Abstract
Malnutrition remains a major public health challenge in low- and middle-income countries and contributes substantially to child mortality. In Senegal, it accounts for approximately one third of neonatal, infant, and under-five deaths. Although the Dakar region reports comparatively lower prevalence rates than other regions nationwide, undernutrition remains a serious concern in socioeconomically disadvantaged peri-urban communities where poverty, limited health infrastructure, and poor living conditions increase children’s vulnerability. In the municipality of Medina Gounass, located in the health district of Guediawaye in the suburbs of Dakar, structural poverty, high unemployment, and limited access to sanitation services create a particularly challenging environment for child health and nutrition. This study aimed to identify factors associated with wasting, stunting, and underweight among children aged 6–59 months in this vulnerable setting. An observational cross-sectional study with descriptive and analytical components was conducted from September 13 to 18, 2025. A total of 226 child-mother/caregiver pairs were included. Anthropometric measurements were collected to assess nutritional status using weight-for-height, height-for-age, and weight-for-age indices based on WHO z-score standards. Bivariate and multivariate logistic regression analyses were performed to identify factors independently associated with the different forms of undernutrition. Wasting affected 38 children (16.8%), including 7.5% with severe wasting, indicating a very high prevalence according to WHO classification thresholds. It was independently associated with the absence of a household handwashing facility (aOR=6.32; 95% CI: 1.85–21.56). Stunting was observed in 36 children (15.9%), including 4.0% severe cases, and was significantly associated with lack of exclusive breastfeeding during the first six months of life (aOR=4.28; 95% CI: 1.91–9.57). Underweight affected 39 children (17.2%), including 6.6% severe cases, and was independently associated with the absence of a household handwashing facility (aOR=10.33; 95% CI: 2.38–44.86) and lack of exclusive breastfeeding (aOR=3.79; 95% CI: 1.70–8.44). These findings highlight the substantial burden of child undernutrition in this disadvantaged peri-urban setting and underscore the critical role of household hygiene conditions and early infant feeding practices in shaping nutritional outcomes. Strengthening community-based interventions that promote hand hygiene and exclusive breastfeeding may contribute to reducing undernutrition in low-income urban settings.
|
Published in
|
Central African Journal of Public Health (Volume 12, Issue 2)
|
|
DOI
|
10.11648/j.cajph.20261202.14
|
|
Page(s)
|
84-104 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2026. Published by Science Publishing Group
|
Keywords
Malnutrition, Undernutrition, Wasting, Stunting, Underweight, Child Nutrition
1. Introduction
Nutrition reflects the complex interactions between dietary intake and health. Malnutrition arises when energy and nutrient intake is insufficient, excessive, or imbalanced. It encompasses three major conditions: (i) undernutrition—manifested as wasting (low weight-for-height), stunting (low height-for-age), and underweight (low weight-for-age); (ii) micronutrient-related malnutrition, including deficiencies or excesses of essential vitamins and minerals; and (iii) overweight, obesity, and diet-related non-communicable diseases such as cardiovascular disease, diabetes, stroke, and certain cancers
.
Wasting represents acute malnutrition and typically results from recent inadequate dietary intake or illness, particularly diarrheal diseases
| [1] | World Health Organization (WHO). Malnutrition. Geneva: World Health Organization; [cited 2025 Nov 4]. Available from:
https://www.who.int/fr/news-room/fact-sheets/detail/malnutrition |
| [2] | United Nations Children’s Fund (UNICEF), World Health Organization, International Bank for Reconstruction and Development/The World Bank. Levels and trends in child malnutrition: UNICEF / WHO / World Bank Group Joint Child Malnutrition Estimates. Key findings of the 2025 edition. Geneva: World Health Organization; 2025. Licence: CC BY-NC-SA 3.0 IGO. |
[1, 2]
. Stunting reflects chronic malnutrition and is the cumulative consequence of long-term exposure to adverse conditions, including poverty, poor maternal health and nutrition, recurrent infections, and suboptimal infant and young child feeding practices
| [1] | World Health Organization (WHO). Malnutrition. Geneva: World Health Organization; [cited 2025 Nov 4]. Available from:
https://www.who.int/fr/news-room/fact-sheets/detail/malnutrition |
| [2] | United Nations Children’s Fund (UNICEF), World Health Organization, International Bank for Reconstruction and Development/The World Bank. Levels and trends in child malnutrition: UNICEF / WHO / World Bank Group Joint Child Malnutrition Estimates. Key findings of the 2025 edition. Geneva: World Health Organization; 2025. Licence: CC BY-NC-SA 3.0 IGO. |
| [3] | Islam MM, Sanin KI, Mahfuz M, Ahmed AMS, Mondal D, Haque R, Ahmed T. Risk factors of stunting among children living in an urban slum of Bangladesh: findings of a prospective cohort study. BMC Public Health. 2018 Jan 30; 18(1): 197. https://doi.org/10.1186/s12889-018-5101-x |
[1-3]
. Underweight captures both acute and chronic nutritional deficits; a child classified as underweight may simultaneously be wasted, stunted, or both
.
Although malnutrition affects all populations, its burden falls disproportionately on low-and middle-income countries
. In early childhood, malnutrition compromises cognitive, psychomotor, social, and emotional development, reduces educational attainment, limits future productivity. At the population level, it contributes to intergenerational poverty and remains a major determinant of morbidity and mortality among children under five years of age
.
Globally, the scale of the problem remains substantial. In 2022, an estimated 149 million children under five years of age were stunted, 45 million were wasted, and 37 million were overweight or obese. Undernutrition contributes to nearly half of all deaths in this group age. According to the United Nations report on the State of Food Security and Nutrition
| [9] | FAO, FIDA, UNICEF, WFP, WHO. The State of Food Security and Nutrition in the World 2025: Addressing high food price inflation for food security and nutrition. Rome: FAO; 2025 [cited 2025 Nov 5]. Available from: https://doi.org/10.4060/cd6008en |
[9]
, the global prevalence of stunting declined from 26.4% in 2012 to 23.2% in 2024, reflecting gradual but insufficient progress toward global nutrition targets. In contrast, the prevalence of wasting and overweight has remained relatively stable at 6.6% and 5.5%, respectively. Encouragingly, the proportion of infants younger than six months who were exclusively breastfed increased from 37% in 2012 to 47.8% in 2023. Recent estimates further indicate that one third of children aged 6–23 months and two thirds of women aged 15–49 years achieve minimum dietary diversity, highlighting persistent gaps in optimal feeding practices.
Despite these global gains, progress in Africa remains insufficient
. In 2024, 43% of all children under five affected by stunting were living on the African continent. Africa also accounted for 27% of the global burden of wasting and 27% of overweight among children under five
| [2] | United Nations Children’s Fund (UNICEF), World Health Organization, International Bank for Reconstruction and Development/The World Bank. Levels and trends in child malnutrition: UNICEF / WHO / World Bank Group Joint Child Malnutrition Estimates. Key findings of the 2025 edition. Geneva: World Health Organization; 2025. Licence: CC BY-NC-SA 3.0 IGO. |
[2]
.
In Senegal, malnutrition contributes directly or indirectly to approximately one third of child mortality, with neonatal mortality at 23 per 1,000 live births, infant mortality at 31 per 1,000 live births, and under-five mortality at 40 per 1,000 live births mortality
. Nationally, 18% of children under five are stunted (including 4% severely), 10% are wasted (including 1% severely), and 16% are underweight (including 3% severely). Between 2015 and 2023, stunting declined from 21% to 18%, whereas wasting increased from 8% to 10%. Malnutrition remains more prevalent in rural than in urban areas (stunting: 21% vs. 12%; wasting: 12% vs. 7%). Regional disparities are marked, and nutritional outcomes are strongly associated with maternal education: stunting affects 19% of children whose mothers have no formal education compared with 13% among those whose mothers have at least secondary education)
.
Although Dakar reports comparatively the lower levels of malnutrition, important pockets of vulnerability persist in its suburban districts, including Pikine, Guediawaye, Yeumbeul, and Keur Massar, where socioeconomic deprivation exacerbates nutritional risk
| [12] | Nene M. État de la nutrition au Sénégal [Nutrition situation in Senegal]. In: Analyse et perspectives: 15 années d’expérience dans le développement de la politique de nutrition au Sénégal [Analysis and perspectives: 15 years of experience in the development of nutrition policy in Senegal]. Washington (DC): World Bank; Dakar: Cellule de Lutte contre la Malnutrition; 2018 [cited 2025 Nov 5]. Available from:
https://thedocs.worldbank.org/en/doc/946681594229136241-0090022020/original/1NutritionSituationFREFINAL.pdf |
| [13] | Diouf JBN, Sougou N, Tall C, Kane M, Sarr LP, Ndiaye O. Prevalence and factors associated with deficiency malnutrition in the health district of Guediawaye, Senegal. J Pediatr Neonatol. 2021; 3(2): 1–6. https://doi.org/10.33425/2689-1085.1021 |
[12, 13]
. Within the Guediawaye health district, the burden remains particularly high: 29.3% of children experience acute malnutrition, 20.4% chronic malnutrition, and 25.5% underweight. Empirical evidence from this context indicates that multiple interrelated determinants influence child nutritional outcomes, including household and demographic factors (e.g., having three or more children), recent morbidity (e.g., fever or diarrhea within the preceding weeks), suboptimal hygiene practices (e.g., failure to wash hands after using toilet), incomplete immunization, female sex, and inadequate dietary diversification at six months of age
| [13] | Diouf JBN, Sougou N, Tall C, Kane M, Sarr LP, Ndiaye O. Prevalence and factors associated with deficiency malnutrition in the health district of Guediawaye, Senegal. J Pediatr Neonatol. 2021; 3(2): 1–6. https://doi.org/10.33425/2689-1085.1021 |
[13]
.
