Background: Intestinal malrotation is a congenital condition caused by incomplete or absent rotation of the intestine around the superior mesenteric artery during embryonic development. It is typically presents in the neonatal period. In adults, it is rare (0.2%) and often asymptomatic, discovered incidentally during exams or surgeries. The clinical context in an adult patient can cause chronic symptoms such as intermittent abdominal pain, dyspepsia, nausea, vomiting and abdominal swelling. Diagnosis is best achieved with an upper gastrointestinal contrast study, while CT scan or MRI may detect it incidentally. Surgical correction (Ladd’s procedure) involves reducing volvulus (if present), removing Ladd's bands, and broadening the mesenteric base. This case is noteworthy due to the limited number of similar reports documented globally. Case Presentation: A 67-year-old woman presented with a 4-month history of weight loss, loss of appetite, and episodes of abdominal pain. An abdominal CT revealed signs of intestinal malrotation, and an MRI confirmed these findings, showing abnormal positioning of intestinal loops and vascular structures. Exploratory laparoscopy was performed, and intraoperative findings confirmed the diagnosis. The entire adhered right colon was released from the sigmoid at the angle of Treitz and was repositioned to the right side of the abdomen with the cecum. The patient recovered well, was discharged on the second postoperative day, and remained asymptomatic during follow-up visits at 8 days, 45 days, 3 months post-surgery and ten years after. Discussion and Conclusion: Identifying intestinal malrotation in adults is challenging because of the broad range and vague nature of the symptoms. Diagnostic delays can result in serious complications and less favorable surgical outcomes. Treatment depends on symptomatology and intraoperative findings. Ladd’s Procedure remains the standard approach, involving repositioning of the intestines and release of abnormal bands. The patient in question underwent successful laparoscopic correction, with complete symptom resolution and no complications during follow-up.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Yin M-D, Hao L-L, Li G, Li Y-T, Xu B-L, Chen X-R. Adult-onset congenital intestinal malrotation: A case report and literature review. Medicine (Baltimore) [Internet]. 2024; 103(8): e37249.
due to incomplete rotation or non-rotation of the intestine on the superior mesenteric artery axis during embryological development
[2]
Yin M-D, Hao L-L, Li G, Li Y-T, Xu B-L, Chen X-R. Adult-onset congenital intestinal malrotation: A case report and literature review. Medicine (Baltimore) [Internet]. 2024; 103(8): e37249.
Araújo URM e. F de, El Tawil II. Má rotação intestinal em adulto, relato de caso e revisão da literatura. ArqBrasCir Dig [Internet]. 2009; 22(4): 240-2.
Elgeyoushy F, Qari AS, Faidh RA. A rare case of congenital intestinal malrotation presented as an intestinal obstruction in an adult. Cureus [Internet]. 2023; 15(12): e49812.
. It most commonly presents during the neonatal period
[5]
Kanazawa T, Kasugai K, Miyata M, Miyashita M, Mizuno M, Nagase F, et al. Midgut malrotation in adulthood. Intern Med. 2000; 39(8): 626-31.
[5]
, in the first months of life, but can sometimes present late, causing difficulty and error in diagnosis
[3]
Araújo URM e. F de, El Tawil II. Má rotação intestinal em adulto, relato de caso e revisão da literatura. ArqBrasCir Dig [Internet]. 2009; 22(4): 240-2.
Applegate KE. Evidence-based diagnosis of malrotation and volvu- lus. Pediatr Radiol. 2009; 39(2): S161-3.
[3, 6]
.
Malrotation occurs in about 1 in 2.500 live births (under 1 year of age), however, as an anatomical entity, it occurs more commonly in 0.2% to 1.0% of the population
[1]
Adams SD, Stanton MP. Malrotation and intestinal atresias. Early Hum Dev [Internet]. 2014; 90(12): 921-5.
. It is known that 64% of cases become clinically evident in the first months of life and 82% within the first year. In contrast, in adults, it is usually asymptomatic and is only detected during investigations, operations or autopsies
[7]
Ray D, Morimoto M. Malrotation of the intestine in adult and colorectal cancer. Indian J Surg [Internet]. 2015; 77(6): 525-31.
. Consequently, in adults, the incidence is 0.2%, with about 15% of all patients with a confirmed diagnosis of intestinal malrotation remaining asymptomatic for life
[3]
Araújo URM e. F de, El Tawil II. Má rotação intestinal em adulto, relato de caso e revisão da literatura. ArqBrasCir Dig [Internet]. 2009; 22(4): 240-2.
