Method: We examined how body weight affects cardiovascular health in adults aged 30–50 in Khyber Pakhtunkhwa (KPK), Pakistan, by analyzing de-identified records from hospitals (June 2022–March 2025). We calculated body mass index (BMI) and classified patients by WHO Asian criteria: normal (18.5–22.9), overweight (23.0–27.4), and obese (≥27.5 kg/m2). We recorded hypertension (HTN), coronary artery disease (CAD), myocardial infarction (MI), and arrhythmia, and applied statistical tests (ANOVA, logistic regression) to derive odds ratios (OR) with 95% confidence intervals (CI). Results: Mean age was 39.8 years (SD 5.7); 48% were female; 200 were normal-weight, 178 overweight, and 122 obese. Hypertension was present in 20.0%, 39.9%, and 58.2% of the normal, overweight, and obese participants (p<0.001). CAD rates were 4.5%, 6.7%, and 22.1%; MI rates were 2.5%, 9.6%, and 15.6% in the normal, overweight, and obese groups (p<0.001). Systolic BP rose from 120 mmHg (normal) to 139 mmHg (obese) (p<0.001), and BMI strongly correlated with BP (r≈0.50, p<0.001). In adjusted models, overweight vs normal had OR=2.70 (95% CI 1.61–4.52) and obese vs normal had OR=5.75 (3.34–9.91) for HTN (p<0.001). For CAD, obese vs normal had OR=6.14 (2.77–13.61, p<0.001); for MI, overweight had OR≈4.14 (1.04–16.47) and obese OR≈7.10 (2.69–18.70). Obesity also increased arrhythmia odds (OR≈2.79 [1.16–6.71]). ROC AUCs were 0.79 for both HTN (CI 0.74–0.84) and CAD (CI 0.72–0.86). Conclusion: Excess body weight is a major problem directly linked to high blood pressure and serious heart conditions, reflecting a global pattern. Preventing obesity should be a priority to reduce the growing heart disease burden in the region.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Body Mass Index, Cardiovascular Disease Risk Factors, Overweight and Obesity, Hypertension
1. Introduction
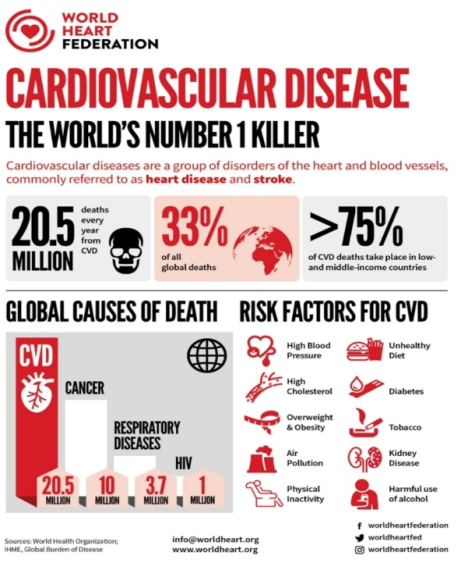
KPK is a populous province of Pakistan with diverse urban and rural populations. Cardiovascular diseases (CVD) are the leading cause of death globally, responsible for roughly 17.9 million deaths each year
[1]
World Health Organization. Cardiovascular diseases. Available from:
. Major risk factors include overweight and obesity, which have reached epidemic proportions globally. In 2022, WHO estimated ~43% of adults were overweight and 16% have obesity
[2]
World Health Organization. Obesity and overweight: fact sheet. Available from:
. Excess adiposity contributes to diabetes, dyslipidemia, hypertension, and atherosclerosis, thus markedly increasing CVD risk
[3]
Lavie CJ, Milani RV, Ventura HO. Obesity and cardiovascular disease: risk factor, paradox, and impact of weight loss. Journal of the American college of cardiology. 2009 May 26; 53(21): 1925-32.
[3]
. Notably, South Asian populations develop metabolic disease at lower BMI thresholds than Western populations, leading WHO experts to recommend lower cutoffs for Asians
[4]
Jih J, Mukherjea A, Vittinghoff E, Nguyen TT, Tsoh JY, Fukuoka Y, Bender MS, Tseng W, Kanaya AM. Using appropriate body mass index cut points for overweight and obesity among Asian Americans. Preventive medicine. 2014 Aug 1; 65: 1-6.
[4]
. In Pakistan, the rapid adoption of sedentary lifestyles and calorie-dense diets has driven a surge in non-communicable diseases (NCDs8)
[5]
Kazmi T, Nagi ML, Razzaq S, Hussnain S, Shahid N, Athar U. Burden of noncommunicable diseases in Pakistan. Eastern Mediterranean Health Journal. 2022; 28(11): 798-804.
[6]
Elahi A, Ali AA, Khan AH, Samad Z, Shahab H, Aziz N, Almas A. Challenges of managing hypertension in Pakistan-a review. Clinical Hypertension. 2023 Jun 15; 29(1): 17.
