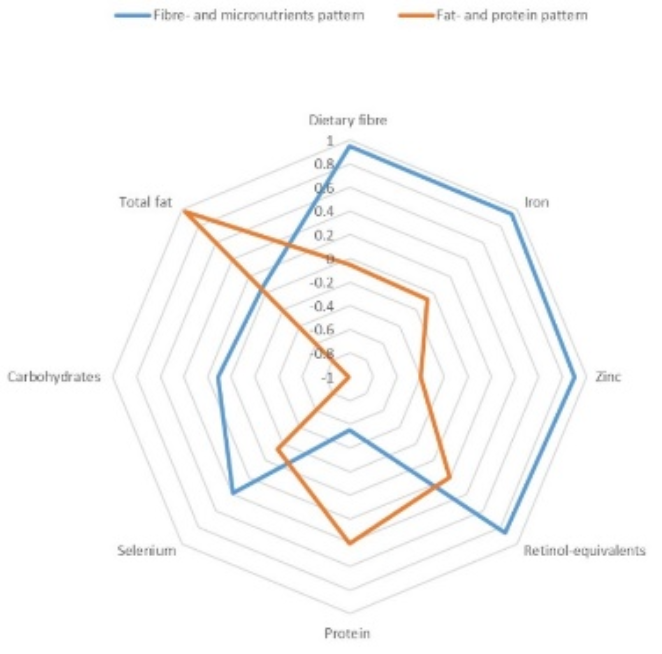
Malaria remains a public health concern among young children in sub-Saharan Africa. Climate change may deplete essential nutrients in major food crops. The impacts of climate-sensitive nutrients on clinical malaria are yet to be established. This study aimed at identifying nutrient patterns and their cross-sectional associations with clinical malaria among young children living in rural Kenya. We used baseline data of a cluster-randomized controlled trial with 506 children aged 6-23 months, recruited within the Siaya Health and Demographic Surveillance System (HDSS) between August and December 2021. We performed physical examinations, malaria microscopy, medical history taking, and questionnaire-based interviews on socio-demographic and dietary variables. Nutrient patterns were derived by Principal Component Analysis (PCA) with orthogonal rotation. Multiple-adjusted logistic regression analyses were used to calculate odds ratios (OR), 95% confidence intervals (CIs), and p-values for the associations of nutrient patterns with clinical malaria (defined as Plasmodium spc. with fever (≥37.5°C) or a history of fever or prescribed anti-malaria medication) and anemia (Hb <11g/dL). In this study population (boys: 54%; mean age: 15.0 ± 5.0 months), 12% had clinical malaria and 73% had anemia. Two nutrient patterns were identified: The fibre- and micronutrient pattern explained 4% of the variation in nutrient intakes, and the fat- and protein pattern explained 2%. Stronger adherence to the fibre- and micronutrient pattern tended to increase the chance of clinical malaria (OR per 1 score-standard deviation increase: 2.18; 95% CI: 0.86, 5.56). There was no association of the fat- and protein pattern with clinical malaria, and both patterns were not associated with anemia. In conclusion, clinical malaria and anemia are common among young children in Siaya County, Kenya. On this background, enhanced availability of climate-sensitive micronutrients may increase their risk of clinical malaria.