Aregawi AB, Geremew TT, Legese AT, Bahru TT. A rare case of adult intestinal malrotation: A case report. Int J Surg Case Rep [Internet]. 2025; 127(110848): 110848.
. In adults, chronic, partial or intermittent volvulus may present with abdominal pain, intermittent vomiting, diarrhea, occult gastrointestinal bleeding, protein-loss enteropathy due to lymphatic obstruction, failure to thrive or malnutrition
[9]
Langer JC. Intestinal rotation abnormalities and midgut volvulus. Surg Clin North Am [Internet]. 2017; 97(1): 147-59.
Abdillahi Mahamoud C, Egueh Nour A, Bouknani N, Benslima N, Rami A. Diagnostic challenges in adult intestinal malrotation: A case report and literature review. Cureus [Internet]. 2024; 16(1): e52281.
The identification of symptoms, diagnosis, and appropriate treatment is frequently postponed due to the rarity of malrotation. This represents a significant risk in cases of intestinal volvulus, as it may cause extensive intestinal injury, resulting in short bowel syndrome or even death
[6]
Applegate KE. Evidence-based diagnosis of malrotation and volvu- lus. Pediatr Radiol. 2009; 39(2): S161-3.
[10]
Abdillahi Mahamoud C, Egueh Nour A, Bouknani N, Benslima N, Rami A. Diagnostic challenges in adult intestinal malrotation: A case report and literature review. Cureus [Internet]. 2024; 16(1): e52281.
Martinez SA, Fligor SC, Tsikis S, Short M, Corcoran KE, Rogers A, et al. IMPOWER: a national patient-generated registry for intestinal malrotation exploring diagnosis, treatment, and surgical outcomes. Orphanet J Rare Dis [Internet]. 2023; 18(1): 113.
The GI swollen series continues to be the gold standard for diagnosing intestinal malrotation and is commonly utilized in pediatric practice
[12]
Birajdar S, Rao SC, Bettenay F. Role of upper gastrointestinal contrast studies for suspected malrotation in neonatal population. J Paediatr Child H. 2017; 53(7): 644-9.
[12]
. The US is also recommended as a screening tool for detecting malrotation with volvulus
[13]
Shimanuki Y, Aihara T, Takano H, Moritani T, Oguma E, Kuroki H, et al. Clockwise whirlpool sign at color Doppler US: an objective and definite sign of midgut volvulus. Radiology [Internet]. 1996; 199(1): 261-4.
In adults, abdominal CT, particularly with intravenous and oral contrast, offers higher diagnostic accuracy. The CT imaging not only reveals the abnormal findings seen on UGI and ultrasound but also overcomes the limitations caused by intestinal gas, providing comprehensive anatomical details of the bowel
[14]
Xiong Z, Shen Y, Morelli JN, Li Z, Hu X, Hu D. CT facilitates improved diagnosis of adult intestinal malrotation: a 7-year retrospective study based on 332 cases. Insights Imaging [Internet]. 2021; 12(1): 58.
Martinez SA, Fligor SC, Tsikis S, Short M, Corcoran KE, Rogers A, et al. IMPOWER: a national patient-generated registry for intestinal malrotation exploring diagnosis, treatment, and surgical outcomes. Orphanet J Rare Dis [Internet]. 2023; 18(1): 113.
, which involves reduction of volvulus, if present, removal of Ladd's bands, and widening of the mesenteric base to prevent volvulus
[15]
Eccleston JL, Su H, Ling A, Heller T, Koh C. Gastrointestinal: Adult presentation of intestinal malrotation: Journal of Gastroenterology and Hepatology. J GastroenterolHepatol [Internet]. 2016; 31(8): 1382-1382.
Thus, we present a case of a 67-year-old female adult, with a history of weight loss and 4-month abdominal pain, diagnosed with poor intestinal inversion with the help of imaging exams, undergoing surgical intervention by laparoscopy to correct the problem. This case is noteworthy due to the limited number of similar reports documented globally.
2. Case Presentation
A 67-year-old Brazilian female presented weight loss for approximately 4 months. In addition, she reported an episode of acute abdominal pain, associated with melena, evolving with other abdominal pain in the left flank after eating. In addition, she lost 10kg in weight associated with loss of appetite.
Abdominal CT scan showed suggestive signs: 1) intestinal malrotation, characterized by inversion of the relationship between the mesenteric vessels; 2) duodenojejunal junction on the right side of the spine; 3) the small intestine on the right side; 4) colon on the left side.
