Gastric GISTs are rare tumours that are often detected late. The aim of this study was to describe the different treatment modalities for gastric GISTs at Bouake University Hospital. It was retrospective study of 17 patients with gastric GIST between January 2013 and December 2023. GISTs accounted for 4.2% of all gastric tumours. The main reason for consultation was an abdominal mass. The average duration of progression was 10.9 months ± 2.1 months. FOGD, performed in 7 patients, suspected GIST in only one case. Abdominal CT scan, performed in 15 patients, was suggestive of GIST in 8 cases. The tumour was located in the antrum in 11 cases. There was extension to neighbouring organs in 5 cases. The tumours were classified as stage III in 9 cases. Immunohistochemistry confirmed the diagnosis of GIST with expression of C-KIT (CD117) antibodies in all cases. GIST is most often diagnosed at the stage of a large abdominal mass. Immunohistochemistry, which allows for diagnostic confirmation, is not accessible to most patients.
| Published in | Journal of Surgery (Volume 13, Issue 5) |
| DOI | 10.11648/j.js.20251305.13 |
| Page(s) | 134-140 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Stomach, GIST, Immunohistochemistry, Stromal Tumours
Clinical signs | Numbers | Percentages |
|---|---|---|
Abdominal mass | 17 | 100 |
Abdominal pain | 12 | 70,6 |
Constipation | 10 | 58,8 |
Weight loss | 9 | 52,9 |
Clinical anaemia | 7 | 41,2 |
Anorexia, asthenia | 5 | 29,4 |
Vomiting | 4 | 23,5 |
Oedema of the lower limbs | 2 | 11,8 |
TNM grade | Numbers | Percentage | |
|---|---|---|---|
T | T1 | 0 | 0 |
T2 | 1 | 5,9 | |
T3 | 9 | 52,9 | |
T4 | 7 | 41.2 | |
N | N0 | 15 | 88,2 |
N1 | 2 | 11,8 | |
M | M0 | 17 | 100 |
Procedures | Numbers | Perrcentages |
|---|---|---|
Partial gastrectomy | 17 | 100 |
Segmental colectomy of the transverse colon | 03 | 17,6 |
Splenectomy | 02 | 11,8 |
Partial resection of the mesocolon | 01 | 5,9 |
Characteristics | Patient 1 | Patient 2 | Patients 3 |
|---|---|---|---|
Gender | Male | Male | Female |
Age | 59 years old | 69 years old | 49 years old |
History | Epigastric pain | Epigastric pain | Epigastric pain |
Time to progression | 16 months | 10 months | 6 months |
Mode of onset | Recurrent | Primary | Primary |
General condition | Preserved | Preserved | Altered |
Tumour size | 25 cm | 30 cm | 20 cm |
Tumour location | Antrum | Large curvature | Antrum |
Local spread | Localised | Invasion of the transverse colon | Invasion of transverse colon, liver, spleen |
Procedure | Sealed gastrectomy | Sealed gastrectomy, colectomy | Sealed gastrectomy + colectomy + splenectomy |
Type of resection | R0 | R0 | R1 |
Stage of progression | pT4 | pT4 | |
Cause of death | Haemorrhagic shock | PPO | Cachexia |
Time to death | H8 | Day 7 | Day 10 |
GIST | Gastro Intestinal Stroma Tumour |
OGDE | Esophago-Gastroduodenal Endoscopy |
TNM | Tumour, Node, Metastasis |
| [1] | Brun-stang C, Bedossa P, Blay JY, JMC, Le Cesne A, Monges G. Les tumeurs stromales gastro-intestinales: prévalences et incidences en France. Gastroenterol Clin Biol 2004; 28: 102-5. |
| [2] | Saïd HRT, Nawal Y. Advances and therapeutic indications in gastrointestinal stromal tumours. Alg J med Heal res 2022; 1(3): 6. |
| [3] | Bucher P, Egger J, Gervaz P. An audit of surgical management of gastrointestinal stromal tumors (GIST). Eur J Surg Oncol 2006; 32: 310-4. |
| [4] | Bucher P, Villiger P, Egger J. Management of gastrointestinal stromal tumors: From diagnosis to treatment. swiss Med Wkly 2004; 134: 145-53. |
| [5] | Yan H, Marchettini P, Acherman YI. Prognostic assessment of gastrointestinal stromal tumour. Am J Clin Oncol. 2003; 26: 221-228. |
