This study aimed to develop and validate a nomogram for predicting ICU mortality risk in patients with spinal fractures to improve prognostic accuracy. Using data from 1,146 patients in the eICU Collaborative Research Database, independent risk factors—including age, BMI, APACHE IV score, admission source, mechanical ventilation, spinal cord injury, sepsis, oxygen saturation, white blood cell count, hemoglobin, and glucose—were identified via forward stepwise logistic regression and incorporated into the nomogram. The model demonstrated excellent performance, with AUCs of 0.902 (0.857–0.938) in the training cohort and 0.903 (0.825–0.953) in the validation cohort, significantly outperforming APACHE IV according to the DeLong test. Further validation via Hosmer-Lemeshow test, calibration curves, NRI, IDI, and DCA confirmed the nomogram’s superior calibration and clinical utility. As the first comprehensive predictive tool of its kind for spinal fracture patients, this nomogram offers improved mortality risk estimation and supports clinical decision-making.
| Published in | Clinical Medicine Research (Volume 14, Issue 5) |
| DOI | 10.11648/j.cmr.20251405.12 |
| Page(s) | 169-180 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Spinal Fractures, ICU Mortality, eICU Collaborative Research Database, Prognosis, Nomogram
level | Training cohort | Validation cohort | p-value |
|---|---|---|---|
802 | 344 | ||
Age (year) | 56.00 (38.00, 74.00) | 54.00 (34.00, 69.00) | 0.066 |
Gender (%) | 0.960 | ||
Male | 510 (63.6) | 220 (64.0) | |
Female | 292 (36.4) | 124 (36.0) | |
Ethnicity (%) | 0.949 | ||
White | 672 (83.8) | 287 (83.4) | |
Others | 130 (16.2) | 57 (16.6) | |
BMI (kg/m2) | 26.46 (23.34, 30.55) | 25.88 (22.92, 30.05) | 0.308 |
APACHE IV | 46.00 (32.00, 66.00) | 43.00 (29.75, 65.00) | 0.086 |
Unit admit source (%) | 0.228 | ||
Emergency department | 589 (73.4) | 265 (77.0) | |
Others | 213 (26.6) | 79 (23.0) | |
Unit type (%) | 1.000 | ||
MICU/SICU | 574 (71.6) | 246 (71.5) | |
Others | 228 (28.4) | 98 (28.5) | |
Site of fracture (%) | 0.127 | ||
Cervical spine | 308 (38.4) | 123 (35.8) | |
Thoracic spine | 247 (30.8) | 99 (28.8) | |
Lumbar spine | 214 (26.7) | 97 (28.2) | |
Sacrum | 33 (4.1) | 25 (7.3) | |
Combined spinal cord injury (%) | 0.233 | ||
No | 751 (93.6) | 329 (95.6) | |
Yes | 51 (6.4) | 15 (4.4) | |
Combined with other fractures (%) | 0.093 | ||
No | 383 (47.8) | 145 (42.2) | |
Yes | 419 (52.2) | 199 (57.8) | |
Surgery (%) | 0.542 | ||
No | 682 (85.0) | 298 (86.6) | |
Yes | 120 (15.0) | 46 (13.4) | |
Vasopressors (%) | 0.721 | ||
No | 732 (91.3) | 311 (90.4) | |
Yes | 70 (8.7) | 33 (9.6) | |
Ventilator (%) | 0.535 | ||
No | 316 (39.4) | 143 (41.6) | |
Yes | 486 (60.6) | 201 (58.4) | |
Comorbidities | |||
Sepsis (%) | 0.547 | ||
No | 736 (91.8) | 320 (93.0) | |
Yes | 66 (8.2) | 24 (7.0) | |
CHF (%) | 1.000 | ||
No | 767 (95.6) | 329 (95.6) | |
Yes | 35 (4.4) | 15 (4.4) | |
Hypertension (%) | 0.895 | ||
No | 719 (89.7) | 310 (90.1) | |
Yes | 83 (10.3) | 34 (9.9) | |
Stroke (%) | 0.668 | ||
No | 773 (96.4) | 334 (97.1) | |
Yes | 29 (3.6) | 10 (2.9) | |
COPD (%) | 0.134 | ||