[5, 6]
. According to WHO data, roughly 43% of adults worldwide are now overweight and about 16% have obesity, indicating an obesity epidemic that disproportionately affects wealthier regions. Overweight and obesity are established risk factors for hypertension and other cardiac conditions. WHO reports estimate that 2.5 billion adults were overweight in 2022 (890 million people have obesity)
[2]
World Health Organization. Obesity and overweight: fact sheet. Available from:
, and that obesity contributes to millions of premature deaths from heart disease and stroke. In Pakistan and KPK, overweight and obesity are increasingly common. A national survey (NDSP 2016–17) found 58% prevalence of generalized obesity (using Asian cutoffs), with KPK having among the highest rates (59%)
[7]
Basit A, Askari S, Zafar J, Riaz M, Fawwad A, Members ND. NDSP 06: Prevalence and risk factors for obesity in urban and rural areas of Pakistan: A study from second National Diabetes Survey of Pakistan (NDSP), 2016–2017. Obesity Research & Clinical Practice. 2021 Jan 1; 15(1): 19-25.
[7]
. Hypertension is also rampant; NDSP reported 46% of adults hypertensive
[8]
Basit A, Tanveer S, Fawwad A, Naeem N, NDSP Members. Prevalence and contributing risk factors for hypertension in urban and rural areas of Pakistan; a study from second National Diabetes Survey of Pakistan (NDSP) 2016–2017. Clinical and Experimental Hypertension. 2020 Apr 2; 42(3): 218-24.
[8]
. In KPK specifically, over half of women were found to be overweight or have obesity. Moreover, about 75% of hypertensive patients were overweight/obese
[9]
Haq Z, Afaq S, Ibrahim M, Zala, Asim M. Prevalence of communicable, non-communicable diseases, disabilities and related risk factors in Khyber Pakhtunkhwa Pakistan: Findings from the Khyber Pakhtunkhwa Integrated Population and Health Survey (2016–17). PloS One. 2025 Feb 3; 20(2): e0308209.
[9]
, underscoring the link between weight and blood pressure in this region. Despite these alarming trends, few studies have directly examined how BMI relates to hard CV outcomes (CAD, MI, arrhythmias) in middle-aged Pakistanis.The current analysis addresses this gap by combining data from two cohorts of middle-aged (30–50 y) adults in KPK. We analyzed 500 patients from major KPK hospitals to test whether higher BMI category is associated with a graded increase in HTN, CAD, MI, and arrhythmia. We applied WHO Asian BMI thresholds
[10]
Whatley M. One-Way ANOVA and the chi-square test of independence. InIntroduction to quantitative analysis for international educators 2022 Apr 26 (pp. 57-74). Cham: Springer International Publishing.
[10]
, and used ANOVA, logistic regression, and ROC methods to quantify these relationships. By linkingregional data to global patterns, our study aims to inform local cardiovascular prevention strategies.
Figure 2. Global CVD risk factors, highlighting overweight/obesity among key contributors.
2. Methods
We conduct a retrospective cross-sectional analysis of de-identified dataset of adults aged between 30–50 who visited to the cardiology departments or internal medicine departments at tertiary care hospitals in Khyber Pakhtunkhwa, Pakistan (including Lady Reading Hospital, KTH, MMC, SGTH) between June 2022 and March 2025. Under a proper approval and informed consent, patient data were reviewed. Exclusion criteria were congenital heart disease or major comorbidities (e.g. chronic kidney disease, cancer). For each patient, height and weight were measured at the index visit. BMI was calculated and categorized according to WHO Asian criteria: normal (18.5–22.9 kg/m2), overweight (23.0–27.4), people with obesity (≥27.5)
[10]
Whatley M. One-Way ANOVA and the chi-square test of independence. InIntroduction to quantitative analysis for international educators 2022 Apr 26 (pp. 57-74). Cham: Springer International Publishing.
[10]
. Blood pressure of patients (Both systolic and Dystolic) were recorded, and laboratory data (fasting glucose, lipid profiles) was also collected from thier medical records. All patients were categorized by BMI as normal, overweight, or people having obesity and were surveyed for history of diabetes, smoking, and the cardiac endpoints. Standard procedures were used for measurement and data collection.
Descriptive statistics characterized each BMI group Table 1. Continuous variables (e.g. BP, glucose) were compared across BMI categories by one-way ANOVA; categorical prevalences by chisquare test
. Pearson correlation evaluated linear relationships (e.g. BMI vs. SBP). Multivariable logistic regression (stepwise age- and sex-adjusted)
[12]
Fawcett T. An introduction to ROC analysis. Pattern recognition letters. 2006 Jun 1; 27(8): 861-74.
[12]
estimated odds ratios (OR) with 95% confidence intervals (CI) for each outcome (HTN, CAD, MI, arrhythmia) comparing overweight vs. normal and obese vs. normal. Model discrimination was assessed by ROC analysis (AUC)
[13]
Hossain FB, Adhikary G, Chowdhury AB, Shawon MS. Association between body mass index (BMI) and hypertension in south Asian population: evidence from nationally-representative surveys. Clinical hypertension. 2019 Dec 15; 25(1): 28.
[13]
. All tests were two-sided, with p<0.05 as significance threshold. Analyses were performed in R (v4.2.2) and SPSS v28.
