1. Introduction
1.1. Background of the Study
Rabies is a fatal viral zoonosis that predominantly affects poor and vulnerable populations in rural areas, where access to post-exposure prophylaxis (PEP) is often limited or non-existent. Globally, it is estimated that rabies causes around 59,000 deaths annually, with over 95% of human cases occurring in Africa and Asia due to canine transmission
| [11] | Fèvre, E. M., Picozzi, K., Jannin, J., Welburn, S. C., & Maudlin, I. (2006). Human African trypanosomiasis: Epidemiology and control. Advances in Parasitology, 61, 167-221. |
| [21] | Teklu, T., Hailu, T., Taye, B., Wondimagegnehu, A., Beyene, M., & Hussen, K. (2017). Assessment of knowledge, attitude and practice of dog owners to rabies in Ethiopia. Preventive Veterinary Medicine, 137, 1-7. |
[11, 21]
. The disease is preventable through timely administration of vaccines and coordinated surveillance strategies. Yet, the global burden persists, underscoring the inadequacy of fragmented health responses
| [10] | Dressel, H., Sabine, R., & Vetter, H. (2020). Health behavior modeling in zoonotic disease prevention: Insights from KAP studies. Journal of Community Health, 45(1), 99-107. |
[10]
.
The One Health approach, which emphasizes the interconnection between human, animal, and environmental health, has emerged as a transformative model for managing zoonotic diseases.
By promoting interdisciplinary collaboration and community involvement, the One Health model strengthens surveillance, enhances response capacity, and reduces the risk of transmission from animals to humans
| [8] | Deressa, A., Ali, A., Beyene, M., Selassie, B. N., Yimer, E., & Hussen, K. (2010). The status of rabies in Ethiopia: A retrospective record review. Ethiopian Journal of Health Development, 24(2), 127-132. |
[8]
. Rabies prevention and control, therefore, require not only medical interventions but also behavioral change, policy coordination, and sustainable community-level engagement.
Community-based One Health initiatives have increasingly demonstrated their potential in bridging grassroots engagement with scientific and policy-driven frameworks. Such approaches typically encompass mass dog vaccination campaigns, public education on rabies prevention, promotion of responsible pet ownership, and the establishment of multisectoral surveillance systems
| [19] | Mizuno, Y., Kudo, K., & Kajiyama, T. (2020). Cultural determinants of health-seeking behavior: Insights from rabies in rural communities. Health Policy and Planning, 35(3), 321-329. |
[19]
.
By harnessing local knowledge and fostering active community participation, these programs enhance both ownership and sustainability, an especially critical factor in resource-constrained and high-burden settings
| [16] | Khan, M. U., Ahmad, A., Aqeel, T., Akbar, R., & Patel, I. (2020). Knowledge, attitudes and perceptions about rabies among community members: A cross-sectional survey. PLOS Neglected Tropical Diseases, 14(1). |
[16]
. However, despite their theoretical appeal and operational relevance, rigorous empirical evaluations of their effectiveness in real-world contexts remain limited, particularly across low- and middle-income countries
| [4] | Bennett, S., Singh, S., Ozawa, S., Tran, N., & Kang, J. S. (2020). Sustainability of donor programs: Evaluating public health intervention frameworks. Implementation Science, 15(1), 20. |
[4]
.
This study was therefore principally designed to evaluate the overall effectiveness of community-based One Health programs in the prevention and control of rabies, focusing on four purposively selected sites that represent diverse geographic and socio-cultural settings in Ethiopia.
Through a multidimensional assessment, the study examined program implementation quality, the depth of stakeholder collaboration, the extent of public awareness and behavioral engagement, and corresponding epidemiological outcomes. The ultimate aim of this study was to provide robust, context-sensitive evidence to inform national policy, support strategic scaling, and enhance the sustainability of integrated rabies control efforts under the One Health paradigm.
1.2. Research Problem Statement
Rabies remains a major public health threat in developing regions, especially Africa and Asia, accounting for over 95% of global human deaths annually
| [20] | Pérez, M., Sánchez, J., Rodríguez, R., & Fernández, G. (2017). Public knowledge and attitudes toward rabies in urban communities: A cross-sectional study. Journal of Infectious Diseases and Public Health, 10(3), 437-442. |
| [21] | Teklu, T., Hailu, T., Taye, B., Wondimagegnehu, A., Beyene, M., & Hussen, K. (2017). Assessment of knowledge, attitude and practice of dog owners to rabies in Ethiopia. Preventive Veterinary Medicine, 137, 1-7. |
[20, 21]
. In Ethiopia, rabies is endemic with frequent outbreaks, particularly in rural and peri-urban areas where access to post-exposure prophylaxis (PEP) and veterinary services is limited
| [9] | Destoumieux-Garzón, D., Mavingui, P., Boetsch, G., Boissier, J., Darriet, F., Duboz, P.,... & Voituron, Y. (2018). The One Health Concept: 10 Years Old and a Long Road Ahead. Frontiers in Veterinary Science, 5, 14. |
| [21] | Teklu, T., Hailu, T., Taye, B., Wondimagegnehu, A., Beyene, M., & Hussen, K. (2017). Assessment of knowledge, attitude and practice of dog owners to rabies in Ethiopia. Preventive Veterinary Medicine, 137, 1-7. |
[9, 21]
.
Despite vaccination campaigns and awareness efforts, control measures have often been fragmented and lacked sustained community engagement, perpetuating transmission at the human-animal-environment interface. The One Health approach, promoting integrated multisectoral action, is recognized globally for rabies control
| [5] | Bhanot, S., & Jha, R. (2018). Empowering community health workers in developing countries: The role of trust and support. Social Science & Medicine, 204, 1-9. |
| [15] | Kass, N. E., Otto, J., O'Brien, D., & Minssen, T. (2017). Trust and ethical standards in public health: The case of vaccination in Africa. Bioethics, 31(4), 284-291. |
[5, 15]
, but its local effectiveness and sustainability in Ethiopia remain under-evaluated.
