Maternal healthcare utilization remains suboptimal in Nigeria, with persistent socioeconomic and geographical disparities undermining progress toward reducing maternal morbidity and mortality. This study aims to assess the geographical and socioeconomic inequalities of maternal healthcare utilization in Nigeria. Maternal healthcare utilization in Nigeria remains suboptimal, with persistent socioeconomic and geographical disparities hindering progress in reducing maternal morbidity and mortality. This study assessed inequalities in the utilization of antenatal care (ANC4+), facility-based delivery (FBD), and postnatal care (PNC) using data from the 2018 Nigeria Demographic and Health Survey. Socioeconomic inequalities were examined using Erreygers Normalized Concentration Indices (ENCI) and concentration curves disaggregated by region and residence, while decomposition analysis identified key drivers. Findings revealed significant pro-rich inequalities across all services. Facility-based delivery showed the widest gaps (urban ENCI = 0.295; rural = 0.121), particularly in the Northwest (0.398) and Northeast (0.254). ANC4+ visits displayed moderate inequality, highest in the Northwest (0.169). PNC showed minimal inequality, with ENCI values near zero. Wealth status was the strongest contributor to inequality, supported by education, parity, and religion, while age, marital status, employment, autonomy, and insurance played minor roles. Although overall utilization was higher in urban areas, inequality was more pronounced there, highlighting deep intra-urban socioeconomic divides. Substantial socioeconomic and geographic inequities persist in maternal healthcare utilization in Nigeria. Targeted interventions addressing financial, educational, and sociocultural barriers, especially in northern and urban-poor populations, are crucial to narrowing gaps and improving maternal outcomes.
| Published in | Biomedical Statistics and Informatics (Volume 11, Issue 1) |
| DOI | 10.11648/j.bsi.20261101.12 |
| Page(s) | 14-30 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Maternal Healthcare, Socio-economic Inequalities, Geographical Disparities, Nigeria
Variables | Frequency (%) |
|---|---|
Age Group (years) | |
15 – 19 | 8423 (20.14) |
20 – 24 | 6844 (16.36) |
25 – 29 | 7203 (17.22) |
30 – 34 | 5997 (14.34) |
35 – 39 | 5406 (12.93) |
40 – 49 | 7948 (19.00) |
Educational Level | |
No Education | 14398 (34.43) |
Primary | 6383 (15.26) |
Secondary | 16698 (39.93) |
Higher | 4342 (10.38) |
Marital Status | |
Never Married | 10669 (25.51) |
Married/Living together | 28888 (69.08) |
Widowed/Divorced/Separated | 2264 (5.41) |
Employment Status | |
Unemployed | 14766 (35.31) |
Employed | 27055 (64.69) |
Parity | |
1 – 2 | 9408 (31.37) |
3 – 4 | 8493 (28.32) |
5+ | 12091 (40.31) |
Religion | |
Christian | 20506 (49.03) |
Muslim | 20959 (50.12) |
Other | 356 (0.85) |
Place of Residence | |
Urban | 24837 (59.39) |
Rural | 16984 (40.61) |
Region | |
North Central | 7772 (18.58) |
North-East | 7639 (18.27) |
North-West | 10129 (24.22) |
South-East | 5571 (13.32) |
South-South | 5080 (12.15) |
South-West | 5630 (13.46) |
Wealth Index | |
Poorest/Poorer | 16093 (38.48) |
Middle | 8859 (21.18) |
Richer/Richest | 16869 (40.34) |
Media Exposure | |
None/Less than weekly | 24130 (57.70) |
At least weekly | 17691 (42.30) |
Decision Autonomy | |
No autonomy | 16210 (56.11) |
Has autonomy | 12678 (43.89) |
Insurance | |
Not covered | 40704 (97.33) |
Covered | 1117 (2.67) |
Variables | Ante-Natal Care | Facility-Based Delivery | Post-Natal Care | |||
|---|---|---|---|---|---|---|
Index Value (Std Error) | Z-stat (P-value) | Index Value (Std Error) | Z-stat (P-value) | Index Value (Std Error) | Z-stat (P-value) | |
