi.org/10.3390/jcm12113851 |
| [21] | Falsetta ML. Editorial: Vulvodynia and beyond: innate immune sensing, microbes, inflammation, and chronic pain. Front Cell Infect Microbiol. 2023; 13: 1338659. PMID: 38145051; https://doi.org/10.3389/fcimb.2023.1338659 |
| [22] | Lountzi A, Abhyankar P, Durand H. A scoping review of vulvodynia research: diagnosis, treatment, and care experiences. Womens Health (Lond). 2025; 17: 17455057251345946. PMID: 40525542; https://doi.org/10.1177/17455057251345946 |
| [23] | Bornstein S, Bornstein J. [THE NEW CONSENSUS TERMINOLOGY OF CHRONICVULVAR PAIN AND VULVODYNIA]. Harefuah. 2019; 158(12): 812-816. Hebrew. PMID: 31823537. |
| [16] | Schmelz M. Itch and pain. Neurosci Biobehav Rev. 2010; 34: 171–176. PMID: 19146873; https://doi.org/10.1016/j.neubiorev.2008.12.004 |
| [17] | Ikoma A, Steinhoff M, Ständer S, Yosipovitch G. The neurobiology of itch. Nat Rev Neurosci. 2006; 7: 535-547. PMID: 16791143; https://doi.org/10.1038/nrn1950 |
| [18] | Woolf CJ. Central sensitization: implications for the diagnosis and treatment of pain. Pain. 2011; 152(3 Suppl): S2-S15. PMID: 20961685; https://doi.org/10.1016/j.pain.2010.09.030 |
| [19] | Scholz J, Finnerup NB, Attal N, Aziz Q, Baron R, Bennett MI, et al. Classification of pain: a pragmatic proposal for ICD-11. Pain. 2019; 160(1): 53-59. PMID: 30586071; https://doi.org/10.1097/j.pain.0000000000001365 |
| [20] | Rubal L, Pereira A, Calles Sastre L, Perez Cejuela BA, Herrero Gamiz S, et al. Managing vulvodynia with central sensitization: challenges and strategies. J Clin Med. 2023; 12(11): 3851. PMID: 37298046; https://doi.org/10.3390/jcm12113851 |
| [21] | Falsetta ML. Editorial: Vulvodynia and beyond: innate immune sensing, microbes, inflammation, and chronic pain. Front Cell Infect Microbiol. 2023; 13: 1338659. PMID: 38145051; https://doi.org/10.3389/fcimb.2023.1338659 |
| [22] | Lountzi A, Abhyankar P, Durand H. A scoping review of vulvodynia research: diagnosis, treatment, and care experiences. Womens Health (Lond). 2025; 17: 17455057251345946. PMID: 40525542; https://doi.org/10.1177/17455057251345946 |
| [23] | Bornstein S, Bornstein J. [THE NEW CONSENSUS TERMINOLOGY OF CHRONICVULVAR PAIN AND VULVODYNIA]. Harefuah. 2019; 158(12): 812-816. Hebrew. PMID: 31823537. |
| [24] | Harni V, Babic D, Hadzavdic S, Barisic D. Diagnostic accuracy of the Vulvoscopy Index for detection of vulvar dermatosis (DATRIV study, Part 1). J Gynecol Obstet. 2022; 10(1): 39-47. https://doi.org/10.11648/j.jgo.20221001.16 |
| [25] | Harni V, Babic D, Hadzavdic S, Barisic D. Clinical value of the N-S-P scheme for detection of vulvar dermatosis (DATRIV study, Part 2). J Gynecol Obstet. 2022; 10(3): 159-166. https://doi.org/10.11648/j.jgo.20221003.11 |
| [26] | Yosipovitch G, Greaves MW, Schmelz M. Itch. Lancet. 2003; 361(9358): 690-694. PMID: 12606187; https://doi.org/10.1016/S0140-6736(03)12570-6 |
| [27] | Serra J, Bostock H, Sola R, Aleu J, Garcia E, et al. Microneurographic identification of spontaneous activity in C-nociceptors in neuropathic pain states in humans and rats. Pain. 2012; 153(1): 42-55. PMID: 21993185; https://doi.org/10.1016/j.pain.2011.08.015 |
| [28] | Dukefoss TT, Kleggetveit IP, Helas T, Jørum E. Pain and small-fiber affection in hereditary neuropathy with liability to pressure palsies (HNPP). Scand J Pain. 2020; 20(1): 61-68. https://doi.org/10.1515/sjpain-2019-0090 |
| [29] | Garcia-Larrea L, Peyron R. Pain matrices and neuropathic pain matrices: a review. Pain. 2013; 154 Suppl 1: S29–43. PMID: 24021862; https://doi.org/10.1016/j.pain.2013.09.001 |
[10, 13, 16, 17, 20-23, 16-29]
. This mapping reflects the contemporary understanding of afferent fiber function:
1) Burning: Mediated by C-fibers; associated with neurogenic inflammation and central sensitization.
2) Stinging: Mediated by A-delta fibers; indicates peripheral nerve hyperexcitability and neuropathic pain features.
3) Soreness: Involves deep C-fiber nociceptors; reflects subepithelial or muscular inflammation.
4) Irritation: Arises from polymodal nociceptors with mixed fiber input; suggests low-threshold nociceptive activation.
5) Itching: Transmitted by pruriceptive C-fibers; involves mast cell activation and neuroimmune interactions.
6) Inflammation: C-fiber–related; indicative of inflammatory nociception driven by immune signaling.
7) Aching: Mediated by deep somatic C-fibers; typically reflects visceral or myofascial pain.
8) Knife-like pain: A-delta fiber–mediated; associated with mechanical allodynia and neuropathic states.
9) Paper-cut-like pain: A-delta fiber–mediated; likely reflects superficial mechanical microtrauma.
10) Stabbing: A-delta fiber–mediated; reflects localized, punctate nociceptive input.
This neuroanatomical framework supported the development of sensory profiles and allowed for mechanistic interpretation of pain quality across diagnostic groups.
2.3. Sensory Phenotyping
Based on the distribution of selected descriptors, patients were categorized into one of four sensory phenotypes:
1) C-fiber dominant phenotype: Burning or stinging sensation
2) A-delta dominant phenotype: Sharp or stabbing sensations
3) Mixed phenotype: Combination of C-fiber and A-delta fiber descriptors
4) Non-specific or minimal sensory input.
These phenotypes were analyzed in relation to clinical diagnoses to determine whether specific patterns of afferent activation corresponded with vulvar dermatosis or vulvodynia.
2.4. Statistical Analysis
Descriptive statistics were used to summarize demographic and clinical variables. Frequencies of pain descriptors were compared across diagnostic categories using the chi-squared test with Yates’ correction or Fisher’s exact test, depending on cell distribution. Differences between proportions were analyzed using the z-test for two proportions or Student’s t-test where appropriate.
Continuous variables were tested for normality using the Kolmogorov-Smirnov test. Normally distributed data were compared using t-tests or one-way ANOVA with Tukey’s HSD for post hoc analysis. Non-normally distributed data were analyzed with the Mann-Whitney U test or Kruskal-Wallis ANOVA as appropriate.
To evaluate internal descriptor relationships, co-occurrence matrices were constructed, and p-value heatmaps were generated to visualize hierarchical patterns. These visualizations allowed for the identification of dominant pain descriptors and clustering tendencies within each diagnostic group.
All statistical analyses were conducted using SPSS 12.0 (IBM Corp., Armonk, NY, USA), with a significance level set at p < 0.05.
2.5. Ethical Approval
All participants were informed about the voluntary nature of study participation and could decline the questionnaire without consequence. Written informed consent was obtained from all women undergoing vulvoscopy and biopsy, ensuring understanding of the procedures, risks, and rights.
The study was approved by the Institutional Review Board of Polyclinic Harni (Approval Number: 20111201001) and was registered on ClinicalTrials. gov (Identifier: NCT02732145), ensuring transparency and adherence to ethical research standards.
3. Results
3.1. Dull Pain Profiles in Vulvar Dermatosis and Vulvodynia
Table 1 summarizes, and
Figure 2 illustrates the frequency of dull or slow pain descriptors in women with vulvar dermatosis and vulvodynia (each group
n = 82). Dull pain was nearly universal in both conditions (100% in dermatosis vs. 98.8% in vulvodynia,
p = 0.316), underscoring its central role in the sensory experience of chronic vulvar discomfort.