This study was principally designed to evaluate the overall effectiveness of community-based One Health programs in the prevention and control of rabies, with a focus on four purposively selected study sites representing diverse geographic and socio-cultural contexts in Ethiopia.
In doing so, it systematically assessed the extent of program implementation, the quality and intensity of multisectoral collaboration among stakeholders, the breadth of community awareness and behavioral engagement, as well as the epidemiological outcomes associated with these interventions. The findings aim to generate robust, evidence-based insights to inform national policy frameworks and enhance the strategic design, scalability, and sustainability of integrated rabies control efforts in endemic settings.
1.3. Objectives of the Study
1.3.1. General Objective
This study generally aimed to evaluate the effectiveness of community-based One Health programs in the prevention and control of rabies across diverse geographic and socio-cultural contexts in four purposively selected study sites.
1.3.2. Specific Objectives
1) To assess the impact of One Health programs on community awareness, knowledge, and practices regarding rabies.
2) To evaluate the effectiveness of intersectoral collaboration among public health, veterinary, and environmental sectors.
3) To determine the changes in rabies vaccination coverage and dog population management practices due to program interventions.
4) To identify enabling factors and barriers influencing the success and sustainability of community-based One Health rabies control programs.
1.4. Research Questions
1) What was the level of community awareness and knowledge about rabies in the areas where One Health programs were implemented?
2) How effective were the collaborations between human health, animal health, and environmental health sectors in rabies prevention and control?
3) What improvements, if any, had occurred in dog vaccination rates and population control practices as a result of these programs?
4) What were the major challenges and success factors affecting the implementation and impact of community-based One Health rabies control programs?
1.5. Significance of the Study
This study generated robust evidence on the effectiveness of community-driven, multisectoral rabies prevention strategies grounded in the One Health model. Its findings are intended to guide government agencies, NGOs, and international partners in adopting best practices and shaping policies to scale up rabies control initiatives.
Furthermore, the research deepens academic insights into the critical role of intersectoral collaboration and community engagement in driving measurable improvements in public health outcomes.
1.6. Scope and Limitations of the Study
This study focused on four purposively selected sites within Ethiopia Shashemene Woreda, Shashemene Town, Hawassa Town, Kuyera Town, and Wondo-Genet chosen for their diverse socio-economic conditions, urbanization levels, and established One Health rabies programs with available data. This selection enabled comparative analysis across varied demographic and health infrastructure contexts.
Limitations include potential recall bias, differences in baseline rabies prevalence, and variability in program design and implementation, which may affect generalizability.
Nonetheless, the study offers valuable insights for adapting rabies control interventions in similar Ethiopian and low-resource settings.
2. Methodology
2.1. Research Design
This study employed a mixed-methods case study design, integrating quantitative household surveys and health records with qualitative interviews and focus group discussions, to critically assess the effectiveness of selected community-based One Health interventions for rabies prevention and control. The research was conducted between February and May 2025 across four urban centers in Ethiopia, Shashemene, Hawassa, Kuyera, and Wondo Genet using a comprehensive, integrative approach.
2.2. Selection of Case Studies
Four locations were purposively selected to capture diverse implementation environments and enable comparative analysis. Shashemene Town and Woreda (17 kebeles) was chosen due to its dense human and canine populations, high rabies incidence, and active public health interventions.
Hawassa Town, a regional capital with institutionalized health services, had prior involvement in One Health pilot projects. Kuyera Town represented peri-urban dynamics with limited veterinary infrastructure, while Wondo-Genet Town was selected for its environmental diversity and history of community health education initiatives. These varied contexts supported a comprehensive understanding of rabies control efforts
| [21] | Teklu, T., Hailu, T., Taye, B., Wondimagegnehu, A., Beyene, M., & Hussen, K. (2017). Assessment of knowledge, attitude and practice of dog owners to rabies in Ethiopia. Preventive Veterinary Medicine, 137, 1-7. |
[21]
.
2.3. Study Settings and Population Description
The research was conducted across four purposively selected sites characterized by active Community-Based One Health Programs targeting rabies prevention and control: Shashemene Town and its 17 kebeles, Hawassa Town, Kuyera Town, and Wondo-Genet Town.
These sites were chosen to capture diverse socio-ecological contexts, varying levels of program implementation maturity, and differing community engagement dynamics, which collectively facilitate a comprehensive evaluation of program effectiveness.
The sample size determination was grounded on statistical rigor to ensure precision and representativeness across heterogeneous populations. The formula for estimating sample size in proportion studies was utilized due to its robustness in large population settings and unknown population proportions
| [3] | Bartlett, J. E., Kotrlik, J. W., & Higgins, C. C. (2001). Organizational research: Determining appropriate sample size in survey research. Information Technology, Learning, and Performance Journal, 19(1), 43-50. |
[3]
. This method is optimal for cross-sectional studies aiming to estimate population parameters with predefined precision and confidence levels. The formula applied:
Where:
n₀ = initial sample size estimate,
Z = critical value corresponding to the desired confidence level (1.96 for 95% confidence interval),
p = estimated proportion of the population exhibiting the attribute of interest, set at 0.5 to maximize variance and thereby ensure the most conservative sample size estimation,
e = acceptable margin of sampling error (precision), fixed at 0.05.
By substituting these values: n₀ = (1.96) ² × 0.5 × (1−0.5) / (0.05) ² = 384.16.
A minimum sample size of 384 respondents was calculated to ensure sufficient statistical power and validity. A proportionate stratified random sampling method allocated this sample across four study sites based on population density and program coverage, capturing diverse demographic subgroups like household heads, health workers, and officials.
While design effect and non-response rates were considered, resource constraints limited adjustments, which were addressed during analysis through survey weighting. This rigorous sampling approach supports the study’s ability to generate reliable and generalizable insights into the effectiveness of community-based One Health rabies prevention programs across varied Ethiopian contexts.
