Abstract
Healthcare leadership increasingly requires more than administrative efficiency, communication skill, and operational oversight. In contemporary public health systems, leaders are expected to interpret evidence, evaluate data quality, understand research designs, assess uncertainty, and translate findings into practical policy and program decisions. This manuscript argues that research literacy should be recognized as a core healthcare leadership competency because evidence-based decision-making depends on leaders’ ability to understand research methods and statistics. Research literacy enables leaders to differentiate strong evidence from weak evidence, interpret quantitative and qualitative findings, evaluate program outcomes, and make transparent decisions in complex health systems. Drawing on principles of research methodology, hierarchy of evidence, epidemiology, program evaluation, and evidence-informed policymaking, the paper discusses how healthcare leaders can use research methods and statistics to improve public health planning, resource allocation, implementation, monitoring, and evaluation. It also highlights the risks of evidence-blind leadership, including inefficient spending, poorly targeted interventions, weak accountability, and preventable health inequities. The paper concludes that research literacy should be embedded in healthcare leadership education, institutional decision-making structures, and continuing professional development. A research-literate healthcare leader is not necessarily a full-time researcher, but must be able to ask answerable questions, critically appraise evidence, interpret statistical findings, engage with technical experts, and translate knowledge into ethical, equitable, and context-sensitive public health action.
|
Published in
|
American Journal of Health Research (Volume 14, Issue 4)
|
|
DOI
|
10.11648/j.ajhr.20261404.11
|
|
Page(s)
|
179-188 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2026. Published by Science Publishing Group
|
Keywords
Research Literacy, Healthcare Leadership, Evidence-based Decision-making, Public Health, Research Methods, Statistics, Health Policy, Evidence-informed Practice
1. Introduction
Healthcare leaders operate in environments shaped by disease burden, limited resources, changing population needs, political pressures, technological innovation, and rising expectations for accountability. In such settings, leadership decisions cannot rely only on personal experience, institutional tradition, hierarchy, or intuition. Decisions about public health programs, service delivery models, financing priorities, workforce planning, emergency preparedness, disease prevention, and quality improvement require a systematic understanding of evidence. Research literacy, therefore, is no longer an optional academic skill; it is a practical leadership competency.
Research is commonly understood as a systematic process of gathering and analyzing information to generate knowledge that can be generalized beyond an individual case or isolated observation. The uploaded course material similarly presents research as a systematic investigation designed to develop or contribute to generalizable knowledge and describes the research process as moving from a question or problem to literature review, hypothesis formulation, protocol design, data collection, analysis, conclusion, and application. In healthcare leadership, this systematic orientation is essential because leaders are frequently required to make decisions affecting large populations, not only individual patients.
Public health decision-making is particularly dependent on evidence because public health interventions often affect communities, institutions, and entire populations. The CDC describes public health as work that protects and improves the health of people and communities through activities such as promoting healthy lifestyles, researching disease and injury prevention, and detecting, preventing, and responding to infectious diseases
. This broad mandate requires leaders to understand not only what works clinically, but also what works socially, economically, culturally, and operationally.
The World Health Organization emphasizes evidence-informed decision-making as a process of identifying, appraising, and mobilizing the best available evidence for safe and effective health policy and programs
. This definition is important because it recognizes that evidence does not automatically translate into policy. Evidence must be interpreted, contextualized, communicated, and applied. Healthcare leaders are the bridge between research knowledge and public health action. Without research literacy, this bridge becomes weak.
This manuscript argues that research literacy should be treated as a core healthcare leadership competency. It examines the meaning of research literacy, its relationship with evidence-based decision-making, the role of research methods and statistics, and the leadership capabilities needed to strengthen evidence-based public health practice
| [3] | Sanaeifar E, Houshmand E, Moghri J, Vejdani M, Tabatabaee SS. Requirements for evidence?based management competency in healthcare: a scoping review. Front Public Health. 2025; 13: 1490454.
https://doi.org/10.3389/fpubh.2025.1490454 |
[3]
.
2. Conceptualizing Research Literacy in Healthcare Leadership
Research literacy refers to the ability to understand, interpret, critically appraise, and use research evidence. For healthcare leaders, research literacy includes the ability to formulate relevant questions, understand research designs, interpret quantitative and qualitative findings, evaluate methodological quality, recognize bias, understand basic statistical concepts, and translate findings into decisions. It does not mean that every healthcare leader must become a biostatistician or academic researcher. Rather, it means that leaders should be competent enough to engage intelligently with evidence and with experts.
