Abstract
Introduction: The WHO’s prompt declaration of a Public Health Emergency of International Concern (PHEIC) shepherded an effective coordinated response to contain the epidemic. Objective: The aim of this study is to describe the experiences, challenges, and lessons learned during the Implementation of Emergency Preparedness and Response-Rapid Response Team (EPR-RRT) program. Method: The study used mixed methods approach quantitative and qualitative data from a literature review of WHO AFRO coordination mechanisms and the Niger Public Health Emergency Operational Centre (PHEOC). The study was conducted in the National Public Health Emergency Operational Centre (PHEOC) of Niger during 12 months from September 2022 to September 2023. Results: The implementation of this program began with the evaluation of Niger's capacities and capacity building of teams to prepare, detect and respond to public health emergencies within 24 hours of an alert. The team of multi-disciplinary and multi-sector experts was identified and selected and trained on series of modules training. The team is composed of a total of 50 experts from 6 ONE HEALTH sectoral ministries. The average age is 49.94 (±5.9) years with extremes ranging from 33 to 56 years. The sex ratio is 0.35. The team have acquired the experience of being deployed in 4 regions of the country, 6 districts as part of the response to 6 public health events. Conclusion: The rapid response team has made it possible not only to acquire the technical and operational skills, financial, human and logistical capacities to respond rapidly when a public health emergency occurs.
Keywords
Emergency Preparedness and Response, Rapid Response Team, Niger
1. Introduction
Most countries in the WHO African region face a number of challenges related to the occurrence of public health events, but also to the coordination of responses to the various public health emergencies. The recent outbreak of COVID-19 clearly highlighted the need for a mechanism to coordinate the response to public health emergencies, both nationally and internationally.
Since 1997, the World Health Organization (WHO) has established a mechanism for outbreak detection, verification, and information sharing as part of global disease surveillance. With the entry into force of the International Health Regulations (2005) (IHR) in June 2007, WHO and States Parties committed to detect, verify, assess and report events that may pose a threat to global health security.
| [1] | OMS/Niger/ WHO/Niger. Mission de cadrage du programme SURGE « Renforcement et utilisation des groupes de riposte aux situations d’urgence au Niger ». https://niger.un.org/fr/173868-mission-de-cadrage-du-programme-surge-«-renforcement-et-utilisation-des-groupes-de-riposte |
| [2] | OMS/Niger/ WHO/Niger. Premier déploiement réussi de l’équipe SURGE pour contenir une épidémie de choléra. https://www.afro.who.int/fr/countries/niger/news/premier-deploiement-reussi-de-lequipe-surge-pour-contenir-une-epidemie-de-cholera |
| [3] | OMS/Niger/ WHO/Niger. Remise de certificat aux 50 experts SURGE dans l’urgence épidémiologique. https://www.afro.who.int/fr/countries/niger/news/remise-de-certificat-aux-50-experts-surge-dans-lurgence-epidemiologique |
| [4] | Ishata Nannie Conteh, Francis Chisaka Kasolo, Paul Olaiya Abiodun, Ebenezer Obi Daniel, Alhassan Fouard Kanu, Rashidatu Fouard Kamara, Aziza Amina Sahid, Olaniyi Felix Sanni, Aminata Tigiedankay Koroma, Josephine Amine Koroma, Lynda Foray-Rhall, Mukeh Kenneth Fahnbulleh, Charles Keimbe, Joseph Sam Kanu, Mohamed Vandy, Daniel Ganu. Public Health Emergency Preparedness and Response to Natural Disaster in Sierra Leone: The Milestone in a Decade. World Journal of Public Health. Vol. 8, No. 4, 2023, pp. 272-279. https://doi.org/10.11648/j.wjph.20230804.14 |
| [5] | Zinsou C, Guedegbe G, Dossou L, et al. Lessons learned in improving the quality of a free reproductive health hotline in Benin. Glob Health Sci Pract. 2023; 11(6): e2200296. https://doi.org/10.9745/GHSP-D-22-00296 |
[1-5]
Globally, in 2019, a total of 483 public health events were detected, recorded in the EMS, and monitored by WHO, of which 108 (22%) occurred in 35 IHR States Parties in the WHO African Region.