In response, the non-governmental organization
Action and Development (ACDEV) | [14] | Action and Development (ACDEV). Dakar (Senegal): Action and Development; [cited 2026 Feb 12]. Available from:
https://acdev-inter.org/ |
[14]
, in partnership with the Ministry of Health through the Directorate of Maternal and Child Health (DSME)
and the King Baudoin Foundation
| [16] | King Baudoin Foundation. Brussels (Belgium): King Baudoin Foundation; [cited 2026 Feb 12]. Available from:
https://kbs-frb.be/en/home |
[16]
, has been implementing the “Xeex Xiboon” (combat malnutrition) project since January 2024. The initiative seeks to improve the nutritional status of children aged 0–59 months through a multisectoral, community-based approach focused on prevention, nutritional management, and community engagement.
Program monitoring identified the municipality of Medina Gounass
as a priority area requiring a tailored intervention strategy. This municipality, one of the five within the district, is characterized by structural poverty, extremely high unemployment (90%), and high illiteracy (80%). Access to health and education services is limited, with only one health post serving a population of 43,502 inhabitants. Approximately 20% of its territory consists of flood-prone areas, further exposing households to precarious living conditions and heightened vulnerability.
In this context, identifying the factors associated with wasting, stunting, and underweight among children aged 6–59 months in Medina Gounass is essential. A clearer understanding of these determinants may inform targeted, evidence-base interventions and strengthen the effectiveness of ongoing nutrition programs.
2. Materials and Methods
We conducted an observational cross-sectional study with descriptive and analytical components from September 13 to 18, 2025, in the municipality of Medina Gounass. The study population consisted of child-mother/caregiver pairs residing in the municipality. Each pair included a child aged 6–59 months and his or her biological mother or primary caregiver.
The sample size was calculated using the Schwartz formula, assuming a proportion (p) of 18% corresponding to the national prevalence of chronic malnutrition among children under five years of age—the most prevalent form of undernutrition in Senegal within this age group. The minimum required sample size was 227 child-mother/caregiver pairs.
Eligible participants were child-mother/caregiver pairs meeting all of the following criteria: (i) the mother or caregiver had resided in the municipality for at least six months; (ii) she was the child’s principal caregiver responsible for daily care; (iii) she provided free and informed consent; (iv) the child was a permanent household resident and present at the time of data collection; and (v) the household was located within the catchment area of the Medina Gounass health post and agreed to participate.
Pairs were excluded if the mother/caregiver or child was absent during the survey visit, if consent was refused or withdrawn, or if the child presented with a severe acute illness or congenital malformation likely to compromise accurate anthropometric measurement. Furthermore, children with known chronic diseases or conditions affecting growth and nutritional status (e.g., congenital heart disease, chronic kidney disease, endocrine disorders, or other long-term medical conditions) were also excluded to minimize potential bias in the assessment of malnutrition.
A probability proportional to size sampling strategy combined with random selection was used. The number of participants allocated to each neighborhood was proportional to the distribution of children aged 0–59 months across the municipality, thereby preserving the statistical weight of each area. Within neighborhoods, households were randomly selected from an exhaustive list of mothers and caregivers who had participate in educational talks, community dialogues, and cooking demonstrations organized under the project during the six months preceding the survey. When more than one eligible child was present in a household, one child was randomly selected.
The study was grounded in the United Nations Children’s Fund (UNICEF) conceptual framework of malnutrition
, with particular emphasis on the immediate causes of undernutrition. We hypothesized that undernutrition results from the interaction of multiple determinants operating at the child, maternal/caregiver, household, health, and feeding levels. Based on this framework and the study objectives, an anonymous questionnaire (Appendix) was developed and organized into six sections: (i) child characteristics; (ii) mother/caregiver characteristics; (iii) household characteristics; (iv) child health status; (v) feeding practices; and (vi) anthropometric measurements. The questionnaire was pre-tested in the neighboring municipality of Golf Sud among 25 child-mother/caregiver pairs prior to finalization.
The data collection team comprised 10 interviewers and 5 supervisors, organized into five teams of three members (two interviewers and one supervisor per team). Interviewers were community-based health promotion and prevention actors, including Bajenu Gox (community godmothers) and community health workers. Supervisors were health and nutrition professionals from the Guediawaye health district and were responsible for ensuring strict adherence to the study protocol. All team members received prior training covering technical procedures and ethical considerations. The principal investigator coordinated field activities, community mobilization, logistics, and overall supervision, with support from the local health post.
Data were collected on: (i) child characteristics: age, sex, weight, height; (ii) maternal/caregiver characteristic: age, marital status, educational level, and antenatal care attendance; (iii) household characteristics: household size, monthly income, number of children under five, presence of a handwashing facility; (iv) child health status: symptoms in the preceding 15 days, vaccination status, presence of bilateral lower-limb edema; and (v) feeding practices: exclusive breastfeeding, initiation of complementary feeding, daily meal frequency (excluding breast milk), dietary diversity. Anthropometric indicators included: (i) weight-for-height; (ii) height-for-age; (iii) weight-for-age; and (iv) mid-upper arm circumference (MUAC).
Nutritional status based on z-scores was assessed using the World Health Organization (WHO) simplified tables. For MUAC classification, national thresholds were applied: moderate acute malnutrition was defined as 120–130 mm, and severe acute malnutrition as <120 mm. Dietary diversity was assessed using WHO/UNICEF minimum dietary diversity indicator, defined as the number of distinct group foods consumed in the 24 hours preceding the survey. A score ranging from 0 to 8 was calculated across the following food groups: (i) breast milk; (ii) grains, roots, and tubers; (iii) legumes and nuts; (iv) dairy products (milk, yogurt, cheese); (v) meat, fish, and poultry; (vi) eggs; (vii) vitamin A-rich fruits and vegetables; and (viii) other fruits and vegetables. A score ≥5 indicated achievement of minimum dietary diversity.
Exclusive breastfeeding was defined according to the WHO as feeding the infant only breast milk during the first six months of life, with no other liquids or solids, except prescribed drops or syrups. A household was defined as all individuals living in the same dwelling, regardless of kinship. A caregiver referred to a person—most often a woman in the Senegal sociocultural context—other than the biological mother, who regularly assumed responsibility for a child’s care. Adequate antenatal care attendance was defined as completion of at least four contacts with a trained provider during pregnancy, with the first occurring before 12 weeks of amenorrhea. This information, along with vaccination status, was verified using the mother and child health booklet.
Data were entered using Microsoft Excel (Office 365), cleaned, and analyzed using R software (version 4.4.2). Descriptive analyses were conducted for both explanatory and outcome variables (wasting, stunting, and underweight). Categorical variables were summarized using frequencies and percentages, while continuous variables were presented as means and standard deviations (SD). Medians and ranges were reported when appropriate. For analytical purposes, variables were recoded into binary categories.
Bivariate analyses were conducted using cross-tabulations between each outcome and explanatory variables. Variables with a p-value ≤0.25 in bivariate analysis were considered eligible for multivariate modeling. Multivariate analysis was performed using binary logistic regression. A backward stepwise selection approach was applied using two strategies: (i) an automated backward procedure including variables with a p-value ≤0.25 at the bivariate level; and (ii) a backward procedure starting from a full model including all collected variables. The most parsimonious model obtained from the two approaches was retained for each outcome.
Model parsimony was evaluated using the Akaike Information Criterion (AIC). Residual diagnostics was performed graphically, and high-leverage observations were removed to improve model robustness. Multicollinearity was assessed using the Variance Inflation Factor (VIF). Interactions were examined and tested, and the best-fitting models were selected by comparing the AIC values of models with and without interaction terms. Model calibration was assessed using the Hosmer-Lemeshow goodness-of-fit test. Model performance was evaluated using receiver operating characteristic (ROC) curves and the corresponding area under the curve (AUC).
The study strictly adhered to ethical principles governing research involving human participants. Participation was voluntary, and free and informed consent was obtained from parents or caregivers. No financial incentives were provided. No biological samples were collected, and no medications were administered. Clinical assessment was limited to detection of lower-limb edema and the anthropometric measurements. All households received counseling on disease prevention and optimal child development. Confidentiality was ensured through anonymized identification codes, with no personal identifiers recorded. Data were analyzed in aggregate form, and results were presented in a manner that precluded individual identification.
3. Results
3.1. Study Population
A total of 227 child-mother/caregiver pairs were initially included. After exclusion of one pair due to incomplete data, 226 pairs were included in the final analysis.
3.2. Descriptive Results
3.2.1. Characteristics of the Children, Mothers/Caregivers, and Households Surveyed
Table 1. Characteristics of the Children, Mothers/Caregivers, and Households Surveyed.
