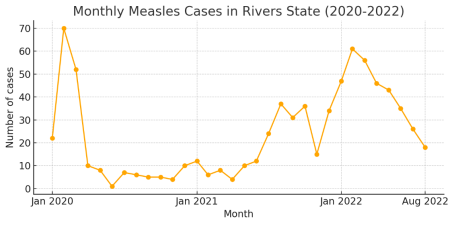
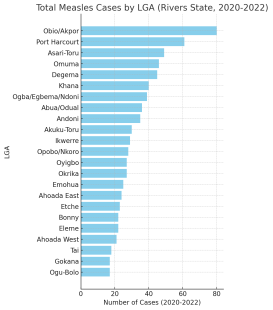
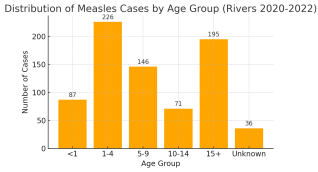
Background: Measles remains a leading cause of child mortality globally despite an effective vaccine. Nigeria has persistent measles transmission due to suboptimal immunization coverage (around 54% for first dose)]. The study analyzed measles surveillance data of Rivers State from 2020-2022 to identify spatiotemporal clusters and outbreak characteristics by Local Government Area (LGA) and age group. Methods: A retrospective cross-sectional study conducted on measles case-based surveillance data for Rivers State from January 2020 to December 2022. Cases were aggregated by month, LGA, and age. Measles outbreak was defined as the number of laboratory-confirmed cases ≥3 in an LGA within 4 weeks Descriptive statistics summarized case counts by time, place, and age. Chi-square tests assessed associations between categorical variables (e.g. age group verses LGA, year verses age distribution). An epidemic curve and bar charts were used to visualize temporal trends and the distribution of cases by LGA and age group. Results: A total of 761 measles cases were reported in Rivers State from 2020-2022 (200 in 2020; 229 in 2021; 332 in 2022). The epidemic curve showed a peak of 70 cases in February 2020, a decline, a resurgence in mid-2021, and a larger outbreak in early 2022 (peak 61 cases in February 2022). Transmission persisted year-round at lower levels between these outbreaks. Spatial distribution of Cases occurred in all 23 LGAs, but 10 LGAs (led by Obio/Akpor and Port Harcourt) accounted for ~60% of cases. The age distribution of Cases ranged from infants to 79 years (median ~6 years, IQR 2-16). Children <5 years comprised 41% of cases, and 25% were aged ≥15 years. children (1-4 years) and adults also contributed substantial proportions, indicating gaps in historical vaccination coverage. Conclusion: Rivers State experienced recurrent measles outbreaks in 2020-2022 with clear spatiotemporal clustering. The pattern suggests a two-year cycle of major outbreaks, with an early 2020 peak, a smaller mid-2021 wave, and a large 2022 outbreak. All LGAs were affected, but the burden was more in certain urban centers and varied over time. Gaps in immunity were evident in both young children and older age groups, reflecting inadequate vaccination coverage.
| Published in | World Journal of Public Health (Volume 10, Issue 3) |
| DOI | 10.11648/j.wjph.20251003.31 |
| Page(s) | 398-406 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Spatiotemporal, Patterns, Measles, Outbreak, Rivers State
Age Group | 2020 Cases (n=200) | 2021 Cases (n=229) | 2022 Cases (n=332) | Total 2020-22 (n=761) |
|---|---|---|---|---|
< 1 year | 22 (11.0%) | 30 (13.1%) | 35 (10.5%) | 87 (11.4%) |
1-4 years | 61 (30.5%) | 51 (22.3%) | 114 (34.3%) | 226 (29.7%) |
5-9 years | 44 (22.0%) | 33 (14.4%) | 69 (20.8%) | 146 (19.2%) |
10-14 years | 15 (7.5%) | 30 (13.1%) | 26 (7.8%) | 71 (9.3%) |
≥15 years | 39 (19.5%) | 77 (33.6%) | 79 (23.8%) | 195 (25.6%) |
Unknown | 19 (9.5%) | 8 (3.5%) | 9 (2.7%) | 36 (4.7%) |
Total | 200 (100%) | 229 (100%) | 332 (100%) | 761 (100%) |
IDSR | Integrated Disease Surveillance and Response. |
LGA | Local Government Area |
MCV | Measles Containing Vaccine |
MCV1 | First Dose of Measles Containing Vaccine |
MCV2 | Second Dose of Measles Containing Vaccine |
NCDC | Nigeria Centre for Disease Control |
ORI | Outbreak Response Immunization |
SIA | Supplementary Immunization Activity |
UNICEF | United Nations Children’s Fund |
WHO | World Health Organization |
| [1] | WHO. Measles - Key facts. Geneva: World Health Organization; 2019. Available from: |
| [2] | WHO. Global measles deaths fell by 73% between 2000 and 2018. Geneva: World Health Organization; 2019. |
| [3] | Masresha BG, Hatcher C, Lebo E, et al. Progress Toward Measles Elimination — African Region, 2017-2021. MMWR Morb Mortal Wkly Rep. 2023; 72(36): 985-991. |
| [4] | Dabbagh A, Laws RL, Steulet C, et al. Progress toward regional measles elimination — worldwide, 2000-2020. MMWR Morb Mortal Wkly Rep. 2021; 70(45): 1563-1569. |