| [5] | Zinsou C, Guedegbe G, Dossou L, et al. Lessons learned in improving the quality of a free reproductive health hotline in Benin. Glob Health Sci Pract. 2023; 11(6): e2200296. https://doi.org/10.9745/GHSP-D-22-00296 |
| [6] | Pete Skelton, Flavio Salio & Nedret Emiroglu. Emergency preparedness and readiness; anticipating the need for rehabilitation, Bull World Health Organ 2022; 100: 744–746 http://dx.doi.org/10.2471/BLT.22.289085 |
| [7] | Aliyu A. Management of disasters and complex emergencies in Africa: The challenges and constraints. Ann Afr Med. 2015 Jul-Sep; 14 (3): 123-31. |
| [8] | Khan Y, Schwartz B, Johnson I. (2014). Surveillance and epidemiology in natural disasters: a novel framework and assessment of reliability. PLoS Curr. (10); 6 https://doi.org/10.1371%2Fcurrents.dis.6773eb9d5e64b733ab490f78de346003 |
[5-8]
While the IHR (2005) uses an all-hazards approach, infectious diseases have represented the vast majority of hazards among substantiated events reported globally and specifically across the WHO African Region among the 103 substantiated events, 81 (79%) were classified as infectious, 13 (13%) as disaster, 6 (6%) as animal/zoonosis, and 3 (3%) as food safety.
For instance, coordination has been noted as an essential component of the quality of emergency response management particularly for previous responses of Ebola and Marburg
| [8] | Khan Y, Schwartz B, Johnson I. (2014). Surveillance and epidemiology in natural disasters: a novel framework and assessment of reliability. PLoS Curr. (10); 6 https://doi.org/10.1371%2Fcurrents.dis.6773eb9d5e64b733ab490f78de346003 |
| [9] | Ishata Nannie Conteh, Francis Chisaka Kasolo, Paul Olaiya Abiodun, Ebenezer Obi Daniel, Alhassan Fouard Kanu, Rashidatu Fouard Kamara, Aziza Amina Sahid, Olaniyi Felix Sanni, Aminata Tigiedankay Koroma, Josephine Amie Koroma, Lynda Foray-Rhall, Mukeh Kenneth Fahnbulleh, Charles Keimbe, Joseph Sam Kanu, Mohamed Vandy, Daniel Ganu. Infectious Disease Outbreaks in Sierra Leone: Exploration of the Emergency Preparedness and Response in a Decade. World Journal of Public Health. Vol. 8, No. 4, 2023, pp. 291-299 https://doi.org/10.11648/j.wjph.20230804.16 |
| [10] | World Health Organization. Emergency Response Framework. https://www.who.int/publications/i/item/9789241512299 |
| [11] | World Health Organization. Strengthening the global Architecture for Health Emergency Preparedness, response, and resilience: Ten proposals to build a safer world together. https://apps.who.int/gb/ebwha/pdf_files/EB152/B152_12-en.pdf |
[8-11]
. The coordination of the 2014-2016 Ebola outbreak in West Africa was characterized by the unpreparedness and poor coordination of the response at the national and regional levels, leading to its fast spread
| [5] | Zinsou C, Guedegbe G, Dossou L, et al. Lessons learned in improving the quality of a free reproductive health hotline in Benin. Glob Health Sci Pract. 2023; 11(6): e2200296. https://doi.org/10.9745/GHSP-D-22-00296 |
| [10] | World Health Organization. Emergency Response Framework. https://www.who.int/publications/i/item/9789241512299 |
| [11] | World Health Organization. Strengthening the global Architecture for Health Emergency Preparedness, response, and resilience: Ten proposals to build a safer world together. https://apps.who.int/gb/ebwha/pdf_files/EB152/B152_12-en.pdf |
| [12] | Nsenga Ngoy, Boniface Oyugi, Paul O. Ouma, Ishata Nannie Conteh, Solomon Fisseha Woldetsadik, Miriam Nanyunja, Joseph Chukwudi Okeibunor, Zabulon Yoti and Abdou Salam Gueye. Coordination mechanisms for COVID-19 in the WHO Regional office for Africa, BMC Health Services Research (2022) 22: 711 https://doi.org/10.1186/s12913-022-08035-w |