| Published in | American Journal of Nursing and Health Sciences (Volume 6, Issue 3) |
| DOI | 10.11648/j.ajnhs.20250603.16 |
| Page(s) | 70-80 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Malaria, Climate Change, Nutrient Patterns, Young Children, Kenya
Characteristics | Total | Malaria | No malaria | p-value |
|---|---|---|---|---|
N | 506 | 60 | 446 | |
Male sex | 53.9 (273) | 48.3 (29) | 54.7 (244) | 0.352 |
Child’s age (months) | 15.0 ± 5.0 | 15.9 ± 5.1 | 14.8 ± 5.0 | 0.123 |
Mother’s age (years) | 29.4 ± 7.8 | 29.0 ± 6.0 | 29.5 ± 8.0 | 0.676 |
Number of people in the household | 6.1 ± 2.2 | 6.4 ± 2.9 | 6.1 ± 2.1 | 0.376 |
Ethnic group, Luo | 95.5 (483) | 93.3 (56) | 95.7 (427) | 0.401 |
Mother’s education | 0.759 | |||
None | 0.6 (3) | 0.0 (0) | 0.7 (3) | |
Primary | 64.4 (322) | 61.4 (35) | 64.8 (287) | |
Secondary | 30.2 (151) | 31.6 (18) | 30.0 (133) | |
Tertiary | 4.8 (24) | 7.0 (4) | 4.5 (20) | |
Mother’s marital status | 0.408 | |||
Married | 80.6 (408) | 76.7 (46) | 81.2 (362) | |
Mother’s religion | 0.602 | |||
Christian | 97.6 (494) | 98.3 (58) | 99.3 (436) | |
Other | 2.4 (12) | 3.3 (2) | 2.2 (10) | |
Energy intake (kcal/d) | 1806 (1280, 2421) | 1815 (1443, 2276) | 1803 (1259, 2436) | 0.788 |
Carbohydrates (energy%) | 61.3 (56.6, 64.8) | 59.5 (56.1, 63.7) | 61.5 (56.9, 64.8) | 0.205 |
Total fat (energy%) | 26.5 (22.5, 30.2) | 27.2 (22.5, 31.3) | 26.4 (22.5, 29.9) | 0.410 |
Protein (energy%) | 12.6 (11.6, 13.6) | 12.8 (11.8, 13.8) | 12.6 (11.6, 13.6) | 0.333 |
Dietary fibre (g/d) | 29.6 (20.4, 37.3) | 30.4 (22.4, 37.6) | 29.5 (20.1, 37.3) | 0.445 |
Iron (mg/d) | 14.6 (10.4, 18.4) | 14.4 (11.1, 18.8) | 14.6 (10.3, 18.3) | 0.607 |
Zinc (mg/d) | 10.9 (7.2, 14.1) | 11.1 (7.4, 13.1) | 10.9 (7.2, 14.2) | 0.837 |
Retinol-eq (µg/d) | 928.6 (607.6, 1314.7) | 963.2 (677.6, 1387.3) | 915.7 (599.7, 1306.2) | 0.389 |
Selenium (µg/d) | 90.5 (57.6, 123.1) | 97.8 (68.7, 125.7) | 89.1 (55.5, 123.1) | 0.217 |
Nutrient pattern | Odds ratios (95% confidence intervals) for clinical malaria | ||||
|---|---|---|---|---|---|
Quintile 1 | Quintile 5 | p-value | per 1 score-SD increase | p-value | |
Fibre- and micronutrients | |||||
Malaria | 10 cases / 90 controls | 15 cases / 87 controls | |||
Crude | 1.00 (reference) | 1.38 (0.73, 2.58) | 0.321 | 1.09 (0.83, 1.42) | 0.530 |
Model 1 | 1.00 (reference) | 1.84 (0.72, 4.66) | 0.202 | 1.76 (0.75, 4.16) | 0.197 |
Model 2 | 1.00 (reference) | 2.24 (0.82, 6.13) | 0.118 | 2.18 (0.86, 5.56) | 0.101 |
Fat- and protein | |||||
Malaria | 12 cases / 88 controls | 15 cases / 86 controls | |||
Crude | 1.00 (reference) | 1.40 (0.74, 2.62) | 0.300 | 1.10 (0.85, 1.43) | 0.467 |
Model 1 | 1.00 (reference) | 1.34 (0.72, 2.60) | 0.338 | 1.08 (0.83, 1.41) | 0.558 |
Model 2 | 1.00 (reference) | 1.49 (0.77, 2.89) | 0.238 | 1.14 (0.87, 1.50) | 0.345 |
Nutrient pattern | Odds ratios (95% confidence intervals) for anemia | ||||
|---|---|---|---|---|---|
Quintile 1 | Quintile 5 | p-value | per 1 score-SD increase | p-value | |
Fibre- and micronutrients | |||||
Anemia | 76 cases / 24 controls | 73 cases / 29 controls | |||
Crude | 1.00 (reference) | 0.90 (0.55, 1.45) | 0.655 | 0.91 (0.75, 1.11) | 0.372 |