Place of Residence | 18.67 (<0.001) | 24.22 (<0.001) | 2.06 (0.0394) | |||
Urban | 0.163 (0.004)* | 0.295 (0.006)* | 0.020 (0.004)* | |||
Rural | 0.068 (0.003)* | 0.121 (0.004)* | 0.009 (0.002)* | |||
Region | 63.33 (<0.001) | 131.39 (<0.001) | 3.56 (0.0033) | |||
North Central | 0.157 (0.007)* | 0.168 (0.008)* | 0.035 (<0.001)* | |||
North-East | 0.109 (0.008)* | 0.254 (0.011)* | 0.005 (0.008) | |||
North-West | 0.169 (0.007)* | 0.398 (0.013)* | 0.010 (0.007) | |||
South-East | 0.035 (0.004)* | 0.097 (0.004)* | 0.020 (0.005)* | |||
South-South | 0.078 (0.007)* | 0.157 (0.012)* | 0.019 (0.007)* | |||
South-West | 0.030 (0.003)* | 0.032 (0.005)* | 0.012 (0.003)* | |||
Variables | Maternal Healthcare | |||||
|---|---|---|---|---|---|---|
Ante-Natal Care | Facility-Based Delivery | Post-Natal Care | ||||
( | % Contr. | ( | % Contr. | ( | % Contr. | |
Age Group | ||||||
15 – 19 yrs | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 |
20 – 24 yrs | - | - | - | - | - | - |
25 – 29 yrs | 0.003 (0.004) | -0.001 | 0.004 (0.002) | -0.0001 | 0.026 (0.005) | -0.001 |
30 – 34 yrs | 0.038 (0.003) | -0.001 | 0.038 (0.001) | -0.0001 | 0.015 (0.006) | -0.0001 |
35 – 39 yrs | 0.021 (0.003) | -0.0001 | 0.029 (0.001) | -0.0001 | 0.002 (0.004) | -0.0001 |
40 – 49 yrs | -0.005 (0.002) | 0.00001 | -0.008 (0.001) | 0.00001 | -0.030 (0.002) | -0.001 |
Educational Level | ||||||
No Education | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 |
Primary | -0.0001 (-0.001) | 0.00001 | -0.0001 (0.0001) | -0.0001 | -0.0001 (0.008) | 0.001 |
Secondary | -0.005 (0.003) | -0.002 | -0.005 (0.009) | -0.006 | -0.0001 (0.027) | -0.001 |
Higher | -0.004 (0.001) | -0.001 | -0.004 (0.005) | -0.004 | -0.001 (0.008) | -0.004 |
Marital Status | ||||||
Never Married | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 |
Married/Living together | 0.0001 (0.0001) | 0.0001 | 0.0001 (0.0001) | 0.0001 | 0.0001 (0.0001) | 0.0001 |
Widowed/Divorced/Separated | 0.0001 (0.0001) | 0.0001 | 0.0001 (0.0001) | 0.0001 | 0.0001 (0.0001) | 0.0001 |
Employment Status | ||||||
Unemployed | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 |
Employed | -0.003 (-0.0001) | 0.0001 | -0.003 (-0.0001) | 0.0001 | -0.001 (-0.011) | 0.0001 |
Parity | ||||||
1 – 2 | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 |
3 – 4 | -0.002 (0.031) | -0.003 | -0.002 (0.035) | -0.005 | -0.001 (0.002) | 0.0001 |
5+ | 0.007 (0.026) | 0.010 | 0.007 (0.025) | 0.014 | 0.001 (0.0001) | 0.0001 |
Religion | ||||||
Christian | -0.006 (-0.030) | 0.017 | -0.0001 (-0.013) | 0.008 | -0.0001 (-0.018) | 0.001 |
Muslim | 0.003 (-0.026) | -0.016 | -0.002 (-0.009) | -0.009 | 0.0001 (0.001) | 0.0001 |
Other | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 |
Place of Residence | ||||||
Urban | -0.001 (0.003) | -0.002 | -0.001 (-0.0001) | 0.0001 | -0.001 (0.007) | -0.002 |
Rural | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 |
Region | ||||||
North Central | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 |
North-East | -0.001 (-0.001) | -0.001 | -0.001 (-0.0001) | 0.0001 | -0.0001 (-0.004) | -0.002 |
North-West | -0.001 (-0.002) | -0.001 | -0.003 (0.001) | 0.002 | -0.0001 (-0.002) | 0.0001 |
South-East | 0.001 (-0.003) | 0.003 | 0.002 (-0.001) | 0.001 | 0.0001 (0.001) | -0.0001 |
South-South | 0.0001 (-0.0001) | 0.0001 | 0.0001 (-0.0001) | 0.0001 | -0.0001 (-0.0001) | -0.0001 |
South-West | -0.001 (0.002) | 0.001 | -0.001 (0.002) | -0.002 | -0.0001 (-0.003) | 0.001 |
Wealth Index | ||||||
Poorest/Poorer | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 |
Middle | -0.001 (-0.003) | 0.001 | -0.001 (-0.005) | 0.001 | 0.001 (-0.004) | -0.0001 |
Richer/Richest | -0.005 (-0.006) | 0.004 | -0.012 (-0.016) | 0.011 | -0.004 (-0.014) | 0.003 |