| [13] | World Health Organization. Health Emergency Information and Risk Assessment, WEEKLY BULLETIN ON OUTBREAKS AND OTHER WEEK 23: 29MAY-04 JUN 2023. |
| [14] | Reshma Trasi, Cecelia Angelone, Ginette Hounkanrin. Designing and Implementing the Adaptive Learning Meeting Cycle: The (re)solve Project Experience in Burkina Faso. Global Health: Science and Practice 2023 | Volume 11 | Supplement 2 https://doi.org/10.9745/GHSP-D-22-00217 |
[5, 10-14]
. Learning from the past lessons of response, the subsequent coordination efforts in the 2018–2020 Ebola outbreak in the Democratic Republic of the Congo (which faced additional challenges due to armed rebel groups being at the epicenters’ of the epidemic) and in Guinea in 2021
| [5] | Zinsou C, Guedegbe G, Dossou L, et al. Lessons learned in improving the quality of a free reproductive health hotline in Benin. Glob Health Sci Pract. 2023; 11(6): e2200296. https://doi.org/10.9745/GHSP-D-22-00296 |
| [14] | Reshma Trasi, Cecelia Angelone, Ginette Hounkanrin. Designing and Implementing the Adaptive Learning Meeting Cycle: The (re)solve Project Experience in Burkina Faso. Global Health: Science and Practice 2023 | Volume 11 | Supplement 2 https://doi.org/10.9745/GHSP-D-22-00217 |
| [15] | Cai HTN, Tran HT, Nguyen YHT, Vu GQT, Tran TP, Bui PB, Nguyen HTT, Pham TQ, Lai AT, Van Nuil JI and Lewycka S (2022) Challenges and Lessons Learned in the Development of a Participatory Learning and Action Intervention to Tackle Antibiotic Resistance: Experiences From Northern Vietnam. Front. Public Health 10: 822873. https://doi.org/10.3389/fpubh.2022.822873 |
| [16] | Ganeshkumar P, Ilangovan K, Jagadeesan M, et al. Experiences, challenges, and lessons learned during implementation of a remote monitoring program for home-isolated COVID-19 patients in Chennai, India. Glob Health Sci Pract. 2023; 11(1): e2100458. https://doi.org/10.9745/GHSP-D-21-00458 |
| [17] | Ragazzoni L, Caviglia M, Rosi P, Buson R, Pini S, Merlo F, Della Corte F, Vandy MJ, Jambai A, Putoto G. Designing, implementing, and managing a National Emergency Medical Service in Sierra Leone. Prehosp Disaster Med. 2021; 36(1): 115–120. https://doi.org/10.1017/S1049023X20001442 |
[5, 14-17]
resulted in strengthened inter-state coordination. The coordination mechanism involved the WHO regional office for Africa and Africa Union (AU) member states through the Africa Centre for Disease Control and Prevention (Africa CDC). The WHO’s prompt declaration of a Public Health Emergency of International Concern (PHEIC) shepherded an effective coordinated response to contain the epidemic.
Emerging lessons from the different countries’ coordination of the COVID-19 response has shown the implementation of several strategies to mitigate the impact of the response. This has enabled countries governments to reflect on new strategies and approaches to ensure a more coordinated and effective response to epidemic outbreaks. With this in mind, Niger, like other WHO AFRO countries, has been experimenting with an epidemic response approach.
This study describe the implementation processes of the national Rapid Response Team (RRT) of Niger Republic. The aim of this study is to describe the experiences, challenges, and lessons learned during the Implementation of Emergency Program Response-Rapid Response Team (EPR-RRT) program in Niger.
2. Methodology
The study used mixed methods approach quantitative and qualitative data from a literature review of WHO AFRO coordination mechanisms and the Niger Public Health Emergency Operational Centre (PHEOC). The study was conducted the National Public Health Emergency Operational Centre (PHEOC) of Niger.