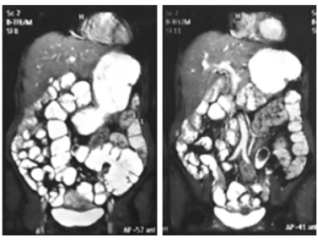
To support the CT scan findings, an MRI was conducted one month later to confirm the presence of intestinal malrotation. The most recent imaging revealed features consistent with malrotation, including the small bowel loops predominantly situated on the right side of abdomen, a distended cecum located in the left pelvic region, and a reversed relationship between the superior mesenteric artery and vein (Figure 1). Additionally, there was an inversion in the positioning of the aorta and inferior vena cava, with the aorta positioned on the right side.
Figure 1. Internal magnetic resonance imaging of the abdomen: the cecum distended and located in the pelvic region on the left, including, an inversion of the relationship between the superior mesenteric artery and the superior mesenteric vein.
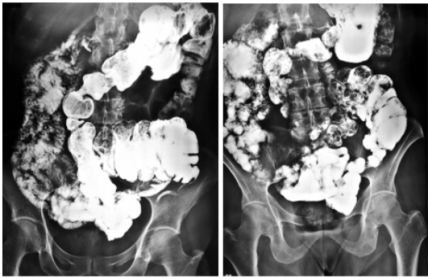
One month later, in addition to the exams already carried out, seeking to associate abdominal pain and weight loss with some findings on imaging, an intestinal transit study via X-ray of the small intestine was requested. It showed signs of intestinal malrotation, characterized by the distribution of abnormal small bowel loops, which were found in the right hemiabdomen, and colonic loops distributed between the midline and left hemiabdomen (figure 2). The descending colon and sigmoid colon are demonstrated in anatomical topography (left side).
Figure 2. Small intestine X-ray: intestinal transit demonstrating complete intestinal inversion: small intestine on the right side and cecum located in the left iliac fossa.
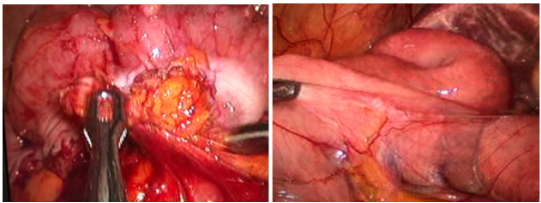
Subsequently, based on the clinical and imaging evidence presented above, the patient was subjected to an exploratory videolaparoscopy. During the procedure, the findings already observed on the abdominal CT, the abdominal MRI and small intestine x-ray were proven. The entire adhered right colon was released from the sigmoid at the angle of Treitz. Therefore, the cecum and right colon were placed on the right side of the abdomen (figure 3). To avoid another future relapse, a preventive appendectomy was performed.
The patient had a satisfactory evolution, being discharged from the hospital on the 2nd postoperative day. She then performed routine outpatient consultations after 8 days, 45 days, 3 months postoperatively and remaining asymptomatic 10 years later.
3. Discussion
Intestinal malrotation is a congenital defect in which the fetal intestines do not completely or at all rotate around the axis of the superior mesenteric artery during fetal development. The embryological phase of the midgut into the abdominal cavity involves rotation and fixation, which can be anomalous at different stages, leading to malrotation of the intestine
[7]
Ray D, Morimoto M. Malrotation of the intestine in adult and colorectal cancer. Indian J Surg [Internet]. 2015; 77(6): 525-31.
. Thus, failure of normal physiologic rotation of the midgut leads to varying degrees of anomaly, including the entire small intestine remaining on the right side of the abdomen, cecum, appendix, and colon on the left, and an absent of Treitz ligament
[17]
Emanuwa OF, Ayantunde AA, Davies TW. Midgut malrotation first presenting as acute bowel obstruction in adulthood: a case report and literature review. World J EmergSurg [Internet]. 2011; 6(1).
The initial presentation of symptomatic intestinal malrotation is rare in adults
[17]
Emanuwa OF, Ayantunde AA, Davies TW. Midgut malrotation first presenting as acute bowel obstruction in adulthood: a case report and literature review. World J EmergSurg [Internet]. 2011; 6(1).
, thus, according to some authors, most cases of intestinal malrotation in adults are asymptomatic
[3]
Araújo URM e. F de, El Tawil II. Má rotação intestinal em adulto, relato de caso e revisão da literatura. ArqBrasCir Dig [Internet]. 2009; 22(4): 240-2.
. Diagnosing malrotation in adults is challenging, as it is seldom considered based on clinical suspicion. Many individuals show no symptoms, and the condition is often identified incidentally during imaging or surgery for unrelated issues later in life
[17]
Emanuwa OF, Ayantunde AA, Davies TW. Midgut malrotation first presenting as acute bowel obstruction in adulthood: a case report and literature review. World J EmergSurg [Internet]. 2011; 6(1).