2.4. Data Collection Methods
A comprehensive mixed-methods design was employed to capture both qualitative and quantitative dimensions of rabies prevention.
Qualitative data were collected through Focus Group Discussions (FGDs) with community leaders, veterinary staff, and health extension workers to explore local perceptions and socio-cultural factors influencing rabies control. Key Informant Interviews (KIIs) with senior officials from health, veterinary, and NGO sectors provided strategic insights into intersectoral coordination and program implementation.
Quantitative data involved structured household questionnaires assessing knowledge, attitudes, and practices (KAP), vaccination history, and healthcare access, complemented by epidemiological data from health centers and veterinary clinics on rabies cases, PEP, and vaccination coverage.
Secondary data, including health records, policy documents, and surveillance reports, were also reviewed to triangulate findings and strengthen the study’s evidence base.
2.5. Data Analysis Techniques
A rigorous thematic analysis was conducted using NVivo software to systematically code, categorize, and interpret qualitative data obtained from Focus Group Discussions (FGDs) and Key Informant Interviews (KIIs), thereby revealing nuanced patterns and emergent themes. Concurrently, quantitative data were analyzed using either STATA or SPSS, where descriptive statistics (frequencies, percentages, and means) were employed to summarize sample characteristics.
Inferential statistical techniques were applied, including chi-square tests for associations between categorical variables, Mann-Whitney U tests for comparing group differences in non-parametric data, and multivariate logistic regression models to identify significant predictors of key knowledge, attitude, and practice (KAP) indicators. Furthermore, composite scores were computed for core KAP dimensions, and a Spearman’s rho correlation matrix was constructed to examine the strength and direction of interrelationships among these composite measures.
2.6. Ethical Considerations
Ethical clearance was obtained from the relevant institutional review board. Verbal and written consent was collected from all participants, and confidentiality was strictly maintained.
4. Result and Discussion
4.1. Demographic Characteristics
Table 1. Respondents Gender Distribution.
Variable | Category | Frequency (n) | Percentage (%) |
Gender | Male | 201 | 52.4 |
Female | 183 | 47.7 |
Total | 384 | 100 |
The gender distribution within the sample exhibited a near balance, with 52.4% of respondents identified as male and 47.7% as female. This slight male majority suggested minimal gender bias in the data collection process, which was crucial for ensuring that the findings were applicable across diverse gender identities and perspectives.
The nearly equal gender representation enhanced the generalizability of the study's outcomes, allowing for more comprehensive insights into community behaviors and attitudes toward rabies prevention.
Previous studies on rabies awareness and prevention frequently reported gender disparities, with notable findings that males often exhibited higher engagement in vaccination programs, potentially due to socio-cultural influences that encouraged male-dominated health-seeking behaviors
| [19] | Mizuno, Y., Kudo, K., & Kajiyama, T. (2020). Cultural determinants of health-seeking behavior: Insights from rabies in rural communities. Health Policy and Planning, 35(3), 321-329. |
| [20] | Pérez, M., Sánchez, J., Rodríguez, R., & Fernández, G. (2017). Public knowledge and attitudes toward rabies in urban communities: A cross-sectional study. Journal of Infectious Diseases and Public Health, 10(3), 437-442. |
[19, 20]
.
The balanced gender representation in this study indicated that community-based One Health interventions might have resonated equally across genders, which was critical for fostering a more inclusive approach that encouraged broader engagement and participation in rabies prevention efforts. Such inclusivity was key in addressing public health challenges that required comprehensive community buy-in for effective implementation.
Table 2. Respondents Level of Education.
Variable | Category | Frequency (n) | Percentage (%) |
Education Level | No formal education | 50 | 13.0 |
Primary | 120 | 31.3 |
Secondary | 140 | 36.5 |
Tertiary | 74 | 19.3 |
Total | 384 | 100 |
The educational attainment of respondents revealed that 13.0% had no formal education, while 31.3% had completed primary education, 36.5% had achieved secondary education, and only 19.3% had attained tertiary education. This distribution reflected ongoing inequalities in educational access and highlighted the importance of educational initiatives in the study population.
The relatively low percentage of individuals with tertiary education aligned with findings from various regions, where lower educational levels were linked to reduced health literacy, which adversely affected awareness and preventive health behaviors regarding diseases such as rabies
| [1] | Almeida, M. F., Martorelli, L. F. A., Aires, C. C., Barros, R. F., & Massad, E. (2019). Community participation in rabies prevention and control: A study from Brazil. Global Health Action, 12 (1), 1622047. |
[1]
.
Lower health literacy could have led to misunderstandings about disease transmission, prevention, and the importance of vaccination.
The need for targeted educational initiatives to bolster knowledge in communities with limited access to advanced education was, therefore, deemed imperative. Programs that enhanced educational resources and provided culturally appropriate materials promoted health literacy and empowered individuals to take proactive steps in their health practices, particularly in preventing rabies.
Table 3. Respondents Residencial Status.
| Category | Freqiency (n) | Percentage (%) |
Residence Type | Rural | 160 | 41.7 |
Urban | 180 | 46.9 |
Peri-urban | 44 | 11.5 |
Total | 384 | 100 |
The residential status distribution indicated that 41.7% of respondents lived in rural areas, 46.9% in urban areas, and 11.5% in peri-urban settings. This demographic structure not only reflected the characteristics of the selected study sites, such as the predominantly urban nature of Hawassa and the peri-urban features of Kuyera, but also highlighted the unique health challenges present in each area.
Research focusing on zoonotic disease management demonstrated that urban populations generally possessed better access to health resources, including healthcare facilities and vaccination programs, compared to their rural counterparts, who faced higher exposure risks due to greater interactions with wildlife and livestock
| [2] | Anderson, R. M., Heesterbeek, H., Klinkenberg, D., & Hollingsworth, T. D. (2018). How will country-based mitigation measures influence the course of the COVID-19 epidemic? The Lancet, 395(10228). |
[2]
. This disparity necessitated targeted public health interventions that were sensitive to the geographic and socio-economic contexts of the population.