The population were all health and non-health personal of the PHEOC and others EPR-RRT members.
Quantitative method was a cross-sectional study conducted during 12 months form September 2022 to September 2023.
Qualitative data from a literature review of WHO AFRO and the Niger Public Health Emergency Operational Centre (PHEOC).
In the literature review we analyzed government and medias policy reports, the countries’ coordination mechanism documents, all the PHEOC strategic document (SOPs, responses strategies, plans, regulations, meeting reports, training report and investigations outbreaks reports…), ministry of health website, WHO website and peer reviewed literature.
Personal data were collected from a survey of health and non-health personal of the PHEOC and others EPR-RRT members, there is no individual medical patient.
Study Period: The study was conducted during 12 months from September 2022 to September 2023.
2.2. Inclusion and Exclusion Criteria
We included in this study all health and non-health personal of the PHEOC and others EPR-RRT members who give their consent during the study period regardless of age, sex, profession or ministry of provenance.
2.3. Ethical Consideration
No ethical concerns were not identified in this study aimed. Consequently the ethical committee permission is not necessary. We obtained the permission to conduct the study of authorities of the National PHEOC. Personal data collected as part of this study was confidential.
3. Results
3.1. Implementation Process
The EPR implementation plan was began on country visit by the WHO-AFRO experts, national and facility level assessment to identify gap and strengths and to define the country’s priorities.
The implementation of this program began with the evaluation of Niger's capacities and capacity building of teams to prepare for, detect and respond to public health emergencies within 24 hours of an alert.
WHO-Afro's top-level scoping mission first went to present the project to the Niger government. This included working sessions with the Prime Minister's office, the Ministers of Health, Agriculture, Environment, Livestock and technical and financial partners, with a visit to emergency response facilities, including the National Center for Emergency Public Health Operations (COUSP), the National School of Public Health (ENSP), CERMES, and the Ministry of Health warehouses, to assess their response capacities within 24-48 hours following an alert and the needs to respond to them.
Next, the team of multi-disciplinary and multi-sector experts was identified and selected. The experts were selected according to rigorous criteria, enabling us to put together a team capable of responding within 24-48 hours of a public health alert. The team is made up of 50 professionals representing ONE-HEALTH sector ministries.
This was followed by a series of expert training sessions on the following modules: Management of PHEOC-IMS-ERF, PHEAS, Rapid response team, overview of humanitarian aid and coordination of the health cluster completed the implementation process of the Niger Rapid Response Team.
3.2. Composition and Socio-Demographic Profiles of RRT Members
The team is composed of a total of 50 experts from 6 ONE HEALTH sectoral ministries. The average age is 49.94 (±5.9) years with extremes ranging from 33 to 56 years. The sex ratio is 0.35 in favor of men.
Table 1. Socio-demographic profiles of RRT members.
Variables | Nombre | Pourcentage |
Sex | | |
Female | 13 | 26% |
Male | 37 | 74% |
RRT members by organizations | | |
Ministry of Defense | 2 | 4% |
Ministry of Women empow’ment | 1 | 2% |
Ministry of Health | 43 | 86% |
Ministry of Livestock | 1 | 2% |
Ministry of Environmental and the Fight against Desertification | 1 | 2% |
Ministry of security | 2 | 4% |
Qualification of members | | |
Program Manager | 1 | 2% |
Risk Communication and Community Engagement (RCCE) Officers | 4 | 8% |
Accounts | 2 | 4% |
Entomologist | 1 | 2% |
Surveillance Officers/Epidemiologists | 14 | 28% |
Data Managers | 2 | 4% |
WASH/IPC Officers | 6 | 12% |
Logistic and fleet officers | 5 | 10% |
Clinicians | 3 | 6% |
Microbiologists | 2 | 4% |
Pharmacists | 4 | 8% |
Psychologists/anthropologist | 3 | 6% |
Security Officers | 2 | 4% |
Veterinar | 1 | 2% |
Total | 50 | 100% |
The Key Capacities of emergency Preparedness and Response-Rapid Response Team (EPR-RRT) Program are: creation of a multi-sectoral, multi-disciplinary national rapid response team: these trained experts are volunteers ready to be deployed in any field in the event of a national or international deployment. These teams have drawn up strategic documents and procedures enabling them to plan their activities both during and after deployment. They also have a work plan and organization inspired by the WHO incident management plan;
Acquiring the human, material and financial resources to respond to a declared public health emergency within 24 to 48 hours: Operations support and logistics by the ensuring of the availability of medical commodities. These teams have acquired the experience of being deployed in 4 regions of the country, 6 districts as part of the response to 6 public health events. (
Table 2 and
figure 2) This team has its own logistics adapted to the different areas of intervention.