. As a result, delays in diagnosis are frequent in this population due to the vague and nonspecific nature of their symptoms
[17]
Emanuwa OF, Ayantunde AA, Davies TW. Midgut malrotation first presenting as acute bowel obstruction in adulthood: a case report and literature review. World J EmergSurg [Internet]. 2011; 6(1).
Emanuwa OF, Ayantunde AA, Davies TW. Midgut malrotation first presenting as acute bowel obstruction in adulthood: a case report and literature review. World J EmergSurg [Internet]. 2011; 6(1).
, so recent studies have shown that, in this age group, malrotation can cause chronic symptoms such as intermittent abdominal pain, dyspepsia, nausea, vomiting and abdominal swelling in 80% of cases
[7]
Ray D, Morimoto M. Malrotation of the intestine in adult and colorectal cancer. Indian J Surg [Internet]. 2015; 77(6): 525-31.
Emanuwa OF, Ayantunde AA, Davies TW. Midgut malrotation first presenting as acute bowel obstruction in adulthood: a case report and literature review. World J EmergSurg [Internet]. 2011; 6(1).
. The case of the patient presented here, who complained of weight loss associated with abdominal pain in the right and left iliac fossa, being more intense in the left iliac fossa. These atypical presentations can lead to confusion, leading to misdiagnosis of conditions, such as acute appendicitis, cholecystitis, pancreatitis, perforated peptic ulcer, and left colon diverticulitis
[17]
Emanuwa OF, Ayantunde AA, Davies TW. Midgut malrotation first presenting as acute bowel obstruction in adulthood: a case report and literature review. World J EmergSurg [Internet]. 2011; 6(1).
Alghamdi T, Alghamdi AM, Agafli FH, Mahmoud A. Adult intestinal malrotation with atypical presentation: A case report and diagnostic challenge. Am J Case Rep [Internet]. 2024; 25: e945197.
The preoperative diagnosis of malrotation is preferably performed by abdominal CT scan. Abdominal CT scans done for unrelated reasons can incidentally reveal intestinal malrotation
[14]
Xiong Z, Shen Y, Morelli JN, Li Z, Hu X, Hu D. CT facilitates improved diagnosis of adult intestinal malrotation: a 7-year retrospective study based on 332 cases. Insights Imaging [Internet]. 2021; 12(1): 58.
. Furthermore, diagnostic indicators of midgut malrotation can be identified using plain X-rays, US, MRI, and mesenteric arteriography
[17]
Emanuwa OF, Ayantunde AA, Davies TW. Midgut malrotation first presenting as acute bowel obstruction in adulthood: a case report and literature review. World J EmergSurg [Internet]. 2011; 6(1).
In this way, the difficulty is perceived to reside in the absence of specific physical signs and in a direct method of investigation with which the diagnosis can be confirmed
[19]
Gilbert HW, Armstrong CP, Thompson MH. The presentation of malrotation of the intestine in adults. Ann R Coll Surg Engl. 1990; 72(4): 239-42.
[19]
. The patient in question was treated by the aforementioned exams. Firstly, she underwent a CT scan of the chest and abdomen, then followed by an Entero-magnetic resonance and lastly the small intestine X-ray: intestinal transit.
There is no standardized treatment for intestinal malrotation in adults, as it depends on surgical findings and associated abnormalities
[3]
Araújo URM e. F de, El Tawil II. Má rotação intestinal em adulto, relato de caso e revisão da literatura. ArqBrasCir Dig [Internet]. 2009; 22(4): 240-2.
. Surgery is necessary for symptomatic cases, but management of asymptomatic patients remains debated
[17]
Emanuwa OF, Ayantunde AA, Davies TW. Midgut malrotation first presenting as acute bowel obstruction in adulthood: a case report and literature review. World J EmergSurg [Internet]. 2011; 6(1).
Gilbert HW, Armstrong CP, Thompson MH. The presentation of malrotation of the intestine in adults. Ann R Coll Surg Engl. 1990; 72(4): 239-42.
[17, 19]
. The study by Choi et al, who reviewed 177 patients over a period of 35 years, found that asymptomatic patients had a low risk of intestinal volvulus and therefore advised that routine investigations, screening and elective surgery were not necessary with close follow-up
[17]
Emanuwa OF, Ayantunde AA, Davies TW. Midgut malrotation first presenting as acute bowel obstruction in adulthood: a case report and literature review. World J EmergSurg [Internet]. 2011; 6(1).