Research literacy begins with asking the right question. Poorly framed questions lead to poorly selected evidence and weak decisions. A strong research or policy question is clear, focused, answerable, and relevant to the problem at hand. For example, a healthcare leader should not simply ask, “Is this program good?” A more useful question would be, “Among low-income pregnant women attending public primary care facilities, does community-based nutrition counseling improve antenatal care attendance and reduce anemia compared with routine care?” Such a question helps define the population, intervention, comparator, outcome, and context.
Research literacy also requires an understanding of different types of research questions. Descriptive questions ask what exists or what is happening. Relational questions examine associations between variables. Causal questions assess whether one factor produces change in another. The uploaded research methods material identifies descriptive, relational, and causal questions as progressively demanding types of inquiry. This distinction is crucial for leadership because different decisions require different levels of evidence. A descriptive survey may be enough to identify low service coverage, but a causal question about whether an intervention improves outcomes requires stronger design and analysis.
For healthcare leaders, research literacy is directly connected to accountability. Leaders must justify why one program is funded over another, why a guideline is adopted, why a service model is changed, or why a population is prioritized. Evidence-literate leaders can explain the basis of their decisions transparently. Evidence-illiterate leaders may make decisions based on anecdote, authority, convenience, or political pressure, even when better evidence exists
.
3. Research Methods as Leadership Tools
Research methods are not only academic procedures; they are practical tools for leadership. A leader who understands research methods can better evaluate proposals, interpret reports, commission studies, monitor programs, and identify whether evidence is suitable for a decision.
3.1. Quantitative Methods
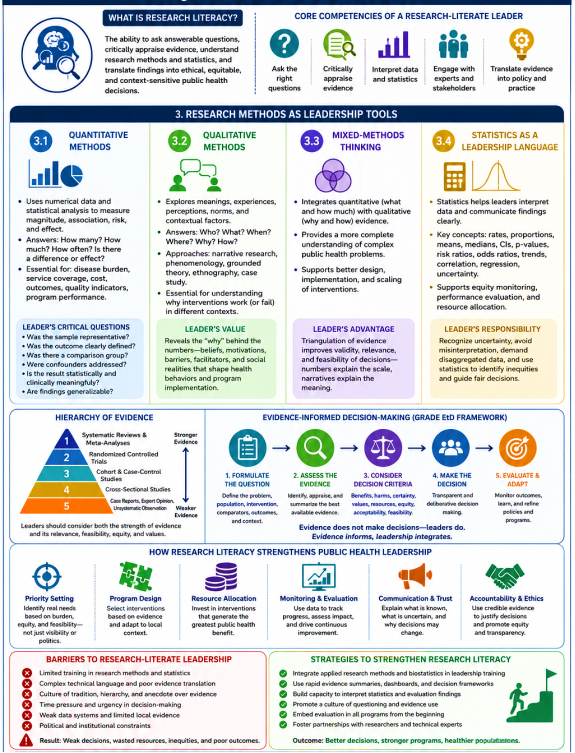
Quantitative research uses numerical data and statistical analysis to measure frequency, magnitude, association, risk, and effect. In healthcare leadership, quantitative methods are essential for measuring disease burden, service coverage, cost, mortality, morbidity, patient outcomes, workforce productivity, waiting time, quality indicators, and program performance. The uploaded course material describes quantitative research as numerical, statistical, and often linked with experimental and quasi-experimental designs.
For public health leaders, quantitative data answer questions such as: How many children are under-immunized? What proportion of patients are lost to follow-up? Which districts have the highest maternal mortality? Did a health education campaign reduce tobacco use? Is a screening program cost-effective? Such questions cannot be answered through opinion alone.
However, quantitative literacy also requires caution. Numbers can create an impression of certainty, but poor measurement, biased sampling, confounding, missing data, and inappropriate statistical analysis can produce misleading conclusions. A research-literate leader should therefore ask: Was the sample representative? Was the outcome clearly defined? Was there a comparison group? Were confounders addressed? Was the result statistically significant and clinically meaningful? Are the findings generalizable to the target population?
3.2. Qualitative Methods
Qualitative research explores meanings, experiences, perceptions, social norms, implementation barriers, and contextual factors. It is particularly valuable in public health because many health problems are shaped by behavior, culture, trust, stigma, gender norms, health system relationships, and socioeconomic realities. The uploaded course material presents qualitative research as descriptive, interpretive, and useful for exploring questions such as who, what, when, where, why, and how. It also identifies approaches such as narrative research, phenomenology, grounded theory, ethnography, and case study
.