Variables | Frequency (N=226) | Percentage (%) |
Child Characteristics |
Age (months) | | |
6–11 | 35 | 15.5 |
12–23 | 60 | 26.5 |
24–35 | 53 | 23.5 |
36–59 | 78 | 34.5 |
Sex | | |
Female | 103 | 45.6 |
Male | 123 | 54.4 |
Weight (kg) | | |
Mean (SD) | 11.7 (3.01) | |
Median [Min, Max] | 11.5 [5.0, 21.0] | |
Height (cm) | | |
Mean (SD) | 87.8 (12.0) | |
Median [Min, Max] | 88.2 [63.5, 117] | |
Mother/Caregiver Characteristics |
Age (years) | | |
Mean (SD) | 30.1 (7.59) | |
Median [Min, Max] | 29.0 [15.0, 70.0] | |
Marital status | | |
Single | 6 | 2.7 |
Married | 215 | 95.1 |
Divorced | 4 | 1.8 |
Widowed | 1 | 0.4 |
Educational level | | |
No formal education | 77 | 34.1 |
Primary | 89 | 39.4 |
Secondary | 54 | 23.9 |
University | 6 | 2.7 |
Adequate antenatal care attendances | | |
Yes | 198 | 87.6 |
No | 28 | 12.4 |
Household Characteristics |
Household size | | |
Mean (SD) | 6.82 (1.88) | |
Median [Min, Max] | 7.0 [2.0, 14.0] | |
Number of children <5 years | | |
Mean (SD) | 2.26 (1.39) | |
Median [Min, Max] | 2.0 [1.0, 9.0] | |
Monthly income (CFA francs) | | |
<100,000 | 70 | 31.0 |
100,000–200,000 | 103 | 45.6 |
200,000–300,000 | 48 | 21.2 |
300,000–400,000 | 3 | 1.3 |
>400,000 | 2 | 0.9 |
Handwashing facility | | |
Yes | 79 | 35.0 |
No | 147 | 65.0 |
Children aged 36 –59 months represented the largest age group (34.5%), followed by those aged 12–23 months (26.5%). Slightly more than half of the children were male (54.4%). The mean body weight was 11.7 kg (SD=3.01), with a median of 11.5 kg (range: 5–21). The mean height was 87.8 cm (SD=12.0), with a median of 88.2 cm (range: 63.5–117).
Mothers/caregivers had a mean age of 30.1 years (SD=7.59), with a median of 29 years (range: 15–70). The vast majority were married (95.1%), and nearly three-quarters (73.5%) had a primary level of education or less. Approximately one in eight mothers (12.4%) had not completed adequate antenatal care attendances during the pregnancy of the surveyed child.
Household comprised a mean of 6.82 members (SD=1.88), with a median of 7 members (range: 2–14). The average number of children under five years of age per household was 2.26 (SD=1.39), with a median of 2 (range: 1–9). Most households (76.6%) reported a monthly income of ≤200,000 CFA francs (363.74 USD), and 65% lacked a designated handwashing facility with water and soap.
Table 1 presents the characteristics of the children, mothers/caregivers, and households surveyed.
3.2.2. Health Status of the Children
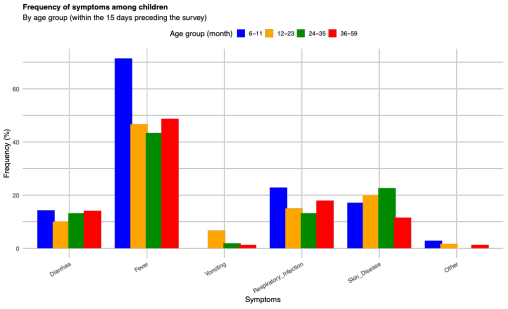
Vaccination coverage was high, with 87.2% of children up to date with age-appropriate immunizations. However, 29 children (12.8%) had missed one or more scheduled vaccines. Bilateral lower-limb edema was observed in 1.3% of children at the time of the survey. The most frequently reported symptoms during the 15 days preceding data collection were fever, respiratory infections, and dermatological conditions.
Figure 1 illustrates the distribution of the main symptoms reported in the previous 15 days according to children’s age groups.
Figure 1. Distribution of the Main Symptoms Reported During the Previous 15 Days by Age Group.
3.2.3. Feeding Practices of the Children
All children were receiving complementary foods at the time of the survey. Exclusive breastfeeding during the first six months of life was reported for 79.2% of children, whereas 20.8% had not been exclusively breastfed.
Children consumed an average of 3.58 solid and liquid meals per day (SD=1.09), excluding breast milk, with a median of 3 meals (range: 1–8). The mean dietary diversity score was 4.65 (SD=1.78), and half of the children (50.4%) did not meet the minimum dietary diversity threshold.
3.2.4. Nutritional Status Assessment
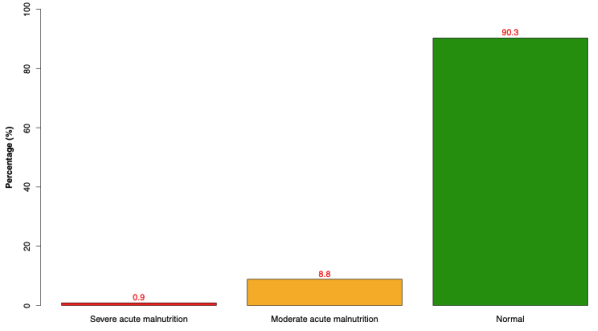
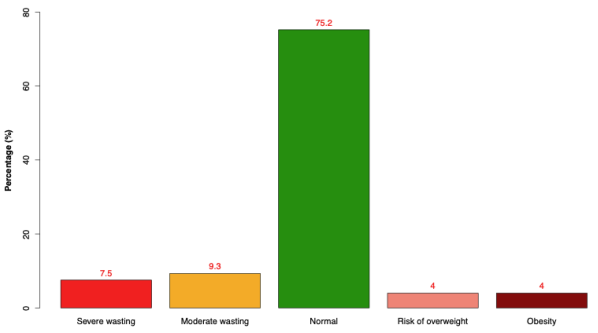
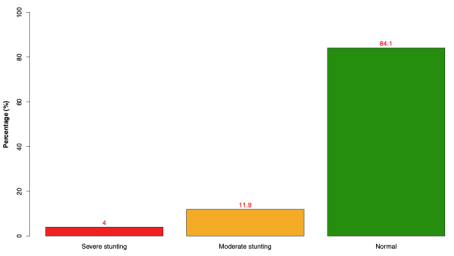
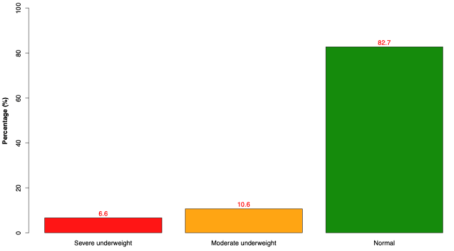
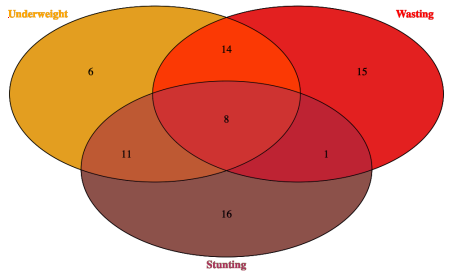
The mean MUAC was 149 mm (SD=14.5), with a median of 150 mm (range: 114–188). Based on MUAC classification, 8.8% of children had moderate acute malnutrition and 0.9% had severe acute malnutrition. According to weight-for-height z-scores, 9.3% of children were moderately wasted and 7.5% were severely wasted. Overweight and obesity were each observed in 4.0% of children. Stunting affected 11.9% of children in its moderate form and 4.0% in its severe form. Underweight was observed in 10.6% (moderate) and 6.6% (severe) of children. Among children classified as underweight, 14 (35.9%) also had wasting, 11 (28.2%) had stunting, and 8 (20.5%) experienced both wasting and stunting simultaneously.
Figures 2-5 present the results of nutritional assessment according to MUAC (
Figure 2), weight-for-height (
Figure 3), height-for-age (
Figure 4), and weight-for-age (
Figure 5).
Figure 6 shows a Venn diagram illustrating the distribution and overlap of the different forms of undernutrition.
Figure 2. Nutritional Screening Using Mid-Upper Arm Circumference.
Figure 3. Nutritional Status Based on Weight-for-Height.
Figure 4. Nutritional Status Based on Height-for-Age.
Figure 5. Nutritional Status Based on Weight-for-Age.
Figure 6. Venn Diagram Illustrating the Distribution and Overlap of Different Forms of Undernutrition.
3.3. Analytical Results
3.3.1. Bivariate Analysis
Wasting was significantly associated with the absence of a household handwashing facility with water and soap (OR=3.50; 95% CI: 1.48–9.82). Stunting was significantly associated with lack of exclusive breastfeeding during the first six months of life (OR=3.51; 95% CI: 1.61–7.56). Underweight was significantly associated with the absence of a handwashing facility (OR=4.32; 95% CI: 1.74–13.3), lack of exclusive breastfeeding (OR=3.48; 95% CI: 1.63–7.37), and inadequate dietary diversity (OR=2.23; 95% CI: 1.09–4.76).
Table 2 presents the results of the bivariate analysis of wasting, stunting, and underweight among children aged 6–59 months in the municipality of Medina Gounass in 2025.
Table 2. Bivariate Analysis of Wasting, Stunting, and Underweight Among Children Aged 6–59 Months in the Municipality of Medina Gounass, 2025.