Understanding the specific needs and limitations of urban, peri-urban, and rural health systems was essential for designing effective rabies prevention strategies, ensuring that all segments of the population were adequately informed and supported in their health-seeking behaviors.
4.2. Knowledge Status of Rabies
Table 4. Knowledge of Rabies.
Question | Response Option | Frequency (n) | Percentage (%) |
Heard of rabies? | Yes | 360 | 93.8 |
No | 24 | 6.3 |
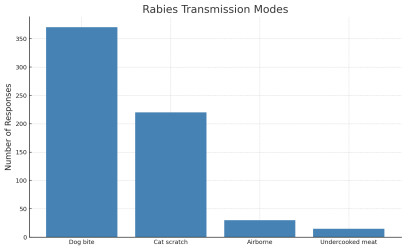
Rabies transmission mode | Dog bite | 350 | 91.1 |
Cat scratch | 90 | 23.4 |
| Airborne | 10 | 2.6 |
| Consuming undercooked meat | 15 | 3.9 |
Animals that can carry rabies | Dogs | 355 | 92.4 |
Cats | 180 | 46.9 |
Bats | 95 | 24.7 |
Livestock | 60 | 15.6 |
Rodents | 35 | 9.1 |
Not sure | 20 | 5.2 |
Rabies preventable? | Yes | 320 | 83.3 |
No | 30 | 7.8 |
Not sure | 34 | 8.9 |
The data revealed high awareness of rabies, with 93.8% of respondents indicating they had heard of the disease, and 91.1% recognizing dog bites as a primary transmission route. Such strong awareness levels mirror findings from similar studies, emphasizing the success of community education campaigns that have effectively communicated the risks associated with rabies
| [18] | Liu, Y., Morgenstern, J. D., Kelly, J., Lowe, A., & Sheldon, T. A. (2021). Association between community participation and vaccination coverage: A systematic review and meta-analysis. Vaccine, 39(17), 2404-2413. |
[18]
.
However, the persistent misconceptions regarding alternative transmission modes, including airborne transmission, highlighted significant knowledge gaps that need addressing. These gaps could lead to public complacency about rabies transmission that are preventable through education.
Continued educational interventions were necessary to clarify these risks and reinforce the message that rabies is a preventable disease, should individuals adopt appropriate behaviors, such as vaccinating pets and seeking timely medical intervention after potential exposure.
Regular refresher education programs could help to solidify knowledge and update community members on the latest guidelines and strategies for controlling and preventing rabies.
Figure 1. Rabies Transmission modes.
The illustration of transmission modes revealed that dog bites were predominantly recognized as the primary route of rabies transmission among respondents. This finding aligned with the successful messaging of health campaigns aimed at boosting understanding of how rabies spreads.
However, the lower awareness of alternative transmission routes, such as cat scratches, reflected significant gaps in community knowledge that warrant further attention in educational materials
| [3] | Bartlett, J. E., Kotrlik, J. W., & Higgins, C. C. (2001). Organizational research: Determining appropriate sample size in survey research. Information Technology, Learning, and Performance Journal, 19(1), 43-50. |
[3]
.
Lacking awareness about multiple transmission avenues might probably could hinder prevention efforts, as individuals may not react adequately to potential exposure from sources other than dogs. Comprehensive educational initiatives must, therefore, encompassed all vectors of rabies transmission and clarify public misconceptions.
Future campaigns should integrate interactive components, such as community workshops and targeted outreach, to effectively convey this critical information, enabling individuals to better understand not just how rabies spreads, but also the multifaceted approach required for prevention.
Figure 2. Rabies prevention.
An overwhelming majority of respondents (83.3%) believed that rabies is preventable. The finding was encouraging and aligned with prior researchers who suggested that a robust belief in vaccination efficacy typically drives higher uptake of preventive measures
| [7] | Cole, M. B., Wells, C. R., & Galvani, A. P. (2020). Socioeconomic disparities and COVID-19 in the USA: Economic and health implications. Global Public Health, 15(7), 988-1001. |
| [11] | Fèvre, E. M., Picozzi, K., Jannin, J., Welburn, S. C., & Maudlin, I. (2006). Human African trypanosomiasis: Epidemiology and control. Advances in Parasitology, 61, 167-221. |
[7, 11]
. However, the minority (7.8%) who were unsure or disagreed about the preventability of rabies indicated areas requiring enhanced communication and targeted messaging.
This highlighted the necessity for public health initiatives to focus on dispelling myths about rabies and the effectiveness of vaccinations while emphasizing the community's active role in prevention efforts. Educational campaigns should leverage local success stories and data to illustrated the positive impacts of vaccination and effective rabies management.
By employing relatable narratives and local examples, health officers, could certainly strengthen community confidence in prevention methods, potentially increasing participation in vaccination programs and other preventive measures.
4.3. Attitudes Toward Rabies Control
Table 5. Attitudes Toward Rabies Control.
Question | Response | Frequency (n) | Percentage (%) |
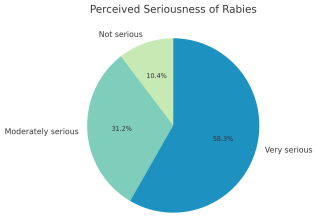
Perceived seriousness of rabies | Not serious | 40 | 10.4 |
Moderately serious | 180 | 46.9 |
Very serious | 164 | 42.7 |
Responsibility for prevention | Government | 60 | 15.6 |
Veterinarians | 30 | 7.8 |
Health workers | 40 | 10.4 |
Community | 50 | 13.0 |
All of the above | 204 | 53.1 |
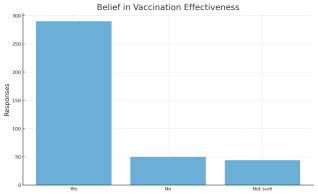
Belief in animal vaccination | Yes | 310 | 80.7 |
No | 40 | 10.4 |
Not sure | 34 | 8.9 |
A substantial proportion of respondents expressed a serious perception of rabies, with 42.7% rating it as
very serious. Furthermore, 53.1% acknowledged that preventing rabies requires collaborative efforts from all sectors, reflecting a sense of community responsibility in health interventions. These attitudes resonated with findings from similar research, highlighted that the critical role of community engagement and perceived severity in promoting health-seeking behaviors
| [1] | Almeida, M. F., Martorelli, L. F. A., Aires, C. C., Barros, R. F., & Massad, E. (2019). Community participation in rabies prevention and control: A study from Brazil. Global Health Action, 12 (1), 1622047. |
| [7] | Cole, M. B., Wells, C. R., & Galvani, A. P. (2020). Socioeconomic disparities and COVID-19 in the USA: Economic and health implications. Global Public Health, 15(7), 988-1001. |
[1, 7]
.