Table 1. Baseline demographics and cardiovascular outcomes by BMI category.
Variable
Normal (n=200)
Overweight (n=178)
Individuals with Obesity (n=122)
Mean age (mean±SD)
39.8±5.7
39.7± 5.6
39.8±5.9
% Female
45.0%
46.6%
49.2%
Hypertension prevalence
20.0%
39.9%
58.2%
Coronary artery disease
4.5%
6.7%
22.1%
Myocardial infarction
2.5%
9.6%
15.6%
Arrhythmia prevalence
4.5%
6.7%
11.5%
3. Results
The study included 500 patients (mean age ≈39.8 ± 5.7 years; 48% female). BMI groups were 200 normalweight, 178 overweight, and 122 individual with obesity. Baseline characteristics are shown in [Table 1]. Age and sex were similar across groups. Prevalence of hypertension rose sharply with BMI: 20.0% in normal-weight vs. 39.9% (overweight) vs. 58.2% (people with obesity) (p<0.001 by χ2)
[14]
Gupta RD, Parray AA, Kothadia RJ, Pulock OS, Pinky SD, Haider SS, Akonde M, Haider MR. The association between body mass index and abdominal obesity with hypertension among South Asian population: findings from nationally representative surveys. Clinical Hypertension. 2024 Feb 1; 30(1): 3.
[15]
Khan A, Haq FU, Pervez MB, Saleheen D, Frossard PM, Ishaq M, Hakeem A, Sheikh HT, Ahmad U. Anthropometric correlates of blood pressure in normotensive Pakistani subjects. International journal of cardiology. 2008 Feb 29; 124(2): 259-62.
[16]
Yusuf S, Hawken S, Ounpuu S, Bautista L, Franzosi MG, Commerford P, Lang CC, Rumboldt Z, Onen CL, Lisheng L, Tanomsup S. Obesity and the risk of myocardial infarction in 27 000 participants from 52 countries: a case-control study. The Lancet. 2005 Nov 5; 366(9497): 1640-9.
[14-16]
. Coronary artery disease prevalence increased from 4.5% to 6.7% to 22.1% across the normal/overweight/obese categories (p<0.001). Myocardial infarction rates were 2.5%, 9.6%, and 15.6%, respectively (p<0.001). Arrhythmia prevalence likewise rose (4.5%, 6.7%, 11.5%; p=0.002)
[17]
Chew NW, Chong B, Kuo SM, Jayabaskaran J, Cai M, Zheng H, Goh R, Kong G, Chin YH, Imran SS, Liang M. Trends and predictions of metabolic risk factors for acute myocardial infarction: findings from a multiethnic nationwide cohort. The Lancet Regional Health–Western Pacific. 2023 Aug 1; 37.
[18]
Usman S, Bajaj A, Vedamurthy D, Billheimer J. Enhanced Cardiovascular Risk in Pakistan Compared to Other South Asian Countries. Asian Journal of Cardiology Research. 2024 Aug 5; 7(1): 157-75.
[19]
Song R, Jiang Y, Pang J, Wu S, Ma J, Li P, Wu X, Xu F, Wang J, Chen X, Chen Y. Association of obesity phenotypes with risk of cardiovascular disease mortality: a prospective cohort study. BMC Public Health. 2025 Dec; 25(1): 1-9.
[17-19]
. Mean systolic BP increased from 120 to 139 mmHg across BMI groups (ANOVA F≈28.6, p<0.001)
[14]
Gupta RD, Parray AA, Kothadia RJ, Pulock OS, Pinky SD, Haider SS, Akonde M, Haider MR. The association between body mass index and abdominal obesity with hypertension among South Asian population: findings from nationally representative surveys. Clinical Hypertension. 2024 Feb 1; 30(1): 3.
[16]
Yusuf S, Hawken S, Ounpuu S, Bautista L, Franzosi MG, Commerford P, Lang CC, Rumboldt Z, Onen CL, Lisheng L, Tanomsup S. Obesity and the risk of myocardial infarction in 27 000 participants from 52 countries: a case-control study. The Lancet. 2005 Nov 5; 366(9497): 1640-9.
[14, 16]
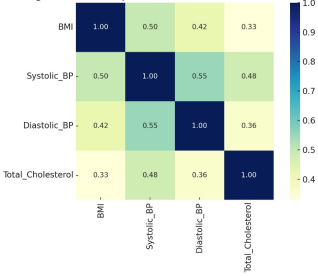
. Figure 2 confirms strong positive correlation of BMI with SBP (r≈0.50, p<0.001).