. On the other hand, there are others who claim that surgical treatment should be instituted to prevent complications caused by volvulus or internal hernia
[3]
Araújo URM e. F de, El Tawil II. Má rotação intestinal em adulto, relato de caso e revisão da literatura. ArqBrasCir Dig [Internet]. 2009; 22(4): 240-2.
Indeed, intervention with symptomatic patients was first described by William Ladd in 1936 and this remains the mainstay of treatment
[17]
Emanuwa OF, Ayantunde AA, Davies TW. Midgut malrotation first presenting as acute bowel obstruction in adulthood: a case report and literature review. World J EmergSurg [Internet]. 2011; 6(1).
. The surgical procedure aims to place the intestine in a non-rotating position, with the small intestine on the right side of the abdomen and the colon on the left
[9]
Langer JC. Intestinal rotation abnormalities and midgut volvulus. Surg Clin North Am [Internet]. 2017; 97(1): 147-59.
In this way, the surgical intervention of the discussed patient was carried out. Exploratory laparoscopic and Ladd's procedure was done as the patient had chronic symptoms attributable to malrotation. In the follow-up evaluation, the patient returned within 3 months and 10 years after without recurrence of symptoms and without complications. For which there are few reports of this approach in adults and has been suggested, as it has good results and low morbidity
[3]
Araújo URM e. F de, El Tawil II. Má rotação intestinal em adulto, relato de caso e revisão da literatura. ArqBrasCir Dig [Internet]. 2009; 22(4): 240-2.
Intestinal malrotation in adults manifests with a wide range of symptoms, making diagnosis challenging
[10]
Abdillahi Mahamoud C, Egueh Nour A, Bouknani N, Benslima N, Rami A. Diagnostic challenges in adult intestinal malrotation: A case report and literature review. Cureus [Internet]. 2024; 16(1): e52281.
. Its occurrence in adulthood is uncommon, and clinical diagnosis can be difficult
[21]
Ribeiro T, Greene B, Bennett S, Msallak H, Karanicolas P. Variations of intestinal malrotation in adults: A case report of midgut volvulus and literature review for the surgeon. Int J Surg Case Rep [Internet]. 2022; 91(106750): 106750.
. Timely imaging and early medical intervention are essential for enhancing patient outcomes.
The Ladd procedure remains a reliable and efficient surgical method for managing this condition. There are recent reports of the use of the laparoscopic approach in the surgical treatment of intestinal malrotation. The technique seems to be safe and effective when performed by experienced laparoscopic surgeons, especially in the absence of volvulus
[17]
Emanuwa OF, Ayantunde AA, Davies TW. Midgut malrotation first presenting as acute bowel obstruction in adulthood: a case report and literature review. World J EmergSurg [Internet]. 2011; 6(1).
. With this, a less invasive surgical technique via laparoscopy achieved complete correction of the malrotation and improvement of the patient's symptoms.
Fernando Freire Lisboa Junior: Investigation, Resources
Luis Fernando Nunes Ferreira: Software, Validation
Gabriel Diniz Câmara Dantas: Investigation, Writing - original draft
Gabriel Carvalho de Oliveira Cruz: Conceptualization, Validation
Ethics Approval
The study followed the ethical and legal standards recommended by Resolution 466/12 of the National Health Council and was approved by the Research Ethics Committee of the Onofre Lopes University Hospital. Written informed consent was obtained from the patient for publication of the details of her medical case and any accompanying images.
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
Adams SD, Stanton MP. Malrotation and intestinal atresias. Early Hum Dev [Internet]. 2014; 90(12): 921-5.
Yin M-D, Hao L-L, Li G, Li Y-T, Xu B-L, Chen X-R. Adult-onset congenital intestinal malrotation: A case report and literature review. Medicine (Baltimore) [Internet]. 2024; 103(8): e37249.
Araújo URM e. F de, El Tawil II. Má rotação intestinal em adulto, relato de caso e revisão da literatura. ArqBrasCir Dig [Internet]. 2009; 22(4): 240-2.
Elgeyoushy F, Qari AS, Faidh RA. A rare case of congenital intestinal malrotation presented as an intestinal obstruction in an adult. Cureus [Internet]. 2023; 15(12): e49812.
Aregawi AB, Geremew TT, Legese AT, Bahru TT. A rare case of adult intestinal malrotation: A case report. Int J Surg Case Rep [Internet]. 2025; 127(110848): 110848.
Abdillahi Mahamoud C, Egueh Nour A, Bouknani N, Benslima N, Rami A. Diagnostic challenges in adult intestinal malrotation: A case report and literature review. Cureus [Internet]. 2024; 16(1): e52281.