Wasting |
Variables | No N=179 n (%) | Yes N=38 n (%) | OR [95% CI] | p-value |
Child’s age (months) | | | | 0.663 |
12–23 | 45 (77.6) | 13 (22.4) | Ref. | |
24–35 | 41 (82.0) | 9 (18.0) | 0.77 [0.28–1.98] | |
36–59 | 65 (85.5) | 11 (14.5) | 0.59 [0.24–1.45] | |
6–11 | 28 (84.8) | 5 (15.2) | 0.63 [0.18–1.90] | |
Child’s sex | | | | 0.210 |
Female | 84 (86.6) | 13 (13.4) | Ref. | |
Male | 95 (79.2) | 25 (20.8) | 1.69 [0.82–3.62] | |
Mother/caregiver age group | | | | 0.094 |
Adults | 140 (85.4) | 24 (14.6) | Ref. | |
Adolescents | 4 (66.7) | 2 (33.3) | 2.99 [0.35–17.2] | |
Young women | 35 (74.5) | 12 (25.5) | 2.00 [0.88–4.36] | |
Mother/caregiver marital status | | | | 0.632 |
Married | 173 (82.8) | 36 (17.2) | Ref. | |
Single/Divorced/Widowed | 6 (75.0) | 2 (25.0) | 1.67 [0.21–7.89] | |
Mother/caregiver educational level | | | | 0.958 |
University | 5 (83.3) | 1 (16.7) | Ref. | |
No formal education | 63 (84.0) | 12 (16.0) | 0.87 [0.12–24.5] | |
Primary | 68 (81.0) | 16 (19.0) | 1.07 [0.15–29.7] | |
Secondary | 43 (82.7) | 9 (17.3) | 0.96 [0.12–27.5] | |
Adequate antenatal care attendances | | | | 0.786 |
Yes | 158 (82.7) | 33 (17.3) | Ref. | |
No | 21 (80.8) | 5 (19.2) | 1.16 [0.36–3.13] | |
Household size | | | | 0.124 |
<5 members | 17 (68.0) | 8 (32.0) | Ref. | |
5–10 members | 149 (84.7) | 27 (15.3) | 0.38 [0.15–1.04] | |
≥10 members | 13 (81.2) | 3 (18.8) | 0.51 [0.09–2.23] | |
Number of children <5 years in the household | | | | 0.157 |
≤3 children | 145 (80.6) | 35 (19.4) | Ref. | |
>3 children | 34 (91.9) | 3 (8.11) | 0.38 [0.09–1.16] | |
Monthly household income (CFA francs) | | | | 0.247 |
>300,000 | 3 (60.0) | 2 (40.0) | Ref. | |
<100,000 | 55 (85.9) | 9 (14.1) | 0.25 [0.03–2.37] | |
100,000–300,000 | 121 (81.8) | 27 (18.2) | 0.33 [0.05–2.96] | |
Handwashing facility | | | | 0.008 |
Yes | 72 (92.3) | 6 (7.69) | Ref. | |
No | 107 (77.0) | 32 (23.0) | 3.50 [1.48–9.82] | |
Vaccination status up to date | | | | 0.793 |
Yes | 155 (82.0) | 34 (18.0) | Ref. | |
No | 24 (85.7) | 4 (14.3) | 0.78 [0.21–2.21] | |
Exclusive breastfeeding | | | | 0.528 |
Yes | 143 (83.6) | 28 (16.4) | Ref. | |
No | 36 (78.3) | 10 (21.7) | 1.43 [0.61–3.15] | |
Dietary diversity | | | | 0.355 |
Yes | 93 (85.3) | 16 (14.7) | Ref. | |
No | 86 (79.6) | 22 (20.4) | 1.48 [0.73–3.06] | |
Stunting |
Variables | No N=190 n (%) | Yes N=36 n (%) | OR [95% CI] | p-value |
Child’s sex | | | | 1.000 |
Female | 87 (84.5) | 16 (15.5) | Ref. | |
Male | 103 (83.7) | 20 (16.3) | 1.05 [0.51–2.19] | |
Mother/caregiver age group | | | | 0.207 |
Adults | 139 (81.8) | 31 (18.2) | Ref. | |
Adolescents | 6 (85.7) | 1 (14.3) | 0.83 [0.03–5.31] | |
Young women | 45 (91.8) | 4 (8.16) | 0.41 [0.11–1.12] | |
Mother/caregiver marital status | | | | 0.689 |
Married | 181 (84.2) | 34 (15.8) | Ref. | |
Single/Divorced/Widowed | 9 (81.8) | 2 (18.2) | 1.25 [0.17–5.23] | |
Mother/caregiver educational level | | | | 0.989 |
University | 5 (83.3) | 1 (16.7) | Ref. | |
No formal education | 65 (84.4) | 12 (15.6) | 0.84 [0.11–23.7] | |
Primary | 74 (83.1) | 15 (16.9) | 0.92 [0.13–25.6] | |
Secondary | 46 (85.2) | 8 (14.8) | 0.80 [0.10–23.2] | |
Adequate antenatal care attendances | | | | 0.410 |
Yes | 168 (84.8) | 30 (15.2) | Ref. | |
No | 22 (78.6) | 6 (21.4) | 1.55 [0.53–3.97] | |
Household size | | | | 0.604 |
<5 members | 20 (76.9) | 6 (23.1) | Ref. | |
5–10 members | 156 (84.8) | 28 (15.2) | 0.59 [0.23–1.76] | |
≥10 members | 14 (87.5) | 2 (12.5) | 0.50 [0.06–2.67] | |
Number of children <5 years in the household | | | | 0.828 |
≤3 children | 159 (84.6) | 29 (15.4) | Ref. | |
>3 children | 31 (81.6) | 7 (18.4) | 1.25 [0.46–3.01] | |
Monthly household income (CFA francs) | | | | 0.318 |
>200,000 | 46 (86.8) | 7 (13.2) | Ref. | |
<100,000 | 55 (78.6) | 15 (21.4) | 1.77 [0.68–5.04] | |
100,000–200,000 | 89 (86.4) | 14 (13.6) | 1.02 [0.39–2.91] | |
Handwashing facility | | | | 0.240 |
Yes | 70 (88.6) | 9 (11.4) | Ref. | |
No | 120 (81.6) | 27 (18.4) | 1.73 [0.79–4.12] | |
Vaccination status up to date | | | | 0.586 |
Yes | 164 (83.2) | 33 (16.8) | Ref. | |
No | 26 (89.7) | 3 (10.3) | 0.60 [0.13–1.85] | |
Exclusive breastfeeding | | | | 0.002 |
Yes | 158 (88.3) | 21 (11.7) | Ref. | |
No | 32 (68.1) | 15 (31.9) | 3.51 [1.61–7.56] | |
Dietary diversity | | | | 0.626 |
Yes | 96 (85.7) | 16 (14.3) | Ref. | |
No | 94 (82.5) | 20 (17.5) | 1.27 [0.62–2.65] | |
Underweight |
Variables | No N=187 n (%) | Yes N=39 n (%) | OR [95% CI] | p-value |
Child’s sex | | | | 0.247 |
Female | 89 (86.4) | 14 (13.6) | Ref. | |
Male | 98 (79.7) | 25 (20.3) | 1.61 [0.79–3.38] | |
Mother/caregiver age group | | | | 0.554 |
Adults | 140 (82.4) | 30 (17.6) | Ref. | |
Adolescents | 5 (71.4) | 2 (28.6) | 1.94 [0.24–9.91] | |
Young women | 42 (85.7) | 7 (14.3) | 0.79 [0.30–1.85] | |
Mother/caregiver marital status | | | | 0.101 |
Married | 180 (83.7) | 35 (16.3) | Ref. | |
Single/Divorced/Widowed | 7 (63.6) | 4 (36.4) | 2.96 [0.72–10.6] | |
Mother/caregiver educational level | | | | 0.786 |
University | 5 (83.3) | 1 (16.7) | Ref. | |
No formal education | 62 (80.5) | 15 (19.5) | 1.10 [0.15–30.6] | |
Primary | 73 (82.0) | 16 (18.0) | 0.99 [0.14–27.6] | |
Secondary | 47 (87.0) | 7 (13.0) | 0.69 [0.09–20.1] | |
Adequate antenatal care attendances | | | | 0.284 |
Yes | 166 (83.8) | 32 (16.2) | Ref. | |
No | 21 (75.0) | 7 (25.0) | 1.75 [0.63–4.32] | |
Household size | | | | 0.623 |
<5 members | 20 (76.9) | 6 (23.1) | Ref. | |
5–10 members | 154 (83.7) | 30 (16.3) | 0.64 [0.25–1.90] | |
≥10 members | 13 (81.2) | 3 (18.8) | 0.79 [0.14–3.70] | |
Number of children <5 years in the household | | | | 1.000 |
≤3 children | 156 (83.0) | 32 (17.0) | Ref. | |
>3 children | 31 (81.6) | 7 (18.4) | 1.12 [0.42–2.65] | |
Monthly household income (CFA francs) | | | | 1.000 |
>300,000 | 4 (80.0) | 1 (20.0) | Ref. | |
<100,000 | 58 (82.9) | 12 (17.1) | 0.76 [0.09–22.1] | |
100,000–300,000 | 125 (82.8) | 26 (17.2) | 0.76 [0.10–21.3] | |
Handwashing facility | | | | 0.003 |
Yes | 74 (93.7) | 5 (6.33) | Ref. | |
No | 113 (76.9) | 34 (23.1) | 4.32 [1.74–13.3] | |
Vaccination status up to date | | | | 1.000 |
Yes | 163 (82.7) | 34 (17.3) | Ref. | |
No | 24 (82.8) | 5 (17.2) | 1.02 [0.32–2.70] | |
Exclusive breastfeeding | | | | 0.001 |
Yes | 156 (87.2) | 23 (12.8) | Ref. | |
No | 31 (66.0) | 16 (34.0) | 3.48 [1.63–7.37] | |
Dietary diversity | | | | 0.040 |
Yes | 99 (88.4) | 13 (11.6) | Ref. | |
No | 88 (77.2) | 26 (22.8) | 2.23 [1.09–4.76] | |
3.3.2. Multivariate Analysis
In multivariate logistic regression models, absence of a household handwashing facility remained independently associated with both wasting (aOR=6.32; 95% CI: 1.85–21.56) and underweight (aOR=10.33; 95% CI: 2.38–44.86). Lack of exclusive breastfeeding during the first six months of life was independently associated with stunting (aOR=4.28; 95% CI: 1.91–9.57) and underweight (aOR=3.79; 95% CI: 1.70–8.44).
