Abstract
Orthopedic trauma patients with limited mobility and prolonged bed rest are at high risk of venous thromboembolism and pulmonary embolism (PE). When acute hypoxemia and respiratory dysfunction occur in such patients, it is clinically challenging to distinguish PE from acute exacerbation of underlying chronic obstructive pulmonary disease (COPD) or asthma, which directly affects perioperative safety. This study aimed to summarize the diagnostic thinking and standardized anesthetic management strategies for this type of high-risk emergency patient. We reported a 68-year-old male patient diagnosed with L2 burst fracture, who presented with severe hypoxemia (room-air SpO2 75%) before emergency surgery. Combined with the patient’s medical history, lung auscultation, arterial blood gas analysis and chest computed tomography (CT) findings, we rapidly confirmed that hypoxemia was caused by acute airway obstruction rather than PE. Pre-intubation interventions including bronchodilators, corticosteroids and airway surface anesthesia were applied to prevent intraoperative bronchospasm. Intraoperative lung-protective ventilation was implemented, and stepwise respiratory support was adopted after extubation. The patient had an uneventful perioperative course and was discharged on the 5th postoperative day. In conclusion, for immobilized orthopedic trauma patients complicated with chronic airway diseases and acute respiratory abnormalities, comprehensive differential diagnosis combining clinical manifestations and auxiliary examinations is the premise of safe treatment. Targeted pre-operative prevention, standardized intraoperative ventilation and graded postoperative respiratory care can effectively reduce perioperative respiratory complications.
Keywords
Emergency Orthopedic Surgery, COPD, Asthma, Differential Diagnosis, Pulmonary Embolism, Lung-protective Ventilation, Peri-extubation Management
1. Introduction
Orthopedic trauma patients frequently suffer from activity disorders and prolonged bed rest. Trauma-induced hypercoagulability increases the risk of deep vein thrombosis and potentially fatal pulmonary embolism (PE)
| [1] | Wills, J. H., Gaski, G. E. Update on venous thromboembolism in orthopaedic trauma surgery. Journal of the American Academy of Orthopaedic Surgeons. 2024, 32(19), e961-e969.
https://doi.org/10.5435/JAAOS-D-23-06863 |
[1]
. When acute respiratory dysfunction or hypoxemia develops in these patients, systematic differential diagnosis combining past medical history, clinical manifestations, D-dimer levels, and imaging studies is essential to differentiate PE from chronic respiratory diseases such as COPD and asthma
| [2] | Woods, B. D., Sladen, R. N. Perioperative considerations for the patient with asthma and bronchospasm. British Journal of Anaesthesia. 2009, 103(Suppl 1), i57-i65.
https://doi.org/10.1093/bja/aep301 |
[2]
. Clinicians need to master the diagnostic criteria for acute PE in patients complicated with COPD, so as to avoid missed diagnosis and misdiagnosis
| [3] | Lesser, B. A., Leeper, K. V., Jr., Stein, P. D., Saltzman, H. A., Chen, J., Thompson, B. T., Hales, C. A. The diagnosis of acute pulmonary embolism in patients with chronic obstructive pulmonary disease. Chest. 1992, 102(1), 17-22.
https://doi.org/10.1378/chest.102.1.17 |
[3]
. For asthma patients undergoing surgery, standardized perioperative assessment and intervention are essential to reduce airway-related adverse events
| [4] | Bayable, S. D., Melesse, D. Y., Lema, G. F., Ahmed, S. A. Perioperative management of patients with asthma during elective surgery: A systematic review. Annals of Medicine and Surgery. 2021, 70, 102874.
https://doi.org/10.1016/j.amsu.2021.102874 |
[4]
. Meanwhile, it is necessary to formulate targeted diagnosis and treatment plans for acute exacerbation of COPD in acute care settings
| [5] | Celli, B. R., Fabbri, L. M., Aaron, S. D., Agusti, A., Brook, R. D., Criner, G. J., Han, M. K., Martinez, F. J., Roche, C. M., Wedzicha, J. A. Differential diagnosis of suspected chronic obstructive pulmonary disease exacerbations in the acute care setting: Best practice. American Journal of Respiratory and Critical Care Medicine. 2023, 207(9), 1134-1144.