Model 1 | 1.00 (reference) | 0.90 (0.45, 1.80) | 0.755 | 0.72 (0.37, 1.41) | 0.340 |
Model 2 | 1.00 (reference) | 1.02 (0.49, 2.11) | 0.964 | 0.77 (0.38, 1.55) | 0.463 |
Fat- and protein | |||||
Anemia | 78 cases / 22 controls | 75 cases / 26 controls | |||
Crude | 1.00 (reference) | 1.06 (0.65, 1.75) | 0.812 | 0.93 (0.77, 1.13) | 0.475 |
Model 1 | 1.00 (reference) | 1.14 (0.68, 1.89) | 0.628 | 0.96 (0.79, 1.17) | 0.700 |
Model 2 | 1.00 (reference) | 1.27 (0.74, 2.18) | 0.382 | 1.00 (0.81, 1.24) | 0.976 |
Characteristics | Fibre- and micronutrients pattern | Fat- and protein pattern | ||
|---|---|---|---|---|
Quintile 1 (n = 95) | Quintile 5 (n = 99) | Quintile 1 (n = 97) | Quintile 5 (n = 94) | |
Demographic and socio-economic | ||||
Mean age ± SD (months) | 11.6 ± 5.1 | 16.6 ± 3.9 | 13.5 ± 5.1 | 15.9 ± 5.2 |
Male sex | 51.6 (49) | 51.5 (51) | 48.5 (47) | 61.7 (58) |
Mean mother’s age ± SD (years) | 29.8 ± 6.6 | 29.1 ± 6.0 | 27.8 ± 6.7 | 29.9 ± 5.4 |
Mean number of people in household ± SD | 6.3 ± 2.0 | 6.4 ± 3.1 | 6.4 ± 2.3 | 6.3 ± 2.8 |
Ethnic group (Luo) | 94.7 (90) | 96.0 (95) | 94.9 (92) | 97.9 (92) |
Mother’s education (primary) | 79.3 (73) | 58.4 (52) | 58.8 (57) | 71.3 (76) |
Mother’s marital status (married) | 87.4 (83) | 86.9 (86) | 76.3 (74) | 77.7 (73) |
Mother’s religion (Christian) | 81.1 (77) | 75.8 (75) | 84.5 (82) | 79.8 (75) |
Dietary | ||||
Energy (kcal/d) | 827 (589, 957) | 2999 (2721, 3274) | 1544 (1123, 2200) | 1719 (1111, 2378) |
Carbohydrates (energy%) | 61.7 (54.6, 65.6) | 61.6 (58.2, 64.4) | 68.5 (67.2, 69.6) | 52.3 (49.0, 54.3) |
Total fat (energy%) | 24.6 (20.9, 30.2) | 26.9 (24.4, 29.9) | 19.4 (17.9, 20.7) | 34.3 (32.4, 37.1) |
Protein (energy%) | 13.8 (12.9, 15.2) | 11.3 (10.6, 12.1) | 12.1 (11.0, 13.0) | 13.3 (12.0, 14.9) |
Dietary fibre (g/d) | 14.0 (10.8, 16.8) | 44.3 (39.6, 49.8) | 25.7 (18.0, 35.4) | 27.0 (16.3, 37.1) |
Iron (mg/d) | 6.7 (4.7, 8.6) | 21.2 (19.7, 23.7) | 12.7 (9.3, 17.5) | 13.1 (8.8, 17.5) |
Zinc (mg/d) | 5.3 (4.0, 6.5) | 16.9 (14.7, 18.4) | 9.4 (6.3, 12.6) | 10.2 (6.7, 14.0) |
Retinol-equivalents (mg/d) | 382.0 (264.8, 477.1) | 1736.3 (1401.7, 2132.1) | 609.6 (411.6, 980.2) | 969.1 (646.6, 1392.9) |
Selenium (µg/d) | 38.4 (26.9, 59.2) | 130.7 (106.1, 151.4) | 93.6 (52.1, 130.5) | 82.1 (48.2, 114.2) |
Malaria-related | ||||
Fever (T ≥37.5°C) | 3.2 (3) | 3.0 (3) | 1.0 (1) | 3.2 (3) |
History of fever (positive) | 40.0 (38) | 41.4 (41) | 40.2 (39) | 40.4 (38) |
Anemia (Hb < 11 g/dL) | 76.8 (73) | 72.7 (72) | 79.4 (77) | 75.5 (71) |
Anemia (Hb < 10 g/dL) | 37.9 (36) | 41.4 (41) | 38.1 (37) | 37.2 (35) |
Malarial anemia (positive) | 4.2 (4) | 6.1 (6) | 2.1 (2) | 11.7 (11) |
Malaria infection (positive) | 5.3 (5) | 6.1 (6) | 3.1 (3) | 12.8 (12) |
Clinical malaria (positive) | 10.5 (10) | 14.1 (15) | 10.3 (12) | 16.0 (15) |
| [1] | World Health Organization (WHO). World malaria report 2022. Geneva: World Health Organization; 2022. |
| [2] | Division of National Malaria Programme (DNMP) [Kenya] and ICF. Kenya Malaria Indicator Survey 2020. Nairobi, Kenya and Rockville, Maryland, USA: DNMP and ICF; 2021. |
| [3] |
UNCEF, WHO, World Bank Group. Joint Malnutrition Estimates, May 2022 Edition. Available from:
https://data.unicef.org/resources/dataset/malnutrition-data/ [Accessed 07 November 2023]. |