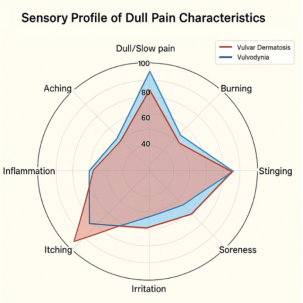
However, important differences were observed in the distribution of individual descriptors. Burning was significantly more frequent in women with vulvodynia (45.1%) than in those with dermatosis (26.8%) (p = 0.015), as were soreness (65.8% vs. 45.1%, p = 0.008) and irritation (58.5% vs. 42.7%, p = 0.042). In contrast, itching was significantly more common in dermatosis (96.3%) than in vulvodynia (76.8%) (p < 0.001), indicating a more pruriceptive profile in dermatosis-related pain.
Table 1. Frequency of Dull Pain Descriptors in Women with Vulvar Dermatosis and Vulvodynia. Dull pain was nearly universal in both groups, but itching was significantly more prevalent in dermatosis, while burning, soreness, and aching were more frequent in vulvodynia.
Vulvar Pain Characteristics | Vulvar Dermatosis N = 82 | Vulvodynia N = 82 | p value |
Dull/Slow Pain | 82 (100%) | 81 (98.8%) | p = 0.316 |
Burning | 22 (26.8%) | 37 (45.1%) | p = 0.015* |
Stinging | 65 (79.3%) | 66 (80.5%) | p = 0.846 |
Soreness | 37 (45.1%) | 54 (65.8%) | p = 0.008* |
Irritation | 35 (42.7%) | 48 (58.5%) | p = 0.042* |
Itching | 79 (96.3%) | 63 (76.8%) | p = 0.000** |
Inflammation | 38 (46.3%) | 49 (59.8%) | p = 0.085 |
Aching | 21 (25.6%) | 45 (54.9%) | p = 0.000** |
Figure 2. Sensory Profile of Dull Pain Characteristics. This is a radar chart comparing the distribution of dull pain descriptors between women diagnosed with vulvar dermatosis (red) and vulvodynia (blue). Shared descriptors include stinging and soreness, while aching and burning are more prevalent in vulvodynia, and itching dominates dermatosis.
Table 1 compares the frequency of dull pain descriptors in both diagnostic groups.
Figure 3 presents a radar chart showing the distribution of these descriptors, with red representing dermatosis and blue representing vulvodynia.
Both groups show a high prevalence of dull/slow pain overall, but the specific sensory qualities differ. Vulvar dermatosis is characterized by dominant itching and stinging, suggesting a pruriceptive profile, while vulvodynia shows higher frequencies of burning and soreness, indicative of deeper nociceptive and possibly neuropathic mechanisms.
Aching also differed significantly, being more prevalent in vulvodynia (54.9%) compared to dermatosis (25.6%) (p < 0.001). No significant differences were found for stinging (79.3% vs. 80.5%; p = 0,846) or inflammation (46.3% vs. 59.8%; p = 0,085).
3.2. Sharp Pain Patterns in Vulvar Dermatosis and Vulvodynia
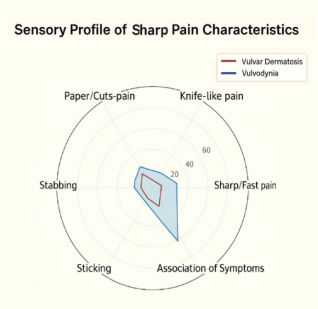
Figure 3. Sensory Profile of Sharp Pain Characteristics. The radar chart illustrates that sharp pain descriptors, such as stabbing and paper-cut-like pain, were significantly more prevalent in vulvodynia, suggesting A-delta fiber hyperexcitability. In contrast, sharp sensations are less pronounced and more diffusely distributed in vulvar dermatosis.
Figure 3 and
Table 2 present the distribution of sharp or fast pain descriptors in women diagnosed with vulvar dermatosis and vulvodynia. Sharp pain was significantly more frequent in vulvodynia (37.8%) than in dermatosis (14.6%) (p = 0.001), indicating a clear sensory divergence likely mediated by A-delta fiber activation or central sensitization mechanisms.
While dull pain was dominant in both groups (p < 0.0001), the presence of sharp sensations suggests a mechanistic distinction between the two conditions.
Among specific descriptors, stabbing pain was significantly more common in vulvodynia (20.7%) than in dermatosis (7.3%) (p = 0.012), as was paper-cut-like pain (12.2% vs. 3.7%; p = 0.042). Knife-like pain showed a borderline difference (15.8% vs. 6.1%; p = 0.051), while sticking pain trended higher in vulvodynia (22.0%) compared to dermatosis (11.0%) (p = 0.067).
Importantly, 78.0% of women with vulvodynia reported at least one sharp or stabbing sensation, compared to 29.3% of those with dermatosis (p < 0.0001), reinforcing the idea that sharp pain is a defining feature of the vulvodynia sensory phenotype.
Table 2 outlines the frequency and statistical comparisons for sharp descriptors in both diagnostic groups.
Figure 4 depicts a radar chart comparing the distribution of sharp pain types, again with red indicating dermatosis and blue indicating vulvodynia.
Table 2. Frequency of Sharp Pain Descriptors in Women with Vulvar Dermatosis and Vulvodynia. Sharp pain was significantly more common in vulvodynia, particularly stabbing and paper-cut-like sensations, indicating greater A fiber activation.
Vulvar Pain Characteristics | Vulvar Dermatosis N = 82 | Vulvodynia N = 82 | p value |
Sharp/Fast Pain | 12 (14.6%) | 31 (37.8%) | p = 0.001** |
Knife-Like | 5 (6.1%) | 13 (15.8%) | p = 0.051 |
Paper-Cuts | 3 (3.7%) | 10 (12.2%) | p = 0.042* |
Stabbing | 6 (7.3%) | 17 (20.7%) | p = 0.012* |
Sticking | 9 (11.0%) | 18 (22.0%) | p = 0.067 |
Association Of Symptoms | 24 (29.3%) | 64 (78.0%) | p = 0.0000** |
t-test Proportion (Dull vs. Sharp Pain) | p = 0.0000** | p = 0.0000** | |
3.3. Internal Sensory Hierarchies: Heatmap Analysis
Pairwise statistical comparisons of dull pain descriptors are summarized in
Tables 3 and 4.In vulvar dermatosis, itching and stinging were significantly more frequent than all other descriptors (p < 0.001 for most comparisons), defining a pruriceptive hierarchy consistent with superficial C-fiber activation.
In vulvodynia, stinging emerged as the most statistically dominant descriptor, occurring significantly more often than burning, soreness, irritation, inflammation, and aching (p < 0.05 for all). Itching showed variable statistical weight, while aching did not differ significantly from other symptoms. These patterns indicate that itching–stinging dominance characterizes dermatosis, whereas stinging in vulvodynia may represent a neurophysiological marker linked to A-delta fiber hyperexcitability.
Table 3. Pairwise Statistical Comparison of Dull Pain Descriptors in Vulvar Dermatosis. Itching and stinging were significantly more frequent than all other descriptors, reflecting a pruriceptive hierarchy.
Dull/Slow Pain in Vulvar Dermatosis (N=82) | t-test proportion |
Itching vs. | Burning | p=0.000** |
Itching vs. | Stinging | p=0.001** |
Itching vs. | Soreness | p=0.000** |
Itching vs. | Irritation | p=0.000** |
Itching vs. | Inflammation | p=0.000** |
Itching vs. | Aching | p=0.000** |
Stinging vs. | Burning | p=0.000** |
Stinging vs. | Soreness | p=0.000** |
Stinging vs. | Irritation | p=0.000** |
Stinging vs. | Inflammation | p=0.000** |
Stinging vs. | Aching | p=0.000** |
Aching vs. | Burning | p=0.859 |
Aching vs. | Soreness | p=0.009* |
Aching vs. | Irritation | p=0.021* |
Aching vs. | Inflammation | p=0.006* |
Table 4. Pairwise Statistical Comparison of Dull Pain Descriptors in Vulvodynia. Stinging emerged as the dominant descriptor, with weaker or non-significant associations for aching and inflammation.