https://doi.org/10.1164/rccm.202206-1210CI |
[5]
. For patients with unexplained deterioration of respiratory function in COPD, PE is always an important differential diagnosis item
| [6] | Tillie-Leblond, I., Marquette, C. H., Perez, T., Scherpereel, A., Dehoux, M., Cotte, E., Leroy, S., Weitzenblum, E., Chaouat, A. Pulmonary embolism in patients with unexplained exacerbation of chronic obstructive pulmonary disease: prevalence and risk factors. Annals of Internal Medicine. 2006, 144(6), 390-396. https://doi.org/10.7326/0003-4819-144-6-390 |
[6]
.
2. Case Presentation
2.1. Patient Information
A 68 year old male, 155 cm tall and weighing 60 kg, was admitted on June 3, 2025, with 5 days of low back and left thigh pain following a fall. He had restricted movement and required strict bed rest after injury.
2.2. Past Medical History
1) Hypertension for 5 years with irregular medication.
2) Childhood onset asthma, exacerbated by cold exposure, without regular anti asthma treatment.
3) Long term chronic bronchitis reported by family.
4) History of right hernia surgery more than 50 years ago.
2.3. Key Auxiliary Examinations
1) D dimer: 1.93 mg/L (elevated). Laboratory indicators such as D-dimer play an important auxiliary role in screening PE among high-risk orthopedic patients
| [7] | Borowski, B., Haratym, M., Piech, P., Jarecki, J., Staśkiewicz, G. D-dimers or more? Assessing the role of laboratory factors in predicting and confirming pulmonary embolism in high-risk orthopedic patients. Pract Lab Med. 2025, 44, e00452.
https://doi.org/10.1016/j.plabm.2025.e00452 |
[7]
.
2) Lumbar MRI: L2 burst fracture with spinal canal stenosis.
3) Chest CT: bilateral chronic pulmonary inflammation; no evidence of PE, pneumothorax, or massive pleural effusion. Computed tomography pulmonary angiography is the mainstream imaging method for detecting PE in trauma population
| [8] | Yaghoobpoor, S., Fathi, M., Taher, H. J., Farhood, A. J., Bahrami, A., Eshraghi, R., Hajibeygi, R., Tutunchian, Z., Myers, L., Ahmadi, R., Gholamrezanezhad, A. Computed tomography pulmonary angiography (CTPA) for the detection of pulmonary embolism (PE) among trauma patients: a systematic review and meta-analysis. Emerg Radiol. 2024, 31(4), 567-580. https://doi.org/10.1007/s10140-024-02249-7 |
[8]
.
4) Echocardiography: no acute right heart dysfunction; left ventricular ejection fraction 68%.
5) Lower extremity venous ultrasound: no deep vein thrombosis. Blunt chest trauma combined with long bone fracture can easily induce early-onset PE
| [9] | Thivaharan, Y., Dayapala, A., Thanushan, M. A case of early pulmonary embolism following blunt trauma to chest and a long bone fracture. Egyptian Journal of Forensic Sciences. 2023, 13(1), 9. https://doi.org/10.1186/s41935-023-00327-4 |
[9]
. Occult PE is not rare in patients with lower limb fractures, which requires clinicians to stay highly alert
| [10] | Di, L., Chen, Z., Wang, X. Y., Zhang, J., Zhang, J., Ding, J. Q. Early diagnosis of occult pulmonary embolism secondary to lower limb fractures: summary of 18 cases. Front Med (Lausanne). 2024, 11, 1355030.
https://doi.org/10.3389/fmed.2024.1355030 |
[10]
.
2.4. Ethical Approval and Informed Consent
This retrospective case report was based on routine clinical practice without additional investigational interventions, so ethical approval was waived by West China Tianfu Hospital, Sichuan University. Written informed consent was obtained from the patient for the publication of relevant clinical data.
3. Perioperative Management
3.1. Key Differential Diagnosis for Respiratory Abnormality
This patient had immobility, prolonged bed rest, and trauma related hypercoagulable state, all of which indicate high PE risk. He presented with severe acute hypoxemia (room air SpO2 75%) upon entering the operating room.