For healthcare leaders, qualitative evidence helps explain why an intervention works in one setting but fails in another. For example, vaccination coverage may be low not only because of supply problems but also because of misinformation, fear, religious concerns, poor communication, inconvenient clinic hours, or disrespectful treatment by providers. Quantitative data may show the coverage gap, but qualitative data can explain the reasons behind the gap.
The Boston University public health material included in the uploaded file notes that qualitative methods help understand public health problems in greater depth by capturing beliefs, opinions, norms, behaviors, and contextual information that traditional quantitative methods may miss. This is highly relevant for leadership because public health decisions often fail when leaders understand data but not context.
3.3. Mixed-Methods Thinking
Strong healthcare leadership requires mixed-methods thinking. Quantitative evidence tells leaders what is happening and how much. Qualitative evidence helps explain why it is happening and how change may be achieved. A leader deciding whether to scale up a maternal health intervention should examine quantitative outcomes, such as facility delivery rates, antenatal care attendance, complications, and costs, but also qualitative evidence on women’s experiences, provider attitudes, family decision-making, transportation barriers, and cultural acceptability.
Research-literate leadership is therefore not about choosing between numbers and narratives. It is about integrating both forms of evidence to make better decisions
| [6] | Guetterman TC, Fetters MD, Creswell JW. Integrating quantitative and qualitative results in health science mixed methods research through joint displays. Ann Fam Med. 2015; 13(6): 554–561.
https://doi.org/10.1370/afm.1865 |
[6]
.
3.4. Statistics as a Leadership Language
Statistics is often viewed as a technical subject reserved for researchers. However, in healthcare leadership, statistics functions as a language of decision-making. Leaders do not need to perform every statistical calculation themselves, but they must understand enough to interpret results and ask critical questions.
Basic statistical literacy includes understanding rates, proportions, means, medians, confidence intervals, p-values, risk ratios, odds ratios, trends, correlation, regression, and uncertainty. These concepts are necessary for interpreting epidemiological reports, quality dashboards, monitoring indicators, clinical trial results, budget impact analyses, and evaluation findings.
For example, a statistically literate leader knows that a statistically significant result may not always be practically meaningful. A very small effect can become statistically significant in a large sample, while a meaningful effect may fail to reach statistical significance in a small study. Similarly, correlation does not prove causation. A leader who understands this distinction is less likely to overstate findings or make premature policy claims.
Statistics also supports equity-oriented leadership. Disaggregated data can reveal differences by gender, income, geography, ethnicity, disability, age, or service access. Without statistical monitoring, inequities may remain hidden behind national averages. For example, an immunization program may appear successful at the national level while remote, poor, or marginalized communities remain underserved
.
Healthcare leaders also need statistical literacy to evaluate program performance. The CDC explains that program evaluation answers important questions about public health programs through methodical and intentional engagement with stakeholders and produces findings that can support program improvement and decision-making
. Leaders who understand evaluation statistics can better judge whether a program achieved outcomes, whether implementation was adequate, whether observed change was attributable to the program, and whether resources were used efficiently.
Figure 1. Research Methods as Leadership Tools.
Table 1.
Research Methods as Leadership Tools | [18] | Achana F, Hubbard S, Sutton A, Kendrick D, Cooper N. An exploration of synthesis methods in public health evaluations of interventions concludes that the use of modern statistical methods would be beneficial. J Clin Epidemiol. 2014 Apr; 67(4): 376-90. https://doi.org/10.1016/j.jclinepi.2013.09.018 |
Research Method / Tool | Main Purpose | What It Helps Leaders Understand | Leadership Use in Healthcare | Key Questions Leaders Should Ask |
Quantitative Methods | Uses numerical data and statistical analysis to measure frequency, magnitude, risk, association, and effect. | What is happening, how often it is happening, how large the problem is, and whether an intervention has measurable impact. | Helps leaders measure disease burden, service coverage, mortality, morbidity, cost, waiting time, workforce productivity, quality indicators, and program performance. | Was the sample representative? Was the outcome clearly defined? Was there a comparison group? Were confounders controlled? Are results statistically and clinically meaningful? |
Qualitative Methods | Explores experiences, perceptions, meanings, social norms, barriers, and context. | Why a problem is happening and how people experience health services or interventions. | Helps leaders understand patient behavior, trust, stigma, culture, gender norms, provider relationships, and implementation barriers. | What are the beliefs, fears, opinions, or social factors affecting the issue? Why did the intervention succeed or fail in this setting? What contextual factors must be considered? |
Mixed-Methods Thinking | Combines quantitative and qualitative evidence. | Both the size of the problem and the reasons behind the problem. | Supports balanced decision-making by integrating numerical outcomes with human experience and field realities. | What do the numbers show? What do people’s experiences explain? Do both types of evidence support the same decision? |
Statistics as a Leadership Language | Uses statistical concepts to interpret evidence and guide decisions. | Whether findings are meaningful, reliable, generalizable, and useful for policy or program decisions. | Helps leaders interpret reports, dashboards, clinical trials, evaluation findings, trends, risk ratios, confidence intervals, and equity gaps. | Is the result statistically significant? Is it practically meaningful? Does correlation imply causation? Are inequities hidden behind averages? |
Program Evaluation | Systematically assesses whether a program is working as intended. | Whether a program achieved outcomes, was implemented properly, and used resources efficiently. | Helps leaders improve programs, justify funding, monitor progress, and make evidence-based decisions. | Did the program achieve its objectives? Was the change due to the program? Were resources used efficiently? What should be improved? |
Table 2. Summary Relationship.