Dull/Slow Pain in Vulvodynia (N=82) | t-test proportion |
Stinging vs. | Burning | p=0.000** |
Stinging vs. | Soreness | p=0.034* |
Stinging vs. | Irritation | p=0.002* |
Stinging vs. | Itching | p=0.567 |
Stinging vs. | Inflammation | p=0.004* |
Stinging vs. | Aching | p=0.000** |
Itching vs. | Burning | p=0.000** |
Itching vs. | Stinging | p=0.5675 |
Itching vs. | Soreness | p=0.1201 |
Itching vs. | Irritation | p=0.012* |
Itching vs. | Inflammation | p=0.019* |
Itching vs. | Aching | p=0.003* |
Aching vs. | Burning | p=0.211 |
Aching vs. | Soreness | p=0.151 |
Aching vs. | Irritation | p=0.636 |
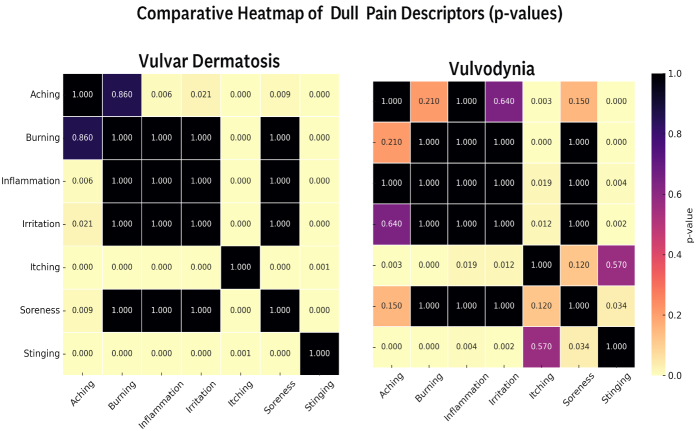
To visualize these relationships, a comparative heatmap was generated (
Figure 4). In dermatosis, the map showed a concentrated clustering of itching and stinging, indicating surface-level sensory dominance typical of inflammatory or irritative conditions.
In vulvodynia, clustering was more dispersed, with burning and aching tending to co-occur, consistent with deeper and more diffuse nociceptive processing.
Figure 4. Comparative Heatmap of Dull Pain Descriptors (p values). This heatmap illustrates the pairwise p-values among dull pain descriptors reported in vulvar dermatosis (left) and vulvodynia (right). Yellow indicates significant associations; black indicates non-significance. In dermatosis, itching and stinging dominate, while vulvodynia shows overlapping patterns with partial burning–aching clustering.
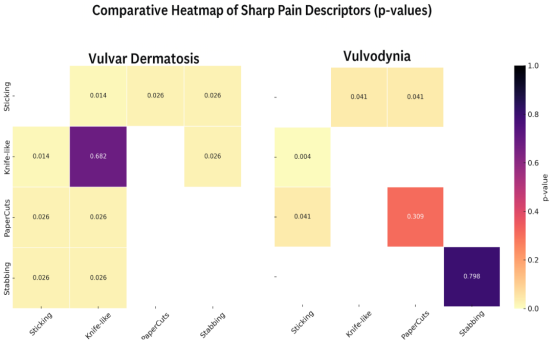
Sharp pain profiles were less hierarchically organized. In patients with vulvar dermatosis (
Tables 5-6). In dermatosis, sticking was reported more frequently than paper-cut–like pain (p = 0.014), while other comparisons were non-significant. In vulvodynia, sticking also showed weak statistical dominance over paper-cut–like pain (p = 0.041), but the overall distribution was diffuse, suggesting heterogeneous A-delta activation and possible central modulation.
Table 5. Pairwise Statistical Comparison of Sharp Pain Descriptors in Vulvar Dermatosis. Sticking was more frequent than paper-cut-like pain, but other sharp descriptors showed no clear dominance.
Sharp/Fast Pain in Vulvar Dermatosis (N=12) | t-test proportion |
Sticking | Knife-like | p=0.098 |
Sticking | Paper-Cuts | p=0.014* |
Sticking | Stabbing | p=0.206 |
Stabbing | Knife-like | p=0.682 |
Stabbing | Paper-Cuts | p=0.206 |
Table 6. Pairwise Statistical Comparison of Dull Pain Descriptors in Vulvodynia. Sticking pain weak statistical dominance; other sharp descriptors were more diffusely distributed, suggesting heterogeneous A delta activation.
Sharp/Fast Pain in Vulvodynia (N=31) | t-test proportion |
Sticking | Knife-like | p=0.204 |
Sticking | Paper-cuts | p=0.041* |
Sticking | Stabbing | p=0.798 |
Stabbing | Knife-like | p=0.309 |
Stabbing | Paper-cuts | p=0.073 |
The corresponding heatmap (
Figure 5) further illustrates these patterns. In dermatosis, sticking was the most differentiated descriptor, whereas in vulvodynia, the associations lacked clear structure, reinforcing the interpretation of a heterogeneous, possibly centrally mediated sharp pain mechanism.
Figure 5. Comparative Heatmap of Sharp Pain Descriptors (p values). The figure compares statistical associations among sharp pain descriptors in vulvar dermatosis (left) and vulvodynia (right). Color intensity is inversely proportional to p-value. Dermatosis shows partial sticking dominance, whereas vulvodynia demonstrates diffuse, non-hierarchical associations.
3.4. Sensory Phenotyping
To further delineate the neurophysiological mechanisms underlying chronic vulvar discomfort, patients were classified into four sensory phenotypes according to the dominant qualitative descriptors of pain:
1) C-fiber dominant phenotype: burning, stinging, or itching sensations.
2) A-delta dominant phenotype: sharp, stabbing, or knife-like sensations.
3) Mixed profile: descriptors reflecting both C and A-delta input.
4) Non-specific or minimal input: no clear descriptor dominance.
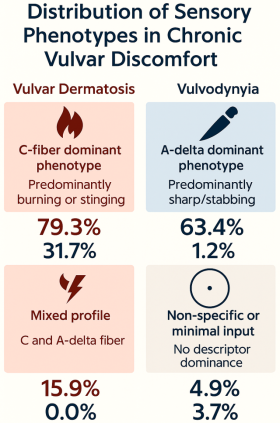
Table 7 summarizes the distribution of phenotypes across diagnostic groups. C-fiber–dominant pain was the prevailing pattern in vulvar dermatosis (79.3%), reflecting superficial nociceptor activation associated with inflammation or irritation. In contrast, vulvodynia was characterized primarily by A-delta–dominant pain (63.4%), indicating preferential involvement of fast-conducting nociceptive pathways and potential neuropathic sensitization. Mixed phenotypes were observed exclusively in dermatosis (15.9%), while non-specific or minimal profiles were rare in both groups.
Table 7. Distribution of Sensory Phenotype in Women with Chronic Vulvar Pain.
Sensory Phenotype | Vulvar Dermatosis (N=82) | Vulvodynia (N=82) |
Predominantly burning/stinging (C-fiber) | 65 (79.3%) | 26 (31.7%) |
Predominantly sharp/stabbing (A-delta) | 1 (1.2%) | 52 (63.4%) |
Mixed profile (C and A-delta) | 13 (15.9%) | 0 (0.0%) |
Non-specific or minimal sensory input | 3 (3.7%) | 4 (4.9%) |
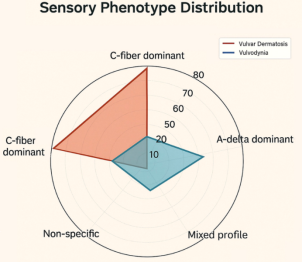
Figure 6. Sensory Phenotype Distribution. Radar chart illustrating the predominance of C-fiber-mediated burning/stinging pain was predominant in dermatosis, while A-delta-mediated sharp/stabbing pain was most frequent in vulvodynia. Mixed phenotypes are exclusive to dermatosis; non-specific input remains low in both groups.