Table 2. Repartition of districts and areas where RRT intervention took place.
States | Diseases | Nombre |
Maradi | Madarounfa District | Cholera | 2 |
| Gazaoua District | Yellow Fever | |
Tahoua | Abalak District | Diphteria | 2 |
| Illela District | Diphteria | |
Zinder | FVR | 1 |
Tillabery | Diphteria | 1 |
Total | 4 | 6 |
Ability to rapidly contain an epidemic outbreak: the creation of this rapid response team has made it possible not only to reduce the response time in the event of a declared public health emergency, but also to reduce the morbidity and mortality of outbreaks by reducing their duration and impact, and rapidly breaking the chain of transmission;
Better coordination of responses at all levels of the health pyramid: the composition of the response team is organized around an incident management system housed within the COUSP (PHEOC), enabling it to have effective operational capabilities and to better coordinate response activities with other partners.
The team's work organization and operating mechanism are summarized below.
Figure 1. Map of districts and areas where RRT intervention took place.
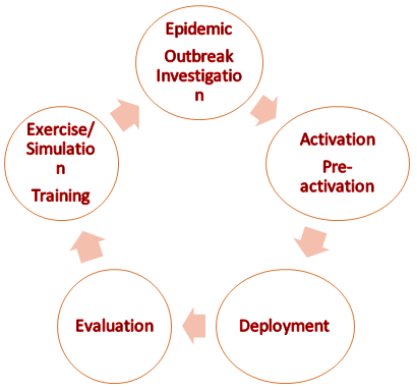
Figure 2. Program design and development process.
Figure 3. Rapid Response Team Organigram.
4. Discussions
We identified themes related to the challenges and some limitations of implementing the rapid response team.
Despite these encouraging results, it should be noted that there are a number of difficulties that limit the RTT's activities in the field or during deployment. These include difficulties of geographical accessibility to certain areas plagued by insecurity due to the activities of non-state armed groups, some of which have already been the focus of Rapid Intervention Team deployments. Another difficulty which limits the activities of the EIR is certain logistical problems linked to certain zones where there are no service stations for the supply of fuel.
4.2. Challenges and Prospects
One of the main challenges for this rapid response team is its ability to keep its personnel constantly mobilized and to be able to intervene within 24-48 hours of a public health emergency being declared. Another major challenge would be to ensure the sustainability of response activities and procedures as defined in the various strategic documents. It would also be desirable to have operational and functional teams at all levels of the country's health pyramid;
5. Conclusion
The process of setting up rapid response teams in Niger was a long and tedious one, but with the commitment of all the stakeholders, namely the government and its partners, these teams were able to see the light of day, to the great delight of Niger populations.
The implementation of this rapid response team has made it possible not only to acquire the technical and operational skills, financial, human and logistical capacities to respond rapidly when a public health emergency occurs, but also and above all to reduce the mortality and morbidity associated with it. In view of the success of the national team, it is desirable to train and make operational teams at local level so that they can take over before and after the deployment of the national team.
Author Contributions
Kadri Sani: Conceptualization, Formal Analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing
Mahamadou Yacouba Moustapha: Conceptualization, Formal Analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing
Garba Salifou Mohamed: Conceptualization, Formal Analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing
Bagouari Adamou: Supervision, Visualization, Validation
Ide Amadou Habibatou: Supervision, Visualization, Validation
Issiaka Gandou Aboubacar: Conceptualization, Formal Analysis, Investigation, Methodology, Supervision
Mohamed Abdel Karim: Data curation, Supervision
Elhadji Ibrahim Tassiou: Supervision, Writing – review & editing
Hanki Yayé: Supervision, Writing – review & editing
Kourouma Mamadou: Conceptualization, Supervision, Writing – review & editing
Ibrahim Salifou Alkassoum: Conceptualization, Supervision, Writing – review & editing
Funding
The program was supported the WHO-AFRO Emergencies Program (AVoHC-SURGE).