| [4] | Sestito, P., Velásquez, S. R., Orel, E., Keiser, O. The COVID-19 pandemic and child malnutrition in sub-Saharan Africa: A scoping review. medRxiv. 2021, 2021.07.21.21260929. |
| [5] | Smith, M. R., Myers, S. S. Impact of anthropogenic CO2 emissions on global human nutrition. Nature Climate Change. 2018, 8, 834-839. |
| [6] |
UNICEF. Nutrition in Kenya – Preventing and treating maternal, adolescent and child malnutrition. Available from:
https://www.unicef.org/kenya/nutrition [Accessed 07 November 2023]. |
| [7] | Nyakeriga, A. M., Troye-Blomberg, M., Chemtai, A. K., Marsh, K., Williams, T. N. Malaria and nutritional status in children living on the coast of Kenya. Am J Clin Nutr. 2004, 80(6), 1604-1610. |
| [8] | Das, D., Grais, R. F., Okiro, E. A., Stepniewska, K., Mansoor, R., van der Kam, S., Terlouw, D. J., Tarning, J., Barnes, K. I., Guerin, P. J. Complex interactions between malaria and malnutrition: a systematic literature review. BMC Med. 2018, 16(1), 186. |
| [9] |
World Health Organization (WHO). Daily Iron Supplementation in Adult Women and Adolescent Girls. Available from:
http://www.Who.Int/nutrition/publications/micronutrients/guidelines/daily_iron_supp_womenandgirls/en/ [Accessed 31 May 2017]. |
| [10] | World Health Organization (WHO). Conclusions and recommendations of the WHO Consultation on prevention and control of iron deficiency in infants and young children in malaria-endemic areas. Food Nutr Bull. 2007, 28(4 Suppl), S621-627. |
| [11] | Basnet, S., Mathisen, M., Strand, T. A. Oral zinc and common childhood infections – An update. J Trace Elem Med Biol. 2015, 31, 163-166. |
| [12] |
Kenya National Bureau of Statistics (KNBS). Leading Economic Indicators 2019. Available from:
https://www.knbs.or.ke [Accessed 08 November 2023]. |
| [13] | Mank, I., Sorgho, R., Zerbo, F., Kagoné, M., Coulibaly, B., Oguso, J., Mbata, M., Khagayi, S., Muok, M. O. E., Sié, A., Danquah, I. ALIMUS – We are feeding! Study protocol of a multi-center, cluster-randomized controlled trial on the effects of a home garden and nutrition counselling intervention to reduce child undernutrition in rural Burkina Faso and Kenya. Trials. 2022, 23, 449. |
| [14] | Galbete, C., Nicolaou, M., Meeks, K. A., de Graft Aikins, A., Addo, J., Amoah, S. K., Smeeth, L., Owusu-Dabo, E., Klipstein-Grobusch, K., Bahendeka, S., Agyemang, C., Mockenhaupt, F. P., Beune, E. J., Stronks, K., Schulze, M. B., Danquah, I. Food consumption, nutrient intake, and dietary patterns in Ghanaian migrants in Europe and their compatriots in Ghana. Food Nutr Res. 2017, 61, 1341809. |
| [15] |
Food and Agriculture Organization (FAO) and Government of Kenya. Kenya Food Composition Tables 2018. Available from:
http://www.fao.org/3/I9120EN/i9120en.pdf [Accessed 08 November 2023]. |
| [16] | Enock, M., Langat, B., Kinyari, T., Igunza, P., Apat, D., Kimori, J., Carter, J., Kiplimo, R., Muhula, S. Implementation of community case management of malaria in malaria endemic counties of western Kenya: are community health volunteers up to the task in diagnosing malaria? Malaria Journal. 2022, 21, 73. |