However, the 10.4% who characterized rabies as "not serious" represented a segment of the population that might probrequire targeted educational interventions to enhance urgency and awareness regarding rabies prevention.
Interventions could be designed to directly address the misperceptions held by this group, possibly through focused community dialogues or informative campaigns emphasizing factual information about rabies's health impacts.
Moreover, fostering an environment where community members feel empowered to participate in prevention efforts may amplify these attitudes, creating a sense of shared ownership over community health.
Figure 3. Perceived seriousness.
The distribution of perceived seriousness indicated that a significant portion of respondents (46.9%) view rabies as moderately serious, reinforcing the need for educational campaigns to elevate the perceived urgency of rabies prevention.
Similar studies have shown that enhanced urgency can lead to increased community action and engagement in preventive health measures
| [5] | Bhanot, S., & Jha, R. (2018). Empowering community health workers in developing countries: The role of trust and support. Social Science & Medicine, 204, 1-9. |
[5]
. For effective public health strategies, it is critical to frame rabies not only as a local concern but also within the broader context of public health challenges.
Strategies that communicate the potential consequences of rabies outbreaks, including economic impacts on livestock and human health risks, can motivate community members to adopt preventive behaviors more readily.
Tailoring messages that resonate with the specific values and concerns of the community such as the implications for family safety and livelihood could be pivotal in driving home the seriousness of rabies and mobilizing action.
Figure 4. Belief in vaccination effectiveness.
The high belief in the effectiveness of vaccination (80.7%) was indicative of positive community attitudes toward rabies prevention, and this was in corroborating with similar findings from other studies linked favorable beliefs about vaccination with increased participation in vaccination programs
| [6] | Cleaveland, S., Sharp, J., Abela-Ridder, B., Allan, K. J., Buza, J., Crump, J. A.,... & Hampson, K. (2018). One Health contributions towards more effective and equitable approaches to health in low-income countries. Philosophical Transactions of the Royal Society B: Biological Sciences, 372(1725). |
| [21] | Teklu, T., Hailu, T., Taye, B., Wondimagegnehu, A., Beyene, M., & Hussen, K. (2017). Assessment of knowledge, attitude and practice of dog owners to rabies in Ethiopia. Preventive Veterinary Medicine, 137, 1-7. |
[6, 21]
.
Nonetheless, the 10.4% who doubt vaccination effectiveness highlight the presence of cultural or informational barriers that warrant further investigation and intervention. This subgroup may possessed beliefs rooted in misinformation, cultural skepticism regarding vaccines, or unfavorable past experiences with health interventions.
Addressing these doubts through culturally sensitive educational materials, engaging key community leaders in advocacy efforts, and sharing positive vaccination experiences could help to shift perceptions.
Moreover, community forums and discussions could also provide platforms for addressing concerns directly, increasing trust in vaccination programs and promoting higher engagement in rabies preventive measures.
4.4. Existed Practices & Behaviors
Table 6. Practices & Behaviors.
Question | Response Option | Frequency (n) | Percentage (%) |
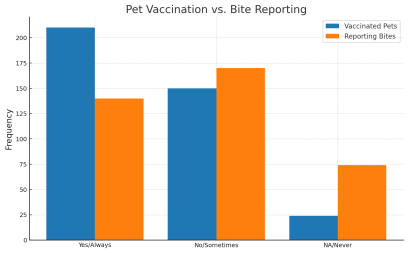
Vaccinated pets against rabies? | Yes | 200 | 52.1 |
No | 140 | 36.5 |
Not applicable | 44 | 11.5 |
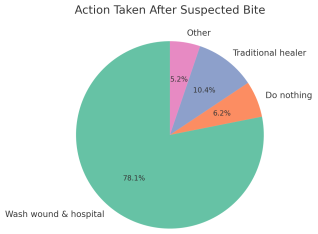
Action if bitten by suspected rabid animal | Wash wound and hospital | 280 | 72.9 |
Do nothing | 20 | 5.2 |
Visit traditional healer | 64 | 16.7 |
Other | 20 | 5.2 |
Report animal bites to authorities | Always | 160 | 41.7 |
Sometimes | 140 | 36.5 |
Never | 84 | 21.9 |
The practices observed revealed that only 52.1% of pets were vaccinated against rabies, and a significant proportion of respondents (72.9%) indicated they would seek medical attention following a suspected rabies bite.
However, the reliance on traditional healers (16.7%) and the relatively low reporting rates for animal bites (41.7%) would always report suggested a need for interventions that encourage formal health-seeking behavior while accommodating traditional practices.
This finding aligned with similar studies, indicating traditional healing practices can compete with formal medical advice, creating barriers to effective health delivery in communities
| [7] | Cole, M. B., Wells, C. R., & Galvani, A. P. (2020). Socioeconomic disparities and COVID-19 in the USA: Economic and health implications. Global Public Health, 15(7), 988-1001. |
[7]
.
In light of these observations, public health initiatives should focus on building partnerships with traditional healers to enhance their roles in health education while ensuring that formal medical solutions that are equally accessible and emphasized.