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
OMS/Niger/ WHO/Niger. Mission de cadrage du programme SURGE « Renforcement et utilisation des groupes de riposte aux situations d’urgence au Niger ».
https://niger.un.org/fr/173868-mission-de-cadrage-du-programme-surge-«-renforcement-et-utilisation-des-groupes-de-riposte
|
| [2] |
OMS/Niger/ WHO/Niger. Premier déploiement réussi de l’équipe SURGE pour contenir une épidémie de choléra.
https://www.afro.who.int/fr/countries/niger/news/premier-deploiement-reussi-de-lequipe-surge-pour-contenir-une-epidemie-de-cholera
|
| [3] |
OMS/Niger/ WHO/Niger. Remise de certificat aux 50 experts SURGE dans l’urgence épidémiologique.
https://www.afro.who.int/fr/countries/niger/news/remise-de-certificat-aux-50-experts-surge-dans-lurgence-epidemiologique
|
| [4] |
Ishata Nannie Conteh, Francis Chisaka Kasolo, Paul Olaiya Abiodun, Ebenezer Obi Daniel, Alhassan Fouard Kanu, Rashidatu Fouard Kamara, Aziza Amina Sahid, Olaniyi Felix Sanni, Aminata Tigiedankay Koroma, Josephine Amine Koroma, Lynda Foray-Rhall, Mukeh Kenneth Fahnbulleh, Charles Keimbe, Joseph Sam Kanu, Mohamed Vandy, Daniel Ganu. Public Health Emergency Preparedness and Response to Natural Disaster in Sierra Leone: The Milestone in a Decade. World Journal of Public Health. Vol. 8, No. 4, 2023, pp. 272-279.
https://doi.org/10.11648/j.wjph.20230804.14
|
| [5] |
Zinsou C, Guedegbe G, Dossou L, et al. Lessons learned in improving the quality of a free reproductive health hotline in Benin. Glob Health Sci Pract. 2023; 11(6): e2200296.
https://doi.org/10.9745/GHSP-D-22-00296
|
| [6] |
Pete Skelton, Flavio Salio & Nedret Emiroglu. Emergency preparedness and readiness; anticipating the need for rehabilitation, Bull World Health Organ 2022; 100: 744–746
http://dx.doi.org/10.2471/BLT.22.289085
|
| [7] |
Aliyu A. Management of disasters and complex emergencies in Africa: The challenges and constraints. Ann Afr Med. 2015 Jul-Sep; 14 (3): 123-31.
|
| [8] |
Khan Y, Schwartz B, Johnson I. (2014). Surveillance and epidemiology in natural disasters: a novel framework and assessment of reliability. PLoS Curr. (10); 6
https://doi.org/10.1371%2Fcurrents.dis.6773eb9d5e64b733ab490f78de346003
|
| [9] |
Ishata Nannie Conteh, Francis Chisaka Kasolo, Paul Olaiya Abiodun, Ebenezer Obi Daniel, Alhassan Fouard Kanu, Rashidatu Fouard Kamara, Aziza Amina Sahid, Olaniyi Felix Sanni, Aminata Tigiedankay Koroma, Josephine Amie Koroma, Lynda Foray-Rhall, Mukeh Kenneth Fahnbulleh, Charles Keimbe, Joseph Sam Kanu, Mohamed Vandy, Daniel Ganu. Infectious Disease Outbreaks in Sierra Leone: Exploration of the Emergency Preparedness and Response in a Decade. World Journal of Public Health. Vol. 8, No. 4, 2023, pp. 291-299
https://doi.org/10.11648/j.wjph.20230804.16
|
| [10] |
World Health Organization. Emergency Response Framework.