No | 744 (92.8) | 328 (95.3) | |
Yes | 58 (7.2) | 16 (4.7) | |
Renal failure (%) | 0.064 | ||
No | 791 (98.6) | 344 (100.0) | |
Yes | 11 (1.4) | 0 (0.0) | |
Liver disease (%) | 0.428 | ||
No | 796 (99.3) | 339 (98.5) | |
Yes | 6 (0.7) | 5 (1.5) | |
Diabetes (%) | 0.423 | ||
No | 713 (88.9) | 312 (90.7) | |
Yes | 89 (11.1) | 32 (9.3) | |
Cancer (%) | 0.064 | ||
No | 733 (91.4) | 326 (94.8) | |
Yes | 69 (8.6) | 18 (5.2) | |
Vital signs | |||
Heart rate (min-1) | 87.00 (73.00, 101.00) | 87.00 (75.00, 101.00) | 0.571 |
BP (mmHg) | 121.00 (108.00, 137.00) | 120.00 (107.00, 134.00) | 0.289 |
Respiratory rate (min-1) | 18.00 (15.00, 21.00) | 18.00 (15.00, 21.00) | 0.479 |
Temperature (°F) | 98.40 (97.70, 99.10) | 98.40 (97.90, 99.10) | 0.643 |
SaO2 (%) | 98.00 (96.00, 100.00) | 98.00 (96.00, 100.00) | 0.422 |
Laboratory test results | |||
WBC (K/mcL) | 10.20 (8.00, 13.29) | 10.18 (7.90, 13.80) | 0.829 |
RBC (K/mcL) | 3.76 (3.24, 4.19) | 3.62 (3.14, 4.11) | 0.048 |
HGB (g/dL) | 11.40 (9.80, 12.90) | 11.30 (9.60, 12.70) | 0.215 |
HCT (%) | 34.30 (29.42, 38.30) | 33.25 (28.67, 37.70) | 0.062 |
MCHC (g/dL) | 33.60 (32.80, 34.30) | 33.70 (33.00, 34.40) | 0.082 |
MCH (pg) | 30.40 (29.20, 31.60) | 30.50 (29.67, 31.60) | 0.164 |
MCV (fL) | 90.50 (87.00, 94.07) | 91.00 (87.90, 93.90) | 0.423 |
RDW (%) | 13.80 (13.00, 14.70) | 13.90 (13.10, 14.72) | 0.560 |
Platelets (K/mcL) | 176.00 (134.00, 226.75) | 169.50 (130.00, 225.00) | 0.204 |
AG (mmol/L) | 9.85 (7.00, 12.00) | 9.40 (7.00, 12.00) | 0.637 |
Bicarbonate (mmol/L) | 24.00 (22.00, 27.00) | 25.00 (22.00, 27.00) | 0.619 |
Sodium (mmol/L) | 139.00 (137.00, 141.00) | 139.00 (137.00, 141.00) | 0.720 |
Potassium (mmol/L) | 4.00 (3.80, 4.40) | 4.10 (3.80, 4.40) | 0.802 |
Chloride (mmol/L) | 106.00 (103.00, 110.00) | 106.00 (103.00, 110.00) | 0.652 |
Calcium (mmol/L) | 8.20 (7.70, 8.70) | 8.10 (7.70, 8.50) | 0.075 |
Glucose (mg/dL) | 122.50 (105.00, 144.00) | 125.50 (106.75, 148.25) | 0.388 |
Creatinine (mg/dL) | 0.81 (0.68, 1.08) | 0.80 (0.67, 1.00) | 0.155 |
BUN (mg/dL) | 15.00 (11.00, 20.00) | 14.00 (10.00, 20.00) | 0.213 |
OR | 95% CI | P-value | ||
|---|---|---|---|---|
Age | 1.022 | 1.007 | 1.038 | 0.005 |
BMI | 0.915 | 0.859 | 0.968 | 0.003 |
APACHE IV | 1.050 | 1.037 | 1.065 | <0.001 |
Unit admit source | 0.002 | |||
Emergency department | reference | |||
Others | 0.292 | 0.129 | 0.620 | |
Ventilator | 0.005 | |||
No | reference | |||
Yes | 4.199 | 1.639 | 12.629 | |
Combined spinal cord injury | 0.010 | |||
No | reference | |||
Yes | 4.301 | 1.332 | 12.555 | |
Sepsis | 0.016 | |||
No | reference | |||
Yes | 2.832 | 1.186 | 6.574 | |
SaO2 | 0.830 | 0.741 | 0.920 | 0.001 |
WBC | 1.068 | 1.011 | 1.126 | 0.017 |
HGB | 0.728 | 0.607 | 0.865 | <0.001 |
Glucose | 1.008 | 1.002 | 1.013 | 0.009 |
ICU | Intensive Care Unit |
APACHE | Acute Physiology and Chronic Health Evaluation |
APS | Acute Physiology Score |
eICU-CRD | eICU Collaborative Research Database |
MIT | Massachusetts Institute of Technology |
ICD-9-CM | International Classification of Diseases, Ninth Revision, Clinical Modification |
BMI | Body Mass Index |
MICU | Medical Intensive Care Unit |
SICU | Surgical Intensive Care Unit |