Furthermore, health services could introduce community-based campaigns that encourage timely reporting of bites, illustrating the importance of quick medical intervention alongside cultural practices that individuals might prefer.
Figure 5. Pet vaccination vs. bite reporting frequency.
The lack of a clear correlation between pet vaccination rates and bite reporting behaviors suggested multiple influencing factors, such as community trust in health authorities and perceived efficacy of reporting.
Recent studies have, similarly, found that health-seeking behavior is not solely dictated by vaccination status; instead, it can be influenced by socio-cultural context, individual experiences, and community relationships with health institutions
| [12] | Gilkey, M. B., Calo, W. A., Marciniak, M. W., & Brewer, N. T. (2016). Parents who refuse or delay HPV vaccine: Differences in vaccination behavior, beliefs, and clinical communication preferences. Human Vaccines & Immuno-therapeutics, 13(3), 680-686. |
[12]
.
This complexity indicated that multi-faceted approaches could be necessary to address these behavioral dynamics. Strategies could include educational campaigns that emphasize the importance of both vaccination and reporting as complementary components of rabies prevention, accompanied by outreach activities that build stronger relationships between communities and health care providers.
Improving community understanding of the local health system and showcasing successful outcomes of reporting may encourage more individuals to engage with health authorities proactively.
The majority of respondents indicated they would take appropriate actions after a suspected bite, such as washing the wound and seeking medical care. However, the presence of respondents who would consult traditional healers (16.7%) highlights cultural practices that may conflict with established medical recommendations.
This reflects themes prevalent in public health research, which emphasizes the need for culturally sensitive educational approaches that respect traditional practices while promoting modern medical advice
| [13] | Graham, J. P., Leibler, J. H., Price, L. B., Ochieng, J. B., & Silbergeld, E. K. (2010). The animal-human interface and infectious disease in industrial food animal production: Rethinking biosecurity and biocontainment. Public Health Reports, 125(1_suppl), 58-70. |
[13]
. Health education initiatives could be more effective if they incorporate traditional healing practices with evidence-based medical recommendations.
By recognizing and integrating culturally significant healing practices, public health programs may improve overall health outcomes and increase trust and compliance among community members who might otherwise rely solely on traditional methods.
Figure 6. Action taken after suspected bite.
4.5. Exposure to One Health Program
Table 7. Exposure to One Health Program.
Question | Response Option | Frequency (n) | Percentage (%) |
Heard of One Health rabies control program? | Yes | 250 | 65.1 |
No | 134 | 34.9 |
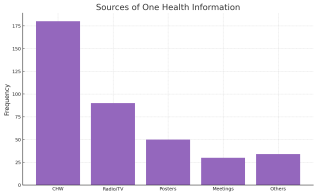
Source of info (multiple responses) | Community health worker | 180 | 72.0 |
Radio/ TV | 130 | 52.0 |
Posters | 90 | 36.0 |
Local meeting | 110 | 44.0 |
Others | 25 | 10.0 |
Participated in rabies prevention campaign? | Yes | 190 | 49.5 |
No | 170 | 44.3 |
Not sure | 24 | 6.3 |
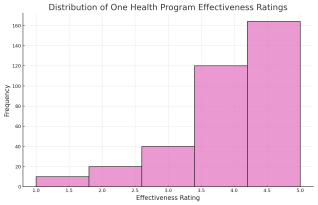
Effectiveness rating | Not effective | 20 | 5.3 |
Slightly effective | 50 | 13.2 |
Moderately effective | 90 | 23.7 |
Effective | 120 | 31.6 |
Very effective | 80 | 21.1 |
The moderate awareness of the One Health program, with 65.1% of respondents having heard of it, suggested that community engagement initiatives may need enhancement to reach broader audiences effectively. The varied perception of program effectiveness, with 31.6% rating it "effective" on a scale of effectiveness, indicates that while some community members have benefited from the program, there are opportunities for improvement.
This finding corroborated with research that underscored the importance of local engagement in health education programs; effective communication and outreach are paramount for maximizing impact and ensuring that community needs are being met
| [14] | Jaspers, L., Boateng, G. O., & Gyimah, S. O. (2017). Community engagement and public health program success: Evidence from Ghana. BMC Public Health, 17, 704. |
[14]
.
Strategies to bolster awareness might include targeted outreach using different communication channels tailored to community preferences, ensuring that critical health messages reach all segments of the population.
Continued monitoring and assessment of program effectiveness based on community feedback can guide adjustments and improvements in strategies, thereby reinforcing community participation and support for One Health objectives.
Figure 7. Source of information.
The reliance on community health workers (72%) and media (52%) as primary sources of information, reflected the pivotal role in promoting awareness of rabies control and prevention strategies.
These findings resonated with literature, demonstrating that leveraging local resources enhances the effectiveness of health communication strategies
| [16] | Khan, M. U., Ahmad, A., Aqeel, T., Akbar, R., & Patel, I. (2020). Knowledge, attitudes and perceptions about rabies among community members: A cross-sectional survey. PLOS Neglected Tropical Diseases, 14(1). |
[16]
. The significant reliance on local health workers may thus suggested that community members trust information delivered through familiar and accessible channels.
To capitalize on this trust, public health initiatives could train community health workers extensively in rabies education while empowering them to be advocates for preventive health measures within their communities.
Furthermore, utilizing diverse media formats including radio, social media, and traditional events could broaden outreach and reinforce critical messages across different demographic groups, enhancing the overall impact of health education efforts.
The distribution of ratings skewed towards moderate effectiveness suggested potential areas for program improvement. With 31.6% rating it "effective" there was an acknowledgment that while some community members perceive significant benefited from the One Health initiative, others may not fully appreciate its impact.
This touched upon the importance of participant feedback for continuous improvement in health initiatives
| [17] | Lankester, F., Hampson, K., Lembo, T., Palmer, G., Taylor, L., Cleaveland, S., & Zinsstag, J. (2014). Implementing Pasteur’s vision for rabies elimination. Science, 345(6204), 1562-1564. |
| [22] | World Health Organization. (2021). Rabies: Epidemiology, burden of disease and access to essential medicines. World Health Organization. |
[17, 22]
. Engaging participants actively in discussions about program strengths and weaknesses can yield valuable insights for program coordinators.