Media Exposure | ||||||
None/Less than weekly | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 |
At least weekly | -0.0001 (0.002) | -0.001 | -0.0001 (0.0001) | -0.0001 | -0.0001 (-0.001) | 0.0001 |
Decision Autonomy | ||||||
No autonomy | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 |
Has autonomy | -0.0001 (0.0001) | -0.0001 | -0.0001 (0.001) | -0.0001 | -0.0001 (-0.003) | 0.0001 |
Insurance | ||||||
Not covered | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 |
Covered | -0.0001 (-0.0001) | 0.0001 | -0.0001 (-0.001) | 0.0001 | -0.0001 (-0.0001) | 0.0001 |
Total | 0.038 (-0.010) | 0.008 | 0.036 (-0.001) | 0.010 | 0.016 (0.001) | -0.001 |
ANC | Antenatal Care |
FBD | Facility-Based Delivery |
PNC | Postnatal Care |
NDHS | Nigeria Demographic and Health Survey |
WHO | World Health Organisation |
SDG | Sustainable Development Goal |
LMICs | Low and Middle Income Countries |
UN | United Nation |
BGV | Between-group Variance |
ECI | Erreygers-corrected Concentration Index |
| [1] | Adatara, P., Strumpher, J., Ricks, E., & Mwini-Nyaledzigbor, P. P. (2019). Cultural beliefs and practices of women influencing home births in rural Northern Ghana. International journal of women's health, 11, 353–361. |
| [2] | Adedokun, S. T., & Uthman, O. A. (2022). Women’s autonomy and maternal healthcare utilization in Nigeria: Evidence from the 2018 NDHS. BMJ Global Health, 7(4), e008123. |
| [3] | Adewuyi, E. O., Auta, A., Adewuyi, M. I., Philip, A. A., Olutuase, V., Zhao, Y., & Khanal, V. (2024). Antenatal care utilization and receipt of its components in Nigeria: Assessing disparities between rural and urban areas-A nationwide population-based study. PloS one, 19(7), e0307316. |
| [4] | Adejoorin, M. V., Salman, K. K., Adenegan, K. O., Obi-Egbedi, O., Dairo, M. D., & Omotayo, A. O. (2024). Utilization of maternal health facilities and rural women's well-being: towards the attainment of sustainable development goals. Health economics review, 14(1), 40. |
| [5] | Adeyanju, O., Tubeuf, S., & Ensor, T. (2021). Socioeconomic inequalities in maternal healthcare utilization in Nigeria: Evidence from 2003–2018 Demographic and Health Surveys. Health Policy and Planning, 36(6), 839–849. |
| [6] | Adjiwanou, V., & LeGrand, T. (2014). Gender inequality and the use of maternal healthcare services in rural sub-Saharan Africa. Health & place, 29, 67-78. |
| [7] | Afape, A. O., Azubuike, P. C., Ibikunle, O. O., & Barrow, A. (2024). Prevalence and determinants of skilled birth attendance among young women aged 15-24 years in Northern Nigeria: evidence from Multiple Indicator Cluster Survey 2011 to 2021. BMC public health, 24(1), 2471. |
| [8] | Akinyemi, Y. C. (2021). Spatiotemporal patterns and determinants of reproductive health care utilization in Nigeria: 2008–2018. Papers in Applied Geography, 7(4), 453-481. |
| [9] | Alam, C. E., Abou-Abbas, L., Ramadan, M. S., & Asmar, M. K. (2025). Exploring the barriers to accessing antenatal care at the primary health care center level of a tertiary hospital in Lebanon: a qualitative study. BMC Health Services Research, 25(1), 1-14. |
| [10] | Ali, B., & Chauhan, S. (2020). Inequalities in the utilization of maternal health Care in Rural India: Evidences from National Family Health Survey III & IV. BMC public health, 20(1), 369. |
| [11] | Alibhai, K. M., Ziegler, B. R., Meddings, L., Batung, E., & Luginaah, I. (2022). Factors impacting antenatal care utilization: a systematic review of 37 fragile and conflict-affected situations. Conflict and health, 16(1), 33. |
| [12] | Al-Mujtaba, M., Sam-Agudu, N. A., & Khatri, R. (2022). Impact of insecurity on maternal healthcare access in northern Nigeria: A mixed-methods study. BMC Health Services Research, 22(1), 987. |