The predictive model for wasting showed high sensitivity (85.3%; 95% CI: 73.4–97.2) but moderate specificity (48.6%; 95% CI: 41.2–56.0). The stunting model demonstrated balanced sensitivity (69.7%; 95% CI: 54.0–85.4) and specificity (66.3%; 95% CI: 59.5–73.1). The underweight model showed lower sensitivity (38.9%; 95% CI: 23.0–54.8) but high specificity (88.6%; 95% CI: 84.1–93.2).
Table 3 presents the results of the multivariate analysis of predictors of wasting, stunting, and underweight among children aged 6–59 months in the municipality of Medina Gounass in 2025.
Table 3. Multivariate Analysis of Predictors of Wasting, Stunting, and Underweight Among Children Aged 6–59 Months in the Municipality of Medina Gounass, 2025.
Variables | Adjusted OR | [95% CI] | p-value |
Wasting: Yes vs. No (Ref.) |
Number of children <5 years in the household | | | 0.098 |
≤3 children | Ref. | | |
>3 children | 0.33 | [0.07–1.47] | |
*Handwashing facility | | | < 0.001 |
Yes | Ref. | | |
No | 6.32 | [1.85–21.56] | |
Stunting: Yes vs. No (Ref.) |
Child’s sex | | | 0.54 |
Female | Ref. | | |
Male | 1.28 | [0.58–2.8] | |
Mother/caregiver educational level | | | 0.71 |
University | Ref. | | |
No formal education | 0.51 | [0.05–4.97] | |
Primary | 0.73 | [0.08–6.91] | |
Secondary | 0.44 | [0.04–4.59] | |
*Exclusive breastfeeding | | | < 0.001 |
Yes | Ref. | | |
No | 4.28 | [1.91–9.57] | |
Underweight: Yes vs. No (Ref.) |
*Handwashing facility | | | < 0.001 |
Yes | Ref. | | |
No | 10.33 | [2.38–44.86] | |
*Exclusive breastfeeding | | | 0.001 |
Yes | Ref. | | |
No | 3.79 | [1.7–8.44] | |
4. Discussion
Wasting and associated factors
In this study, 16.8% of children aged 6–59 months were affected by wasting, including 7.5% with severe wasting. This prevalence substantially exceeds the regional estimate for Dakar (5%, including 0.1% severe forms)
, suggesting that marked intra-urban disparities persist despite comparatively favorable regional averages. The higher burden observed in Medina Gounass likely reflects the concentration of socioeconomic deprivation, environmental insecurity, and precarious living conditions that characterize peri-urban municipalities within the Dakar metropolitan area.
The absence of a household handwashing facility with water and soap was independently associated with wasting, with affected children being more than six times as likely to be wasted (aOR=6.32). This statistically significant association underscores the critical role of household hygiene conditions in the prevention of acute malnutrition. Wasting, as an indicator of acute nutritional deficit, often reflects recent exposure to infectious diseases and inadequate nutrient intake. Poor hygiene environments increase children’s susceptibility to enteric infections—particularly diarrheal diseases—which impair nutrient absorption, increase metabolic demands, and can precipitate rapid weight loss.
Our findings are consistent with those reported by Diouf JBN et al.
| [13] | Diouf JBN, Sougou N, Tall C, Kane M, Sarr LP, Ndiaye O. Prevalence and factors associated with deficiency malnutrition in the health district of Guediawaye, Senegal. J Pediatr Neonatol. 2021; 3(2): 1–6. https://doi.org/10.33425/2689-1085.1021 |
[13]
, who documented a 29.3% prevalence of acute malnutrition among children aged 6–59 months in the Guediawaye health district, which includes Medina Gounass. In their study, failure to wash hands after using the toilet was significantly associated with acute malnutrition (p=0.01), further highlighting the central role of hygiene practices in shaping nutritional outcomes. Although the prevalence observed in our study is lower than that reported at the district level in 2021, the persistence of a substantial burden reinforces the structural vulnerability of this setting.
At a broader level, our results align with evidence synthesized by Akombi et al.
| [5] | Akombi BJ, Agho KE, Hall JJ, Wali N, Renzaho AMN, Merom D. Stunting, Wasting and Underweight in Sub-Saharan Africa: A Systematic Review. Int J Environ Res Public Health. 2017 Aug 1; 14(8): 863.
https://doi.org/10.3390/ijerph14080863 |
[5]
, whose 2017 systematic review identified the use of unimproved water sources as a major risk factor for acute malnutrition in sub-Saharan Africa. Similarly, Harding et al.
| [19] | Harding KL, Aguayo VM, Webb P. Factors associated with wasting among children under five years old in South Asia: Implications for action. PLoS One. 2018 Jul 3; 13(7): e0198749. https://doi.org/10.1371/journal.pone.0198749 |
[19]
, analyzing data from 252,797 children across six South Asian countries in 2018, demonstrated that lack of access to improved water sources and household poverty were significantly associated with wasting across multiple national contexts. Together, these findings converge toward a consistent epidemiological pattern linking inadequate water, sanitation, and hygiene (WASH) conditions to increased risk of acute undernutrition.
The biological plausibility of this association is well established. Recurrent enteric infections and chronic exposure to contaminated environments may contribute not only to overt diarrheal episodes but also to subclinical conditions such as environmental enteric dysfunction, which compromise intestinal integrity and nutrient absorption. In resource-constrained urban settings, where overcrowding and limited sanitation infrastructure are common, these mechanisms may amplify children’s vulnerability to acute nutritional deterioration.
Taken together, our findings support the integration of WASH interventions within child nutrition strategies. In settings such as Medina Gounass, strengthening access to functional handwashing facilities and promoting sustained hygiene practices may represent a critical, yet underutilized, lever for reducing the burden of wasting.
Stunting and associated factors
In this study, 15.9% of children aged 6–59 months were affected by stunting, including 4.0% with severe forms. Additionally, 20.8% of children had not been exclusively breastfed during the first six months of life. Children who did not benefit from exclusively breastfeeding were more than four times as likely to be stunted compared with those who were exclusively breastfed (aOR=4.28), underscoring the protective role of optimal early feeding practices against chronic undernutrition.
The prevalence observed in our study is slightly lower than reported by Diouf JBN et al.
| [13] | Diouf JBN, Sougou N, Tall C, Kane M, Sarr LP, Ndiaye O. Prevalence and factors associated with deficiency malnutrition in the health district of Guediawaye, Senegal. J Pediatr Neonatol. 2021; 3(2): 1–6. https://doi.org/10.33425/2689-1085.1021 |
[13]
, who documented a 20.4% prevalence of chronic malnutrition in the Guediawaye health district. In their study, nearly 97.1% of children were reported to have been exclusively breastfed up to six months. While differences in study design and contextual factors may partly explain this variation, the persistence of stunting at substantial levels across the district highlights the enduring structural determinants of chronic growth failure in this setting.
At the national level, trends in exclusive breastfeeding practices reveal limited sustained progress. The proportion of infants under six months who were exclusively breastfed increased from 34% in 2005 to 41% in 2019 but declined again to 34% in 2023
. This regression suggests persistent challenges in maintaining adherence to recommended infant feeding practices, despite ongoing awareness campaigns and policy efforts. In socioeconomically vulnerable environments, competing economic pressures, maternal workload, limited maternity protection, and sociocultural norms may hinder sustained exclusive breastfeeding.
Our findings are consistent with the systematic review by Mu’Alifah et al.
, which demonstrated that exclusive breastfeeding is associated with a reduced prevalence of stunting, particularly in disadvantaged socioeconomic settings where it serves as a critical protective factor. Breast milk provides optimal nutrient composition, enhances immune protection, and reduces exposure to contaminated food or water sources during a biologically vulnerable period of life. However, the authors also note heterogeneity in observed associations and caution that prolonged breastfeeding beyond 12 months, in the absence of adequate complementary feeding, may compromise growth and immune function. These observations are supported by the systematic review conducted by Akombi et al.
, which identified extended breastfeeding (>12 months) without appropriate dietary diversification as a factor frequently associated with stunting, wasting, and underweight.
Evidence from other contexts reinforces the interaction between feeding practices and household socioeconomic conditions. A study conducted in Indonesia
| [21] | Hadi H, Fatimatasari F, Irwanti W, Kusuma C, Alfiana RD, Asshiddiqi MIN, Nugroho S, Lewis EC, Gittelsohn J. Exclusive Breastfeeding Protects Young Children from Stunting in a Low-Income Population: A Study from Eastern Indonesia. Nutrients. 2021 Nov 26; 13(12): 4264.
https://doi.org/10.3390/nu13124264 |
[21]
found that children under two years of age from wealthier households who were exclusively breastfed had a 50% lower risk of stunting compared with children from poorer households who were not exclusively breastfed. Qualitative findings from that study further indicated that limited maternal awareness regarding the importance of exclusive breastfeeding contributed to suboptimal practices. These findings highlight that breastfeeding behaviors are shaped not only by knowledge but also by structural constraints and household resources.
Collectively, these results emphasize exclusive breastfeeding as a central and modifiable determinant of chronic undernutrition. In low-income urban settings such as Medina Gounass, strengthening community-based education, reinforcing counseling during antenatal and postnatal care, and addressing structural barriers to sustained breastfeeding may represent key strategies for reducing the burden of stunting.