| [5] | WHO Regional Office for Africa. Measles outbreaks in Africa. Brazzaville: WHO AFRO; 2021. |
| [6] | Nnaji CA, et al. Vaccine hesitancy and challenges of measles elimination in sub-Saharan Africa. Vaccine. 2022; 40(35): 5162-5168. |
| [7] | UNICEF/WHO Estimates of National Immunization Coverage (WUENIC). Geneva; 2021. |
| [8] | Nigeria Centre for Disease Control. Weekly epidemiological report, 2021. Abuja: NCDC. |
| [9] | Gavi, the Vaccine Alliance. COVID-19 pandemic threatens measles elimination. Gavi; 2022. |
| [10] | Utulu R, Urang J, Usman A, et al. Performance of measles case-based surveillance system in Rivers State, Nigeria 2011-2018. J Immunol Sci. 2020; 4(1): 10-18. |
| [11] | Enitan SS, Iduh MU, Itodo GE, et al. Combating measles in Nigeria: Epidemiological trends and interventions. Afro-Egypt J Infect Endem Dis. 2024; 14(4): 375-95. |
| [12] | Naku D. Measles: 50 children feared dead in Rivers communities. Punch Nigeria. 2022 Aug 8. |
| [13] | News Agency of Nigeria. Measles outbreak spreads to eight states. Peoples Gazette. 2022 Mar 4. |
| [14] | Okonko IO, et al. An overview of measles resurgence in Nigeria. Int J Trop Dis Health. 2019; 36(4): 1-10. |
| [15] | Goodson JL, et al. Measles outbreaks and progress toward elimination in Africa, 2016-2018. J Infect Dis. 2020;222(Suppl 5): S652-60. |
| [16] | Fatiregun AA, et al. Outbreak response to measles in Nigeria: lessons from the field. Pan Afr Med J. 2021; 38: 123. |
| [17] | Orenstein WA, Cairns L, Hinman A, et al. Measles and rubella global strategic plan 2012-2020 midterm review. Vaccine. 2018; 36 Suppl 1: A1-34. |
| [18] | Moss WJ. Measles. Lancet. 2017; 390(10111): 2490-502. |
| [19] | Aaby P, Martins CL, Garly ML, Rodrigues A, Benn CS, Whittle H. Non-specific effects of measles vaccine on child survival: review. Trop Med Int Health. 2010; 15(9): 1079-87. |
| [20] | WHO. Vitamin A supplementation in measles control. Geneva: WHO; 2020. |
| [21] | Pomeroy LW, et al. Seasonality of measles in Africa: a systematic review. BMC Infect Dis. 2019; 19: 297. |
| [22] | Ferrari MJ, et al. Influence of demographic and seasonal patterns on measles epidemics in Africa. Proc Biol Sci. 2010; 277(1692): 2775-82. |
| [23] | Nsubuga P, et al. Measles outbreak cycles in Africa. J Infect Dis. 2020; 222(Suppl 5): S640-51. |
| [24] | Grais RF, et al. Uncertainty and spatiotemporal heterogeneity in measles epidemics in West Africa. Epidemiol Infect. 2006; 134(5): 1009-19. |
| [25] | Gavi. 24 million Nigerian kids to be vaccinated against measles in major campaign. 2024 Nov 7. |
| [26] | Patel MK, et al. Progress toward regional measles elimination — worldwide, 2000-2019. MMWR. 2020; 69(45): 1700-5. |
| [27] | Goodson JL, et al. Challenges in achieving measles elimination in Africa. J Infect Dis. 2017; 216(Suppl 1): S293-9. |
| [28] | WHO/UNICEF. Nigeria immunization coverage trends. Geneva; 2023. |
| [29] | Leuridan E, Sabbe M, Van Damme P. Measles outbreak in Europe: susceptibility of infants too young to be immunized. Vaccine. 2012; 30(9): 5905-13. |
| [30] | Oyo-Ita A, et al. Barriers to routine immunization in Nigeria: a systematic review. Vaccine. 2016; 34(34): 4144-52. |
| [31] | Abegunde D, et al. Vaccine hesitancy in Nigeria: drivers and interventions. Vaccine. 2023; 41(13): 2090-98. |
| [32] | Nnaji CA, et al. Bridging immunization gaps in LMICs. Trop Med Int Health. 2023; 28(6): 765-73. |
| [33] | Patel MK, et al. Progress toward measles elimination in the WHO African Region, 2013-2016. MMWR. 2017; 66(17): 436-43. |
| [34] | Gidding HF, et al. The impact of supplementary immunization on measles elimination. Vaccine. 2018; 36(41): 6065-72. |
| [35] | Ogbuanu IU, et al. Urban measles outbreaks in sub-Saharan Africa. Vaccine. 2019; 37(24): 3257-63. |
| [36] | Brownwright TK, et al. Equity in measles vaccination coverage. Int J Equity Health. 2017; 16: 134. |
| [37] | Moss WJ, Griffin DE. Measles. Lancet. 2012; 379: 153-64. |
| [38] | Perry RT, Halsey NA. The clinical significance of measles: a review. J Infect Dis. 2004; 189 Suppl 1: S4-16. |