Figures 6 and 7 illustrate these distributions. The radar chart highlights a clear predominance of C-fiber–mediated pain in dermatosis versus A-delta–mediated pain in vulvodynia, while mixed and minimal phenotypes were limited. These patterns support the concept of distinct sensory subtypes in chronic vulvar pain, reflecting different neurophysiological pathways and potentially informing differential diagnosis and mechanism-based treatment.
Figure 7. Distribution of Sensory Phenotypes in Chronic Vulvar Discomfort. C–fiber–mediated burning/stinging pain was predominant in dermatosis, while A–delta–mediated sharp/stabbing pain was most frequent in vulvodynia. Mixed profiles and minimal input were infrequent.
4. Discussion
This study provides a structured sensory profiling of vulvar pain in women with chronic vulvar discomfort, delineating distinct pain qualities in vulvar dermatoses and vulvodynia. By applying comparative analysis of sharp and dull pain descriptors, we identified internal sensory hierarchies within and between diagnostic categories, offering new insight into the underlying neurophysiological mechanisms.
In vulvar dermatoses, dull pain was nearly universal and predominantly characterized by itching (96.2%) and stinging (77.4%), which occurred more frequently than burning, aching, or soreness. These findings are consistent with inflammatory conditions such as lichen sclerosus and lichen planus and reflect pruriceptive C-fiber activation in the superficial dermis. This pattern supports the view that inflammatory input from unmyelinated fibers underlies symptom generation in dermatoses, likely mediated by immune activity, fibrosis, and tissue remodeling
| [16] | Schmelz M. Itch and pain. Neurosci Biobehav Rev. 2010; 34: 171–176. PMID: 19146873; https://doi.org/10.1016/j.neubiorev.2008.12.004 |
| [19] | Scholz J, Finnerup NB, Attal N, Aziz Q, Baron R, Bennett MI, et al. Classification of pain: a pragmatic proposal for ICD-11. Pain. 2019; 160(1): 53-59. PMID: 30586071; https://doi.org/10.1097/j.pain.0000000000001365 |
| [22] | Lountzi A, Abhyankar P, Durand H. A scoping review of vulvodynia research: diagnosis, treatment, and care experiences. Womens Health (Lond). 2025; 17: 17455057251345946. PMID: 40525542; https://doi.org/10.1177/17455057251345946 |
| [27] | Serra J, Bostock H, Sola R, Aleu J, Garcia E, et al. Microneurographic identification of spontaneous activity in C-nociceptors in neuropathic pain states in humans and rats. Pain. 2012; 153(1): 42-55. PMID: 21993185; https://doi.org/10.1016/j.pain.2011.08.015 |
| [33] | Pukall CF, Strigo IA, Binik YM, Amsel R, Khalife S, Bushnell MC. Neural correlates of painful genital touch in women with vulvar vestibulitis syndrome. Pain. 2005; 115(1-2): 118-127. PMID: 15836975; https://doi.org/10.1016/j.pain.2005.02.020 |
[16, 19, 22, 27, 33]
.
By contrast, vulvodynia demonstrated a more neuropathic sensory profile. Stinging emerged as the most consistent and statistically dominant descriptor, pointing to persistent A-delta fiber activation. This differs from earlier reports that described vulvodynia predominantly as a burning pain syndrome
| [3] | Arnold LD, Bachmann GA, Rosen R, Kelly S, Rhoads GG. Vulvodynia: characteristics and associations with comorbidities and quality of life. Obstet Gynecol. 2006; 107: 617–624. PMID 16507933; https://doi.org/10.1097/01.AOG.0000199951.26822.27 |
| [12] | Bornstein J, Goldstein AT, Stockdale CK, Bergeron S, Pukall C, Zolnoun D, Coady D. Descriptors of vulvodynia: a multisocietal definition and consensus statement. J Low Genit Tract Dis. 2019; 23: 161-163. PMID: 30768446; https://doi.org/10.1097/LGT.0000000000000461 |
| [24] | Harni V, Babic D, Hadzavdic S, Barisic D. Diagnostic accuracy of the Vulvoscopy Index for detection of vulvar dermatosis (DATRIV study, Part 1). J Gynecol Obstet. 2022; 10(1): 39-47. https://doi.org/10.11648/j.jgo.20221001.16 |
| [28] | Dukefoss TT, Kleggetveit IP, Helas T, Jørum E. Pain and small-fiber affection in hereditary neuropathy with liability to pressure palsies (HNPP). Scand J Pain. 2020; 20(1): 61-68. https://doi.org/10.1515/sjpain-2019-0090 |
[3, 12, 24, 28]
. The predominance of stinging suggests a more specific neurophysiological marker of vulvodynia than previously recognized, possibly indicating peripheral sensitization in the absence of visible histological changes. Aching, in contrast, had low discriminative value, reinforcing its interpretation as a nonspecific secondary descriptor. The coexistence of burning, stinging, and mechanical allodynia aligns with central sensitization and abnormal somatosensory processing previously documented in vulvodynia
| [23] | Bornstein S, Bornstein J. [THE NEW CONSENSUS TERMINOLOGY OF CHRONICVULVAR PAIN AND VULVODYNIA]. Harefuah. 2019; 158(12): 812-816. Hebrew. PMID: 31823537. |
| [25] | Harni V, Babic D, Hadzavdic S, Barisic D. Clinical value of the N-S-P scheme for detection of vulvar dermatosis (DATRIV study, Part 2). J Gynecol Obstet. 2022; 10(3): 159-166. https://doi.org/10.11648/j.jgo.20221003.11 |
| [29] | Garcia-Larrea L, Peyron R. Pain matrices and neuropathic pain matrices: a review. Pain. 2013; 154 Suppl 1: S29–43. PMID: 24021862; https://doi.org/10.1016/j.pain.2013.09.001 |
| [35] | Haefner HK, Collins ME, Davis GD, Edwards L, Foster DC, et al. The vulvodynia guideline. J Low Genit Tract Dis. 2005; 9(1): 40-51. PMID: 15870521; https://doi.org/10.1097/00128360-200501000-00009 |
[23, 25, 29, 35]
.
Sharp pain descriptors—including knife-like, stabbing, and paper-cut sensations—were significantly more common in vulvodynia, suggesting a direct link to A-delta fiber hyperexcitability. These associations may be mediated by increased density of free nerve endings, changes in epithelial innervation, or loss of nociceptor inhibition
| [12] | Bornstein J, Goldstein AT, Stockdale CK, Bergeron S, Pukall C, Zolnoun D, Coady D. Descriptors of vulvodynia: a multisocietal definition and consensus statement. J Low Genit Tract Dis. 2019; 23: 161-163. PMID: 30768446; https://doi.org/10.1097/LGT.0000000000000461 |
| [20] | Rubal L, Pereira A, Calles Sastre L, Perez Cejuela BA, Herrero Gamiz S, et al. Managing vulvodynia with central sensitization: challenges and strategies. J Clin Med. 2023; 12(11): 3851. PMID: 37298046; https://doi.org/10.3390/jcm12113851 |
| [30] | Goldstein AT, Klingman D, Christopher K, Johnson C, Marinoff SC. Surgical treatment of vulvar vestibulitis syndrome: outcome assessment derived from a postoperative questionnaire. J Sex Med. 2006; 5: 923-931. PMID: 16942537; https://doi.org/10.1111/j.1743-6109.2006.00303.x |
[12, 20, 30]
.
When interpreted through the nociceptive- neuropathic-dysfunctional pain model, the findings suggest:
1) Nociceptive pain (aching, soreness) predominates in dermatoses.
2) Neuropathic features (stinging, stabbing) are central to vulvodynia.
3) Dysfunctional or centrally mediated pain may be reflected in disproportionate descriptors such as paper-cut-like pain.