Evidence Type | Answers | Example in Public Health Leadership |
Quantitative Evidence | What is happening? How much? How many? | How many children are under-immunized? Which district has the highest maternal mortality? |
Qualitative Evidence | Why is it happening? How do people experience it? | Why are families refusing vaccination? What barriers do women face in accessing maternal care? |
Mixed-Methods Evidence | What is happening and why? | Combining immunization coverage data with community interviews to design better vaccination strategies. |
Statistical Evidence | How reliable and meaningful are the findings? | Understanding whether a health campaign truly reduced tobacco use or whether the change happened by chance. |
Evaluation Evidence | Did the program work and should it continue? | Assessing whether a screening program improved early diagnosis and was cost-effective. |
4. Hierarchy of Evidence and Leadership Judgment
Evidence-based decision-making requires leaders to understand that not all evidence has equal strength. A single anecdote, expert opinion, case report, observational study, randomized controlled trial, and systematic review do not carry the same evidentiary weight.
The uploaded material on hierarchy of evidence places unsystematic clinical observation and physiologic studies at lower levels, observational studies at intermediate levels, and randomized trials and systematic reviews at higher levels for clinical decision-making. It also explains that observational studies may be limited by bias, lack of control, small sample size, unknown factors, and limited follow-up, while randomization helps balance known and unknown factors between groups
.
For healthcare leaders, this hierarchy matters because public health policies often affect large populations and involve substantial resources. Leaders must avoid overgeneralizing from weak evidence. At the same time, leadership judgment is needed because the highest level of evidence may not always be available, ethical, feasible, or directly applicable to the local context.
The GRADE Evidence to Decision framework is useful in this regard. It was developed to support health system and public health decisions by moving from evidence to decision through structured steps: formulating the question, making evidence-informed assessments, and drawing conclusions
. This approach recognizes that policy decisions require more than effect estimates. Leaders must consider benefits, harms, certainty of evidence, resource use, feasibility, equity, acceptability, and values.
Thus, research literacy helps leaders avoid two extremes. The first extreme is blind acceptance of any published evidence. The second is rejection of evidence because it is imperfect. A research-literate leader understands uncertainty, weighs evidence proportionately, and makes transparent decisions.
5. Research Literacy and Evidence-Based Public Health Decision-Making
Evidence-based public health involves using the best available evidence to improve population health. It requires integration of scientific evidence, community values, professional expertise, available resources, and implementation realities. The CDC has emphasized that increasing disease rates, limited funding, and expanding scientific knowledge require public health practitioners to use proven strategies to improve population health and sustain resources
| [11] | GRADE Working Group / Moberg J, et al. The GRADE Evidence to Decision Framework for health system and public health decisions. In: GRADE Handbook for Grading Quality of Evidence and Strength of Recommendations. Springer; 2015.
https://doi.org/10.1007/978-3-319-22011-6_13 |
[11]
.
Healthcare leaders influence evidence-based public health at several stages.
First, leaders shape priority setting. Research literacy allows them to distinguish urgent problems from visible but less impactful issues. For example, media attention may focus on a rare disease outbreak, while routine data may show that hypertension, diabetes, antimicrobial resistance, maternal anemia, or childhood malnutrition produces a much larger burden. Leaders need evidence to balance urgency, burden, equity, and feasibility.
Second, leaders influence program design. Evidence-literate leaders can select interventions based on systematic reviews, guidelines, implementation studies, and local data. They can also identify whether an intervention proven in one country or population needs adaptation before local use.
Third, leaders guide resource allocation. Public health budgets are finite. Research literacy helps leaders ask which interventions produce the greatest benefit for the available resources, which populations are most underserved, and which programs should be scaled, redesigned, or discontinued.