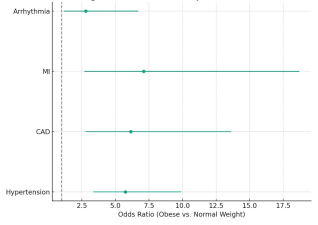
Multivariable logistic regression (age- and sex-adjusted) confirmed these trends [Table 2]. Compared to normal-weight subjects, overweight patients had about 2.7× higher odds of hypertension (OR=2.70; 95% CI 1.61–4.52; p<0.001), whereas obese patients had ≈5.75× higher odds (OR=5.75; 3.34–9.91; p<0.001). For MI, overweight vs. normal OR≈4.14 (CI1.04–16.47, p=0.04), and people with obesity vs. normal OR≈7.10 (CI 2.69–18.70, p<0.001). Coronary artery disease risk was strongly elevated in obesity (OR≈6.14; CI 2.77–13.61; p<0.001). Obese subjects also had higher odds of arrhythmia (OR≈2.79; CI 1.16–6.71; p=0.022). Overweight did not significantly raise arrhythmia risk (OR≈1.54; p=0.38)
[15]
Khan A, Haq FU, Pervez MB, Saleheen D, Frossard PM, Ishaq M, Hakeem A, Sheikh HT, Ahmad U. Anthropometric correlates of blood pressure in normotensive Pakistani subjects. International journal of cardiology. 2008 Feb 29; 124(2): 259-62.
[18]
Usman S, Bajaj A, Vedamurthy D, Billheimer J. Enhanced Cardiovascular Risk in Pakistan Compared to Other South Asian Countries. Asian Journal of Cardiology Research. 2024 Aug 5; 7(1): 157-75.
[19]
Song R, Jiang Y, Pang J, Wu S, Ma J, Li P, Wu X, Xu F, Wang J, Chen X, Chen Y. Association of obesity phenotypes with risk of cardiovascular disease mortality: a prospective cohort study. BMC Public Health. 2025 Dec; 25(1): 1-9.
[15, 18, 19]
. Overall, a clear dose–response was evident, with risk rising stepwise from normal→overweight→obese.
The ROC curves showed good discrimination: the HTN model had AUC≈0.79 (95% CI 0.74–0.84) and the CAD model AUC≈0.79 (0.72–0.86)
[18]
Usman S, Bajaj A, Vedamurthy D, Billheimer J. Enhanced Cardiovascular Risk in Pakistan Compared to Other South Asian Countries. Asian Journal of Cardiology Research. 2024 Aug 5; 7(1): 157-75.
[20]
Our World in Data. Death rate from obesity. Availablefrom
, indicating acceptable predictive performance. (Figures of the OR forest plot and correlation heatmap are presented as Figures 3 [21] and 4, respectively.)
4. Discussion
This combined analysis of two KPK cohorts demonstrates a clear, graded relationship between BMI and cardiovascular risk in adults aged 30–50. Even after adjusting for age and sex, overweight and individuals with obesity had substantially higher odds of hypertension, myocardial infarction, and coronary disease than their normal-weight peers. These findings align with extensive literature
[22]
Ibrahim S, Akram Z, Noreen A, Baig MT, Sheikh S, Huma A, Jabeen A, Lodhi M, Khan SA, Hudda A. Overweight and obesity prevalence and predictors in people living in Karachi. J Pharm Res Int. 2021; 33(31B): 194-202.
[22]
. For example, several metaanalyses in South Asian populations have reported a roughly two- to three-fold increased odds of hypertension in overweight/obese versus normal-weight individuals
[14]
Gupta RD, Parray AA, Kothadia RJ, Pulock OS, Pinky SD, Haider SS, Akonde M, Haider MR. The association between body mass index and abdominal obesity with hypertension among South Asian population: findings from nationally representative surveys. Clinical Hypertension. 2024 Feb 1; 30(1): 3.
[14]
a Karachi community survey found 25% hypertension and overweight/obesity in 34–49% of adults
[23]
Yang Y, Song L, Wang L, Li D, Chen S, Wu S, Tian Y. Effect of body mass index trajectory on lifetime risk of cardiovascular disease in a Chinese population: A cohort study. Nutrition, Metabolism and Cardiovascular Diseases. 2023 Mar 1; 33(3): 523-31.
[23]
, and Chinese cohort studies likewise found elevated MI risk in those with higher BMI
[24]
Wanahita N, Messerli FH, Bangalore S, Gami AS, Somers VK, Steinberg JS. Atrial fibrillation and obesity—results of a meta-analysis. American heart journal. 2008 Feb 1; 155(2): 310-5.
[24]
. Moreover, our finding that obesity confers 5–7×higher odds of HTN and CAD is biologically plausible, as excess adiposity is well known to perturb hemodynamic and metabolic systems
[3]
Lavie CJ, Milani RV, Ventura HO. Obesity and cardiovascular disease: risk factor, paradox, and impact of weight loss. Journal of the American college of cardiology. 2009 May 26; 53(21): 1925-32.
[3]
.
Our results are also consistent with global epidemiology: obesity is estimated to cause 10% of premature deaths worldwide
[2]
World Health Organization. Obesity and overweight: fact sheet. Available from:
Lavie CJ, Milani RV, Ventura HO. Obesity and cardiovascular disease: risk factor, paradox, and impact of weight loss. Journal of the American college of cardiology. 2009 May 26; 53(21): 1925-32.