| [13] | Anindya, K., Marthias, T., Vellakkal, S., Carvalho, N., Atun, R., Morgan, A., & Lee, J. T. (2021). Socioeconomic inequalities in effective service coverage for reproductive, maternal, newborn, and child health: a comparative analysis of 39 low-income and middle-income countries. E Clinical Medicine, 40. |
| [14] | Asefa, A., Gebremedhin, S., Marthias, T., Nababan, H., Christou, A., Semaan, A., & Beňová, L. (2023). Wealth-based inequality in the continuum of maternal health service utilization in 16 sub-Saharan African countries. International journal for equity in health, 22(1), 203. |
| [15] | Biswas, B., Kumar, N., Rahaman, M. M., Das, S., & Hoque, M. A. (2024). Socioeconomic inequality and urban-rural disparity of antenatal care visits in Bangladesh: A trend and decomposition analysis. Plos one, 19(3), e0301106. |
| [16] | Bobo, F. T., Asante, A., Woldie, M., Dawson, A., & Hayen, A. (2021). Spatial patterns and inequalities in skilled birth attendance and caesarean delivery in sub-Saharan Africa. BMJ global health, 6(10), e007074. |
| [17] | Chi, H., Jung, S., Subramanian, S. V., & Kim, R. (2024). Socioeconomic and geographic inequalities in antenatal and postnatal care components in India, 2016-2021. Scientific reports, 14(1), 10221. |
| [18] | Dickson, K. S., Ayebeng, C., Adu-Gyamfi, A. B., & Okyere, J. (2023). Postnatal care service utilization for babies within the first two months after childbirth: an analysis of rural-urban differences in eleven Sub-Saharan African countries. BMC pregnancy and childbirth, 23(1), 423. |
| [19] | Doctor, H. V., & Dahiru, T. (2020). Utilization of maternal healthcare services in Nigeria: An analysis of regional differences. African Population Studies, 34(1), 23–39. |
| [20] | Dowhaniuk, N. (2021). Exploring country-wide equitable government health care facility access in Uganda. International journal for equity in health, 20(1), 38. |
| [21] | Dzomeku, V. M., Duodu, P. A., Okyere, J., Aduse-Poku, L., Dey, N. E. Y., Mensah, A. B. B., Nakua, E. K., Agbadi, P., & Nutor, J. J. (2021). Prevalence, progress, and social inequalities of home deliveries in Ghana from 2006 to 2018: insights from the multiple indicator cluster surveys. BMC pregnancy and childbirth, 21(1), 518. |
| [22] | Exley, J., Pitchforth, E., Okeke, E., Glick, P., Abubakar, I. S., Chari, A., & Onwujekwe, O. (2016). Persistent barriers to care; a qualitative study to understand women’s experiences in areas served by the midwives service scheme in Nigeria. BMC Pregnancy and Childbirth, 16(1), 232. |
| [23] | Fagbamigbe, A. F., & Idemudia, E. S. (2017). Wealth and antenatal care utilization in Nigeria: policy implications. Health care for women international, 38(1), 17-37. |
| [24] | Fagbamigbe, A. F., Idemudia, E. S., & Adebowale, A. S. (2023). Spatial and socioeconomic inequalities in maternal healthcare utilization in Nigeria: Evidence from the 2018 NDHS. PLoS ONE, 18(4), e0284267. |
| [25] | Federal Ministry of Health. (2023). Nigeria Health Sector Strategic Plan 2023–2027. Abuja: Federal Ministry of Health. |
| [26] | Fetene, S. M., Fentie, E. A., Shewarega, E. S., & Kidie, A. A. (2024). Socioeconomic inequality in postnatal care utilization among reproductive age women in sub-Saharan African countries with high maternal mortality: a decomposition analysis. BMJ open, 14(10), e076453. |
| [27] | Gu, D., Andreev, K., & Dupre, M. E. (2021). Major Trends in Population Growth Around the World. China CDC weekly, 3(28), 604–613. |
| [28] | Imo, C. K. (2022). Influence of women's decision-making autonomy on antenatal care utilization and institutional delivery services in Nigeria: evidence from the Nigeria Demographic and Health Survey 2018. BMC Pregnancy and Childbirth, 22(1), 141. |