These descriptors correspond to specific fiber types: stinging and stabbing (A-delta fibers), burning and aching (C fibers), and itching (C-fiber pruriceptors and non-histaminergic pathways)
| [13] | Treede RD, Mayer RA, Raja N, Campbell N. Peripheral and central mechanisms of cutaneous hyperalgesia. Prog Neurobiol. 1992; 38(4): 397-421. PMID: 1574584; https://doi.org/10.1016/0301-0082(92)90027-C |
| [17] | Ikoma A, Steinhoff M, Ständer S, Yosipovitch G. The neurobiology of itch. Nat Rev Neurosci. 2006; 7: 535-547. PMID: 16791143; https://doi.org/10.1038/nrn1950 |
| [21] | Falsetta ML. Editorial: Vulvodynia and beyond: innate immune sensing, microbes, inflammation, and chronic pain. Front Cell Infect Microbiol. 2023; 13: 1338659. PMID: 38145051; https://doi.org/10.3389/fcimb.2023.1338659 |
| [31] | Pukall CF, Goldstein AT, Bergeron S, Foster D, Stein A, et al. Vulvodynia: definition, prevalence, impact, and pathophysiological factors. J Sex Med. 2016; 13(3): 291-304. PMID: 26944961; https://doi.org/10.1016/j.jsxm.2015.12.021 |
[13, 17, 21, 31]
. The overlap of multiple descriptors in individual patients indicates convergent input from diverse fiber types and supports the role of altered nociceptive integration at spinal or supraspinal levels.
From a clinical perspective, sensory profiling adds diagnostic value. A stinging-dominant profile without visible pathology suggests vulvodynia, while an itching-dominant profile with inflammation points to a dermatosis.
4.1. Therapeutic Implications
This distinction may guide therapy. In dermatoses with pruritic C-fiber activation, anti-inflammatory and immunomodulatory approaches (corticosteroids, calcineurin inhibitors, antihistamines) remain central
. In vulvodynia with predominant A-delta activation, neuromodulatory strategies (gabapentin, tricyclic antidepressants, pregabalin, duloxetine, topical lidocaine) are more relevant
. Adjunctive measures such as pelvic floor physical therapy, cognitive behavioral therapy, and, in refractory cases, botulinum toxin have been proposed
| [26] | Yosipovitch G, Greaves MW, Schmelz M. Itch. Lancet. 2003; 361(9358): 690-694. PMID: 12606187; https://doi.org/10.1016/S0140-6736(03)12570-6 |
| [31] | Pukall CF, Goldstein AT, Bergeron S, Foster D, Stein A, et al. Vulvodynia: definition, prevalence, impact, and pathophysiological factors. J Sex Med. 2016; 13(3): 291-304. PMID: 26944961; https://doi.org/10.1016/j.jsxm.2015.12.021 |
| [34] | Engman M, Lindehammar H, Wijma B. Surface electromyography diagnostics in women with or without vulvar vestibulitis and in asymptomatic women. J Psychosom Obstet Gynaecol. 2004; 25(3-4): 281-294. PMID: 15715027; https://doi.org/10.1080/01674820400017921 |
[26, 31, 34]
. Interventional techniques, including laser or radiofrequency neuromodulation, remain investigational
.
Thus, treatment should align with sensory phenotype:
1) C-fiber–driven pruritic dermatoses → anti-inflammatory and immunomodulatory therapy.
2) A-delta–driven neuropathic vulvodynia → neuromodulatory and central sensitization-targeted therapy.
Mixed or minimal-input profiles were rare, suggesting that most patients express a clear nociceptive pathway preference. This supports a mechanism-based classification system that goes beyond simple symptom labeling.
An additional consideration is whether vulvodynia and vulvar dermatoses always represent distinct nosological entities, or in some women, stages of a histopathological continuum. Vulvodynia is more often diagnosed in younger women, whereas dermatoses such as lichen sclerosus occur later in life
. Our findings raise the hypothesis that persistent A-delta activation in untreated vulvodynia may induce microenvironmental changes in epithelial and stromal compartments that predispose to inflammatory dermatoses. Although mixed sensory phenotypes were infrequent, their presence could indicate transitional states. Patients reporting both stinging and itching at clinically significant levels may constitute a subgroup at higher risk for progression. This raises clinically important questions: Can sensory profiling predict histopathological transitions? And if so, could effective early treatment of vulvodynia prevent later development of dermatoses? Demonstrating such a preventive role would represent a major contribution to the pathology of the vulva.
4.2. Limitations and Future Directions
Several limitations should be acknowledged. This was a single-center study conducted in Croatia, which may limit generalizability due to cultural or geographic influences on pain reporting. Multicenter studies are needed to confirm sensory profiles across diverse populations
| [2] | Reed BD, Harlow SD, Sen A, Legocki LJ, Edwards RM, Arato N, Haefner HK. Prevalence and demographic characteristics of vulvodynia in a population-based sample. Am J Obstet Gynecol. 2012; 206: 170. e1–9. PMID 21963307; https://doi.org/10.1016/j.ajog.2011.08.021 |
| [7] | Bohm-Starke N, Ramsay KW, Lytsy P, Nordgren B, Sjöberg I, Moberg K, Flink I. Treatment of provoked vulvodynia: a systematic review. J Sex Med. 2022; 19(5): 789-808. PMID: 35331660; https://doi.org/10.1016/j.jsxm.2022.02.008 |
[2, 7]
. Another limitation is the reliance on self-reported descriptors, which introduces subjectivity; objective validation through quantitative sensory testing, microneurography, or functional neuroimaging is necessary to link descriptors more reliabily to fiber activation
| [14] | Campbell JN, Meyer RA. Mechanisms of neuropathic pain. Neuron. 2006; 52: 77–92. PMID: 17015228; https://doi.org/10.1016/j.neuron.2006.09.021 |
| [20] | Rubal L, Pereira A, Calles Sastre L, Perez Cejuela BA, Herrero Gamiz S, et al. Managing vulvodynia with central sensitization: challenges and strategies. J Clin Med. 2023; 12(11): 3851. PMID: 37298046; https://doi.org/10.3390/jcm12113851 |
| [21] | Falsetta ML. Editorial: Vulvodynia and beyond: innate immune sensing, microbes, inflammation, and chronic pain. Front Cell Infect Microbiol. 2023; 13: 1338659. PMID: 38145051; https://doi.org/10.3389/fcimb.2023.1338659 |
[14, 20, 21]
.
The cross-sectional design precludes conclusions about temporal progression. Prospective longitudinal studies integrating repeated sensory mapping with histopathology and molecular profiling are essential to determine whether mixed phenotypes represent transitional states along a continuum from vulvodynia to dermatoses
| [8] | Dworkin RH, Turk DC, Farrar JT, Haythornthwaite JA, Jensen MP, Katz NP, et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain. 2005; 113: 9–19. PMID 15621359; https://doi.org/10.1016/j.pain.2004.09.012 |
| [9] | Baron R, Binder A, Wasner G. Neuropathic pain: diagnosis, pathophysiological mechanisms, and treatment. Lancet Neurol. 2010; 9: 807–819. PMID 20650402; https://doi.org/10.1016/S1474-4422(10)70143-5 |
| [33] | Pukall CF, Strigo IA, Binik YM, Amsel R, Khalife S, Bushnell MC. Neural correlates of painful genital touch in women with vulvar vestibulitis syndrome. Pain. 2005; 115(1-2): 118-127. PMID: 15836975; https://doi.org/10.1016/j.pain.2005.02.020 |
[8, 9, 33]
. Statistical approaches also warrant refinement: while chi-squared testing and heatmaps provided useful contrasts, effect size measures (e.g., odds ratios) and multivariate models adjusting for confounders such as age, hormonal status, and comorbidities would enhance interpretability.
Another important consideration is that the mapping of descriptors to A-delta or C-fiber input was based on prior research rather than direct validation. Future work should combine psychophysical, histological, and molecular methods to substantiate these associations
| [12] | Bornstein J, Goldstein AT, Stockdale CK, Bergeron S, Pukall C, Zolnoun D, Coady D. Descriptors of vulvodynia: a multisocietal definition and consensus statement. J Low Genit Tract Dis. 2019; 23: 161-163. PMID: 30768446; https://doi.org/10.1097/LGT.0000000000000461 |
| [13] | Treede RD, Mayer RA, Raja N, Campbell N. Peripheral and central mechanisms of cutaneous hyperalgesia. Prog Neurobiol. 1992; 38(4): 397-421. PMID: 1574584; https://doi.org/10.1016/0301-0082(92)90027-C |
| [20] | Rubal L, Pereira A, Calles Sastre L, Perez Cejuela BA, Herrero Gamiz S, et al. Managing vulvodynia with central sensitization: challenges and strategies. J Clin Med. 2023; 12(11): 3851. PMID: 37298046; https://doi.org/10.3390/jcm12113851 |
[12, 13, 20]
. The control group also presents limitations: asymptomatic patients were recruited from women scheduled for elective vulvar procedures, which may introduce selection bias. Community-based controls are needed to better capture normative variability in vulvar sensitivity and mucocutaneous architecture
| [1] | Harlow BL, Stewart EG. A population-based assessment of chronic unexplained vulvar pain: have we underestimated the prevalence of vulvodynia? J Am Med Womens Assoc. 2003; 58(2): 82–88. PMID 12744420 |
| [10] | Backonja MM, Krause SJ. Neuropathic pain questionnaire – short form. Clin J Pain. 2003; 19(5): 315-316. PMID: 12966257; https://doi.org/10.1097/00002508-200309000-00005 |
[1, 10]
.