Underweight and associated factors
In this study, 17.2% of children aged 6–59 months were underweight, including 6.6% with severe underweight. Two factors were independently associated with this condition: the absence of a household handwashing facility with water and soap and the lack of exclusive breastfeeding during the first six months of life. Children living in households without a handwashing facility were more than ten times as likely to be underweight (aOR=10.33), while those who had not been exclusively breastfed had nearly four times the odds of underweight (aOR=3.79).
The prevalence observed in Medina Gounass remains substantial, although lower than the 25.5% reported by Diouf JBN et al.
| [13] | Diouf JBN, Sougou N, Tall C, Kane M, Sarr LP, Ndiaye O. Prevalence and factors associated with deficiency malnutrition in the health district of Guediawaye, Senegal. J Pediatr Neonatol. 2021; 3(2): 1–6. https://doi.org/10.33425/2689-1085.1021 |
[13]
in the Guediawaye health district. The concordance between the two studies nevertheless underscores the persistence of undernutrition in this peri-urban context, where structural poverty and environmental vulnerabilities continue to shape child health outcomes.
Underweight is a composite indicator reflecting both acute and chronic nutritional deficits. Its association with inadequate hygiene infrastructure and suboptimal infant feeding practices mirrors the determinants identified for wasting and stunting, suggesting overlapping causal pathways. Poor household hygiene increases exposure to infectious diseases that impair nutrient absorption and increase metabolic demands, while lack of exclusive breastfeeding deprives infants of optimal nutrition and immunological protection during a critical development window.
The association between hand hygiene and weight-for-age has also been documented in other settings. A nationally representative study conducted in Nepal among 2,352 children in 2016
| [22] | Shrestha SK, Vicendese D, Erbas B. Water, sanitation and hygiene practices associated with improved height-for-age, weight-for-height and weight-for-age z-scores among under-five children in Nepal. BMC Pediatr. 2020 Mar 23; 20(1): 134. https://doi.org/10.1186/s12887-020-2010-9 |
[22]
reported that handwashing with water and soap was positively associated with weight-for-age z-scores, with a mean increase of 0.15 (95% CI: 0.04–0.25). This finding supports the hypothesis that improved hygiene practices may contribute not only to reduced morbidity but also to measurable improvements in growth indicators.
Similarly, our results align with the systematic review by Mardani et al.
| [23] | Mardani RAD, Wu WR, Nhi VT, Huang HC. Association of breastfeeding with undernutrition among children under 5 years of age in developing countries: A systematic review and meta-analysis. J Nurs Scholarsh. 2022 Nov; 54(6): 692-703. https://doi.org/10.1111/jnu.12799 Epub 2022 Jul 18. |
[23]
, which identified exclusive breastfeeding as a major protective factor against overall undernutrition, including both stunting and underweight, with statistically significant improvements in nutritional outcomes observed in low-resource settings (p<0,05). The protective mechanisms are multifactorial, encompassing optimal nutrient composition, enhanced immune protection, and reduced exposure to contaminated complementary foods.
The converge of these findings highlights the interconnected nature of underweight with both wasting and stunting, reflecting the interplay between environmental hygiene conditions and early feeding practices. In peri-urban disadvantaged settings such as Medina Gounass, integrated strategies that simultaneously strengthen household WASH infrastructure and promote sustained exclusive breastfeeding up to six months may represent a critical pathway for reducing burden of underweight and improving overall child nutritional status.
Non-significant factors
Although several determinants of child undernutrition have been widely documented in the literature, a number of variables examined in this study were not significantly associated with wasting, stunting, or underweight. This absence of statistical association may reflect the contextual characteristics of the study setting. In socioeconomically vulnerable peri-urban environments such as Medina Gounass, structural constraints—including poverty, limited access to services, and precarious living conditions—tend to be broadly shared across households, potentially reducing observable variability between exposure groups.
In this context, the significant associations identified for household handwashing facilities and exclusive breastfeeding may capture key proximal pathways linking household environment and caregiving practices to child nutritional outcomes. The lack of association for other variables should therefore not be interpreted as evidence of their irrelevance but rather as an indication that their effects may be mediated through broader environmental and behavioral factors in this setting.
Study limitations
Several limitations should be considered when interpreting the findings of this study.
First, the cross-sectional design precludes establishing causal relationships between the identified factors and undernutrition. Although significant associations were observed, temporal sequencing cannot be ascertained, and reserve causality cannot be entirely excluded. Longitudinal or cohort-based designs would be required to confirm causal pathways.
Second, inclusion was restricted to child-mother/caregiver pairs who had participated in at least one project activity during the six months preceding the survey. This eligibility criterion may have introduced selection bias by excluding households residing in the municipality but not yet reached by the intervention. As a result, the study population may not fully represent all households in Medina Gounass, particularly those with lower levels of engagement in community-based activities.
Third, although probability proportional to size sampling combined with random selection was operationally feasible in this resource-constrained context, alternative sampling strategies—such as multi-stage cluster sampling commonly used in community nutrition surveys—might have enhanced representativeness. Additionally, the relatively modest sample size may have reduced statistical precision, as reflected in some wide confidence intervals, thereby limiting the robustness of certain effect estimates.
Information bias must also be considered. Data on exclusive breastfeeding relied on maternal recall, which may therefore be subject to recall bias or social desirability bias, particularly in a context where breastfeeding promotion activities were ongoing. Such misclassification, could have resulted in either underestimation or overestimation of the observed associations.
The study further focused exclusively on anthropometric indicators of undernutrition—wasting, stunting, and underweight—without assessing micronutrient deficiencies. Given the high prevalence of micronutrient malnutrition among young children in low-resource settings, the absence of biological or clinical markers limits the comprehensiveness of the nutritional assessment. Inclusion of biochemical indicators would have provided a more complete picture of the community’s nutritional burden.
Finally, when more than one eligible child was present within the household, only one child was randomly selected for inclusion. While including all eligible children might have increased statistical power, selecting a single child per household reduced intra-household correlation and minimized clustering effects that could otherwise inflate precision if not analytically accounted for. This approach ensured greater statistical independence of observations within the constraints of the study design. Future studies incorporating larger samples and analytical methods explicitly accounting for household-level clustering would allow for a more detailed exploration of intra-household nutritional dynamics.
Despite these limitations, the study provides valuable context-specific evidence on modifiable determinants of undernutrition in a highly vulnerable peri-urban setting.
5. Conclusion
This study highlights a substantial burden of child undernutrition in the peri-urban municipality of Medina Gounass, within the Guediawaye health district of the Dakar metropolitan area. The prevalence of wasting reached levels classified as very high according to WHO thresholds, while stunting and underweight remain significant public health concerns. These findings underscore the persistence of marked intra-urban nutritional inequalities despite comparatively favorable regional averages.
Two modifiable determinants consistently emerged across nutritional outcomes: inadequate household hygiene infrastructure and the absence of exclusive breastfeeding during the first six months of life. The strong associations observed between lack of handwashing facilities and both wasting and underweight reinforce the critical role of WASH conditions in preventing acute forms of undernutrition. Similarly, the protective effect of exclusive breastfeeding against stunting and underweight confirms its central importance in early-life nutrition strategies.
Taken together, these results emphasize the need for integrated, context-specific interventions that simultaneously address environmental health conditions and optimal infant feeding practices. In vulnerable peri-urban settings such as Medina Gounass, strengthening access to functional handwashing facilities, reinforcing behavior-change communication around hygiene, and sustaining support for exclusive breastfeeding may represent high-impact and cost-effective strategies for reducing the burden of childhood undernutrition.
Beyond the local context, this study contributes to the growing body of evidence highlighting the interconnected roles of structural poverty, household environments, and early feeding practices in shaping child growth trajectories. Addressing these determinants through multisectoral approaches will be essential to accelerate progress toward national and global nutrition targets.
Abbreviations
ACDEV | Action and Development |
AIC | Akaike Information Criterion |
AUC | Area Under Curve |
CI | Confidence Interval |
DSME | Directorate of Maternal and Child Health |
ENDSS | National School of Health and Social Development |
ISED | Institute of Health and Development |
MUAC | Mid-Upper Arm Circumference |
WHO | World Health Organization |
OR | Odds-ratio |
aOR | Adjusted Odds-ratio |
ROC | Receiver Operating Characteristic |
SD | Standard Deviation |
UCAD | Cheikh Anta Diop University |
UGB | Gaston Berger University |
UNICEF | United Nations Children’s Fund |
VIF | Variance Inflation Factor |
WASH | Water, Sanitation, and Hygiene |
Acknowledgments
The authors express their sincere gratitude to all staff members of ACDEV for their continuous support throughout the implementation of this study. They extend their special thanks to Dr. Cheikh Tidiane Athie (Executive Director), Ms. Ramatoulaye Bousso (Administrative and Financial Director), Ms. Mbarka Ndaw (Director of Operations), Mr. Momar Talla Seck (Advocacy Officer), Mr. Djibril Gueye (Nutrition Program Coordinator), Ms. Yacine Mbow (Nutrition Project Officer), Dr. Aissatou Sow (Nutrition Project Officer), Dr. Diawdine Diaw (Quality of Services Officer), Ms. Bintou Diallo (Knowledge Management Officer), Ms. Khadidia Fall Seye (Monitoring and Evaluation Officer), Mr. Ibrahima Sy (Monitoring and Evaluation Officer), Ms. Kounta Mbaye, Ms. Florence Ahouandjinou, Ms. Awa Coly, Ms. Oumou Kalsoum Cisse, and Ms. Mamadou Binta Diallo (Nutrition Project Supervisors), Ms. Aissatou Catherine Sow (Reproductive Health Project Officer), Ms. Awa Fall, Ms. Aminata Sene, and Ms. Oumou Kalsoum Niass (Finance Department), Mr. Mohamed Ka (Legal Department), and Mr. Antoine Tine (Social Protection Officer).