| [29] | Kurji, J. (2021). Assessing the determinants of maternal healthcare service utilization and effectiveness of interventions to improve institutional births in Jimma Zone, Ethiopia (Doctoral dissertation, Université d'Ottawa/University of Ottawa). |
| [30] | Kruk, M. E., Gage, A. D., & Arsenault, C. (2022). High-quality health systems in the Sustainable Development Goals era: Time for a revolution. The Lancet Global Health, 10(3), e347–e355. |
| [31] | Langlois, É. V., Miszkurka, M., Zunzunegui, M. V., Ghaffar, A., Ziegler, D., & Karp, I. (2015). Inequities in postnatal care in low- and middle-income countries: a systematic review and meta-analysis. Bulletin of the World Health Organization, 93(4), 259–270G. |
| [32] | Lateef, M. A., Kuupiel, D., Mchunu, G. G., & Pillay, J. D. (2024). Utilization of Antenatal Care and Skilled Birth Delivery Services in Sub-Saharan Africa: A Systematic Scoping Review. International journal of environmental research and public health, 21(4), 440. |
| [33] | Majumder, K., Sarkar, M., Mallick, R., Mondal, S., & Chouhan, P. (2024). Does women’s decision-making autonomy matter in utilization of antenatal care services in India? An analysis from nationally representative survey. Plos one, 19(8), e0308576. |
| [34] | Maleki, A., Soltani, F., Abasalizadeh, M., & Bakht, R. (2024). Sociodemographic disparities in postnatal care coverage at comprehensive health centers in Hamedan City. Frontiers in public health, 12, 1329787. |
| [35] | Mekonen, A. M., Kebede, N., Dessie, A., Mihret, S., & Tsega, Y. (2024). Wealth disparities in maternal health service utilization among women of reproductive age in Ethiopia: findings from the mini-EDHS 2019. BMC health services research, 24(1), 1034. |
| [36] | Misu, F., Gasbarro, D., & Alam, K. (2025). Inequality in Utilization of Maternal Healthcare Services in Low? and Middle-Income Countries: A Scoping Review of the Literature. Maternal and child health journal, 29(6), 741–766. |
| [37] | National Population Commission [NPC] & ICF. (2019). Nigeria Demographic and Health Survey 2018. Abuja, Nigeria, and Rockville, Maryland, USA: NPC and ICF. |
| [38] | Nayeem, J., Stennett, C., Sharmeen, A., Hossain, M. M., & Al Kibria, G. M. (2023). Rural-urban differences in distributions and determinants of facility delivery among women in Bangladesh. Global Health Journal, 7(4), 222-229. |
| [39] | Ntawukuriryayo, J. T., VanderZanden, A., Amberbir, A., Teklu, A., Huda, F. A., Maskey, M., Sall, M., Garcia, P. J., Subedi, R. K., Sayinzoga, F., Hirschhorn, L. R., & Binagwaho, A. (2024). Inequity in the face of success: understanding geographic and wealth-based equity in success of facility-based delivery for under-5 mortality reduction in six countries. BMC pediatrics, 23(Suppl 1), 651. |
| [40] | Ntegwa, M. J., Mcharo, E. G., & Mlay, J. F. (2023). What explains the rural−urban inequalities in maternal health services utilization in Tanzania? A fairlie decomposition analysis. Asian Journal of Social Health and Behavior, 6(2), 47-55. |
| [41] | Nwosu, C. O., & Ataguba, J. E. (2019). Socioeconomic inequalities in maternal health service utilization: a case of antenatal care in Nigeria using a decomposition approach. BMC Public Health, 19(1), 1493. |
| [42] | Okeke, E. N., Abubakar, I. S., & De Allegri, M. (2021). The impact of free maternal healthcare policies in Nigeria: A quasi-experimental study. Health Policy and Planning, 36(7), 1023–1034. |
| [43] | Okeke, E. N., Wagner, Z., & Abubakar, I. S. (2020). Maternal Cash Transfers Led To Increases In Facility Deliveries And Improved Quality Of Delivery Care In Nigeria: Study examines the prevalence of delayed entry, the reasons for the delays, and their effect on Medicaid spending in a recent cohort of brand-name medications. Health Affairs, 39(6), 1051-1059. |