https://www.who.int/publications/i/item/9789241512299
|
| [11] |
World Health Organization. Strengthening the global Architecture for Health Emergency Preparedness, response, and resilience: Ten proposals to build a safer world together.
https://apps.who.int/gb/ebwha/pdf_files/EB152/B152_12-en.pdf
|
| [12] |
Nsenga Ngoy, Boniface Oyugi, Paul O. Ouma, Ishata Nannie Conteh, Solomon Fisseha Woldetsadik, Miriam Nanyunja, Joseph Chukwudi Okeibunor, Zabulon Yoti and Abdou Salam Gueye. Coordination mechanisms for COVID-19 in the WHO Regional office for Africa, BMC Health Services Research (2022) 22: 711
https://doi.org/10.1186/s12913-022-08035-w
|
| [13] |
World Health Organization. Health Emergency Information and Risk Assessment, WEEKLY BULLETIN ON OUTBREAKS AND OTHER WEEK 23: 29MAY-04 JUN 2023.
|
| [14] |
Reshma Trasi, Cecelia Angelone, Ginette Hounkanrin. Designing and Implementing the Adaptive Learning Meeting Cycle: The (re)solve Project Experience in Burkina Faso. Global Health: Science and Practice 2023 | Volume 11 | Supplement 2
https://doi.org/10.9745/GHSP-D-22-00217
|
| [15] |
Cai HTN, Tran HT, Nguyen YHT, Vu GQT, Tran TP, Bui PB, Nguyen HTT, Pham TQ, Lai AT, Van Nuil JI and Lewycka S (2022) Challenges and Lessons Learned in the Development of a Participatory Learning and Action Intervention to Tackle Antibiotic Resistance: Experiences From Northern Vietnam. Front. Public Health 10: 822873.
https://doi.org/10.3389/fpubh.2022.822873
|
| [16] |
Ganeshkumar P, Ilangovan K, Jagadeesan M, et al. Experiences, challenges, and lessons learned during implementation of a remote monitoring program for home-isolated COVID-19 patients in Chennai, India. Glob Health Sci Pract. 2023; 11(1): e2100458.
https://doi.org/10.9745/GHSP-D-21-00458
|
| [17] |
Ragazzoni L, Caviglia M, Rosi P, Buson R, Pini S, Merlo F, Della Corte F, Vandy MJ, Jambai A, Putoto G. Designing, implementing, and managing a National Emergency Medical Service in Sierra Leone. Prehosp Disaster Med. 2021; 36(1): 115–120.
https://doi.org/10.1017/S1049023X20001442
|
Cite This Article
-
APA Style
Sani, K., Moustapha, M. Y., Mohamed, G. S., Adamou, B., Habibatou, I. A., et al. (2024). Implementation of Emergency Preparedness and Response-Rapid Team Program in Niger. World Journal of Public Health, 9(2), 111-118. https://doi.org/10.11648/j.wjph.20240902.12
 Copy
|
Copy
|
 Download
Download
ACS Style
Sani, K.; Moustapha, M. Y.; Mohamed, G. S.; Adamou, B.; Habibatou, I. A., et al. Implementation of Emergency Preparedness and Response-Rapid Team Program in Niger. World J. Public Health 2024, 9(2), 111-118. doi: 10.11648/j.wjph.20240902.12
Copy
|
Download
AMA Style
Sani K, Moustapha MY, Mohamed GS, Adamou B, Habibatou IA, et al. Implementation of Emergency Preparedness and Response-Rapid Team Program in Niger. World J Public Health. 2024;9(2):111-118. doi: 10.11648/j.wjph.20240902.12
Copy
|
Download
-
@article{10.11648/j.wjph.20240902.12,
author = {Kadri Sani and Mahamadou Yacouba Moustapha and Garba Salifou Mohamed and Bagouari Adamou and Ide Amadou Habibatou and Issiaka Gandou Aboubacar and Mohamed Abdel Karim and Elhadji Ibrahim Tassiou and Hanki Yayé and Kourouma Mamadou and Ibrahim Salifou Alkassoum},
title = {Implementation of Emergency Preparedness and Response-Rapid Team Program in Niger
},
journal = {World Journal of Public Health},
volume = {9},
number = {2},
pages = {111-118},
doi = {10.11648/j.wjph.20240902.12},
url = {https://doi.org/10.11648/j.wjph.20240902.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.wjph.20240902.12},