| [6] | Miettinen M and Lasota J. Gastrointestinal stromal tumors: pathology and prognosis at different sites. Semin Diagn Pathol 2006; 23: 70-83. |
| [7] | Joensuu H, Fletcher C, Dimitrijevic S, Silberman S, Roberts P, Demetri G. Management of malignant gastrointestinal stromal tumors. Lancet Oncol 2002; 3: 655-64. |
| [8] | Miettinen M, Sobin LH, Sarlomo-Rikala M. Immunohistochemical spectrum of GISTs at different sites and their differential diagnosis with a référencez to CD117 (KIT). Mod Pathol 2000; 13: 1134-42. |
| [9] | Nguyen VU, Taylor A. Gastrointestinal stromale tumors leiomyoma/leiomysarcoma. E Med Gastrointest 2006; 11 p. |
| [10] | Bettini G, Morini M, Marcato PS. Gastrointestinal spindle cell tumours of the dog: histological and immunohistochemical study. J. Comp. Pathol 2003; 129: 283-93. |
| [11] | Dematteo RP, Heinrich MC, El-Rifai WM, Demetri G. Clinical management of gastrointestinal stromal tumors: before and after STI 571. Hum Pathol 2002; 33: 466-77. |
| [12] | Demetri GD, Van Oosterom AT, Garrett CR, Blackstein ME, Shah MH, Verweij J et al. Efficacy and safety of sunitinib in patients with advanced gastrointestinal stromal tumour after failure of imatinib: a randomised controlled trial. Lancet. 2006; 368: 1329-38. |
| [13] | Kreiker J, Daou R, Aftimos G. Tumeurs stromales gastriques Présentations de deux cas avec étude immunohistochimique. Revue de la littérature. J Méd Lib 2002; 50(5-6): 226-36. |
| [14] | Clère F, Carola E, Halimi C, Gramont AD, Y Panis. Actualités sur les tumeurs stromales gastro-intestinales: à partir de sept observations de tumeurs malignes. Rev Méd Int 2002; 23: 499- 507. |
| [15] | Barrier A, M. Huguier M, Levard H, Montario T, Fagniez PL, Sauvanet A et les Associations françaises de recherche en chirurgie. Tumeurs gastriques conjonctives. Résultats d’une étude multicentrique. Chirurgie 1999; 124: 494-502. |
| [16] | N’Dah KJ, Troh E, Doukouré B; Koffi KE, Abouna AD, Traoré B et Al. Aspects anatomo-cliniques des tumeurs stromales gastro-intestinales à Abibjan. Rev Afr Pathol 2013; 12(1-2): 21-30. |
| [17] | Ian Judson, Ramesh Bulusu, Beatrice Seddon, Adam Dangoor, Newton Wong, Satvinder Mudan. UK clinical practice guidelines for the management of gastrointestinal stromal tumours (GIST). Clinical Sarcoma Research 2017; 7: 6. |
| [18] | Mazur MT and Clark HB. Gastric stromal tumors. Reappraisal of histogenesis. Am J Surg pathol. 1983; 7: 507-519. |
APA Style
Mamadou, T., Ismael, L. B. K., Bernadette, N. A., Amos, E. S., Amos, K. B., et al. (2025). Gastrointestinal Stromal Tumour Management at the Bouake University Hospital. Journal of Surgery, 13(5), 134-140. https://doi.org/10.11648/j.js.20251305.13
ACS Style
Mamadou, T.; Ismael, L. B. K.; Bernadette, N. A.; Amos, E. S.; Amos, K. B., et al. Gastrointestinal Stromal Tumour Management at the Bouake University Hospital. J. Surg. 2025, 13(5), 134-140. doi: 10.11648/j.js.20251305.13
@article{10.11648/j.js.20251305.13,
author = {Traore Mamadou and Leh Bi Kalou Ismael and N’Dri Ahou Bernadette and Ekra Serge Amos and Kouakou Blaise Amos and Bamba Inza and Akowendo Djahou Eczechiel and Anzoua Kouakou Ibrahim and Kouakou Kouame Bernadin},
title = {Gastrointestinal Stromal Tumour Management at the Bouake University Hospital
},
journal = {Journal of Surgery},
volume = {13},
number = {5},
pages = {134-140},
doi = {10.11648/j.js.20251305.13},
url = {https://doi.org/10.11648/j.js.20251305.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.js.20251305.13},