CHF | Congestive Heart Failure |
COPD | Chronic Obstructive Pulmonary Disease |
HR | Heart Rate |
MAP | Mean Arterial Pressure |
RR | Respiratory Rate |
SaO2 | Arterial Oxygen Saturation |
WBC | White Blood Cell |
RBC | Red Blood Cell |
RDW | Red Blood Cell Distribution Width |
MCV | Mean Corpuscular Volume |
MCH | Mean Corpuscular Hemoglobin |
MCHC | Mean Corpuscular Hemoglobin Concentration |
AG | Anion Gap |
BUN | Blood Urea Nitrogen |
IQR | Interquartile Range |
CI | Confidence Interval |
VIF | Variance Inflation Factor |
ROC | Receiver Operating Characteristic |
AUC | The Area Under the ROC Curve |
IDI | Integrated Discrimination Improvement |
NRI | Net Reclassification Index |
DCA | Decision-Curve Analysis |
SCI | Spinal Cord Injury |
| [1] | Doud, A. N., et al., Has the incidence of thoracolumbar spine injuries increased in the United States from 1998 to 2011? Clin Orthop Relat Res, 2015. 473(1): p. 297-304. |
| [2] | Oliver, M., et al., The changing epidemiology of spinal trauma: a 13-year review from a Level I trauma centre. Injury, 2012. 43(8): p. 1296-300. |
| [3] | Dreimann, M., et al., [Minimally invasive posterior and anterior stabilization of the thoracolumbar spine after traumatic injuries]. Unfallchirurg, 2020. 123(10): p. 752-763. |
| [4] | Munhoz da Rocha Lemos Costa, T., et al., Bone mineral density and vertebral fractures and their relationship with pulmonary dysfunction in patients with chronic obstructive pulmonary disease. Osteoporos Int, 2018. 29(11): p. 2537-2543. |
| [5] | Battisti, S., et al., Vertebral fractures and mortality risk in hospitalised patients during the COVID-19 pandemic emergency. Endocrine, 2021. 74(3): p. 461-469. |
| [6] | Niemi-Nikkola, V., et al., Long-term Posttraumatic Survival of Spinal Fracture Patients in Northern Finland. Spine (Phila Pa 1976), 2018. 43(23): p. 1657-1663. |
| [7] | Curtis, J. R., et al., Is withholding osteoporosis medication after fracture sometimes rational? A comparison of the risk for second fracture versus death. J Am Med Dir Assoc, 2010. 11(8): p. 584-91. |
| [8] | Hyde-Wyatt, J. P., Managing hyperactive delirium and spinal immobilisation in the intensive care setting: a case study and reflective discussion of the literature. Intensive Crit Care Nurs, 2014. 30(3): p. 138-44. |
| [9] | Zimmerman, J. E., et al., Acute Physiology and Chronic Health Evaluation (APACHE) IV: hospital mortality assessment for today's critically ill patients. Crit Care Med, 2006. 34(5): p. 1297-310. |
| [10] | Rahmatinejad, Z., et al., Prognostic utilization of models based on the APACHE II, APACHE IV, and SAPS II scores for predicting in-hospital mortality in emergency department. Am J Emerg Med, 2020. 38(9): p. 1841-1846. |
| [11] | Dosi, R., et al., The predictive ability of SAPS II, APACHE II, SAPS III, and APACHE IV to assess outcome and duration of mechanical ventilation in respiratory intensive care unit. Lung India, 2021. 38(3): p. 236-240. |
| [12] | Lee, H., et al., Validation of the APACHE IV model and its comparison with the APACHE II, SAPS 3, and Korean SAPS 3 models for the prediction of hospital mortality in a Korean surgical intensive care unit. Korean J Anesthesiol, 2014. 67(2): p. 115-22. |