Fourth, leaders strengthen monitoring and evaluation. Without evaluation, public health programs may continue for years without knowing whether they are effective. Research literacy allows leaders to build indicators, choose data sources, interpret findings, and use results for improvement.
Finally, leaders communicate evidence. During public health crises, leaders must explain uncertainty clearly. Poor communication can create panic, mistrust, or misinformation. Research-literate leaders can communicate what is known, what is uncertain, what is being done, and why decisions may change as new evidence emerges.
6. Research Literacy as a Leadership Competency
Leadership competency frameworks commonly include communication, collaboration, systems thinking, professionalism, ethics, policy understanding, and strategic management. Research literacy should be placed alongside these competencies because evidence is central to all of them. The Public Health Foundation describes core competencies as a consensus set of knowledge and skills for broad public health practice, including foundational and crosscutting skills for professionals engaged in practice, education, and research
.
Research literacy strengthens at least five leadership domains.
6.1. Strategic Thinking
Strategic healthcare leadership requires the ability to anticipate future needs, evaluate trends, and choose priorities. Research literacy supports strategic thinking by helping leaders interpret burden-of-disease data, population projections, health financing trends, workforce data, and intervention evidence.
6.2. Ethical Decision-Making
Evidence-blind decisions can waste resources and harm populations. Ethical leadership requires using credible evidence, acknowledging uncertainty, avoiding manipulation of data, and ensuring that vulnerable populations are not ignored. Research literacy strengthens ethical accountability.
6.3. Communication and Trust
Public trust increases when leaders can explain decisions clearly and transparently. Leaders who understand evidence can communicate why a program is being changed, why a vaccine is recommended, why a screening program is prioritized, or why a policy must be revised.
6.4. Collaboration with Experts
Healthcare leaders often work with epidemiologists, statisticians, economists, clinicians, program managers, community organizations, and policymakers. Research literacy allows leaders to ask the right questions, understand technical advice, and coordinate multidisciplinary teams.
Figure 2. Research Literacy as a Leadership Competency.
6.5. Learning Health Systems
Modern health systems must continuously learn from data. Research-literate leaders can promote quality improvement, implementation research, health services research, and routine data use. They can transform organizations from reactive service providers into learning systems.
7. Barriers to Research-Literate Leadership
Despite its importance, research literacy is often underdeveloped among healthcare leaders. Several barriers exist.
First, leadership training may emphasize management, finance, and operations more than research methods and statistics. As a result, leaders may depend heavily on technical teams without fully understanding the evidence.
Second, research findings are often communicated in technical language that is difficult for decision-makers to interpret. Academic papers may not clearly explain policy relevance, implementation implications, or resource considerations.
Third, organizational culture may value experience and hierarchy over evidence. In some institutions, decisions are made because “this is how we have always done it,” rather than because data support the practice.
Fourth, time pressure limits careful evidence review. Healthcare leaders often need to act quickly, especially during outbreaks, emergencies, or political crises. In such contexts, structured evidence appraisal systems become even more important.
Fifth, evidence may be unavailable or incomplete in low-resource settings. Local data systems may be weak, and published research from high-income countries may not fully apply to different social and health system contexts. This makes contextual judgment essential
| [13] | Dobbins M, Thomas H, O’Brien MA, Duggan M. The use of systematic reviews in the development of new provincial public health policies in Ontario. Int J Technol Assess Health Care. 2004; 20: 399–404. |
[13]
.
8. Strengthening Research Literacy Among Healthcare Leaders
Research literacy should be developed through formal education, continuing professional development, institutional systems, and practice-based learning.
First, healthcare leadership programs should include applied research methods, biostatistics, epidemiology, program evaluation, implementation science, and evidence-informed policymaking. These subjects should be taught in a practical way, using real health system problems.
Second, organizations should create evidence review processes before major policy or program decisions. Brief evidence summaries, rapid reviews, data dashboards, and decision frameworks can help leaders use evidence efficiently.
Third, leaders should be trained to interpret statistical outputs. They do not need to conduct advanced modeling, but they should understand key concepts such as effect size, confidence intervals, bias, confounding, subgroup analysis, and data visualization.
Fourth, research teams should communicate findings in decision-ready formats. Evidence should be translated into policy briefs, executive summaries, dashboards, and implementation recommendations.
Fifth, organizations should promote a culture of questioning. Leaders should encourage staff to ask: What is the evidence? How strong is it? Does it apply to our population? What are the risks? What does the data show? How will we evaluate impact?