Differential diagnosis pathway:
1) Past medical history: long term asthma and chronic bronchitis suggesting chronic airflow limitation.
2) Clinical signs: conscious, no severe chest pain or hemodynamic instability; wheezing on lung auscultation indicating airway obstruction rather than PE.
3) D dimer: elevated but non specific in trauma patients, insufficient for PE diagnosis.
4) Pulmonary imaging and echocardiography: chest CT and bedside ultrasound excluded acute PE, pneumothorax, and large effusion.
5) Arterial blood gas: compensated respiratory acidosis consistent with chronic obstructive pulmonary disease.
Final diagnosis: hypoxemia caused by acute exacerbation of uncontrolled COPD/asthma, not pulmonary embolism. Intraoperative acute saddle PE is a lethal emergency during orthopedic fracture surgery
| [11] | Ayad, M., Ikram, J., Husnain, A. R., Anis, H., Tandon, S., Padubidri, A., Ayad, S. Acute Intraoperative Saddle Pulmonary Embolus in a Trauma Patient Undergoing Repair of Tibial Fracture: A Case Report. Clin Case Rep. 2025, 13(11), e71422. https://doi.org/10.1002/ccr3.71422 |
[11]
. The 2019 ESC guidelines provide unified standards for the diagnosis and management of acute PE, which guides clinical practice worldwide
| [12] | Konstantinides, S. V., Meyer, G., Becattini, C., Bueno, H., Geersing, G. J., Harjola, V. P., Huisman, M. V., Humbert, M., Jennings, C. S., Jiménez, D., Kucher, N., Lang, I. M., Lankeit, M., Lorusso, R., Mazzolai, L., Meneveau, N., Ní Áinle, F., Prandoni, P., Pruszczyk, P., Righini, M., Torbicki, A., Van Belle, E., Zamorano, J. L. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J. 2020, 41(4), 543-603.
https://doi.org/10.1093/eurheartj/ehz405 |
[12]
.
3.2. Preoperative Assessment
1) Room air SpO2: 75% (severe hypoxemia).
2) Lung auscultation: scattered wheezes in the right upper lobe.
3) Arterial blood gas: pH 7.422, PaCO2 49.6 mmHg, PaO2 93.0 mmHg, HCO₃⁻ 31.6 mmol/L.
4) Chest CT: bilateral chronic pulmonary inflammation without PE, pneumothorax or large pleural effusion.
5) Respiratory history: confirmed long standing asthma and chronic bronchitis.
Integrated evaluation rapidly identified undiagnosed COPD/asthma with acute bronchospasm. Retrospective studies have confirmed that comprehensive anesthetic management can reduce postoperative respiratory failure in COPD patients
| [13] | Hou, R. X., Miao, F. F., Jin, D., Duan, Q. F., Yin, C., Feng, Q. P., Wang, T. L. General Anesthesia for Patients With Chronic Obstructive Pulmonary Disease and Postoperative Respiratory Failure: A Retrospective Analysis of 120 Patients. Front Physiol. 2022, 13, 842784.
https://doi.org/10.3389/fphys.2022.842784 |
[13]
.
3.3. Pre Intubation Prophylaxis for Airway Spasm
To prevent life threatening bronchospasm during induction and intubation:
1) Inhaled salbutamol (β
2 agonist) for rapid bronchodilation. Albuterol inhalation can effectively relieve hypoxia and bronchospasm in COPD patients under general anesthesia
| [14] | Maddah, S. A., Barzegari, A. The Effect of Albuterol Spray on Hypoxia and Bronchospasm in Patients with Chronic Obstructive Pulmonary Disease (COPD) under General Anesthesia: A double-blind Randomized Clinical Trial. Ethiopian Journal of Health Sciences. 2023, 33(3), 491-498.
https://doi.org/10.4314/ejhs.v33i3.12 |
[14]
.
2) Intravenous methylprednisolone to reduce airway inflammation.
3) Intravenous aminophylline to improve airway function.
4) Airway topical anesthesia with lidocaine to reduce stimulation.
5) Adequate preoxygenation before anesthetic induction.
6) Small dose epinephrine prepared as rescue medication for severe acute asthma or bronchospasm.