| [13] | Li, Z., et al., Dual-energy CT-based radiomics nomogram in predicting histological differentiation of head and neck squamous carcinoma: a multicenter study. Neuroradiology, 2022. 64(2): p. 361-369. |
| [14] | Spolverato, G., et al., Development of a Prognostic Nomogram and Nomogram Software Application Tool to Predict Overall Survival and Disease-Free Survival After Curative-Intent Gastrectomy for Gastric Cancer. Ann Surg Oncol, 2022. 29(2): p. 1220-1229. |
| [15] | Pollard, T. J., et al., The eICU Collaborative Research Database, a freely available multi-center database for critical care research. Sci Data, 2018. 5: p. 180178. |
| [16] | Cheng, J., et al., A variable selection method based on mutual information and variance inflation factor. Spectrochim Acta A Mol Biomol Spectrosc, 2022. 268: p. 120652. |
| [17] | Bencivenga, L., G. Rengo, and G. Varricchi, Elderly at time of COronaVIrus disease 2019 (COVID-19): possible role of immunosenescence and malnutrition. Geroscience, 2020. 42(4): p. 1089-1092. |
| [18] | Kang, S. J. and S. I. Jung, Age-Related Morbidity and Mortality among Patients with COVID-19. Infect Chemother, 2020. 52(2): p. 154-164. |
| [19] | Esme, M., et al., Infections in the Elderly Critically-Ill Patients. Front Med (Lausanne), 2019. 6: p. 118. |
| [20] | Viana, M. V., et al., Nutritional therapy and outcomes in underweight critically ill patients. Clin Nutr, 2020. 39(3): p. 935-941. |
| [21] | Bear, D. E., et al., The role of nutritional support in the physical and functional recovery of critically ill patients: a narrative review. Crit Care, 2017. 21(1): p. 226. |
| [22] | Tsai, J. R., et al., Adequacy of prescribed caloric and protein intake and reduction of mortality in critically ill patients with body mass indices <30 kg/m2. Nutrition, 2022. 94: p. 111529. |
| [23] | Hogue, C. W., Jr., et al., The impact of obesity on outcomes after critical illness: a meta-analysis. Intensive Care Med, 2009. 35(7): p. 1152-70. |
| [24] | Fehlings, M. G., et al., A Clinical Practice Guideline for the Management of Patients With Acute Spinal Cord Injury and Central Cord Syndrome: Recommendations on the Timing (≤24 Hours Versus >24 Hours) of Decompressive Surgery. Global Spine J, 2017. 7(3 Suppl): p. 195s-202s. |
| [25] | Jiang, F., et al., Acute Adverse Events After Spinal Cord Injury and Their Relationship to Long-term Neurologic and Functional Outcomes: Analysis From the North American Clinical Trials Network for Spinal Cord Injury. Crit Care Med, 2019. 47(11): p. e854-e862. |
| [26] | Failli, V., et al., Functional neurological recovery after spinal cord injury is impaired in patients with infections. Brain, 2012. 135(Pt 11): p. 3238-50. |
| [27] | Jaja, B. N. R., et al., Association of Pneumonia, Wound Infection, and Sepsis with Clinical Outcomes after Acute Traumatic Spinal Cord Injury. J Neurotrauma, 2019. 36(21): p. 3044-3050. |
| [28] | Rosca, A., et al., Mortality risk and antibiotic use for COVID-19 in hospitalized patients over 80. Biomed Pharmacother, 2022. 146: p. 112481. |