The authors also wish to thank the Chief Medical Officer of the Guediawaye health district, Dr. Ndiaye Faly Diop, as well as the entire district management team for their collaboration and availability. Finally, they express their appreciation to the Head Nurse of the Medina Gounass health post, Ms. Maguette Sene, and to all community stakeholders for their commitment and valuable contribution to the successful conduct of this study.
Author Contributions
Gad Papin Oholiab Namndiro: Conceptualization, Data curation, Formal analysis, Funding acquisition, Methodology, Resources, Software, Validation, Visualization, Writing – original draft
Raphaela Maporo Edekoyo: Funding acquisition, Investigation, Resources, Validation, Writing – review & editing
Seynabou Ndiaye: Validation, Writing – review & editing
Jean Augustin Diegane Tine: Project administration, Supervision, Validation, Writing – review & editing
Funding
This research was fully funded by the authors’ personal resources. The study nevertheless benefited from logistical and technical support provided by ACDEV, the Guediawaye health district, and the Medina Gounass health post, particularly in facilitating field activities and community mobilization. The authors emphasize that they maintained full independence from these institutions in the design, conduct, analysis, and interpretation of the study findings.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request, subject to compliance with ethical and confidentiality considerations regarding study participants.
Conflicts of Interest
The authors declare that they have no conflicts of interest related to the conduct, analysis, or publication of this research.
Appendix
Questionnaire Overview
Section 1: Child Characteristics
What is the child’s age (in months)?
6–11
12–23
24–35
36–59
What is the child’s sex?
Male
Female
What is the child’s weight (in kg)?
(Measure the child’s weight and record the value.)
_________kg
What is the child’s height (in cm)?
(Measure the child’s height and record the value.)
__________cm
Section 2: Mother/Caregiver Characteristics
What is the mother’s/caregiver’s age (in years)?
________years
What is the mother’s/caregiver’s marital status?
Married
Single
Divorced
Widowed
What is the mother’s/caregiver’s highest level of education completed?
No formal education
Primary education
Secondary education
University education
Did the mother attend at least four antenatal care visits with a trained health professional during pregnancy, with the first visit occurring before 12 weeks of amenorrhea?
(Verify using the mother and child health booklet and tick appropriate response)
Yes
No
Section 3: Household Characteristics
What is the total number of people living in the household?
________ household members
How many children under five years of age live in the household?
________ children under five years
What is the approximate monthly household income (in CFA francs)?
<100,000
100,000–200,000
200,000–300,000
300,000–400,000
>400,000
Does the household have a functional handwashing facility with water and soap available?
Yes
No
Section 4: Child Health Status
In the past two (2) weeks, has the child experienced any of the following symptoms?
(Select all that apply.)
Diarrhea
Fever
Vomiting
Respiratory infection
Skin disease
Other (specify): _______________
Is the child’s vaccination record up to date?
(Verify using the mother and child health booklet and tick appropriate response)
Yes
No
Does the child present with bilateral lower-limb edema?
Yes
No
Section 5: Feeding Practices
Was the child exclusively breastfed during the first six months of life (no water, other liquids, or solid foods)?
Yes
No
Has the child started complementary feeding?
Yes
No
Excluding breastfeeding, how many solid or liquid meals does the child consume per day?
__________meals per day
During the past 24 hours, did the child consume any of the following food groups?
(Select all that apply.)
Group 1: Breast milk
Group 2: Grains, roots, and tubers
Group 3: Legumes and nuts
Group 4: Dairy products (milk, yogurt, cheese)
Group 5: Meat, fish, and poultry
Group 6: Eggs
Group 7: Vitamin A-rich fruits and vegetables
Group 8: Other fruits and vegetables
Section 6: Anthropometric Measurements
What is the child’s nutritional classification according to weight-for-height?
(Take the measurement, interpret according to WHO standards, and tick the appropriate category.)
Normal
Moderate wasting
Severe wasting
Risk of overweight
Obesity
What is the child’s nutritional classification according to height-for-age?
(Take the measurement, interpret according to WHO standards, and tick the appropriate category.)
Normal
Moderate stunting
Severe stunting
What is the child’s nutritional classification according to weight-for-age?
(Take the measurement, interpret according to WHO standards, and tick the appropriate category.)
Normal
Moderate underweight
Severe underweight
What is the child’s nutritional classification according to mid-upper arm circumference?
(Take the measurement, interpret according to WHO standards, and tick the appropriate category.)
Normal
Moderate acute malnutrition
Severe acute malnutrition
References
| [1] |
World Health Organization (WHO). Malnutrition. Geneva: World Health Organization; [cited 2025 Nov 4]. Available from:
https://www.who.int/fr/news-room/fact-sheets/detail/malnutrition
|
| [2] |
United Nations Children’s Fund (UNICEF), World Health Organization, International Bank for Reconstruction and Development/The World Bank. Levels and trends in child malnutrition: UNICEF / WHO / World Bank Group Joint Child Malnutrition Estimates. Key findings of the 2025 edition. Geneva: World Health Organization; 2025. Licence: CC BY-NC-SA 3.0 IGO.
|
| [3] |
Islam MM, Sanin KI, Mahfuz M, Ahmed AMS, Mondal D, Haque R, Ahmed T. Risk factors of stunting among children living in an urban slum of Bangladesh: findings of a prospective cohort study. BMC Public Health. 2018 Jan 30; 18(1): 197.
https://doi.org/10.1186/s12889-018-5101-x
|
| [4] |
Acquah E, Darteh EKM, Amu H, Adjei DKA. Predictors of underweight in children under-five years in Ghana. Ghana Med J. 2019 Mar; 53(1): 71-78.
https://doi.org/10.4314/gmj.v53i1.11
|
| [5] |
Akombi BJ, Agho KE, Hall JJ, Wali N, Renzaho AMN, Merom D. Stunting, Wasting and Underweight in Sub-Saharan Africa: A Systematic Review. Int J Environ Res Public Health. 2017 Aug 1; 14(8): 863.
https://doi.org/10.3390/ijerph14080863
|
| [6] |
United Nations Children’s Fund (UNICEF). The State of the World’s Children 2019: Children, Food and Nutrition — Growing Well in a Changing World. New York: UNICEF; 2019 [cited 2025 Nov 5]. Available from:
https://www.unicef.org/media/62526/file/La-situation-des-enfants-dans-le-monde-2019.pdf
|
| [7] |
United Nations Children’s Fund (UNICEF). UNICEF Nutrition Strategy 2020–2030. New York: UNICEF; 2020 [cited 2025 Nov 5]. Available from:
https://www.unicef.org/media/92031/file/UNICEF%20Nutrition%20Strategy%202020-2030.pdf
|
| [8] |
Obasohan PE, Walters SJ, Jacques R, Khatab K. Risk Factors Associated with Malnutrition among Children Under-Five Years in Sub-Saharan African Countries: A Scoping Review. Int J Environ Res Public Health. 2020 Nov 26; 17(23): 8782.
https://doi.org/10.3390/ijerph17238782
|
| [9] |
FAO, FIDA, UNICEF, WFP, WHO. The State of Food Security and Nutrition in the World 2025: Addressing high food price inflation for food security and nutrition. Rome: FAO; 2025 [cited 2025 Nov 5]. Available from:
https://doi.org/10.4060/cd6008en
|
| [10] |
World Health Organization (WHO). Global hunger declines, but rises in Africa and western Asia: UN report. Geneva: WHO; 2025 Jul 28 [cited 2025 Nov 5]. Available from:
https://www.who.int/fr/news/item/28-07-2025-global-hunger-declines-but-rises-in-africa-and-western-asia-un-report
|
| [11] |
ANSD (Agence nationale de la statistique et de la démographie) [Senegal], ICF. Sénégal: Enquête démographique de santé continue 2023: Rapport final [Senegal Continuous Demographic and Health Survey 2023: Final report]. Dakar (Senegal) and Rockville (MD, USA): ANSD and ICF; 2024 [cited 2025 Nov 4]. Available from:
https://www.ansd.sn/sites/default/files/2025-10/EDSC%202023_Rapport%20final_30_Octobre_2025_OK.pdf
|
| [12] |
Nene M. État de la nutrition au Sénégal [Nutrition situation in Senegal]. In: Analyse et perspectives: 15 années d’expérience dans le développement de la politique de nutrition au Sénégal [Analysis and perspectives: 15 years of experience in the development of nutrition policy in Senegal]. Washington (DC): World Bank; Dakar: Cellule de Lutte contre la Malnutrition; 2018 [cited 2025 Nov 5]. Available from:
https://thedocs.worldbank.org/en/doc/946681594229136241-0090022020/original/1NutritionSituationFREFINAL.pdf
|
| [13] |
Diouf JBN, Sougou N, Tall C, Kane M, Sarr LP, Ndiaye O. Prevalence and factors associated with deficiency malnutrition in the health district of Guediawaye, Senegal. J Pediatr Neonatol. 2021; 3(2): 1–6.