Sixth, evaluation should be embedded into routine program design. The CDC’s program evaluation framework emphasizes systematic evaluation as a way to improve public health programs and strengthen accountability
| [14] | Centers for Disease Control and Prevention. CDC approach to answering program evaluation questions. CDC Evaluation. CDC; 2024. URL: https://www.cdc.gov/evaluation/faq |
[14]
. When evaluation is built from the beginning, leaders can learn during implementation rather than waiting until a program ends.
Research literacy is best understood as a practical leadership competency that links knowledge generation with decision-making. It strengthens the ability of healthcare leaders to move from data to interpretation, from interpretation to action, and from action to evaluation.
The central value of research literacy is that it protects decision-making from avoidable error. In healthcare, error at the leadership level can have population-level consequences. A poorly designed program may waste public money. A weakly evaluated intervention may continue despite no measurable benefit. A policy based on anecdote may ignore vulnerable groups. A misinterpreted statistical finding may cause inappropriate scaling or discontinuation of services. Research literacy reduces these risks.
However, research literacy should not be interpreted narrowly as technical expertise alone. A leader may understand p-values and study designs but still fail to make good decisions if they ignore equity, feasibility, ethics, acceptability, or community context. Therefore, the goal is not purely evidence-based leadership in a mechanical sense, but evidence-informed leadership. Evidence should inform decisions, while leadership judgment integrates social values, resource realities, and public health priorities.
The WHO evidence-informed decision-making approach is particularly relevant because it emphasizes identifying, appraising, and mobilizing evidence for policy and programs rather than simply producing research
| [15] | Yost J, Dobbins M, Traynor R, DeCorby K, Workentine S, Greco L. Tools to support evidence-informed public health decision making. BMC Public Health. 2014; 14: 728.
https://doi.org/10.1186/1471-2458-14-728 |
[15]
. Mobilization is the leadership function. It requires turning research into action.
Another important issue is the relationship between evidence and power. Leaders decide which evidence is considered, whose voices are included, and which outcomes matter. Research literacy should therefore include critical appraisal not only of methods but also of relevance and equity. For example, a program may improve average outcomes but widen inequities if it benefits already advantaged groups more than disadvantaged groups. Research-literate leaders should demand disaggregated data and equity-sensitive evaluation.
Research literacy also supports resilience in health systems. During pandemics, outbreaks, climate-related disasters, and economic crises, leaders must interpret rapidly changing evidence. They must distinguish preliminary findings from established knowledge, balance urgency with uncertainty, and update policies as evidence evolves. This requires both technical understanding and intellectual humility
| [16] | Orton L, Lloyd?Williams F, Taylor?Robinson D, O’Flaherty M, Capewell S. The use of research evidence in public health decision making processes: systematic review. PLoS One. 2011; 6(7): e21704. https://doi.org/10.1371/journal.pone.0021704 |
[16]
.
Finally, research literacy promotes institutional learning. Healthcare systems often generate large amounts of routine data, but data do not automatically produce improvement. Leaders must create systems that convert data into insight and insight into action. This includes investing in data quality, encouraging evaluation, supporting research partnerships, and rewarding evidence use
| [17] | Smith EA, Cooper NJ, Sutton AJ, et al. A review of the quantitative effectiveness evidence synthesis methods used in public health intervention guidelines. BMC Public Health. 2021; 21: 278. https://doi.org/10.1186/s12889-021-10162-8 |
[17]
.
9. Conclusion
Research literacy is a core healthcare leadership competency because modern public health decisions must be evidence-informed, transparent, accountable, and context-sensitive. Healthcare leaders do not need to become full-time researchers, but they must be able to understand research questions, interpret quantitative and qualitative evidence, assess study quality, understand basic statistics, recognize uncertainty, and translate findings into policy and practice.
Research methods and statistics provide leaders with tools to identify problems, evaluate interventions, allocate resources, monitor performance, and improve health outcomes. Without these tools, leadership decisions risk becoming reactive, anecdotal, inefficient, and inequitable. With research literacy, healthcare leaders can strengthen evidence-based public health decision-making, build trust, improve accountability, and support learning health systems.
The future of healthcare leadership should therefore place research literacy at the center of professional development. Evidence-informed leadership is not only a scientific requirement; it is an ethical responsibility to patients, communities, and health systems.