Martinez SA, Fligor SC, Tsikis S, Short M, Corcoran KE, Rogers A, et al. IMPOWER: a national patient-generated registry for intestinal malrotation exploring diagnosis, treatment, and surgical outcomes. Orphanet J Rare Dis [Internet]. 2023; 18(1): 113.
Birajdar S, Rao SC, Bettenay F. Role of upper gastrointestinal contrast studies for suspected malrotation in neonatal population. J Paediatr Child H. 2017; 53(7): 644-9.
[13]
Shimanuki Y, Aihara T, Takano H, Moritani T, Oguma E, Kuroki H, et al. Clockwise whirlpool sign at color Doppler US: an objective and definite sign of midgut volvulus. Radiology [Internet]. 1996; 199(1): 261-4.
Xiong Z, Shen Y, Morelli JN, Li Z, Hu X, Hu D. CT facilitates improved diagnosis of adult intestinal malrotation: a 7-year retrospective study based on 332 cases. Insights Imaging [Internet]. 2021; 12(1): 58.
Eccleston JL, Su H, Ling A, Heller T, Koh C. Gastrointestinal: Adult presentation of intestinal malrotation: Journal of Gastroenterology and Hepatology. J GastroenterolHepatol [Internet]. 2016; 31(8): 1382-1382.
Emanuwa OF, Ayantunde AA, Davies TW. Midgut malrotation first presenting as acute bowel obstruction in adulthood: a case report and literature review. World J EmergSurg [Internet]. 2011; 6(1).
Alghamdi T, Alghamdi AM, Agafli FH, Mahmoud A. Adult intestinal malrotation with atypical presentation: A case report and diagnostic challenge. Am J Case Rep [Internet]. 2024; 25: e945197.
Ribeiro T, Greene B, Bennett S, Msallak H, Karanicolas P. Variations of intestinal malrotation in adults: A case report of midgut volvulus and literature review for the surgeon. Int J Surg Case Rep [Internet]. 2022; 91(106750): 106750.
Lisboa, F. F., Junior, F. F. L., Ferreira, L. F. N., Dantas, G. D. C., Cruz, G. C. D. O. (2025). A Rare Case of Adult Symptomatic Intestinal Malrotation Treated with Laparoscopic Ladd Procedure: Case Report. Journal of Surgery, 13(4), 82-86. https://doi.org/10.11648/j.js.20251304.13
Lisboa, F. F.; Junior, F. F. L.; Ferreira, L. F. N.; Dantas, G. D. C.; Cruz, G. C. D. O. A Rare Case of Adult Symptomatic Intestinal Malrotation Treated with Laparoscopic Ladd Procedure: Case Report. J. Surg.2025, 13(4), 82-86. doi: 10.11648/j.js.20251304.13
@article{10.11648/j.js.20251304.13,
author = {Fernando Freire Lisboa and Fernando Freire Lisboa Junior and Luis Fernando Nunes Ferreira and Gabriel Diniz Câmara Dantas and Gabriel Carvalho de Oliveira Cruz},
title = {A Rare Case of Adult Symptomatic Intestinal Malrotation Treated with Laparoscopic Ladd Procedure: Case Report
},
journal = {Journal of Surgery},
volume = {13},
number = {4},
pages = {82-86},
doi = {10.11648/j.js.20251304.13},
url = {https://doi.org/10.11648/j.js.20251304.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.js.20251304.13},
abstract = {Background: Intestinal malrotation is a congenital condition caused by incomplete or absent rotation of the intestine around the superior mesenteric artery during embryonic development. It is typically presents in the neonatal period. In adults, it is rare (0.2%) and often asymptomatic, discovered incidentally during exams or surgeries. The clinical context in an adult patient can cause chronic symptoms such as intermittent abdominal pain, dyspepsia, nausea, vomiting and abdominal swelling. Diagnosis is best achieved with an upper gastrointestinal contrast study, while CT scan or MRI may detect it incidentally. Surgical correction (Ladd’s procedure) involves reducing volvulus (if present), removing Ladd's bands, and broadening the mesenteric base. This case is noteworthy due to the limited number of similar reports documented globally. Case Presentation: A 67-year-old woman presented with a 4-month history of weight loss, loss of appetite, and episodes of abdominal pain. An abdominal CT revealed signs of intestinal malrotation, and an MRI confirmed