abstract = {Gastric GISTs are rare tumours that are often detected late. The aim of this study was to describe the different treatment modalities for gastric GISTs at Bouake University Hospital. It was retrospective study of 17 patients with gastric GIST between January 2013 and December 2023. GISTs accounted for 4.2% of all gastric tumours. The main reason for consultation was an abdominal mass. The average duration of progression was 10.9 months ± 2.1 months. FOGD, performed in 7 patients, suspected GIST in only one case. Abdominal CT scan, performed in 15 patients, was suggestive of GIST in 8 cases. The tumour was located in the antrum in 11 cases. There was extension to neighbouring organs in 5 cases. The tumours were classified as stage III in 9 cases. Immunohistochemistry confirmed the diagnosis of GIST with expression of C-KIT (CD117) antibodies in all cases. GIST is most often diagnosed at the stage of a large abdominal mass. Immunohistochemistry, which allows for diagnostic confirmation, is not accessible to most patients.
},
year = {2025}
}
TY - JOUR T1 - Gastrointestinal Stromal Tumour Management at the Bouake University Hospital AU - Traore Mamadou AU - Leh Bi Kalou Ismael AU - N’Dri Ahou Bernadette AU - Ekra Serge Amos AU - Kouakou Blaise Amos AU - Bamba Inza AU - Akowendo Djahou Eczechiel AU - Anzoua Kouakou Ibrahim AU - Kouakou Kouame Bernadin Y1 - 2025/09/25 PY - 2025 N1 - https://doi.org/10.11648/j.js.20251305.13 DO - 10.11648/j.js.20251305.13 T2 - Journal of Surgery JF - Journal of Surgery JO - Journal of Surgery SP - 134 EP - 140 PB - Science Publishing Group SN - 2330-0930 UR - https://doi.org/10.11648/j.js.20251305.13 AB - Gastric GISTs are rare tumours that are often detected late. The aim of this study was to describe the different treatment modalities for gastric GISTs at Bouake University Hospital. It was retrospective study of 17 patients with gastric GIST between January 2013 and December 2023. GISTs accounted for 4.2% of all gastric tumours. The main reason for consultation was an abdominal mass. The average duration of progression was 10.9 months ± 2.1 months. FOGD, performed in 7 patients, suspected GIST in only one case. Abdominal CT scan, performed in 15 patients, was suggestive of GIST in 8 cases. The tumour was located in the antrum in 11 cases. There was extension to neighbouring organs in 5 cases. The tumours were classified as stage III in 9 cases. Immunohistochemistry confirmed the diagnosis of GIST with expression of C-KIT (CD117) antibodies in all cases. GIST is most often diagnosed at the stage of a large abdominal mass. Immunohistochemistry, which allows for diagnostic confirmation, is not accessible to most patients. VL - 13 IS - 5 ER -
General and Digestive Surgery Department, Bouake University Hospital, Bouaké, Côte D’Ivoire
General and Digestive Surgery Department, Bouake University Hospital, Bouaké, Côte D’Ivoire
General and Digestive Surgery Department, Bouake University Hospital, Bouaké, Côte D’Ivoire
General and Digestive Surgery Department, Bouake University Hospital, Bouaké, Côte D’Ivoire
General and Digestive Surgery Department, Bouake University Hospital, Bouaké, Côte D’Ivoire
General and Digestive Surgery Department, Bouake University Hospital, Bouaké, Côte D’Ivoire
General and Digestive Surgery Department, Bouake University Hospital, Bouaké, Côte D’Ivoire
General and Digestive Surgery Department, Bouake University Hospital, Bouaké, Côte D’Ivoire
General and Digestive Surgery Department, Bouake University Hospital, Bouaké, Côte D’Ivoire
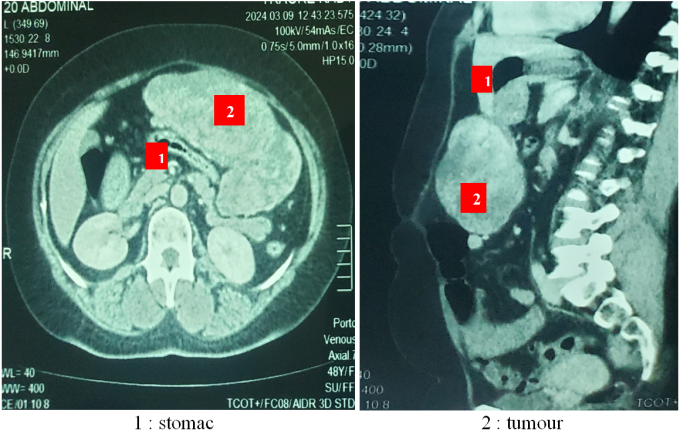
Figure 1. Transverse and sagittal CT scans showing a tumour developing at the expense of the gastric wall.