abstract = {Introduction: The WHO’s prompt declaration of a Public Health Emergency of International Concern (PHEIC) shepherded an effective coordinated response to contain the epidemic. Objective: The aim of this study is to describe the experiences, challenges, and lessons learned during the Implementation of Emergency Preparedness and Response-Rapid Response Team (EPR-RRT) program. Method: The study used mixed methods approach quantitative and qualitative data from a literature review of WHO AFRO coordination mechanisms and the Niger Public Health Emergency Operational Centre (PHEOC). The study was conducted in the National Public Health Emergency Operational Centre (PHEOC) of Niger during 12 months from September 2022 to September 2023. Results: The implementation of this program began with the evaluation of Niger's capacities and capacity building of teams to prepare, detect and respond to public health emergencies within 24 hours of an alert. The team of multi-disciplinary and multi-sector experts was identified and selected and trained on series of modules training. The team is composed of a total of 50 experts from 6 ONE HEALTH sectoral ministries. The average age is 49.94 (±5.9) years with extremes ranging from 33 to 56 years. The sex ratio is 0.35. The team have acquired the experience of being deployed in 4 regions of the country, 6 districts as part of the response to 6 public health events. Conclusion: The rapid response team has made it possible not only to acquire the technical and operational skills, financial, human and logistical capacities to respond rapidly when a public health emergency occurs.
},
year = {2024}
}
Copy
|
Download
-
TY - JOUR
T1 - Implementation of Emergency Preparedness and Response-Rapid Team Program in Niger
AU - Kadri Sani
AU - Mahamadou Yacouba Moustapha
AU - Garba Salifou Mohamed
AU - Bagouari Adamou
AU - Ide Amadou Habibatou
AU - Issiaka Gandou Aboubacar
AU - Mohamed Abdel Karim
AU - Elhadji Ibrahim Tassiou
AU - Hanki Yayé
AU - Kourouma Mamadou
AU - Ibrahim Salifou Alkassoum
Y1 - 2024/04/28
PY - 2024
N1 - https://doi.org/10.11648/j.wjph.20240902.12
DO - 10.11648/j.wjph.20240902.12
T2 - World Journal of Public Health
JF - World Journal of Public Health
JO - World Journal of Public Health
SP - 111
EP - 118
PB - Science Publishing Group
SN - 2637-6059
UR - https://doi.org/10.11648/j.wjph.20240902.12
AB - Introduction: The WHO’s prompt declaration of a Public Health Emergency of International Concern (PHEIC) shepherded an effective coordinated response to contain the epidemic. Objective: The aim of this study is to describe the experiences, challenges, and lessons learned during the Implementation of Emergency Preparedness and Response-Rapid Response Team (EPR-RRT) program. Method: The study used mixed methods approach quantitative and qualitative data from a literature review of WHO AFRO coordination mechanisms and the Niger Public Health Emergency Operational Centre (PHEOC). The study was conducted in the National Public Health Emergency Operational Centre (PHEOC) of Niger during 12 months from September 2022 to September 2023. Results: The implementation of this program began with the evaluation of Niger's capacities and capacity building of teams to prepare, detect and respond to public health emergencies within 24 hours of an alert. The team of multi-disciplinary and multi-sector experts was identified and selected and trained on series of modules training. The team is composed of a total of 50 experts from 6 ONE HEALTH sectoral ministries. The average age is 49.94 (±5.9) years with extremes ranging from 33 to 56 years. The sex ratio is 0.35. The team have acquired the experience of being deployed in 4 regions of the country, 6 districts as part of the response to 6 public health events. Conclusion: The rapid response team has made it possible not only to acquire the technical and operational skills, financial, human and logistical capacities to respond rapidly when a public health emergency occurs.
VL - 9
IS - 2
ER -
Copy
|
Download