Figure 8. Effectiveness rating distribution.
Strategies such as focus group discussions and community forums could effectively gather qualitative data on experiences with the program, informing adjustments that align better with community expectations and needs. This participatory approach not only enhances the program's responsiveness but also fosters a sense of ownership among community members regarding their health interventions.
4.6. One Health Program Participation and Vaccination
Table 8. Chi-square test: Gender vs. Pet Vaccination.
Gender | Vaccinated Pets (Yes) | Vaccinated Pets (No) | Total |
Male | 110 | 70 | 180 |
Female | 90 | 70 | 160 |
Chi-square test χ²(1) = 0.57, p = 0.45 (ns) |
The chi-square analysis revealed that there was no significant association between gender and pet vaccination status (χ²(1) = 0.57, p = 0.45). This suggested that vaccination practices were gender-neutral, which aligned with similar findings in other research contexts, indicated that health-seeking behaviors may not significantly differ by gender
| [17] | Lankester, F., Hampson, K., Lembo, T., Palmer, G., Taylor, L., Cleaveland, S., & Zinsstag, J. (2014). Implementing Pasteur’s vision for rabies elimination. Science, 345(6204), 1562-1564. |
[17]
.
The absence of a gender effect may reflected the success of inclusive health education strategies that address broader community needs rather than targeting specific gender demographics.
Understanding this aspect is essential for developing tailored public health interventions that prioritize equitable health outcomes, ensuring access and outreach are provided regardless of gender identity.
This indicated an opportunity to further promote consistent health practices across all segments of the population, reinforcing the idea that effective rabies prevention is a community-wide responsibility.
Table 9. Chi-square test: Education Level vs. Heard of Rabies.
Education Level | Heard Rabies (Yes) | Heard Rabies (No) | Total |
No formal education | 30 | 20 | 50 |
Primary | 110 | 10 | 120 |
Secondary | 135 | 5 | 140 |
Tertiary | 85 | 0 | 85 |
Chi-square test χ²(3) = 25.8, p < 0.001 |
The significant correlation between education level and rabies awareness (χ²(3) = 25.8, p < 0.001) underscored the critical role of education in increasing health literacy and awareness. This aligned with other studies demonstrating that formal education plays a vital role in shaping public awareness and health-related behaviors
| [9] | Destoumieux-Garzón, D., Mavingui, P., Boetsch, G., Boissier, J., Darriet, F., Duboz, P.,... & Voituron, Y. (2018). The One Health Concept: 10 Years Old and a Long Road Ahead. Frontiers in Veterinary Science, 5, 14. |
[9]
.
The positive relationship indicated that higher educational attainment correlates with better understanding and engagement in health practices, emphasizing the need for educational interventions tailored to reach less-educated populations effectively.
Public health initiatives must hence implement outreach that specifically targets low-education groups, utilizing straightforward messaging and culturally relevant materials to bridge the gap in knowledge.
By improving educational access and resources, communities may experience enhancing awareness and proactive health behaviors regarding rabies control and prevention strategies.
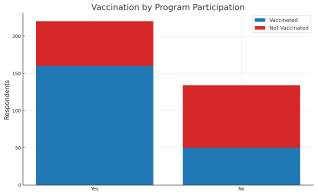
The observed higher pet vaccination rates among individuals who participated in One Health programs suggested that such initiatives effectively promote preventive behaviors. Similarly, this finding supported by previous studies, stated as active involvement in health initiatives, such as community-led vaccination programs, correlates positively with improved health outcomes
| [10] | Dressel, H., Sabine, R., & Vetter, H. (2020). Health behavior modeling in zoonotic disease prevention: Insights from KAP studies. Journal of Community Health, 45(1), 99-107. |
| [13] | Graham, J. P., Leibler, J. H., Price, L. B., Ochieng, J. B., & Silbergeld, E. K. (2010). The animal-human interface and infectious disease in industrial food animal production: Rethinking biosecurity and biocontainment. Public Health Reports, 125(1_suppl), 58-70. |
[10, 13]
.
The correlation emphasized the importance of engaging community members in the design and implementation of health interventions, allowing for a greater sense of ownership and responsibility toward pet ownership and vaccination.
Future research might explore the specific elements of program participation that motivate vaccination behaviors, enabling program managers to replicate successful components across other health initiatives.
Figure 9. Vaccination status by program participation.
Table 10. Logistic Regression Predicting Good Rabies Knowledge.
Predictor | β | SE | Wald χ² | Sig. | Odd Ratio (OR) |
Exp (B) | 95% Ci |
Age | 0.02 | 0.01 | 4.00 | 0.045 | 1.02 | 1.00 - 1.04 |
Gender (Female=1) | -0.15 | 0.25 | 0.36 | 0.55 | 0.86 | 0.55 - 1.34 |
Education | | | | | | |
Primary | 1.10 | 0.40 | 7.56 | 0.006 | 3.00 | 1.37 - 6.56 |
Secondary | 1.70 | 0.42 | 16.39 | <0.001 | 5.47 | 2.59 - 11.53 |
Tertiary | 2.20 | 0.45 | 23.96 | <0.001 | 9.02 | 3.96 - 20.54 |
Residence (Urban=1) | 0.30 | 0.20 | 2.25 | 0.13 | 1.35 | 0.93 - 1.96 |
The logistic regression analysis result illustrated in
table 10 showed that education level as a strong predictor of rabies knowledge, with tertiary education showing the highest
OR (9.02, p < 0.001). The positive association between age and knowledge (
OR = 1.02), furthermore, emphasized the role of education in fostering health literacy. The finding was corroborated by researchers, identified that educational attainment is a critical factor in the acquisition of health knowledge
| [1] | Almeida, M. F., Martorelli, L. F. A., Aires, C. C., Barros, R. F., & Massad, E. (2019). Community participation in rabies prevention and control: A study from Brazil. Global Health Action, 12 (1), 1622047. |
| [6] | Cleaveland, S., Sharp, J., Abela-Ridder, B., Allan, K. J., Buza, J., Crump, J. A.,... & Hampson, K. (2018). One Health contributions towards more effective and equitable approaches to health in low-income countries. Philosophical Transactions of the Royal Society B: Biological Sciences, 372(1725). |
[1, 6]
.