| [29] | Paolucci, M., M. P. Landini, and V. Sambri, How can the microbiologist help in diagnosing neonatal sepsis? Int J Pediatr, 2012. 2012: p. 120139. |
| [30] | Shapiro, M. J., et al., Anemia and blood transfusion in trauma patients admitted to the intensive care unit. J Trauma, 2003. 55(2): p. 269-73; discussion 273-4. |
| [31] | Kawai, Y., et al., Significance of initial hemoglobin levels in severe trauma patients without prehospital fluid administration: a single-center study in Japan. Trauma Surg Acute Care Open, 2021. 6(1): p. e000831. |
| [32] | Akiboye, F. and G. Rayman, Management of Hyperglycemia and Diabetes in Orthopedic Surgery. Curr Diab Rep, 2017. 17(2): p. 13. |
| [33] | Behanova, M., et al., The doubled burden of diabetic bone disease: hip fracture and post-hip fracture mortality. Eur J Endocrinol, 2021. 184(5): p. 627-636. |
| [34] | Laird, A. M., et al., Relationship of early hyperglycemia to mortality in trauma patients. J Trauma, 2004. 56(5): p. 1058-62. |
| [35] | Kerby, J. D., et al., Stress-induced hyperglycemia, not diabetic hyperglycemia, is associated with higher mortality in trauma. Ann Surg, 2012. 256(3): p. 446-52. |
APA Style
Shaojin, L., Wenxu, L. (2025). Construction of a Nomogram for Predicting ICU Mortality Risk in Patients with Spinal Fractures Based on the APACHE IV. Clinical Medicine Research, 14(5), 169-180. https://doi.org/10.11648/j.cmr.20251405.12
ACS Style
Shaojin, L.; Wenxu, L. Construction of a Nomogram for Predicting ICU Mortality Risk in Patients with Spinal Fractures Based on the APACHE IV. Clin. Med. Res. 2025, 14(5), 169-180. doi: 10.11648/j.cmr.20251405.12
@article{10.11648/j.cmr.20251405.12,
author = {Li Shaojin and Li Wenxu},
title = {Construction of a Nomogram for Predicting ICU Mortality Risk in Patients with Spinal Fractures Based on the APACHE IV
},
journal = {Clinical Medicine Research},
volume = {14},
number = {5},
pages = {169-180},
doi = {10.11648/j.cmr.20251405.12},
url = {https://doi.org/10.11648/j.cmr.20251405.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cmr.20251405.12},
abstract = {This study aimed to develop and validate a nomogram for predicting ICU mortality risk in patients with spinal fractures to improve prognostic accuracy. Using data from 1,146 patients in the eICU Collaborative Research Database, independent risk factors—including age, BMI, APACHE IV score, admission source, mechanical ventilation, spinal cord injury, sepsis, oxygen saturation, white blood cell count, hemoglobin, and glucose—were identified via forward stepwise logistic regression and incorporated into the nomogram. The model demonstrated excellent performance, with AUCs of 0.902 (0.857–0.938) in the training cohort and 0.903 (0.825–0.953) in the validation cohort, significantly outperforming APACHE IV according to the DeLong test. Further validation via Hosmer-Lemeshow test, calibration curves, NRI, IDI, and DCA confirmed the nomogram’s superior calibration and clinical utility. As the first comprehensive predictive tool of its kind for spinal fracture patients, this nomogram offers improved mortality risk estimation and supports clinical decision-making.