these findings, showing abnormal positioning of intestinal loops and vascular structures. Exploratory laparoscopy was performed, and intraoperative findings confirmed the diagnosis. The entire adhered right colon was released from the sigmoid at the angle of Treitz and was repositioned to the right side of the abdomen with the cecum. The patient recovered well, was discharged on the second postoperative day, and remained asymptomatic during follow-up visits at 8 days, 45 days, 3 months post-surgery and ten years after. Discussion and Conclusion: Identifying intestinal malrotation in adults is challenging because of the broad range and vague nature of the symptoms. Diagnostic delays can result in serious complications and less favorable surgical outcomes. Treatment depends on symptomatology and intraoperative findings. Ladd’s Procedure remains the standard approach, involving repositioning of the intestines and release of abnormal bands. The patient in question underwent successful laparoscopic correction, with complete symptom resolution and no complications during follow-up.},
year = {2025}
}
TY - JOUR
T1 - A Rare Case of Adult Symptomatic Intestinal Malrotation Treated with Laparoscopic Ladd Procedure: Case Report
AU - Fernando Freire Lisboa
AU - Fernando Freire Lisboa Junior
AU - Luis Fernando Nunes Ferreira
AU - Gabriel Diniz Câmara Dantas
AU - Gabriel Carvalho de Oliveira Cruz
Y1 - 2025/07/23
PY - 2025
N1 - https://doi.org/10.11648/j.js.20251304.13
DO - 10.11648/j.js.20251304.13
T2 - Journal of Surgery
JF - Journal of Surgery
JO - Journal of Surgery
SP - 82
EP - 86
PB - Science Publishing Group
SN - 2330-0930
UR - https://doi.org/10.11648/j.js.20251304.13
AB - Background: Intestinal malrotation is a congenital condition caused by incomplete or absent rotation of the intestine around the superior mesenteric artery during embryonic development. It is typically presents in the neonatal period. In adults, it is rare (0.2%) and often asymptomatic, discovered incidentally during exams or surgeries. The clinical context in an adult patient can cause chronic symptoms such as intermittent abdominal pain, dyspepsia, nausea, vomiting and abdominal swelling. Diagnosis is best achieved with an upper gastrointestinal contrast study, while CT scan or MRI may detect it incidentally. Surgical correction (Ladd’s procedure) involves reducing volvulus (if present), removing Ladd's bands, and broadening the mesenteric base. This case is noteworthy due to the limited number of similar reports documented globally. Case Presentation: A 67-year-old woman presented with a 4-month history of weight loss, loss of appetite, and episodes of abdominal pain. An abdominal CT revealed signs of intestinal malrotation, and an MRI confirmed these findings, showing abnormal positioning of intestinal loops and vascular structures. Exploratory laparoscopy was performed, and intraoperative findings confirmed the diagnosis. The entire adhered right colon was released from the sigmoid at the angle of Treitz and was repositioned to the right side of the abdomen with the cecum. The patient recovered well, was discharged on the second postoperative day, and remained asymptomatic during follow-up visits at 8 days, 45 days, 3 months post-surgery and ten years after. Discussion and Conclusion: Identifying intestinal malrotation in adults is challenging because of the broad range and vague nature of the symptoms. Diagnostic delays can result in serious complications and less favorable surgical outcomes. Treatment depends on symptomatology and intraoperative findings. Ladd’s Procedure remains the standard approach, involving repositioning of the intestines and release of abnormal bands. The patient in question underwent successful laparoscopic correction, with complete symptom resolution and no complications during follow-up.