| [39] | NCDC. Integrated disease surveillance and response report. Abuja; 2022. |
| [40] | Punch Newspaper. Measles outbreak fatalities in Rivers State. 2022. |
| [41] | Utulu R, et al. Performance of measles surveillance, Rivers State. J Immunol Sci. 2020. |
| [42] | WHO. Strengthening surveillance for vaccine-preventable diseases. Geneva: WHO; 2022. |
| [43] | Balogun MS, et al. Evaluation of IDSR performance in Nigeria. BMC Public Health. 2019; 19: 123. |
| [44] | WHO AFRO. New measles elimination target 2030. Geneva; 2023. |
| [45] | Gavi. Supporting measles elimination in Africa. Geneva; 2024. |
| [46] | Goodson JL, et al. Ensuring equity in SIAs for measles control. J Infect Dis. 2017; 216 Suppl 1: S293-301. |
| [47] | Nnaji CA, et al. Role of community engagement in vaccination. Vaccine. 2023; 41(22): 3052-60. |
| [48] | UNICEF. Building trust for vaccines in Nigeria. New York; 2022. |
APA Style
Nwadiuto, I., Mberekpe, O. P., Briggs, C. T., Green, P. A., Onyekwere, N. V., et al. (2025). Spatiotemporal Patterns of Measles Outbreaks in Rivers State, Nigeria (2020-2022). World Journal of Public Health, 10(3), 398-406. https://doi.org/10.11648/j.wjph.20251003.31
ACS Style
Nwadiuto, I.; Mberekpe, O. P.; Briggs, C. T.; Green, P. A.; Onyekwere, N. V., et al. Spatiotemporal Patterns of Measles Outbreaks in Rivers State, Nigeria (2020-2022). World J. Public Health 2025, 10(3), 398-406. doi: 10.11648/j.wjph.20251003.31
@article{10.11648/j.wjph.20251003.31,
author = {Ifeoma Nwadiuto and Ositadinma Pius Mberekpe and Christie Tobin Briggs and Pauline Aruoture Green and Nnanna Victor Onyekwere and Golden Owhonda and Felix Wekere},
title = {Spatiotemporal Patterns of Measles Outbreaks in Rivers State, Nigeria (2020-2022)
},
journal = {World Journal of Public Health},
volume = {10},
number = {3},
pages = {398-406},
doi = {10.11648/j.wjph.20251003.31},
url = {https://doi.org/10.11648/j.wjph.20251003.31},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.wjph.20251003.31},
abstract = {Background: Measles remains a leading cause of child mortality globally despite an effective vaccine. Nigeria has persistent measles transmission due to suboptimal immunization coverage (around 54% for first dose)]. The study analyzed measles surveillance data of Rivers State from 2020-2022 to identify spatiotemporal clusters and outbreak characteristics by Local Government Area (LGA) and age group. Methods: A retrospective cross-sectional study conducted on measles case-based surveillance data for Rivers State from January 2020 to December 2022. Cases were aggregated by month, LGA, and age. Measles outbreak was defined as the number of laboratory-confirmed cases ≥3 in an LGA within 4 weeks Descriptive statistics summarized case counts by time, place, and age. Chi-square tests assessed associations between categorical variables (e.g. age group verses LGA, year verses age distribution). An epidemic curve and bar charts were used to visualize temporal trends and the distribution of cases by LGA and age group. Results: A total of 761 measles cases were reported in Rivers State from 2020-2022 (200 in 2020; 229 in 2021; 332 in 2022). The epidemic curve showed a peak of 70 cases in February 2020, a decline, a resurgence in mid-2021, and a larger outbreak in early 2022 (peak 61 cases in February 2022). Transmission persisted year-round at lower levels between these outbreaks. Spatial distribution of Cases occurred in all 23 LGAs, but 10 LGAs (led by Obio/Akpor and Port Harcourt) accounted for ~60% of cases. The age distribution of Cases ranged from infants to 79 years (median ~6 years, IQR 2-16). Children Conclusion: Rivers State experienced recurrent measles outbreaks in 2020-2022 with clear spatiotemporal clustering. The pattern suggests a two-year cycle of major outbreaks, with an early 2020 peak, a smaller mid-2021 wave, and a large 2022 outbreak. All LGAs were affected, but the burden was more in certain urban centers and varied over time. Gaps in immunity were evident in both young children and older age groups, reflecting inadequate vaccination coverage.