Author Contributions
Maleka Sultana: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing
Noman Perves: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Supervision, Validation, Visualization, Writing – original draft
Muzaherul Huq: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Supervision, Validation, Visualization
Anwar Islam: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Supervision, Validation, Visualization, Writing – original draft
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
CDC Foundation. What is public health? CDC Foundation. Accessed June 6, 2026. URL:
https://www.cdcfoundation.org/what-public-health
|
| [2] |
World Health Organization. Evidence, policy, impact: WHO guide for evidence?informed decision?making. Geneva: World Health Organization; 2021. URL:
https://www.who.int/publications/i/item/9789240039872
|
| [3] |
Sanaeifar E, Houshmand E, Moghri J, Vejdani M, Tabatabaee SS. Requirements for evidence?based management competency in healthcare: a scoping review. Front Public Health. 2025; 13: 1490454.
https://doi.org/10.3389/fpubh.2025.1490454
|
| [4] |
Brownson RC, Fielding JE, Maylahn CM. Evidence?based public health: a fundamental concept for public health practice. Annu Rev Public Health. 2009; 30: 175–201.
https://doi.org/10.1146/annurev.publhealth.031308.100134
|
| [5] |
Tenny S, Brannan JM, Brannan GD. Qualitative study. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2022. URL:
https://www.ncbi.nlm.nih.gov/books/NBK470395
|
| [6] |
Guetterman TC, Fetters MD, Creswell JW. Integrating quantitative and qualitative results in health science mixed methods research through joint displays. Ann Fam Med. 2015; 13(6): 554–561.
https://doi.org/10.1370/afm.1865
|
| [7] |
World Health Organization. Health Equity Assessment Toolkit: HEAT and HEAT Plus. Geneva: WHO. Accessed June 6, 2026. URL:
https://www.who.int/data/inequality-monitor/assessment_toolkit
|
| [8] |
Centers for Disease Control and Prevention. CDC approach to program evaluation. CDC; 2024. URL:
https://www.cdc.gov/evaluation/php/about/index.html
|
| [9] |
Murad MH, Asi N, Alsawas M, Alahdab F. New evidence pyramid. BMJ Evid Based Med. 2016; 21(4): 125–127.
https://doi.org/10.1136/ebmed-2016-110401
|
| [10] |
Centers for Disease Control and Prevention. CDC Program Evaluation Framework. CDC; 2024. URL:
https://www.cdc.gov/evaluation/framework
|
| [11] |
GRADE Working Group / Moberg J, et al. The GRADE Evidence to Decision Framework for health system and public health decisions. In: GRADE Handbook for Grading Quality of Evidence and Strength of Recommendations. Springer; 2015.
https://doi.org/10.1007/978-3-319-22011-6_13
|
| [12] |
Public Health Foundation. Core Competencies for Public Health Professionals. Public Health Foundation; 2024. URL:
https://www.phf.org/programs/corepublichealth
|
| [13] |
Dobbins M, Thomas H, O’Brien MA, Duggan M. The use of systematic reviews in the development of new provincial public health policies in Ontario. Int J Technol Assess Health Care. 2004; 20: 399–404.
|
| [14] |
Centers for Disease Control and Prevention. CDC approach to answering program evaluation questions. CDC Evaluation. CDC; 2024. URL:
https://www.cdc.gov/evaluation/faq
|
| [15] |
Yost J, Dobbins M, Traynor R, DeCorby K, Workentine S, Greco L. Tools to support evidence-informed public health decision making. BMC Public Health. 2014; 14: 728.
https://doi.org/10.1186/1471-2458-14-728
|
| [16] |
Orton L, Lloyd?Williams F, Taylor?Robinson D, O’Flaherty M, Capewell S. The use of research evidence in public health decision making processes: systematic review. PLoS One. 2011; 6(7): e21704.
https://doi.org/10.1371/journal.pone.0021704
|
| [17] |
Smith EA, Cooper NJ, Sutton AJ, et al. A review of the quantitative effectiveness evidence synthesis methods used in public health intervention guidelines. BMC Public Health. 2021; 21: 278.
https://doi.org/10.1186/s12889-021-10162-8
|
| [18] |
Achana F, Hubbard S, Sutton A, Kendrick D, Cooper N. An exploration of synthesis methods in public health evaluations of interventions concludes that the use of modern statistical methods would be beneficial. J Clin Epidemiol. 2014 Apr; 67(4): 376-90.