},
year = {2025}
}
TY - JOUR T1 - Construction of a Nomogram for Predicting ICU Mortality Risk in Patients with Spinal Fractures Based on the APACHE IV AU - Li Shaojin AU - Li Wenxu Y1 - 2025/09/23 PY - 2025 N1 - https://doi.org/10.11648/j.cmr.20251405.12 DO - 10.11648/j.cmr.20251405.12 T2 - Clinical Medicine Research JF - Clinical Medicine Research JO - Clinical Medicine Research SP - 169 EP - 180 PB - Science Publishing Group SN - 2326-9057 UR - https://doi.org/10.11648/j.cmr.20251405.12 AB - This study aimed to develop and validate a nomogram for predicting ICU mortality risk in patients with spinal fractures to improve prognostic accuracy. Using data from 1,146 patients in the eICU Collaborative Research Database, independent risk factors—including age, BMI, APACHE IV score, admission source, mechanical ventilation, spinal cord injury, sepsis, oxygen saturation, white blood cell count, hemoglobin, and glucose—were identified via forward stepwise logistic regression and incorporated into the nomogram. The model demonstrated excellent performance, with AUCs of 0.902 (0.857–0.938) in the training cohort and 0.903 (0.825–0.953) in the validation cohort, significantly outperforming APACHE IV according to the DeLong test. Further validation via Hosmer-Lemeshow test, calibration curves, NRI, IDI, and DCA confirmed the nomogram’s superior calibration and clinical utility. As the first comprehensive predictive tool of its kind for spinal fracture patients, this nomogram offers improved mortality risk estimation and supports clinical decision-making. VL - 14 IS - 5 ER -
Department of Orthopedics, Guangzhou Red Cross Hospital (Guangzhou Red Cross Hospital of Jinan University), Guangzhou, China
Department of Orthopedics, Guangzhou Red Cross Hospital (Guangzhou Red Cross Hospital of Jinan University), Guangzhou, China
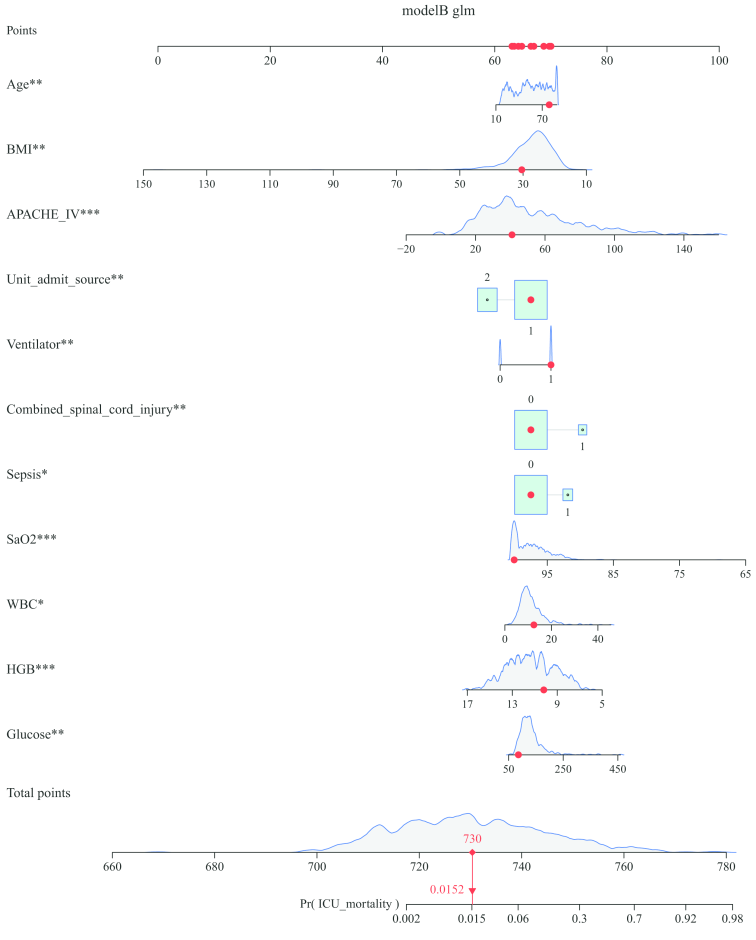
Figure 1. Nomogram (model B) for predicting ICU mortality risk in patients with spinal fractures.
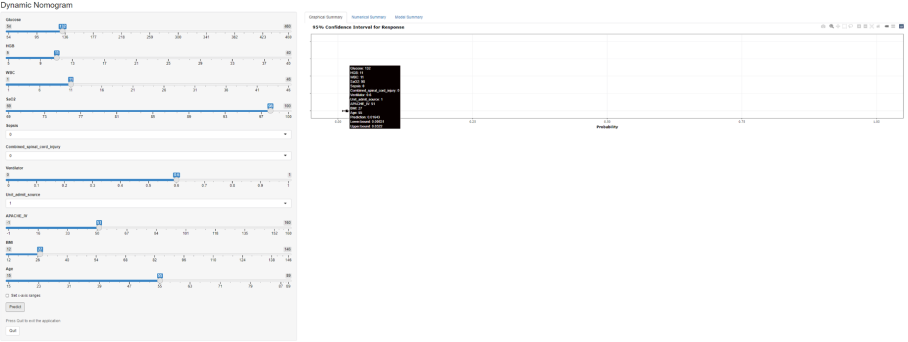
Figure 2. The ICU mortality risk for patients with spinal fractures, and its page.