| [17] | Milner, E. M., Kariger, P., Pickering, A. J., Stewart, C. P., Byrd, K., Lin, A., Rao, G., Achando, B., Dentz, H. N., Null, C., & Fernald, L. C. H. Association between Malaria Infection and Early Childhood Development Mediated by Anemia in Rural Kenya. International Journal of Environmental Research and Public Health. 2020, 17(3), 902. |
| [18] | Chilanga, E., Collin-Vézina, D., MacIntosh, H., Mitchell, C., & Cherney, K. Prevalence and determinants of malaria infection among children of local farmers in Central Malawi. Malaria Journal. 2020, 19(1), 308. |
| [19] | FAO/WHO. Human vitamin and mineral requirements. Report of a Joint FAO/WHO Expert Consultation. Rome: 2002. |
| [20] | Mbagaya, G. M. Child feeding practices in a rural western Kenya community. African Journal of Primary Healthcare & Family Medicine. 2009, 1(1). |
| [21] | Sazawal, S., Black, R. E., Ramsan, M., Chwaya, H. M., Stoltzfus, R. J., Dutta, A., Dhingra, U., Kabole, I., Deb, S., Othman, M. K., Kabole, F. M. Effects of routine prophylactic supplementation with iron and folic acid on admission to hospital and mortality in preschool children in a high malaria transmission setting: community-based, randomized, placebo-controlled trial. Lancet. 2006, 367(9505), 133-143. |
| [22] | Zlotkin, S., Newton, S., Aimone, A. M., Azindow, I., Amenga-Etego, S., Tchum, K., Mahama, E., Thorpe, K. E., Owusu-Agyei, S. Effect of iron fortification on malaria incidence in infants and young children in Ghana: a randomized trial. JAMA. 2013, 310(9), 938-947. |
| [23] | Weiss G. Iron and immunity: a double-edged sword. Eur J Clin Invest. 2002, 32(suppl 1), 70-78. |
| [24] | Skalny, A. V., Aschner, M., Tinkov, A. A. Zinc. Adv Food Nutr Res. 2021, 96, 251-310. |
| [25] | Yakoob, M. Y., Theodoratou, E., Jabeen, A., Imdad, A., Eisele, T. P., Ferguson, J., Jhass, A., Rudan, I., Campbell, H., Black, R. E., Bhutta, Z. A. Preventive zinc supplementation in developing countries: impact on mortality and morbidity due to diarrhea, pneumonia and malaria. BMC Public Health. 2011, 11(S3), S23. |
| [26] | Lynch, S., Pfeiffer, C. M., Georgieff, M. K., Brittenham, G., Fairweather-Tait, S., Hurrell, R. F., McArdle, H. J., Raiten, D. J. Biomarkers of Nutrition for Development (BOND)-Iron review. J Nutr. 2018, 148, 1001S-1067S. |
| [27] | Knez, M., Boy, E. Existing knowledge on Zn status biomarkers (1963 – 2021) with a particular focus on FADS1 and FADS2 diagnostic performance and recommendations for further research. Front Nutr. 2023, 9, 1057156. |
| [28] | Heckl, C., Eisel, M., Lang, A., Homann, C., Paal, M., Vogeser, M., Rühm, A., Sroka, R. Spectroscopic methods to quantify molecules of the heme-biosynthesis pathway: A review of laboratory work and point-of-care approaches. Translational Biophotonics. 2021, 3: e202000026. |
| [29] | Mishra, O. P., Agarwal, K. N., Agarwal, R. M. Salivary iron status in children with iron deficiency and iron overload. J Trop Pediatr. 1992, 38(2), 64-7. |
APA Style
Mbata, M., Angira, C., Awandu, S., Oguso, J., Okinyo, A., et al. (2025). Nutrient Patterns and Their Associations with Clinical Malaria Among Children Aged 6-23 Months in Siaya County, Kenya: A Cross-sectional Analysis. American Journal of Nursing and Health Sciences, 6(3), 70-80. https://doi.org/10.11648/j.ajnhs.20250603.16