| [44] | Okoli, C., Hajizadeh, M., Rahman, M. M., & Khanam, R. (2020). Geographical and socioeconomic inequalities in the utilization of maternal healthcare services in Nigeria: 2003–2017. BMC Health Services Research, 20(1), 849. |
| [45] | Okonofua, F., Ntoimo, L., & Yaya, S. (2022). Cultural and social barriers to maternal healthcare utilization in rural Nigeria. BMC Pregnancy and Childbirth, 22(1), 345. |
| [46] | Ononokpono, D. N., & Odimegwu, C. O. (2020). Determinants of maternal healthcare utilization in Nigeria: A multilevel approach. Journal of Biosocial Science, 52(4), 567–582. |
| [47] | Ononokpono, D. N., Odimegwu, C. O., Adedini, S. A., & Imasiku, E. N. (2016). Ethnic diversity and maternal health care in Nigeria. Women's Reproductive Health, 3(1), 45-59. |
| [48] | Oyedele, O. K., Fagbamigbe, A. F., Akinyemi, O. J., & Adebowale, A. S. (2023). Coverage-level and predictors of maternity continuum of care in Nigeria: implications for maternal, newborn and child health programming. BMC Pregnancy and Childbirth, 23(1), 36. |
| [49] | Pison, G., Couppié, E., & Caporali, A. (2022). The population of the world, 2022. Population & Societies, 603(8), 1-8. |
| [50] | Ruktanonchai, C. W., Ruktanonchai, N. W., Nove, A., Lopes, S., Pezzulo, C., Bosco, C., & Tatem, A. J. (2016). Equality in maternal and newborn health: modelling geographic disparities in utilization of care in five East African countries. PloS one, 11(8), e0162006. |
| [51] | Samuel, O., Zewotir, T., & North, D. (2021). Decomposing the urban–rural inequalities in the utilization of maternal health care services: evidence from 27 selected countries in Sub-Saharan Africa. Reproductive Health, 18(1), 216. |
| [52] | Say, L., Chou, D., Gemmill, A., Tunçalp, Ö., Moller, A. B., Daniels, J., Gülmezoglu, A. M., Temmerman, M., & Alkema, L. (2014). Global causes of maternal death: a WHO systematic analysis. The Lancet. Global health, 2(6), e323–e333. |
| [53] | Sserwanja, Q., Nuwabaine, L., Kamara, K., & Musaba, M. W. (2022). Prevalence and factors associated with utilization of postnatal care in Sierra Leone: a 2019 national survey. BMC public health, 22(1), 102. |
| [54] | Stephen, A. A., & Odunayo, J. (2016). Determinants of maternal utilization of health services and nutritional status in a rural community in South-West Nigeria. African journal of reproductive health, 20(2), 72-85. |
| [55] | Shanto, H. H., Al-Zubayer, M. A., Ahammed, B., Sarder, M. A., Keramat, S. A., Hashmi, R., Haque, R., & Alam, K. (2023). Maternal Healthcare Services Utilization and Its Associated Risk Factors: A Pooled Study of 37 Low- and Middle-Income Countries. International journal of public health, 68, 1606288. |
| [56] | Tessema, Z. T., Teshale, A. B., Tesema, G. A., & Tamirat, K. S. (2021). Determinants of completing recommended antenatal care utilization in sub-Saharan from 2006 to 2018: evidence from 36 countries using Demographic and Health Surveys. BMC pregnancy and childbirth, 21(1), 192. |
| [57] | United Nations. (2020). The Sustainable Development Goals Report 2020. New York: United Nations. |
| [58] | Wong, K. L., Radovich, E., Owolabi, O. O., Campbell, O. M., Brady, O. J., Lynch, C. A., & Benova, L. (2018). Why not? Understanding the spatial clustering of private facility-based delivery and financial reasons for homebirths in Nigeria. BMC health services research, 18(1), 397. |
| [59] | World Health Organization. (2020a). WHO recommendations on antenatal care for a positive pregnancy experience. Geneva: WHO. |
| [60] | World Health Organization. (2020b). WHO recommendations on postnatal care of the mother and newborn. Geneva: WHO. |