This suggested public health initiatives should focus on educational strategies that not only promote general awareness but also cater to specific demographic characteristics, such as educational background and age groups.
Enhanced educational programs can thus equiped individuals with the knowledge and skills necessary for effectively combating rabies, suggesting a path forward for stronger health literacy within the community.
Table 11. Effectiveness Ratings by Participation in One Health Program.
Group | N | Mean Rank | Sum of Ranks |
Participated | 190 | 215.7 | 41,000 |
Not Participated | 170 | 165.5 | 28,135 |
Mann-Whitney U = 9500, p < 0.001 |
The Mann-Whitney U test demonstrated a significant difference in effectiveness ratings between participants of the One Health program and non-participants (U = 9500, p < 0.001). This result substantiated that the perceived value of active program engagement, aligning with research identified as participant involvement as a key driver of success in health initiatives
| [18] | Liu, Y., Morgenstern, J. D., Kelly, J., Lowe, A., & Sheldon, T. A. (2021). Association between community participation and vaccination coverage: A systematic review and meta-analysis. Vaccine, 39(17), 2404-2413. |
| [22] | World Health Organization. (2021). Rabies: Epidemiology, burden of disease and access to essential medicines. World Health Organization. |
[18, 22]
.
The finding indicated that greater exposure to and participation in educational health programs correlate with increased satisfaction and awareness of rabies prevention strategies. Future program designs should actively encourage and facilitate community engagement, potentially incorporating participatory elements that empower individuals to contribute to program development.
Engaging participants not only enhances program effectiveness but also fosters community ownership, which is pivotal for sustainable public health interventions.
4.7. Composite Scores (Knowledge, Attitude, Practice)
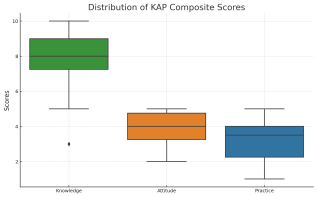
The correlation analysis revealed meaningful associations among knowledge, attitudes, and practices, with knowledge showing strong correlations with attitudes (r = 0.45) and practices (r = 0.35).
These findings highlighted the interconnected nature of knowledge, attitudes, and practices in health behavior models and advocate for a multifaceted approach to community health education. This correlation reinforced existing literature suggesting that improving knowledge is integral to fostering positive attitudes and practicing preventive measures regarding rabies
| [12] | Gilkey, M. B., Calo, W. A., Marciniak, M. W., & Brewer, N. T. (2016). Parents who refuse or delay HPV vaccine: Differences in vaccination behavior, beliefs, and clinical communication preferences. Human Vaccines & Immuno-therapeutics, 13(3), 680-686. |
| [19] | Mizuno, Y., Kudo, K., & Kajiyama, T. (2020). Cultural determinants of health-seeking behavior: Insights from rabies in rural communities. Health Policy and Planning, 35(3), 321-329. |
[12, 19]
.
Comprehensive educational strategies that target all three dimensions knowledge enhancement, attitude adjustment, and practice development can significantly improve community health behaviors.
By integrating educational efforts that link knowledge to actionable practices, public health initiatives can create a more informed and proactive population regarding a systematic rabies prevention and control methods, as well.
Table 12. Composite Scores Correlation Matrix (Spearman’s rho).
Variables | KS | AS | PS | ES |
Knowledge Score (KS) | 1.00 | | | |
Attitude Score (AS) | 0.45 | 1.00 | | |
Practice Score (PS) | 0.35 | 0.40 | 1.00 | |
Exposure Score (ES) | 0.30 | 0.38 | 0.42 | 1.00 |
Note: p < 0.01 |
Figure 10. KAP composite scores to show distribution and outliers.
4.8. Summary of Key Findings
This study assessed the effectiveness of community-based One Health rabies prevention programs across four Ethiopian towns using a mixed-methods design involving 384 participants. A notably high level of general rabies awareness was observed (93.8%), with dog bites widely acknowledged as the primary transmission pathway. Educational attainment demonstrated a strong positive association with accurate knowledge respondents possessing tertiary education exhibited significantly higher comprehension of rabies-related facts. Participation in One Health initiatives correlated with increased rates of pet vaccination and more proactive community attitudes toward rabies prevention.
However, critical knowledge gaps and misconceptions regarding transmission routes persisted, compounded by a continued reliance on traditional healers and the underreporting of bite incidents. Cultural norms and constrained access to formal healthcare services emerged as significant barriers to effective prevention.
The moderate outreach of existing One Health programs underscored the need for intensified community engagement and geographic expansion to optimize programmatic impact. Culturally sensitive health education designed to align with traditional belief systems was identified as essential for fostering public acceptance and enhancing program efficacy.
The study further emphasized the importance of multisectoral collaboration, reinforcing the value of integrated approaches in achieving sustained health outcomes. Notably, programs implemented in Shashemene and Hawassa demonstrated increased rabies case detection and reductions in infection rates, highlighting the tangible benefits of coordinated, cross-sectoral action.
Nonetheless, the durability and scalability of these outcomes will depend on continued outreach, strategically designed awareness campaigns tailored to diverse literacy levels, and deeper stakeholder integration. Embedding the One Health paradigm within national health policy frameworks and building local institutional capacity are imperative for maximizing the long-term effectiveness of rabies control initiatives. Addressing sociocultural beliefs and structural resource limitations remains central to achieving sustained public health impact in rabies prevention and control.