ACS Style
Mbata, M.; Angira, C.; Awandu, S.; Oguso, J.; Okinyo, A., et al. Nutrient Patterns and Their Associations with Clinical Malaria Among Children Aged 6-23 Months in Siaya County, Kenya: A Cross-sectional Analysis. Am. J. Nurs. Health Sci. 2025, 6(3), 70-80. doi: 10.11648/j.ajnhs.20250603.16
AMA Style
Mbata M, Angira C, Awandu S, Oguso J, Okinyo A, et al. Nutrient Patterns and Their Associations with Clinical Malaria Among Children Aged 6-23 Months in Siaya County, Kenya: A Cross-sectional Analysis. Am J Nurs Health Sci. 2025;6(3):70-80. doi: 10.11648/j.ajnhs.20250603.16
@article{10.11648/j.ajnhs.20250603.16,
author = {Michael Mbata and Charles Angira and Shehu Awandu and John Oguso and Austine Okinyo and Isaac Okeyo and Erick Muok},
title = {Nutrient Patterns and Their Associations with Clinical Malaria Among Children Aged 6-23 Months in Siaya County, Kenya: A Cross-sectional Analysis
},
journal = {American Journal of Nursing and Health Sciences},
volume = {6},
number = {3},
pages = {70-80},
doi = {10.11648/j.ajnhs.20250603.16},
url = {https://doi.org/10.11648/j.ajnhs.20250603.16},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajnhs.20250603.16},
abstract = {Malaria remains a public health concern among young children in sub-Saharan Africa. Climate change may deplete essential nutrients in major food crops. The impacts of climate-sensitive nutrients on clinical malaria are yet to be established. This study aimed at identifying nutrient patterns and their cross-sectional associations with clinical malaria among young children living in rural Kenya. We used baseline data of a cluster-randomized controlled trial with 506 children aged 6-23 months, recruited within the Siaya Health and Demographic Surveillance System (HDSS) between August and December 2021. We performed physical examinations, malaria microscopy, medical history taking, and questionnaire-based interviews on socio-demographic and dietary variables. Nutrient patterns were derived by Principal Component Analysis (PCA) with orthogonal rotation. Multiple-adjusted logistic regression analyses were used to calculate odds ratios (OR), 95% confidence intervals (CIs), and p-values for the associations of nutrient patterns with clinical malaria (defined as Plasmodium spc. with fever (≥37.5°C) or a history of fever or prescribed anti-malaria medication) and anemia (Hb <11g/dL). In this study population (boys: 54%; mean age: 15.0 ± 5.0 months), 12% had clinical malaria and 73% had anemia. Two nutrient patterns were identified: The fibre- and micronutrient pattern explained 4% of the variation in nutrient intakes, and the fat- and protein pattern explained 2%. Stronger adherence to the fibre- and micronutrient pattern tended to increase the chance of clinical malaria (OR per 1 score-standard deviation increase: 2.18; 95% CI: 0.86, 5.56). There was no association of the fat- and protein pattern with clinical malaria, and both patterns were not associated with anemia. In conclusion, clinical malaria and anemia are common among young children in Siaya County, Kenya. On this background, enhanced availability of climate-sensitive micronutrients may increase their risk of clinical malaria.