[2, 3]
, largely via cardiometabolic diseases. In the Framingham Heart Study, each 5– 10 kg/m2 increase in BMI was linked to progressively higher CHD and HTN risk. We observed a strong dose–response [Figure 4] that mirrors these patterns. The correlation heatmap [Figure 4] underscores how BMI interrelates with blood pressure and other risk factors: for example, our Pearson r≈0.50 between BMI and systolic BP (p<0.001) echoes prior reports (Song et al. found r≈0.37 in a South Asian sample). Similarly, meta-analyses show obese individuals have 1.5× higher risk of atrial fibrillation
[25]
Asif M, Aslam M, Altaf S, Atif S, Majid A. Prevalence and sociodemographic factors of overweight and obesity among Pakistani adults. Journal of obesity & metabolic syndrome. 2020 Mar 30; 29(1): 58.
[25]
, consistent with our arrhythmia OR≈2.8 for obesity.
Regionally, our findings emphasize public health urgency in Pakistan. National surveys report very high overweight/obesity rates
[8]
Basit A, Tanveer S, Fawwad A, Naeem N, NDSP Members. Prevalence and contributing risk factors for hypertension in urban and rural areas of Pakistan; a study from second National Diabetes Survey of Pakistan (NDSP) 2016–2017. Clinical and Experimental Hypertension. 2020 Apr 2; 42(3): 218-24.
[9]
Haq Z, Afaq S, Ibrahim M, Zala, Asim M. Prevalence of communicable, non-communicable diseases, disabilities and related risk factors in Khyber Pakhtunkhwa Pakistan: Findings from the Khyber Pakhtunkhwa Integrated Population and Health Survey (2016–17). PloS One. 2025 Feb 3; 20(2): e0308209.
[8, 9]
In KPK, >50% of adults (especially women) are already overweight/obese, and as our data show, many of these individuals will have or develop HTN and ischemic heart disease. Comparable studies in Pakistan have similarly linked BMI with HTN and dyslipidemia. The high rates of hypertension (46% nationally) and obesity (≈58%) underscore the double burden of NCDs here
[8]
Basit A, Tanveer S, Fawwad A, Naeem N, NDSP Members. Prevalence and contributing risk factors for hypertension in urban and rural areas of Pakistan; a study from second National Diabetes Survey of Pakistan (NDSP) 2016–2017. Clinical and Experimental Hypertension. 2020 Apr 2; 42(3): 218-24.
[8]
. Weight control and lifestyle modification are thus critical; obesity is a modifiable risk factor for the very outcomes (heart attack, stroke) that dominate CVD mortality worldwide.
Our results also contribute to the understanding of the “obesity paradox.” While some studies note seemingly better short-term prognosis in overweight CVD patients
[3]
Lavie CJ, Milani RV, Ventura HO. Obesity and cardiovascular disease: risk factor, paradox, and impact of weight loss. Journal of the American college of cardiology. 2009 May 26; 53(21): 1925-32.
[3]
, we confirm that overweight/obesity dramatically raise incidence of CVD risk factors and events. In practice, this implies that prevention of excess weight should remain a priority, even if obese patients may sometimes have paradoxically lower mortality after an acute event.
5. Conclusion
In middle-aged adults in Khyber Pakhtunkhwa, higher BMI was strongly associated with worse cardiovascular health. Overweight and individuals with obesity had significantly greater prevalence and odds of hypertension, coronary disease, myocardial infarction, and arrhythmias than normal-weight peers. These findings are consistent with global data linking excess weight to cardiovascular morbidity. Prevention strategies in Pakistan should emphasize weight management through diet, exercise, and early screening for CVD risk. WHO and other health agencies emphasize modifiable risk control: promoting healthy diet, physical activity, and weight management can substantially reduce blood pressure and heart disease risk. Such interventions have the potential to markedly reduce the burden of hypertension and heart disease in this population.
6. Limitations
This observational study has inherent limitations. The retrospective design cannot prove causation and may suffer from selection bias (patients presenting to hospitals may not represent the general population). Our sample is limited to KPK province and selected hospitals, so findings may not generalize to all of Pakistan. We lacked data on important confounders and lifestyle factors (e.g. diet, physical activity, smoking, socioeconomic status), which could influence both BMI and cardiovascular outcomes. Also, some diagnoses were based on medical record history without systematic adjudication. Despite these caveats, the large sample and consistency with other studies lend credibility to our conclusions.
Abbreviations
MI
Myocardial Infarction
BMI
Body Mass Index
CVD
Cardio Vascular Disease
KPK
Khyber Pakhtunkhwa
HTN
Hypertension
CAD
Coronary Artery Disease
Author Contributions
Syed Sardar Shah: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing
Attiq Ur Rehman: Formal Analysis, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing
Lavie CJ, Milani RV, Ventura HO. Obesity and cardiovascular disease: risk factor, paradox, and impact of weight loss. Journal of the American college of cardiology. 2009 May 26; 53(21): 1925-32.
[4]
Jih J, Mukherjea A, Vittinghoff E, Nguyen TT, Tsoh JY, Fukuoka Y, Bender MS, Tseng W, Kanaya AM. Using appropriate body mass index cut points for overweight and obesity among Asian Americans. Preventive medicine. 2014 Aug 1; 65: 1-6.