| [61] | World Health Organization. (2022). World Health Statistics 2022: Monitoring health for the SDGs. Geneva: WHO. |
| [62] | World Health Organization. (2023). Trends in Maternal Mortality 2000 to 2020: Estimates by WHO, UNICEF, UNFPA, World Bank Group, and UNDESA/Population Division. Geneva: WHO. |
| [63] | Zhao, S., Zhang, Y., Xiao, A. Y., He, Q., & Tang, K. (2023). Key factors associated with quality of postnatal care: a pooled analysis of 23 countries. E Clinical Medicine, 62, 102090. |
APA Style
Wegbom, A. I., Green, K. I., Ogbonda, P. N., Ndudim, O. M., Amah-Tariah, F. S. (2026). Geographical and Socioeconomic Inequalities in the Utilization of Maternal Healthcare Services in Nigeria. Biomedical Statistics and Informatics, 11(1), 14-30. https://doi.org/10.11648/j.bsi.20261101.12
ACS Style
Wegbom, A. I.; Green, K. I.; Ogbonda, P. N.; Ndudim, O. M.; Amah-Tariah, F. S. Geographical and Socioeconomic Inequalities in the Utilization of Maternal Healthcare Services in Nigeria. Biomed. Stat. Inform. 2026, 11(1), 14-30. doi: 10.11648/j.bsi.20261101.12
AMA Style
Wegbom AI, Green KI, Ogbonda PN, Ndudim OM, Amah-Tariah FS. Geographical and Socioeconomic Inequalities in the Utilization of Maternal Healthcare Services in Nigeria. Biomed Stat Inform. 2026;11(1):14-30. doi: 10.11648/j.bsi.20261101.12
@article{10.11648/j.bsi.20261101.12,
author = {Anthony Ike Wegbom and Kinikanwo Innocent Green and Priscilia Nyekpunwo Ogbonda and Oluchi Mildred Ndudim and Fortune Somiari Amah-Tariah},
title = {Geographical and Socioeconomic Inequalities in the Utilization of Maternal Healthcare Services in Nigeria},
journal = {Biomedical Statistics and Informatics},
volume = {11},
number = {1},
pages = {14-30},
doi = {10.11648/j.bsi.20261101.12},
url = {https://doi.org/10.11648/j.bsi.20261101.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.bsi.20261101.12},
abstract = {Maternal healthcare utilization remains suboptimal in Nigeria, with persistent socioeconomic and geographical disparities undermining progress toward reducing maternal morbidity and mortality. This study aims to assess the geographical and socioeconomic inequalities of maternal healthcare utilization in Nigeria. Maternal healthcare utilization in Nigeria remains suboptimal, with persistent socioeconomic and geographical disparities hindering progress in reducing maternal morbidity and mortality. This study assessed inequalities in the utilization of antenatal care (ANC4+), facility-based delivery (FBD), and postnatal care (PNC) using data from the 2018 Nigeria Demographic and Health Survey. Socioeconomic inequalities were examined using Erreygers Normalized Concentration Indices (ENCI) and concentration curves disaggregated by region and residence, while decomposition analysis identified key drivers. Findings revealed significant pro-rich inequalities across all services. Facility-based delivery showed the widest gaps (urban ENCI = 0.295; rural = 0.121), particularly in the Northwest (0.398) and Northeast (0.254). ANC4+ visits displayed moderate inequality, highest in the Northwest (0.169). PNC showed minimal inequality, with ENCI values near zero. Wealth status was the strongest contributor to inequality, supported by education, parity, and religion, while age, marital status, employment, autonomy, and insurance played minor roles. Although overall utilization was higher in urban areas, inequality was more pronounced there, highlighting deep intra-urban socioeconomic divides. Substantial socioeconomic and geographic inequities persist in maternal healthcare utilization in Nigeria. Targeted interventions addressing financial, educational, and sociocultural barriers, especially in northern and urban-poor populations, are crucial to narrowing gaps and improving maternal outcomes.},