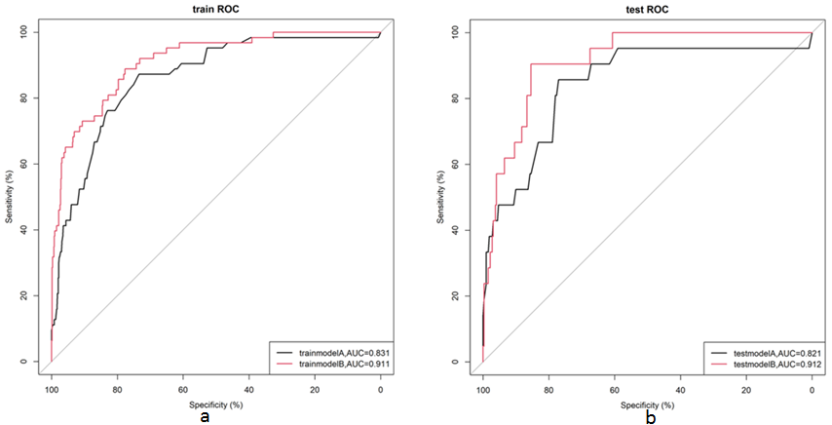
Figure 3. ROC curves for the APACHE IV model (model A) and the nomogram (model B).
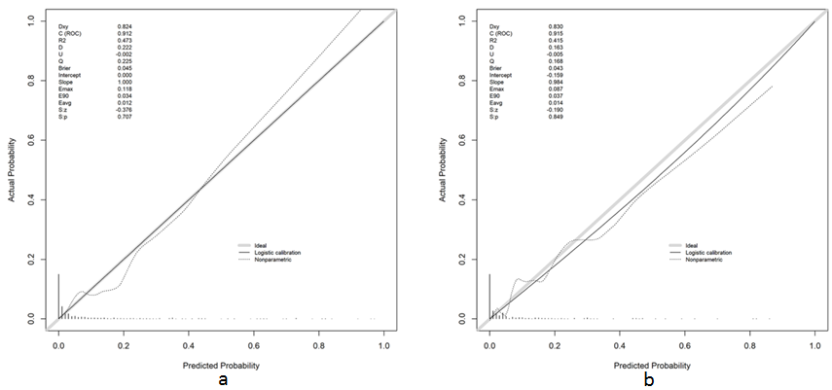
Figure 4. Calibration curves for the validation cohort and the training cohort.
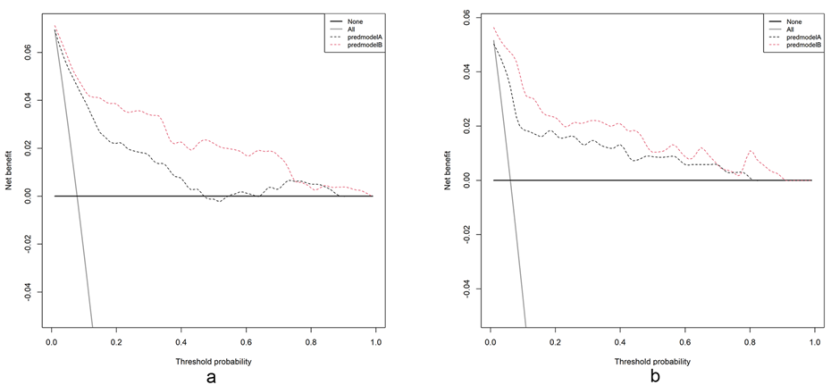
Figure 5. Decision-curve analysis of the validation cohort and the training cohort. Model A represents the APACHE IV model, and model B represents the nomogram.
Information