Finally, therapeutic implications should not be reduced to a binary pharmacological framework. In practice, multimodal strategies—including physical therapy, psychosexual counseling, and management of comorbidities—are often necessary. Randomized controlled trials stratified by sensory phenotype are warranted to determine whether mechanism-based therapy improves outcomes
| [29] | Garcia-Larrea L, Peyron R. Pain matrices and neuropathic pain matrices: a review. Pain. 2013; 154 Suppl 1: S29–43. PMID: 24021862; https://doi.org/10.1016/j.pain.2013.09.001 |
| [36] | Stockdale CK, Lawson HW. 2013 Vulvodynia Guideline update. J Low Genit Tract Dis. 2014 Apr; 18(2): 93-100. https://doi.org/10.1097/LGT.0000000000000021 |
| [37] | Borsook D, Moulton EA, Beccera L. Neuroimaging revolutionizes therapeutic approaches to chronic pain. Mol Pain. 2007; 3: 25. https://doi.org/10.1186/1744-8069-3-25 |
| [38] | Reed BD, Haefner HK, Harlow SD, Gorenflo DW, Sen A. Reliability and validity of self-reported symptoms for predicting vulvodynia. Obstet Gynecol. 2006; 108(4): 906-913. PMID: 17012453; https://doi.org/10.1097/01.AOG.0000237102.70485.5d |
| [39] | Ferraz SD, Rodrigues Candido AC, Rodrigues Uggioni ML, Colonetti T, Santina Dagostin V, Rosa MI. Assessment of anxiety, depression and somatization in women with vulvodynia: a systematic review and meta-analysis. J Affect Disord. 2024; 344: 122-131 |
| [40] | Gerhardt A, Feisst M, Strowitzki T, Zivanovic O, Weinschenk S. Vulvodynia and Chronic Vulvar Pain: Influencing Factors and Long-Term Success After Therapeutic Local Anesthesia (TLA). Pain Ther. 2025; https://doi.org/10.1007/s40122-025-00725-7 |
| [41] | Rains A, Bajzak K, Miller ME, Swab M, Logan GS, Jackman VA, Gustafson DL. Multimodal and Interdisciplinary Interventions. |
[29, 36-41]
.
5. Conclusion
This study provides a systematic sensory profiling of vulvar pain in chronic vulvar discomfort, distinguishing between C-fiber–mediated pruritic dermatoses and A-delta–driven neuropathic vulvodynia. Itching and burning predominated in dermatoses, reflecting inflammatory pruriceptive mechanisms, whereas stinging and sharp pain descriptors were characteristic of vulvodynia, indicating A-delta fiber hyperexcitability. These findings suggest that specific pain qualities can serve as clinical markers of underlying neurophysiological pathways.
The identification of internal sensory hierarchies highlights the diagnostic value of detailed pain assessment. A stinging-dominant profile without visible pathology may indicate vulvodynia, while an itching-dominant profile with inflammation suggests dermatosis. Such stratification supports a mechanism-based framework for diagnosis and treatment selection.
The recognition of mixed sensory phenotypes, though rare, raises the possibility of transitional states between vulvodynia and dermatoses, pointing to a potential histopathological continuum. If confirmed in prospective studies, this would imply that early and effective treatment of vulvodynia could reduce the risk of later inflammatory dermatoses.
These findings build on earlier results of the DATRIV study, which validated the diagnostic accuracy of three-ring vulvoscopy
| [32] | Bohm-Starke N, Hilliges M, Brodda-Jansen G, Rylander E, Torebjork HE. Psychophysical evidence of nociceptor sensitization in vulvar vestibular syndrome. Pain. 2001; 94(2): 177-183. PMID: 11690731; https://doi.org/10.1016/S0304-3959(01)00352-9 |
[32]
, demonstrated the histopathological correlates of chronic pain descriptors
| [33] | Pukall CF, Strigo IA, Binik YM, Amsel R, Khalife S, Bushnell MC. Neural correlates of painful genital touch in women with vulvar vestibulitis syndrome. Pain. 2005; 115(1-2): 118-127. PMID: 15836975; https://doi.org/10.1016/j.pain.2005.02.020 |
[33]
, and described comorbidity clusters and autonomic dysfunction in CVD
. Together with pain mapping, sensory descriptors provide a complementary dimension to the clinical evaluation of chronic vulvar discomfort.
Overall, sensory profiling emerges as a clinically meaningful tool that may enhance diagnostic accuracy, guide personalized therapy, and generate new hypotheses about neuroimmune interactions in vulvar pain. Future longitudinal and mechanistic studies are warranted to test whether sensory descriptors can predict disease evolution and to determine their role in preventive strategies for vulvar pathology.
Abbreviations
DATRIV | Diagnostic Accuracy of Three Rings Vulvoscopy |
CVD | Chronic Vulvar Discomfort |
ISSVD | The International Society for the Study of Vulvovaginal Disease |
TRIV | Three Rings Vulvoscopy |
Author Contributions
Vesna Harni: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Project administration, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing
Damir Babic: Conceptualization, Investigation, Methodology, Supervision, Validation
Suzana Ljubojevic Hadzavdic: Conceptualization, Formal Analysis, Funding acquisition, Methodology, Supervision, Validation
Dubravko Barisic: Conceptualization, Methodology, Supervision
Magdalena Karadza: Conceptualization, Formal Analysis, Investigation, Methodology, Resources, Visualization
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Harlow BL, Stewart EG. A population-based assessment of chronic unexplained vulvar pain: have we underestimated the prevalence of vulvodynia? J Am Med Womens Assoc. 2003; 58(2): 82–88. PMID 12744420
|
| [2] |
Reed BD, Harlow SD, Sen A, Legocki LJ, Edwards RM, Arato N, Haefner HK. Prevalence and demographic characteristics of vulvodynia in a population-based sample. Am J Obstet Gynecol. 2012; 206: 170. e1–9. PMID 21963307;
https://doi.org/10.1016/j.ajog.2011.08.021
|
| [3] |
Arnold LD, Bachmann GA, Rosen R, Kelly S, Rhoads GG. Vulvodynia: characteristics and associations with comorbidities and quality of life. Obstet Gynecol. 2006; 107: 617–624. PMID 16507933;
https://doi.org/10.1097/01.AOG.0000199951.26822.27
|
| [4] |
Goldstein AT, Marinoff SC, Christopher K, Srodon M. Prevalence of vulvar lichen sclerosus in a general gynecology practice. J Reprod Med. 2005; 50 (7): 477–480. PMID 16130842
|
| [5] |
Powell J, Wojnarowska F. Lichen sclerosus. Lancet. 1999; 353: 1777–1783. PMID: 10348006;
https://doi.org/10.1016/S0140-6736(98)08228-2
|
| [6] |
Bornstein J, et al. 2015 ISSVD, ISSWSH and IPPS consensus terminology and classification of persistent vulvar pain and vulvodynia. J Low Genit Tract Dis. 2016; 20: 126–130. PMID 27008217;
https://doi.org/10.1097/LGT.0000000000000190