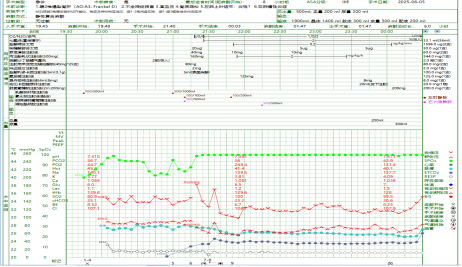
3.4. Intraoperative Anesthetic Management for COPD (Figure 1, Figure 2) Anesthesia regimen: combined intravenous–inhalation anesthesia (propofol, remifentanil, sevoflurane) using short acting agents to minimize residual respiratory depression. Airway control: 7.5# reinforced endotracheal tube with gentle intubation to avoid triggering bronchospasm. Lung-protective ventilation: pressure-controlled ventilation (PCV), VT 6–8 mL/kg, PEEP 5 cmH
2O, I:E 1:3–1:4 to prolong expiration and reduce auto PEEP. For severe COPD patients undergoing orthopedic surgery, noninvasive ventilation assisted by spinal anesthesia is also an effective management mode
| [15] | Lee, M., So, J. Y., Woo, Y. H., Jung, J. W., Chung, Y. H., Koo, B. S. Intraoperative use of noninvasive ventilation during spinal anaesthesia in patients with severe chronic obstructive pulmonary disease undergoing orthopaedic surgery: A case report. J Int Med Res. 2022, 50(5), 3000605221103968.
https://doi.org/10.1177/03000605221103968 |
[15]
. Permissive hypercapnia: maintain PaCO
2 near baseline and pH ≥7.20 to avoid barotrauma and dynamic hyperinflation. Monitoring: invasive arterial pressure, serial blood gas, ETCO
2, SpO
2, and airway pressure; continuous bronchodilator and anti-inflammatory support as needed. Fluid and temperature: restrictive fluid strategy, active warming to prevent hypothermia-induced bronchoconstriction. In addition, general anesthesia combined with peripheral nerve block can also reduce respiratory complications in orthopedic patients
| [16] | Tu, J. H., Peng, P., Xiong, Z. D. General anesthesia with spontaneous breathing and laryngeal mask airway intubation combined with peripheral nerve block in orthopaedic surgery: a retrospective study. Front Med (Lausanne). 2025, 12, 1584437. https://doi.org/10.3389/fmed.2025.1584437 |
[16]
.
Figure 1. Anesthesia record showing key intraoperative monitoring data.
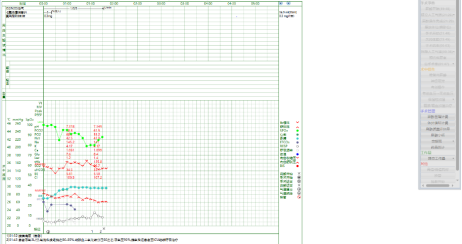
Figure 2. Anesthesia record detailing postoperative respiratory management and recovery parameters.
3.5. Peri-extubation Assessment and Postoperative Respiratory Care
3.5.1. Peri-extubation Evaluation
Extubation prerequisites: full reversal of muscle relaxation (sugammadex), clear consciousness, adequate spontaneous breathing, stable hemodynamics, and acceptable blood gas.
Pre extubation management: gradually reduce FiO2, maintain SpO2 88%–92%, confirm no active bronchospasm.
Goal: avoid reintubation by ensuring safe emergence without CO2 retention or respiratory failure.
3.5.2. Post-extubation Monitoring & Support
Immediate post-extubation: continuous ECG, SpO2, respiratory rate, and ETCO2 monitoring; observe for dyspnea, wheezing, or hypercapnia.
Respiratory support: nasal cannula low flow oxygen; targeted therapy for bronchospasm and CO2 retention.
ICU care: monitor PaCO2 ~60 mmHg (permissive hypercapnia), SpO2 80–85%, avoid excessive oxygenation.
Ward management: low flow oxygen, respiratory consultation, chest physiotherapy, deep breathing exercises, and early mobilization to prevent atelectasis and respiratory failure.