https://doi.org/10.1016/j.jclinepi.2013.09.018
|
Cite This Article
-
APA Style
Sultana, M., Perves, N., Huq, M., Islam, A. (2026). Research Literacy as a Core Healthcare Leadership Competency: Strengthening Evidence-Based Public Health Decision-Making Through Research Methods and Statistics. American Journal of Health Research, 14(4), 179-188. https://doi.org/10.11648/j.ajhr.20261404.11
 Copy
|
Copy
|
 Download
Download
ACS Style
Sultana, M.; Perves, N.; Huq, M.; Islam, A. Research Literacy as a Core Healthcare Leadership Competency: Strengthening Evidence-Based Public Health Decision-Making Through Research Methods and Statistics. Am. J. Health Res. 2026, 14(4), 179-188. doi: 10.11648/j.ajhr.20261404.11
Copy
|
Download
AMA Style
Sultana M, Perves N, Huq M, Islam A. Research Literacy as a Core Healthcare Leadership Competency: Strengthening Evidence-Based Public Health Decision-Making Through Research Methods and Statistics. Am J Health Res. 2026;14(4):179-188. doi: 10.11648/j.ajhr.20261404.11
Copy
|
Download
-
@article{10.11648/j.ajhr.20261404.11,
author = {Maleka Sultana and Noman Perves and Muzaherul Huq and Anwar Islam},
title = {Research Literacy as a Core Healthcare Leadership Competency: Strengthening Evidence-Based Public Health Decision-Making Through Research Methods and Statistics},
journal = {American Journal of Health Research},
volume = {14},
number = {4},
pages = {179-188},
doi = {10.11648/j.ajhr.20261404.11},
url = {https://doi.org/10.11648/j.ajhr.20261404.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajhr.20261404.11},
abstract = {Healthcare leadership increasingly requires more than administrative efficiency, communication skill, and operational oversight. In contemporary public health systems, leaders are expected to interpret evidence, evaluate data quality, understand research designs, assess uncertainty, and translate findings into practical policy and program decisions. This manuscript argues that research literacy should be recognized as a core healthcare leadership competency because evidence-based decision-making depends on leaders’ ability to understand research methods and statistics. Research literacy enables leaders to differentiate strong evidence from weak evidence, interpret quantitative and qualitative findings, evaluate program outcomes, and make transparent decisions in complex health systems. Drawing on principles of research methodology, hierarchy of evidence, epidemiology, program evaluation, and evidence-informed policymaking, the paper discusses how healthcare leaders can use research methods and statistics to improve public health planning, resource allocation, implementation, monitoring, and evaluation. It also highlights the risks of evidence-blind leadership, including inefficient spending, poorly targeted interventions, weak accountability, and preventable health inequities. The paper concludes that research literacy should be embedded in healthcare leadership education, institutional decision-making structures, and continuing professional development. A research-literate healthcare leader is not necessarily a full-time researcher, but must be able to ask answerable questions, critically appraise evidence, interpret statistical findings, engage with technical experts, and translate knowledge into ethical, equitable, and context-sensitive public health action.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Research Literacy as a Core Healthcare Leadership Competency: Strengthening Evidence-Based Public Health Decision-Making Through Research Methods and Statistics
AU - Maleka Sultana
AU - Noman Perves
AU - Muzaherul Huq
AU - Anwar Islam
Y1 - 2026/07/11
PY - 2026
N1 - https://doi.org/10.11648/j.ajhr.20261404.11
DO - 10.11648/j.ajhr.20261404.11
T2 - American Journal of Health Research
JF - American Journal of Health Research
JO - American Journal of Health Research
SP - 179
EP - 188
PB - Science Publishing Group
SN - 2330-8796
UR - https://doi.org/10.11648/j.ajhr.20261404.11
AB - Healthcare leadership increasingly requires more than administrative efficiency, communication skill, and operational oversight. In contemporary public health systems, leaders are expected to interpret evidence, evaluate data quality, understand research designs, assess uncertainty, and translate findings into practical policy and program decisions. This manuscript argues that research literacy should be recognized as a core healthcare leadership competency because evidence-based decision-making depends on leaders’ ability to understand research methods and statistics. Research literacy enables leaders to differentiate strong evidence from weak evidence, interpret quantitative and qualitative findings, evaluate program outcomes, and make transparent decisions in complex health systems. Drawing on principles of research methodology, hierarchy of evidence, epidemiology, program evaluation, and evidence-informed policymaking, the paper discusses how healthcare leaders can use research methods and statistics to improve public health planning, resource allocation, implementation, monitoring, and evaluation. It also highlights the risks of evidence-blind leadership, including inefficient spending, poorly targeted interventions, weak accountability, and preventable health inequities. The paper concludes that research literacy should be embedded in healthcare leadership education, institutional decision-making structures, and continuing professional development. A research-literate healthcare leader is not necessarily a full-time researcher, but must be able to ask answerable questions, critically appraise evidence, interpret statistical findings, engage with technical experts, and translate knowledge into ethical, equitable, and context-sensitive public health action.
VL - 14
IS - 4
ER -
Copy
|
Download