|
| [7] |
Bohm-Starke N, Ramsay KW, Lytsy P, Nordgren B, Sjöberg I, Moberg K, Flink I. Treatment of provoked vulvodynia: a systematic review. J Sex Med. 2022; 19(5): 789-808. PMID: 35331660;
https://doi.org/10.1016/j.jsxm.2022.02.008
|
| [8] |
Dworkin RH, Turk DC, Farrar JT, Haythornthwaite JA, Jensen MP, Katz NP, et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain. 2005; 113: 9–19. PMID 15621359;
https://doi.org/10.1016/j.pain.2004.09.012
|
| [9] |
Baron R, Binder A, Wasner G. Neuropathic pain: diagnosis, pathophysiological mechanisms, and treatment. Lancet Neurol. 2010; 9: 807–819. PMID 20650402;
https://doi.org/10.1016/S1474-4422(10)70143-5
|
| [10] |
Backonja MM, Krause SJ. Neuropathic pain questionnaire – short form. Clin J Pain. 2003; 19(5): 315-316. PMID: 12966257;
https://doi.org/10.1097/00002508-200309000-00005
|
| [11] |
ISSVD Vulvodynia Pattern Questionnaire. Available at: Clinical Protocols: ISSVD
|
| [12] |
Bornstein J, Goldstein AT, Stockdale CK, Bergeron S, Pukall C, Zolnoun D, Coady D. Descriptors of vulvodynia: a multisocietal definition and consensus statement. J Low Genit Tract Dis. 2019; 23: 161-163. PMID: 30768446;
https://doi.org/10.1097/LGT.0000000000000461
|
| [13] |
Treede RD, Mayer RA, Raja N, Campbell N. Peripheral and central mechanisms of cutaneous hyperalgesia. Prog Neurobiol. 1992; 38(4): 397-421. PMID: 1574584;
https://doi.org/10.1016/0301-0082(92)90027-C
|
| [14] |
Campbell JN, Meyer RA. Mechanisms of neuropathic pain. Neuron. 2006; 52: 77–92. PMID: 17015228;
https://doi.org/10.1016/j.neuron.2006.09.021
|
| [15] |
Fields HL. Pain modulation: expectation, opioid analgesia and virtual pain. Prog Brain Res. 2000; 129: 245–253. PMID 10737063;
https://doi.org/10.1016/S0079-6123(08)62143-3
|
| [16] |
Schmelz M. Itch and pain. Neurosci Biobehav Rev. 2010; 34: 171–176. PMID: 19146873;
https://doi.org/10.1016/j.neubiorev.2008.12.004
|
| [17] |
Ikoma A, Steinhoff M, Ständer S, Yosipovitch G. The neurobiology of itch. Nat Rev Neurosci. 2006; 7: 535-547. PMID: 16791143;
https://doi.org/10.1038/nrn1950
|
| [18] |
Woolf CJ. Central sensitization: implications for the diagnosis and treatment of pain. Pain. 2011; 152(3 Suppl): S2-S15. PMID: 20961685;
https://doi.org/10.1016/j.pain.2010.09.030
|
| [19] |
Scholz J, Finnerup NB, Attal N, Aziz Q, Baron R, Bennett MI, et al. Classification of pain: a pragmatic proposal for ICD-11. Pain. 2019; 160(1): 53-59. PMID: 30586071;
https://doi.org/10.1097/j.pain.0000000000001365
|
| [20] |
Rubal L, Pereira A, Calles Sastre L, Perez Cejuela BA, Herrero Gamiz S, et al. Managing vulvodynia with central sensitization: challenges and strategies. J Clin Med. 2023; 12(11): 3851. PMID: 37298046;
https://doi.org/10.3390/jcm12113851
|
| [21] |
Falsetta ML. Editorial: Vulvodynia and beyond: innate immune sensing, microbes, inflammation, and chronic pain. Front Cell Infect Microbiol. 2023; 13: 1338659. PMID: 38145051;
https://doi.org/10.3389/fcimb.2023.1338659
|
| [22] |
Lountzi A, Abhyankar P, Durand H. A scoping review of vulvodynia research: diagnosis, treatment, and care experiences. Womens Health (Lond). 2025; 17: 17455057251345946. PMID: 40525542;
https://doi.org/10.1177/17455057251345946
|
| [23] |
Bornstein S, Bornstein J. [THE NEW CONSENSUS TERMINOLOGY OF CHRONICVULVAR PAIN AND VULVODYNIA]. Harefuah. 2019; 158(12): 812-816. Hebrew. PMID: 31823537.
|
| [24] |
Harni V, Babic D, Hadzavdic S, Barisic D. Diagnostic accuracy of the Vulvoscopy Index for detection of vulvar dermatosis (DATRIV study, Part 1). J Gynecol Obstet. 2022; 10(1): 39-47.
https://doi.org/10.11648/j.jgo.20221001.16
|
| [25] |
Harni V, Babic D, Hadzavdic S, Barisic D. Clinical value of the N-S-P scheme for detection of vulvar dermatosis (DATRIV study, Part 2). J Gynecol Obstet. 2022; 10(3): 159-166.
https://doi.org/10.11648/j.jgo.20221003.11
|
| [26] |
Yosipovitch G, Greaves MW, Schmelz M. Itch. Lancet. 2003; 361(9358): 690-694. PMID: 12606187;
https://doi.org/10.1016/S0140-6736(03)12570-6
|
| [27] |
Serra J, Bostock H, Sola R, Aleu J, Garcia E, et al. Microneurographic identification of spontaneous activity in C-nociceptors in neuropathic pain states in humans and rats. Pain. 2012; 153(1): 42-55. PMID: 21993185;
https://doi.org/10.1016/j.pain.2011.08.015
|
| [28] |
Dukefoss TT, Kleggetveit IP, Helas T, Jørum E. Pain and small-fiber affection in hereditary neuropathy with liability to pressure palsies (HNPP). Scand J Pain. 2020; 20(1): 61-68.
https://doi.org/10.1515/sjpain-2019-0090
|
| [29] |
Garcia-Larrea L, Peyron R. Pain matrices and neuropathic pain matrices: a review. Pain. 2013; 154 Suppl 1: S29–43. PMID: 24021862;
https://doi.org/10.1016/j.pain.2013.09.001
|
| [30] |
Goldstein AT, Klingman D, Christopher K, Johnson C, Marinoff SC. Surgical treatment of vulvar vestibulitis syndrome: outcome assessment derived from a postoperative questionnaire. J Sex Med. 2006; 5: 923-931. PMID: 16942537;
https://doi.org/10.1111/j.1743-6109.2006.00303.x
|
| [31] |
Pukall CF, Goldstein AT, Bergeron S, Foster D, Stein A, et al. Vulvodynia: definition, prevalence, impact, and pathophysiological factors. J Sex Med. 2016; 13(3): 291-304. PMID: 26944961;
https://doi.org/10.1016/j.jsxm.2015.12.021
|
| [32] |
Bohm-Starke N, Hilliges M, Brodda-Jansen G, Rylander E, Torebjork HE. Psychophysical evidence of nociceptor sensitization in vulvar vestibular syndrome. Pain. 2001; 94(2): 177-183. PMID: 11690731;
https://doi.org/10.1016/S0304-3959(01)00352-9
|
| [33] |
Pukall CF, Strigo IA, Binik YM, Amsel R, Khalife S, Bushnell MC. Neural correlates of painful genital touch in women with vulvar vestibulitis syndrome. Pain. 2005; 115(1-2): 118-127. PMID: 15836975;
https://doi.org/10.1016/j.pain.2005.02.020
|
| [34] |
Engman M, Lindehammar H, Wijma B. Surface electromyography diagnostics in women with or without vulvar vestibulitis and in asymptomatic women. J Psychosom Obstet Gynaecol. 2004; 25(3-4): 281-294. PMID: 15715027;
https://doi.org/10.1080/01674820400017921
|
| [35] |
Haefner HK, Collins ME, Davis GD, Edwards L, Foster DC, et al. The vulvodynia guideline. J Low Genit Tract Dis. 2005; 9(1): 40-51. PMID: 15870521;
https://doi.org/10.1097/00128360-200501000-00009
|
| [36] |
Stockdale CK, Lawson HW. 2013 Vulvodynia Guideline update. J Low Genit Tract Dis. 2014 Apr; 18(2): 93-100.
https://doi.org/10.1097/LGT.0000000000000021
|
| [37] |
Borsook D, Moulton EA, Beccera L. Neuroimaging revolutionizes therapeutic approaches to chronic pain. Mol Pain. 2007; 3: 25.