[5]
Kazmi T, Nagi ML, Razzaq S, Hussnain S, Shahid N, Athar U. Burden of noncommunicable diseases in Pakistan. Eastern Mediterranean Health Journal. 2022; 28(11): 798-804.
[6]
Elahi A, Ali AA, Khan AH, Samad Z, Shahab H, Aziz N, Almas A. Challenges of managing hypertension in Pakistan-a review. Clinical Hypertension. 2023 Jun 15; 29(1): 17.
[7]
Basit A, Askari S, Zafar J, Riaz M, Fawwad A, Members ND. NDSP 06: Prevalence and risk factors for obesity in urban and rural areas of Pakistan: A study from second National Diabetes Survey of Pakistan (NDSP), 2016–2017. Obesity Research & Clinical Practice. 2021 Jan 1; 15(1): 19-25.
[8]
Basit A, Tanveer S, Fawwad A, Naeem N, NDSP Members. Prevalence and contributing risk factors for hypertension in urban and rural areas of Pakistan; a study from second National Diabetes Survey of Pakistan (NDSP) 2016–2017. Clinical and Experimental Hypertension. 2020 Apr 2; 42(3): 218-24.
[9]
Haq Z, Afaq S, Ibrahim M, Zala, Asim M. Prevalence of communicable, non-communicable diseases, disabilities and related risk factors in Khyber Pakhtunkhwa Pakistan: Findings from the Khyber Pakhtunkhwa Integrated Population and Health Survey (2016–17). PloS One. 2025 Feb 3; 20(2): e0308209.
[10]
Whatley M. One-Way ANOVA and the chi-square test of independence. InIntroduction to quantitative analysis for international educators 2022 Apr 26 (pp. 57-74). Cham: Springer International Publishing.
Fawcett T. An introduction to ROC analysis. Pattern recognition letters. 2006 Jun 1; 27(8): 861-74.
[13]
Hossain FB, Adhikary G, Chowdhury AB, Shawon MS. Association between body mass index (BMI) and hypertension in south Asian population: evidence from nationally-representative surveys. Clinical hypertension. 2019 Dec 15; 25(1): 28.
[14]
Gupta RD, Parray AA, Kothadia RJ, Pulock OS, Pinky SD, Haider SS, Akonde M, Haider MR. The association between body mass index and abdominal obesity with hypertension among South Asian population: findings from nationally representative surveys. Clinical Hypertension. 2024 Feb 1; 30(1): 3.
[15]
Khan A, Haq FU, Pervez MB, Saleheen D, Frossard PM, Ishaq M, Hakeem A, Sheikh HT, Ahmad U. Anthropometric correlates of blood pressure in normotensive Pakistani subjects. International journal of cardiology. 2008 Feb 29; 124(2): 259-62.
[16]
Yusuf S, Hawken S, Ounpuu S, Bautista L, Franzosi MG, Commerford P, Lang CC, Rumboldt Z, Onen CL, Lisheng L, Tanomsup S. Obesity and the risk of myocardial infarction in 27 000 participants from 52 countries: a case-control study. The Lancet. 2005 Nov 5; 366(9497): 1640-9.
[17]
Chew NW, Chong B, Kuo SM, Jayabaskaran J, Cai M, Zheng H, Goh R, Kong G, Chin YH, Imran SS, Liang M. Trends and predictions of metabolic risk factors for acute myocardial infarction: findings from a multiethnic nationwide cohort. The Lancet Regional Health–Western Pacific. 2023 Aug 1; 37.
[18]
Usman S, Bajaj A, Vedamurthy D, Billheimer J. Enhanced Cardiovascular Risk in Pakistan Compared to Other South Asian Countries. Asian Journal of Cardiology Research. 2024 Aug 5; 7(1): 157-75.
[19]
Song R, Jiang Y, Pang J, Wu S, Ma J, Li P, Wu X, Xu F, Wang J, Chen X, Chen Y. Association of obesity phenotypes with risk of cardiovascular disease mortality: a prospective cohort study. BMC Public Health. 2025 Dec; 25(1): 1-9.
[20]
Our World in Data. Death rate from obesity. Availablefrom
Re F, Oguntade AS, Bohrmann B, Bragg F, Carter JL. Associations of general and central adiposity with hypertension and cardiovascular disease among South Asian populations: a systematic review and meta-analysis. BMJ open. 2023 Dec 1; 13(12): e074050.
[22]
Ibrahim S, Akram Z, Noreen A, Baig MT, Sheikh S, Huma A, Jabeen A, Lodhi M, Khan SA, Hudda A. Overweight and obesity prevalence and predictors in people living in Karachi. J Pharm Res Int. 2021; 33(31B): 194-202.
[23]
Yang Y, Song L, Wang L, Li D, Chen S, Wu S, Tian Y. Effect of body mass index trajectory on lifetime risk of cardiovascular disease in a Chinese population: A cohort study. Nutrition, Metabolism and Cardiovascular Diseases. 2023 Mar 1; 33(3): 523-31.