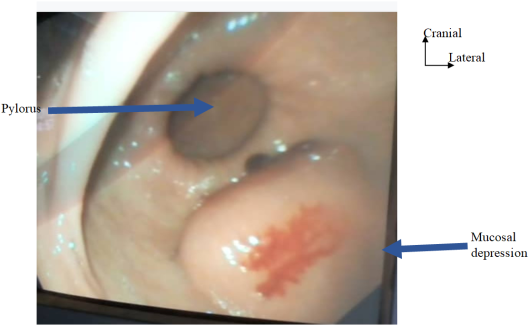
Figure 2. Endoscopic view of a depression in the gastric mucosa caused by an extraluminal mass with erosion of the mucosa, suggesting a GIST.
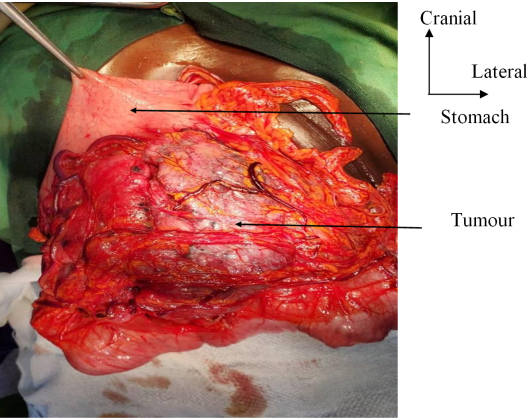
Figure 3. Tumour developed at the expense of the posterior face of the gastric antrum.
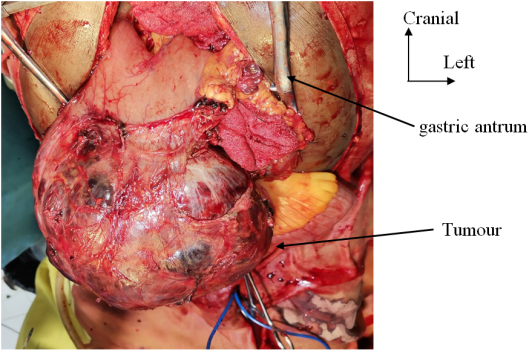
Figure 4. Necrotic-haemorrhagic tumour mass developed at the expense of the lower edge of the antrum.
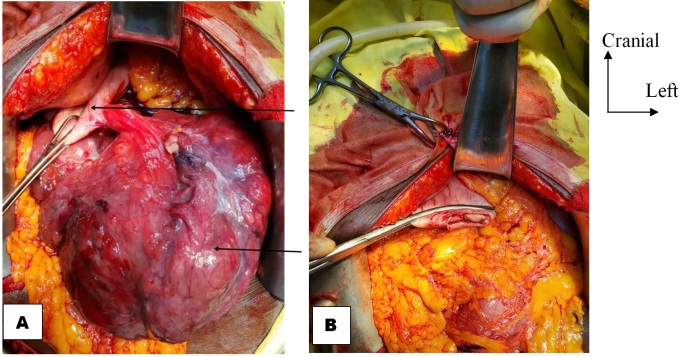
Figure 5. (A) Large pedunculated tumour on the lateral edge of the greater curvature of the stomach. (B) Stump after sealed gastrectomy.

Figure 6. Tumour mass after gastrectomy.
Information