https://doi.org/10.33425/2689-1085.1021
|
| [14] |
Action and Development (ACDEV). Dakar (Senegal): Action and Development; [cited 2026 Feb 12]. Available from:
https://acdev-inter.org/
|
| [15] |
Ministry of Health and Social Action of Senegal. Directorate of Maternal and Child Health. Dakar: Ministry of Health and Social Action; [cited 2026 Feb 12]. Available from:
https://www.sante.gouv.sn/les-directions/la-direction-de-la-sant%C3%A9-de-la-m%C3%A8re-et-de-l%E2%80%99enfant
|
| [16] |
King Baudoin Foundation. Brussels (Belgium): King Baudoin Foundation; [cited 2026 Feb 12]. Available from:
https://kbs-frb.be/en/home
|
| [17] |
SENEGEL—Senegalese Next Generation of Leaders. Commune de Medina Gounass. Dakar (Senegal): SENEGEL; [cited 2026 Feb 12]. Available from:
https://www.senegel.org/fr/senegal/organizations/orgdetails/733
|
| [18] |
Hapsari P. The application of UNICEF’s 2020 conceptual framework of maternal and child nutrition in Indonesia. 2020 [cited 2025 Nov 5]. Available from:
https://www.researchgate.net/publication/349161215_The_Application_of_UNICEF'S_2020_Conceptual_Framework_of_Maternal_and_Child_Nutrition_in_Indonesia
|
| [19] |
Harding KL, Aguayo VM, Webb P. Factors associated with wasting among children under five years old in South Asia: Implications for action. PLoS One. 2018 Jul 3; 13(7): e0198749.
https://doi.org/10.1371/journal.pone.0198749
|
| [20] |
Mu’Alifah U, Lutfiasari E, Riyatno IP. Association between exclusive breastfeeding and stunting in children: a systematic review. Teikyo Med J. 2022; 45(6): 6711. Available from:
https://www.teikyomedicaljournal.com/volume/TMJ/45/06/association-between-exclusive-breastfeeding-and-stunting-in-children-a-systematic-review-62e0db73ba1f7.pdf
|
| [21] |
Hadi H, Fatimatasari F, Irwanti W, Kusuma C, Alfiana RD, Asshiddiqi MIN, Nugroho S, Lewis EC, Gittelsohn J. Exclusive Breastfeeding Protects Young Children from Stunting in a Low-Income Population: A Study from Eastern Indonesia. Nutrients. 2021 Nov 26; 13(12): 4264.
https://doi.org/10.3390/nu13124264
|
| [22] |
Shrestha SK, Vicendese D, Erbas B. Water, sanitation and hygiene practices associated with improved height-for-age, weight-for-height and weight-for-age z-scores among under-five children in Nepal. BMC Pediatr. 2020 Mar 23; 20(1): 134.
https://doi.org/10.1186/s12887-020-2010-9
|
| [23] |
Mardani RAD, Wu WR, Nhi VT, Huang HC. Association of breastfeeding with undernutrition among children under 5 years of age in developing countries: A systematic review and meta-analysis. J Nurs Scholarsh. 2022 Nov; 54(6): 692-703.
https://doi.org/10.1111/jnu.12799
Epub 2022 Jul 18.
|
Cite This Article
-
APA Style
Namndiro, G. P. O., Edekoyo, R. M., Ndiaye, S., Tine, J. A. D. (2026). High Burden of Child Undernutrition and Associated Factors Among Children Aged 6–59 Months in
a Peri-urban Setting of Dakar, Senegal. Central African Journal of Public Health, 12(2), 84-104. https://doi.org/10.11648/j.cajph.20261202.14
 Copy
|
Copy
|
 Download
Download
ACS Style
Namndiro, G. P. O.; Edekoyo, R. M.; Ndiaye, S.; Tine, J. A. D. High Burden of Child Undernutrition and Associated Factors Among Children Aged 6–59 Months in
a Peri-urban Setting of Dakar, Senegal. Cent. Afr. J. Public Health 2026, 12(2), 84-104. doi: 10.11648/j.cajph.20261202.14
Copy
|
Download
AMA Style
Namndiro GPO, Edekoyo RM, Ndiaye S, Tine JAD. High Burden of Child Undernutrition and Associated Factors Among Children Aged 6–59 Months in
a Peri-urban Setting of Dakar, Senegal. Cent Afr J Public Health. 2026;12(2):84-104. doi: 10.11648/j.cajph.20261202.14
Copy
|
Download
-
@article{10.11648/j.cajph.20261202.14,
author = {Gad Papin Oholiab Namndiro and Raphaela Maporo Edekoyo and Seynabou Ndiaye and Jean Augustin Diegane Tine},
title = {High Burden of Child Undernutrition and Associated Factors Among Children Aged 6–59 Months in
a Peri-urban Setting of Dakar, Senegal},
journal = {Central African Journal of Public Health},
volume = {12},
number = {2},
pages = {84-104},
doi = {10.11648/j.cajph.20261202.14},
url = {https://doi.org/10.11648/j.cajph.20261202.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cajph.20261202.14},
abstract = {Malnutrition remains a major public health challenge in low- and middle-income countries and contributes substantially to child mortality. In Senegal, it accounts for approximately one third of neonatal, infant, and under-five deaths. Although the Dakar region reports comparatively lower prevalence rates than other regions nationwide, undernutrition remains a serious concern in socioeconomically disadvantaged peri-urban communities where poverty, limited health infrastructure, and poor living conditions increase children’s vulnerability. In the municipality of Medina Gounass, located in the health district of Guediawaye in the suburbs of Dakar, structural poverty, high unemployment, and limited access to sanitation services create a particularly challenging environment for child health and nutrition. This study aimed to identify factors associated with wasting, stunting, and underweight among children aged 6–59 months in this vulnerable setting. An observational cross-sectional study with descriptive and analytical components was conducted from September 13 to 18, 2025. A total of 226 child-mother/caregiver pairs were included. Anthropometric measurements were collected to assess nutritional status using weight-for-height, height-for-age, and weight-for-age indices based on WHO z-score standards. Bivariate and multivariate logistic regression analyses were performed to identify factors independently associated with the different forms of undernutrition. Wasting affected 38 children (16.8%), including 7.5% with severe wasting, indicating a very high prevalence according to WHO classification thresholds. It was independently associated with the absence of a household handwashing facility (aOR=6.32; 95% CI: 1.85–21.56). Stunting was observed in 36 children (15.9%), including 4.0% severe cases, and was significantly associated with lack of exclusive breastfeeding during the first six months of life (aOR=4.28; 95% CI: 1.91–9.57). Underweight affected 39 children (17.2%), including 6.6% severe cases, and was independently associated with the absence of a household handwashing facility (aOR=10.33; 95% CI: 2.38–44.86) and lack of exclusive breastfeeding (aOR=3.79; 95% CI: 1.70–8.44). These findings highlight the substantial burden of child undernutrition in this disadvantaged peri-urban setting and underscore the critical role of household hygiene conditions and early infant feeding practices in shaping nutritional outcomes. Strengthening community-based interventions that promote hand hygiene and exclusive breastfeeding may contribute to reducing undernutrition in low-income urban settings.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - High Burden of Child Undernutrition and Associated Factors Among Children Aged 6–59 Months in
a Peri-urban Setting of Dakar, Senegal
AU - Gad Papin Oholiab Namndiro
AU - Raphaela Maporo Edekoyo
AU - Seynabou Ndiaye
AU - Jean Augustin Diegane Tine
Y1 - 2026/03/23
PY - 2026
N1 - https://doi.org/10.11648/j.cajph.20261202.14
DO - 10.11648/j.cajph.20261202.14
T2 - Central African Journal of Public Health
JF - Central African Journal of Public Health
JO - Central African Journal of Public Health
SP - 84
EP - 104
PB - Science Publishing Group
SN - 2575-5781
UR - https://doi.org/10.11648/j.cajph.20261202.14
AB - Malnutrition remains a major public health challenge in low- and middle-income countries and contributes substantially to child mortality. In Senegal, it accounts for approximately one third of neonatal, infant, and under-five deaths. Although the Dakar region reports comparatively lower prevalence rates than other regions nationwide, undernutrition remains a serious concern in socioeconomically disadvantaged peri-urban communities where poverty, limited health infrastructure, and poor living conditions increase children’s vulnerability. In the municipality of Medina Gounass, located in the health district of Guediawaye in the suburbs of Dakar, structural poverty, high unemployment, and limited access to sanitation services create a particularly challenging environment for child health and nutrition. This study aimed to identify factors associated with wasting, stunting, and underweight among children aged 6–59 months in this vulnerable setting. An observational cross-sectional study with descriptive and analytical components was conducted from September 13 to 18, 2025. A total of 226 child-mother/caregiver pairs were included. Anthropometric measurements were collected to assess nutritional status using weight-for-height, height-for-age, and weight-for-age indices based on WHO z-score standards. Bivariate and multivariate logistic regression analyses were performed to identify factors independently associated with the different forms of undernutrition. Wasting affected 38 children (16.8%), including 7.5% with severe wasting, indicating a very high prevalence according to WHO classification thresholds. It was independently associated with the absence of a household handwashing facility (aOR=6.32; 95% CI: 1.85–21.56). Stunting was observed in 36 children (15.9%), including 4.0% severe cases, and was significantly associated with lack of exclusive breastfeeding during the first six months of life (aOR=4.28; 95% CI: 1.91–9.57). Underweight affected 39 children (17.2%), including 6.6% severe cases, and was independently associated with the absence of a household handwashing facility (aOR=10.33; 95% CI: 2.38–44.86) and lack of exclusive breastfeeding (aOR=3.79; 95% CI: 1.70–8.44). These findings highlight the substantial burden of child undernutrition in this disadvantaged peri-urban setting and underscore the critical role of household hygiene conditions and early infant feeding practices in shaping nutritional outcomes. Strengthening community-based interventions that promote hand hygiene and exclusive breastfeeding may contribute to reducing undernutrition in low-income urban settings.
VL - 12
IS - 2
ER -
Copy
|
Download