},
year = {2025}
}
TY - JOUR T1 - Spatiotemporal Patterns of Measles Outbreaks in Rivers State, Nigeria (2020-2022) AU - Ifeoma Nwadiuto AU - Ositadinma Pius Mberekpe AU - Christie Tobin Briggs AU - Pauline Aruoture Green AU - Nnanna Victor Onyekwere AU - Golden Owhonda AU - Felix Wekere Y1 - 2025/09/09 PY - 2025 N1 - https://doi.org/10.11648/j.wjph.20251003.31 DO - 10.11648/j.wjph.20251003.31 T2 - World Journal of Public Health JF - World Journal of Public Health JO - World Journal of Public Health SP - 398 EP - 406 PB - Science Publishing Group SN - 2637-6059 UR - https://doi.org/10.11648/j.wjph.20251003.31 AB - Background: Measles remains a leading cause of child mortality globally despite an effective vaccine. Nigeria has persistent measles transmission due to suboptimal immunization coverage (around 54% for first dose)]. The study analyzed measles surveillance data of Rivers State from 2020-2022 to identify spatiotemporal clusters and outbreak characteristics by Local Government Area (LGA) and age group. Methods: A retrospective cross-sectional study conducted on measles case-based surveillance data for Rivers State from January 2020 to December 2022. Cases were aggregated by month, LGA, and age. Measles outbreak was defined as the number of laboratory-confirmed cases ≥3 in an LGA within 4 weeks Descriptive statistics summarized case counts by time, place, and age. Chi-square tests assessed associations between categorical variables (e.g. age group verses LGA, year verses age distribution). An epidemic curve and bar charts were used to visualize temporal trends and the distribution of cases by LGA and age group. Results: A total of 761 measles cases were reported in Rivers State from 2020-2022 (200 in 2020; 229 in 2021; 332 in 2022). The epidemic curve showed a peak of 70 cases in February 2020, a decline, a resurgence in mid-2021, and a larger outbreak in early 2022 (peak 61 cases in February 2022). Transmission persisted year-round at lower levels between these outbreaks. Spatial distribution of Cases occurred in all 23 LGAs, but 10 LGAs (led by Obio/Akpor and Port Harcourt) accounted for ~60% of cases. The age distribution of Cases ranged from infants to 79 years (median ~6 years, IQR 2-16). Children Conclusion: Rivers State experienced recurrent measles outbreaks in 2020-2022 with clear spatiotemporal clustering. The pattern suggests a two-year cycle of major outbreaks, with an early 2020 peak, a smaller mid-2021 wave, and a large 2022 outbreak. All LGAs were affected, but the burden was more in certain urban centers and varied over time. Gaps in immunity were evident in both young children and older age groups, reflecting inadequate vaccination coverage. VL - 10 IS - 3 ER -
Department of Community Medicine, Rivers State University, Port Harcourt, Nigeria
Department of Community Medicine, Rivers State University, Port Harcourt, Nigeria
Department of Community Medicine, Rivers State University, Port Harcourt, Nigeria
Department of Community Medicine, Rivers State University, Port Harcourt, Nigeria
Department of Community Medicine, Rivers State University, Port Harcourt, Nigeria
Department of Community Medicine, Rivers State University, Port Harcourt, Nigeria
Department of Community Medicine, Rivers State University, Port Harcourt, Nigeria
Information