https://doi.org/10.1186/1744-8069-3-25
|
| [38] |
Reed BD, Haefner HK, Harlow SD, Gorenflo DW, Sen A. Reliability and validity of self-reported symptoms for predicting vulvodynia. Obstet Gynecol. 2006; 108(4): 906-913. PMID: 17012453;
https://doi.org/10.1097/01.AOG.0000237102.70485.5d
|
| [39] |
Ferraz SD, Rodrigues Candido AC, Rodrigues Uggioni ML, Colonetti T, Santina Dagostin V, Rosa MI. Assessment of anxiety, depression and somatization in women with vulvodynia: a systematic review and meta-analysis. J Affect Disord. 2024; 344: 122-131
|
| [40] |
Gerhardt A, Feisst M, Strowitzki T, Zivanovic O, Weinschenk S. Vulvodynia and Chronic Vulvar Pain: Influencing Factors and Long-Term Success After Therapeutic Local Anesthesia (TLA). Pain Ther. 2025;
https://doi.org/10.1007/s40122-025-00725-7
|
| [41] |
Rains A, Bajzak K, Miller ME, Swab M, Logan GS, Jackman VA, Gustafson DL. Multimodal and Interdisciplinary Interventions.
|
Cite This Article
-
APA Style
Harni, V., Babic, D., Hadzavdic, S. L., Barisic, D., Karadza, M. (2025). Burning, Stinging, Tenderness: Sensory Profiling of Vulvar Pain in Chronic Discomfort — A DATRIV Study Perspective. Journal of Gynecology and Obstetrics, 13(5), 103-116. https://doi.org/10.11648/j.jgo.20251305.14
 Copy
|
Copy
|
 Download
Download
ACS Style
Harni, V.; Babic, D.; Hadzavdic, S. L.; Barisic, D.; Karadza, M. Burning, Stinging, Tenderness: Sensory Profiling of Vulvar Pain in Chronic Discomfort — A DATRIV Study Perspective. J. Gynecol. Obstet. 2025, 13(5), 103-116. doi: 10.11648/j.jgo.20251305.14
Copy
|
Download
AMA Style
Harni V, Babic D, Hadzavdic SL, Barisic D, Karadza M. Burning, Stinging, Tenderness: Sensory Profiling of Vulvar Pain in Chronic Discomfort — A DATRIV Study Perspective. J Gynecol Obstet. 2025;13(5):103-116. doi: 10.11648/j.jgo.20251305.14
Copy
|
Download
-
@article{10.11648/j.jgo.20251305.14,
author = {Vesna Harni and Damir Babic and Suzana Ljubojevic Hadzavdic and Dubravko Barisic and Magdalena Karadza},
title = {Burning, Stinging, Tenderness: Sensory Profiling of Vulvar Pain in Chronic Discomfort — A DATRIV Study Perspective
},
journal = {Journal of Gynecology and Obstetrics},
volume = {13},
number = {5},
pages = {103-116},
doi = {10.11648/j.jgo.20251305.14},
url = {https://doi.org/10.11648/j.jgo.20251305.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.jgo.20251305.14},
abstract = {Background: Chronic vulvar discomfort (CVD) affects up to 28% of women but remains diagnostically challenging due to overlapping symptoms and limited application of structured sensory profiling. Objective: To delineate qualitative sensory profiles in women with vulvar dermatoses and vulvodynia, identify dominant pain descriptors, and explore internal sensory hierarchies using comparative statistical methods. Methods: A total of 328 women were enrolled in the prospective DATRIV study. All participants underwent structured pain assessment, Three-Rings Vulvoscopy (TRIV), and targeted vulvar biopsy with histopathologic confirmation. Pain descriptors were categorized according to putative neurophysiological mechanisms (C-fiber vs. A-delta fiber input). Statistical analyses included frequency comparisons, co-occurrence matrices, and data visualization through heatmaps and radar plots. Results: Dull pain was nearly universal (>98%). In vulvar dermatoses, itching (96.2%) and stinging (77.4%) predominated, reflecting C-fiber-mediated pruriceptive pathways. In contrast, vulvodynia demonstrated a significantly higher prevalence of sharp pain, particularly stabbing (45.5%) and knife-like sensations (54.5%), indicating A-delta fiber hyperexcitability. Heatmap analysis revealed distinct internal sensory hierarchies: clustering of pruritic descriptors in dermatoses and a more heterogeneous, dispersed pattern in vulvodynia. Conclusion: Women with chronic vulvar discomfort display distinct sensory phenotypes that align with underlying neurophysiological mechanisms. Sensory profiling distinguishes between inflammatory C-fiber–mediated and neuropathic A-delta–mediated patterns, as well as mixed profiles reflecting contributions from both fiber types, and non-specific or minimal input lacking clear descriptor dominance. Notably, a subset of patients with histologically confirmed dermatoses also displayed A-delta–dominant features, suggesting overlapping neuropathic components. These findings indicate that vulvodynia and vulvar dermatoses may represent interconnected conditions along a shared pathophysiological continuum, where untreated or prolonged vulvodynia may evolve toward inflammatory dermatoses. Recognizing these trajectories may enhance diagnostic precision and support personalized, mechanism-based therapeutic strategies.
},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Burning, Stinging, Tenderness: Sensory Profiling of Vulvar Pain in Chronic Discomfort — A DATRIV Study Perspective
AU - Vesna Harni
AU - Damir Babic
AU - Suzana Ljubojevic Hadzavdic
AU - Dubravko Barisic
AU - Magdalena Karadza
Y1 - 2025/10/18
PY - 2025
N1 - https://doi.org/10.11648/j.jgo.20251305.14
DO - 10.11648/j.jgo.20251305.14
T2 - Journal of Gynecology and Obstetrics
JF - Journal of Gynecology and Obstetrics
JO - Journal of Gynecology and Obstetrics
SP - 103
EP - 116
PB - Science Publishing Group
SN - 2376-7820
UR - https://doi.org/10.11648/j.jgo.20251305.14
AB - Background: Chronic vulvar discomfort (CVD) affects up to 28% of women but remains diagnostically challenging due to overlapping symptoms and limited application of structured sensory profiling. Objective: To delineate qualitative sensory profiles in women with vulvar dermatoses and vulvodynia, identify dominant pain descriptors, and explore internal sensory hierarchies using comparative statistical methods. Methods: A total of 328 women were enrolled in the prospective DATRIV study. All participants underwent structured pain assessment, Three-Rings Vulvoscopy (TRIV), and targeted vulvar biopsy with histopathologic confirmation. Pain descriptors were categorized according to putative neurophysiological mechanisms (C-fiber vs. A-delta fiber input). Statistical analyses included frequency comparisons, co-occurrence matrices, and data visualization through heatmaps and radar plots. Results: Dull pain was nearly universal (>98%). In vulvar dermatoses, itching (96.2%) and stinging (77.4%) predominated, reflecting C-fiber-mediated pruriceptive pathways. In contrast, vulvodynia demonstrated a significantly higher prevalence of sharp pain, particularly stabbing (45.5%) and knife-like sensations (54.5%), indicating A-delta fiber hyperexcitability. Heatmap analysis revealed distinct internal sensory hierarchies: clustering of pruritic descriptors in dermatoses and a more heterogeneous, dispersed pattern in vulvodynia. Conclusion: Women with chronic vulvar discomfort display distinct sensory phenotypes that align with underlying neurophysiological mechanisms. Sensory profiling distinguishes between inflammatory C-fiber–mediated and neuropathic A-delta–mediated patterns, as well as mixed profiles reflecting contributions from both fiber types, and non-specific or minimal input lacking clear descriptor dominance. Notably, a subset of patients with histologically confirmed dermatoses also displayed A-delta–dominant features, suggesting overlapping neuropathic components. These findings indicate that vulvodynia and vulvar dermatoses may represent interconnected conditions along a shared pathophysiological continuum, where untreated or prolonged vulvodynia may evolve toward inflammatory dermatoses. Recognizing these trajectories may enhance diagnostic precision and support personalized, mechanism-based therapeutic strategies.
VL - 13
IS - 5
ER -
Copy
|
Download