[24]
Wanahita N, Messerli FH, Bangalore S, Gami AS, Somers VK, Steinberg JS. Atrial fibrillation and obesity—results of a meta-analysis. American heart journal. 2008 Feb 1; 155(2): 310-5.
[25]
Asif M, Aslam M, Altaf S, Atif S, Majid A. Prevalence and sociodemographic factors of overweight and obesity among Pakistani adults. Journal of obesity & metabolic syndrome. 2020 Mar 30; 29(1): 58.
Shah, S. S., Rehman, A. U., Khan, Z., Ali, M., Ahmad, A., et al. (2025). Weight and Cardiac Health in Middle Aged People in Khyber Pakhtunkhwa, Pakistan. Pathology and Laboratory Medicine, 9(2), 49-55. https://doi.org/10.11648/j.plm.20250902.12
Shah, S. S.; Rehman, A. U.; Khan, Z.; Ali, M.; Ahmad, A., et al. Weight and Cardiac Health in Middle Aged People in Khyber Pakhtunkhwa, Pakistan. Pathol. Lab. Med.2025, 9(2), 49-55. doi: 10.11648/j.plm.20250902.12
Shah SS, Rehman AU, Khan Z, Ali M, Ahmad A, et al. Weight and Cardiac Health in Middle Aged People in Khyber Pakhtunkhwa, Pakistan. Pathol Lab Med. 2025;9(2):49-55. doi: 10.11648/j.plm.20250902.12
@article{10.11648/j.plm.20250902.12,
author = {Syed Sardar Shah and Attiq Ur Rehman and Ziad Khan and Mohsin Ali and Aftab Ahmad and Shah Nawaz and Saleem Jan and Syed Shayan Ahmad and Rizwan Ullah and Kashif Rasool and Shayan Ali Yousafzai and Shahid Bacha},
title = {Weight and Cardiac Health in Middle Aged People in Khyber Pakhtunkhwa, Pakistan
},
journal = {Pathology and Laboratory Medicine},
volume = {9},
number = {2},
pages = {49-55},
doi = {10.11648/j.plm.20250902.12},
url = {https://doi.org/10.11648/j.plm.20250902.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.plm.20250902.12},
abstract = {Method: We examined how body weight affects cardiovascular health in adults aged 30–50 in Khyber Pakhtunkhwa (KPK), Pakistan, by analyzing de-identified records from hospitals (June 2022–March 2025). We calculated body mass index (BMI) and classified patients by WHO Asian criteria: normal (18.5–22.9), overweight (23.0–27.4), and obese (≥27.5 kg/m2). We recorded hypertension (HTN), coronary artery disease (CAD), myocardial infarction (MI), and arrhythmia, and applied statistical tests (ANOVA, logistic regression) to derive odds ratios (OR) with 95% confidence intervals (CI). Results: Mean age was 39.8 years (SD 5.7); 48% were female; 200 were normal-weight, 178 overweight, and 122 obese. Hypertension was present in 20.0%, 39.9%, and 58.2% of the normal, overweight, and obese participants (pConclusion: Excess body weight is a major problem directly linked to high blood pressure and serious heart conditions, reflecting a global pattern. Preventing obesity should be a priority to reduce the growing heart disease burden in the region.
},
year = {2025}
}
TY - JOUR
T1 - Weight and Cardiac Health in Middle Aged People in Khyber Pakhtunkhwa, Pakistan
AU - Syed Sardar Shah
AU - Attiq Ur Rehman
AU - Ziad Khan
AU - Mohsin Ali
AU - Aftab Ahmad
AU - Shah Nawaz
AU - Saleem Jan
AU - Syed Shayan Ahmad
AU - Rizwan Ullah
AU - Kashif Rasool
AU - Shayan Ali Yousafzai
AU - Shahid Bacha
Y1 - 2025/10/22
PY - 2025
N1 - https://doi.org/10.11648/j.plm.20250902.12
DO - 10.11648/j.plm.20250902.12
T2 - Pathology and Laboratory Medicine
JF - Pathology and Laboratory Medicine
JO - Pathology and Laboratory Medicine
SP - 49
EP - 55
PB - Science Publishing Group
SN - 2640-4478
UR - https://doi.org/10.11648/j.plm.20250902.12
AB - Method: We examined how body weight affects cardiovascular health in adults aged 30–50 in Khyber Pakhtunkhwa (KPK), Pakistan, by analyzing de-identified records from hospitals (June 2022–March 2025). We calculated body mass index (BMI) and classified patients by WHO Asian criteria: normal (18.5–22.9), overweight (23.0–27.4), and obese (≥27.5 kg/m2). We recorded hypertension (HTN), coronary artery disease (CAD), myocardial infarction (MI), and arrhythmia, and applied statistical tests (ANOVA, logistic regression) to derive odds ratios (OR) with 95% confidence intervals (CI). Results: Mean age was 39.8 years (SD 5.7); 48% were female; 200 were normal-weight, 178 overweight, and 122 obese. Hypertension was present in 20.0%, 39.9%, and 58.2% of the normal, overweight, and obese participants (pConclusion: Excess body weight is a major problem directly linked to high blood pressure and serious heart conditions, reflecting a global pattern. Preventing obesity should be a priority to reduce the growing heart disease burden in the region.