VL - 13
IS - 4
ER -
Lisboa, F. F., Junior, F. F. L., Ferreira, L. F. N., Dantas, G. D. C., Cruz, G. C. D. O. (2025). A Rare Case of Adult Symptomatic Intestinal Malrotation Treated with Laparoscopic Ladd Procedure: Case Report. Journal of Surgery, 13(4), 82-86. https://doi.org/10.11648/j.js.20251304.13
Lisboa, F. F.; Junior, F. F. L.; Ferreira, L. F. N.; Dantas, G. D. C.; Cruz, G. C. D. O. A Rare Case of Adult Symptomatic Intestinal Malrotation Treated with Laparoscopic Ladd Procedure: Case Report. J. Surg.2025, 13(4), 82-86. doi: 10.11648/j.js.20251304.13
@article{10.11648/j.js.20251304.13,
author = {Fernando Freire Lisboa and Fernando Freire Lisboa Junior and Luis Fernando Nunes Ferreira and Gabriel Diniz Câmara Dantas and Gabriel Carvalho de Oliveira Cruz},
title = {A Rare Case of Adult Symptomatic Intestinal Malrotation Treated with Laparoscopic Ladd Procedure: Case Report
},
journal = {Journal of Surgery},
volume = {13},
number = {4},
pages = {82-86},
doi = {10.11648/j.js.20251304.13},
url = {https://doi.org/10.11648/j.js.20251304.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.js.20251304.13},
abstract = {Background: Intestinal malrotation is a congenital condition caused by incomplete or absent rotation of the intestine around the superior mesenteric artery during embryonic development. It is typically presents in the neonatal period. In adults, it is rare (0.2%) and often asymptomatic, discovered incidentally during exams or surgeries. The clinical context in an adult patient can cause chronic symptoms such as intermittent abdominal pain, dyspepsia, nausea, vomiting and abdominal swelling. Diagnosis is best achieved with an upper gastrointestinal contrast study, while CT scan or MRI may detect it incidentally. Surgical correction (Ladd’s procedure) involves reducing volvulus (if present), removing Ladd's bands, and broadening the mesenteric base. This case is noteworthy due to the limited number of similar reports documented globally. Case Presentation: A 67-year-old woman presented with a 4-month history of weight loss, loss of appetite, and episodes of abdominal pain. An abdominal CT revealed signs of intestinal malrotation, and an MRI confirmed these findings, showing abnormal positioning of intestinal loops and vascular structures. Exploratory laparoscopy was performed, and intraoperative findings confirmed the diagnosis. The entire adhered right colon was released from the sigmoid at the angle of Treitz and was repositioned to the right side of the abdomen with the cecum. The patient recovered well, was discharged on the second postoperative day, and remained asymptomatic during follow-up visits at 8 days, 45 days, 3 months post-surgery and ten years after. Discussion and Conclusion: Identifying intestinal malrotation in adults is challenging because of the broad range and vague nature of the symptoms. Diagnostic delays can result in serious complications and less favorable surgical outcomes. Treatment depends on symptomatology and intraoperative findings. Ladd’s Procedure remains the standard approach, involving repositioning of the intestines and release of abnormal bands. The patient in question underwent successful laparoscopic correction, with complete symptom resolution and no complications during follow-up.},
year = {2025}
}
TY - JOUR
T1 - A Rare Case of Adult Symptomatic Intestinal Malrotation Treated with Laparoscopic Ladd Procedure: Case Report
AU - Fernando Freire Lisboa
AU - Fernando Freire Lisboa Junior
AU - Luis Fernando Nunes Ferreira
AU - Gabriel Diniz Câmara Dantas
AU - Gabriel Carvalho de Oliveira Cruz
Y1 - 2025/07/23
PY - 2025
N1 - https://doi.org/10.11648/j.js.20251304.13
DO - 10.11648/j.js.20251304.13
T2 - Journal of Surgery
JF - Journal of Surgery
JO - Journal of Surgery
SP - 82
EP - 86
PB - Science Publishing Group
SN - 2330-0930
UR - https://doi.org/10.11648/j.js.20251304.13
AB - Background: Intestinal malrotation is a congenital condition caused by incomplete or absent rotation of the intestine around the superior mesenteric artery during embryonic development. It is typically presents in the neonatal period. In adults, it is rare (0.2%) and often asymptomatic, discovered incidentally during exams or surgeries. The clinical context in an adult patient can cause chronic symptoms such as intermittent abdominal pain, dyspepsia, nausea, vomiting and abdominal swelling. Diagnosis is best achieved with an upper gastrointestinal contrast study, while CT scan or MRI may detect it incidentally. Surgical correction (Ladd’s procedure) involves reducing volvulus (if present), removing Ladd's bands, and broadening the mesenteric base. This case is noteworthy due to the limited number of similar reports documented globally. Case Presentation: A 67-year-old woman presented with a 4-month history of weight loss, loss of appetite, and episodes of abdominal pain. An abdominal CT revealed signs of intestinal malrotation, and an MRI confirmed these findings, showing abnormal positioning of intestinal loops and vascular structures. Exploratory laparoscopy was performed, and intraoperative findings confirmed the diagnosis. The entire adhered right colon was released from the sigmoid at the angle of Treitz and was repositioned to the right side of the abdomen with the cecum. The patient recovered well, was discharged on the second postoperative day, and remained asymptomatic during follow-up visits at 8 days, 45 days, 3 months post-surgery and ten years after. Discussion and Conclusion: Identifying intestinal malrotation in adults is challenging because of the broad range and vague nature of the symptoms. Diagnostic delays can result in serious complications and less favorable surgical outcomes. Treatment depends on symptomatology and intraoperative findings. Ladd’s Procedure remains the standard approach, involving repositioning of the intestines and release of abnormal bands. The patient in question underwent successful laparoscopic correction, with complete symptom resolution and no complications during follow-up.
VL - 13
IS - 4
ER -