year = {2026}
}
TY - JOUR T1 - Geographical and Socioeconomic Inequalities in the Utilization of Maternal Healthcare Services in Nigeria AU - Anthony Ike Wegbom AU - Kinikanwo Innocent Green AU - Priscilia Nyekpunwo Ogbonda AU - Oluchi Mildred Ndudim AU - Fortune Somiari Amah-Tariah Y1 - 2026/03/04 PY - 2026 N1 - https://doi.org/10.11648/j.bsi.20261101.12 DO - 10.11648/j.bsi.20261101.12 T2 - Biomedical Statistics and Informatics JF - Biomedical Statistics and Informatics JO - Biomedical Statistics and Informatics SP - 14 EP - 30 PB - Science Publishing Group SN - 2578-8728 UR - https://doi.org/10.11648/j.bsi.20261101.12 AB - Maternal healthcare utilization remains suboptimal in Nigeria, with persistent socioeconomic and geographical disparities undermining progress toward reducing maternal morbidity and mortality. This study aims to assess the geographical and socioeconomic inequalities of maternal healthcare utilization in Nigeria. Maternal healthcare utilization in Nigeria remains suboptimal, with persistent socioeconomic and geographical disparities hindering progress in reducing maternal morbidity and mortality. This study assessed inequalities in the utilization of antenatal care (ANC4+), facility-based delivery (FBD), and postnatal care (PNC) using data from the 2018 Nigeria Demographic and Health Survey. Socioeconomic inequalities were examined using Erreygers Normalized Concentration Indices (ENCI) and concentration curves disaggregated by region and residence, while decomposition analysis identified key drivers. Findings revealed significant pro-rich inequalities across all services. Facility-based delivery showed the widest gaps (urban ENCI = 0.295; rural = 0.121), particularly in the Northwest (0.398) and Northeast (0.254). ANC4+ visits displayed moderate inequality, highest in the Northwest (0.169). PNC showed minimal inequality, with ENCI values near zero. Wealth status was the strongest contributor to inequality, supported by education, parity, and religion, while age, marital status, employment, autonomy, and insurance played minor roles. Although overall utilization was higher in urban areas, inequality was more pronounced there, highlighting deep intra-urban socioeconomic divides. Substantial socioeconomic and geographic inequities persist in maternal healthcare utilization in Nigeria. Targeted interventions addressing financial, educational, and sociocultural barriers, especially in northern and urban-poor populations, are crucial to narrowing gaps and improving maternal outcomes. VL - 11 IS - 1 ER -
Department of Public Health Sciences, Rivers State University, Port Harcourt, Nigeria
Department of Public Health Sciences, Rivers State University, Port Harcourt, Nigeria
Department of Public Health Sciences, Rivers State University, Port Harcourt, Nigeria
Department of Public Health Sciences, Rivers State University, Port Harcourt, Nigeria
Department of Human Physiology, Rivers State University, Port Harcourt, Nigeria
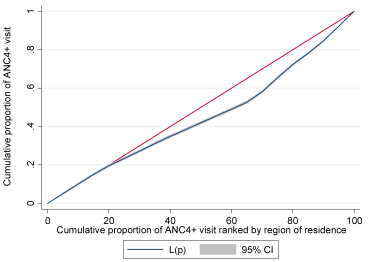
Figure 1. Concentration curve of ANC4+ visits by region of residence.
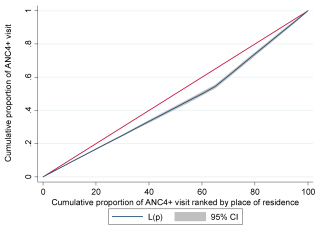
Figure 2. Concentration curve of ANC4+ visit by place of residence.
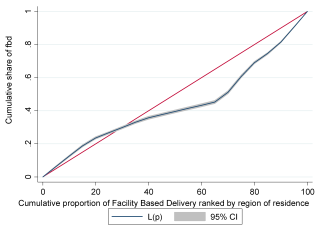
Figure 3. Concentration curve of Facility Based Delivery by region of residence.
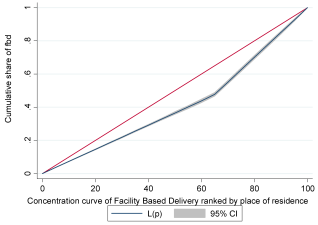
Figure 4. Concentration curve of Facility-Based Delivery by place of residence.
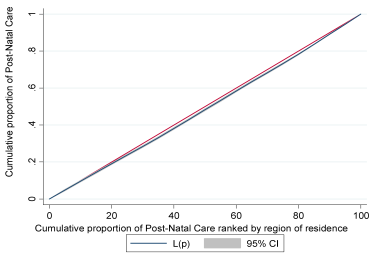
Figure 5. Concentration curve of Post-Natal Care by region of residence.
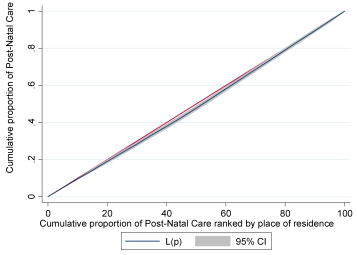
Figure 6. Concentration curve of Post-Natal Care by place of residence.
Information