VL - 9
IS - 2
ER -
Shah, S. S., Rehman, A. U., Khan, Z., Ali, M., Ahmad, A., et al. (2025). Weight and Cardiac Health in Middle Aged People in Khyber Pakhtunkhwa, Pakistan. Pathology and Laboratory Medicine, 9(2), 49-55. https://doi.org/10.11648/j.plm.20250902.12
Shah, S. S.; Rehman, A. U.; Khan, Z.; Ali, M.; Ahmad, A., et al. Weight and Cardiac Health in Middle Aged People in Khyber Pakhtunkhwa, Pakistan. Pathol. Lab. Med.2025, 9(2), 49-55. doi: 10.11648/j.plm.20250902.12
Shah SS, Rehman AU, Khan Z, Ali M, Ahmad A, et al. Weight and Cardiac Health in Middle Aged People in Khyber Pakhtunkhwa, Pakistan. Pathol Lab Med. 2025;9(2):49-55. doi: 10.11648/j.plm.20250902.12
@article{10.11648/j.plm.20250902.12,
author = {Syed Sardar Shah and Attiq Ur Rehman and Ziad Khan and Mohsin Ali and Aftab Ahmad and Shah Nawaz and Saleem Jan and Syed Shayan Ahmad and Rizwan Ullah and Kashif Rasool and Shayan Ali Yousafzai and Shahid Bacha},
title = {Weight and Cardiac Health in Middle Aged People in Khyber Pakhtunkhwa, Pakistan
},
journal = {Pathology and Laboratory Medicine},
volume = {9},
number = {2},
pages = {49-55},
doi = {10.11648/j.plm.20250902.12},
url = {https://doi.org/10.11648/j.plm.20250902.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.plm.20250902.12},
abstract = {Method: We examined how body weight affects cardiovascular health in adults aged 30–50 in Khyber Pakhtunkhwa (KPK), Pakistan, by analyzing de-identified records from hospitals (June 2022–March 2025). We calculated body mass index (BMI) and classified patients by WHO Asian criteria: normal (18.5–22.9), overweight (23.0–27.4), and obese (≥27.5 kg/m2). We recorded hypertension (HTN), coronary artery disease (CAD), myocardial infarction (MI), and arrhythmia, and applied statistical tests (ANOVA, logistic regression) to derive odds ratios (OR) with 95% confidence intervals (CI). Results: Mean age was 39.8 years (SD 5.7); 48% were female; 200 were normal-weight, 178 overweight, and 122 obese. Hypertension was present in 20.0%, 39.9%, and 58.2% of the normal, overweight, and obese participants (pConclusion: Excess body weight is a major problem directly linked to high blood pressure and serious heart conditions, reflecting a global pattern. Preventing obesity should be a priority to reduce the growing heart disease burden in the region.
},
year = {2025}
}
TY - JOUR
T1 - Weight and Cardiac Health in Middle Aged People in Khyber Pakhtunkhwa, Pakistan
AU - Syed Sardar Shah
AU - Attiq Ur Rehman
AU - Ziad Khan
AU - Mohsin Ali
AU - Aftab Ahmad
AU - Shah Nawaz
AU - Saleem Jan
AU - Syed Shayan Ahmad
AU - Rizwan Ullah
AU - Kashif Rasool
AU - Shayan Ali Yousafzai
AU - Shahid Bacha
Y1 - 2025/10/22
PY - 2025
N1 - https://doi.org/10.11648/j.plm.20250902.12
DO - 10.11648/j.plm.20250902.12
T2 - Pathology and Laboratory Medicine
JF - Pathology and Laboratory Medicine
JO - Pathology and Laboratory Medicine
SP - 49
EP - 55
PB - Science Publishing Group
SN - 2640-4478
UR - https://doi.org/10.11648/j.plm.20250902.12
AB - Method: We examined how body weight affects cardiovascular health in adults aged 30–50 in Khyber Pakhtunkhwa (KPK), Pakistan, by analyzing de-identified records from hospitals (June 2022–March 2025). We calculated body mass index (BMI) and classified patients by WHO Asian criteria: normal (18.5–22.9), overweight (23.0–27.4), and obese (≥27.5 kg/m2). We recorded hypertension (HTN), coronary artery disease (CAD), myocardial infarction (MI), and arrhythmia, and applied statistical tests (ANOVA, logistic regression) to derive odds ratios (OR) with 95% confidence intervals (CI). Results: Mean age was 39.8 years (SD 5.7); 48% were female; 200 were normal-weight, 178 overweight, and 122 obese. Hypertension was present in 20.0%, 39.9%, and 58.2% of the normal, overweight, and obese participants (pConclusion: Excess body weight is a major problem directly linked to high blood pressure and serious heart conditions, reflecting a global pattern. Preventing obesity should be a priority to reduce the growing heart disease burden in the region.
VL - 9
IS - 2
ER -