},
year = {2025}
}
TY - JOUR T1 - Nutrient Patterns and Their Associations with Clinical Malaria Among Children Aged 6-23 Months in Siaya County, Kenya: A Cross-sectional Analysis AU - Michael Mbata AU - Charles Angira AU - Shehu Awandu AU - John Oguso AU - Austine Okinyo AU - Isaac Okeyo AU - Erick Muok Y1 - 2025/09/19 PY - 2025 N1 - https://doi.org/10.11648/j.ajnhs.20250603.16 DO - 10.11648/j.ajnhs.20250603.16 T2 - American Journal of Nursing and Health Sciences JF - American Journal of Nursing and Health Sciences JO - American Journal of Nursing and Health Sciences SP - 70 EP - 80 PB - Science Publishing Group SN - 2994-7227 UR - https://doi.org/10.11648/j.ajnhs.20250603.16 AB - Malaria remains a public health concern among young children in sub-Saharan Africa. Climate change may deplete essential nutrients in major food crops. The impacts of climate-sensitive nutrients on clinical malaria are yet to be established. This study aimed at identifying nutrient patterns and their cross-sectional associations with clinical malaria among young children living in rural Kenya. We used baseline data of a cluster-randomized controlled trial with 506 children aged 6-23 months, recruited within the Siaya Health and Demographic Surveillance System (HDSS) between August and December 2021. We performed physical examinations, malaria microscopy, medical history taking, and questionnaire-based interviews on socio-demographic and dietary variables. Nutrient patterns were derived by Principal Component Analysis (PCA) with orthogonal rotation. Multiple-adjusted logistic regression analyses were used to calculate odds ratios (OR), 95% confidence intervals (CIs), and p-values for the associations of nutrient patterns with clinical malaria (defined as Plasmodium spc. with fever (≥37.5°C) or a history of fever or prescribed anti-malaria medication) and anemia (Hb <11g/dL). In this study population (boys: 54%; mean age: 15.0 ± 5.0 months), 12% had clinical malaria and 73% had anemia. Two nutrient patterns were identified: The fibre- and micronutrient pattern explained 4% of the variation in nutrient intakes, and the fat- and protein pattern explained 2%. Stronger adherence to the fibre- and micronutrient pattern tended to increase the chance of clinical malaria (OR per 1 score-standard deviation increase: 2.18; 95% CI: 0.86, 5.56). There was no association of the fat- and protein pattern with clinical malaria, and both patterns were not associated with anemia. In conclusion, clinical malaria and anemia are common among young children in Siaya County, Kenya. On this background, enhanced availability of climate-sensitive micronutrients may increase their risk of clinical malaria. VL - 6 IS - 3 ER -
Department of Biomedical Service, Jaramogi Oginga Odinga University of Science and Technology (JOOUST), Bondo, Kenya; Center for Global Health Research (CGHR), Kenya Medical Research Institute (KEMRI), Kisumu, Kenya
Department of Biomedical Service, Jaramogi Oginga Odinga University of Science and Technology (JOOUST), Bondo, Kenya
Department of Biomedical Service, Jaramogi Oginga Odinga University of Science and Technology (JOOUST), Bondo, Kenya
Center for Global Health Research (CGHR), Kenya Medical Research Institute (KEMRI), Kisumu, Kenya
Center for Global Health Research (CGHR), Kenya Medical Research Institute (KEMRI), Kisumu, Kenya
Department of Health and Biomedical Sciences, The Technical University of Kenya, Nairobi, Kenya
Center for Global Health Research (CGHR), Kenya Medical Research Institute (KEMRI), Kisumu, Kenya
Information