Outcome: stable respiratory recovery, no reintubation, discharged on postoperative day 5.
4. Discussion
4.1. Core Clinical Reasoning
This case demonstrates the core clinical principle: orthopedic trauma patients with prolonged bed rest are at high risk of PE. When respiratory abnormalities occur, differential diagnosis must combine past medical history, signs, D dimer, and pulmonary imaging
| [4] | Bayable, S. D., Melesse, D. Y., Lema, G. F., Ahmed, S. A. Perioperative management of patients with asthma during elective surgery: A systematic review. Annals of Medicine and Surgery. 2021, 70, 102874.
https://doi.org/10.1016/j.amsu.2021.102874 |
| [5] | Celli, B. R., Fabbri, L. M., Aaron, S. D., Agusti, A., Brook, R. D., Criner, G. J., Han, M. K., Martinez, F. J., Roche, C. M., Wedzicha, J. A. Differential diagnosis of suspected chronic obstructive pulmonary disease exacerbations in the acute care setting: Best practice. American Journal of Respiratory and Critical Care Medicine. 2023, 207(9), 1134-1144.
https://doi.org/10.1164/rccm.202206-1210CI |
[4, 5]
.
1) Past medical history is critical for identifying underlying chronic airway disease.
2) Wheezing on auscultation strongly supports obstructive lung disease rather than PE.
3) Elevated D dimer in trauma is non specific; imaging is required to confirm or exclude PE.
4) Integrated assessment avoids misdiagnosis and inappropriate management.
4.2. Key Takeaways for COPD Anesthesia
1) Intraoperative lung-protective ventilation with prolonged expiration and permissive hypercapnia reduces COPD related complications
| [6] | Tillie-Leblond, I., Marquette, C. H., Perez, T., Scherpereel, A., Dehoux, M., Cotte, E., Leroy, S., Weitzenblum, E., Chaouat, A. Pulmonary embolism in patients with unexplained exacerbation of chronic obstructive pulmonary disease: prevalence and risk factors. Annals of Internal Medicine. 2006, 144(6), 390-396. https://doi.org/10.7326/0003-4819-144-6-390 |
[6]
.
2) Strict peri-extubation assessment prevents post-extubation respiratory distress and reintubation.
3) Postoperative monitoring of CO
2 retention, respiratory mechanics, and early rehabilitation are essential to avoid respiratory failure
| [7] | Borowski, B., Haratym, M., Piech, P., Jarecki, J., Staśkiewicz, G. D-dimers or more? Assessing the role of laboratory factors in predicting and confirming pulmonary embolism in high-risk orthopedic patients. Pract Lab Med. 2025, 44, e00452.
https://doi.org/10.1016/j.plabm.2025.e00452 |
[7]
.
5. Conclusions
In immobilized orthopedic patients with acute respiratory dysfunction:
1) Differential diagnosis must integrate past medical history, signs, D dimer, and pulmonary imaging to distinguish PE from chronic airway disease.
2) Preoperative assessment (SpO2, auscultation, blood gas, chest CT, history) rapidly identifies occult COPD/asthma.
3) Pre intubation anti bronchospasm prophylaxis is critical for emergency anesthesia safety.
4) Intraoperative lung-protective ventilation and standardized peri-extubation assessment reduce bronchospasm, CO2 retention, and reintubation risk.
5) Postoperative respiratory monitoring and early mobilization prevent respiratory failure and ensure smooth recovery.
This comprehensive pathway significantly reduces perioperative risks and improves clinical outcomes.
Abbreviations
ASA | American Society of Anesthesiologists |
BIS | Bispectral Index |
COPD | Chronic Obstructive Pulmonary Disease |
CT | Computed Tomography |
pH | Potential of Hydrogen |
ETCO2 | End tidal Carbon Dioxide |
ICU | Intensive Care Unit |
I:E | Inspiratory:Expiratory ratio |
MRI | Magnetic Resonance Imaging |
NIV | Noninvasive Ventilation |
PaCO2 | Partial Pressure of Arterial Carbon Dioxide |
PaO2 | Partial Pressure of Arterial Oxygen |
PCV | Pressure Controlled Ventilation |
PE | Pulmonary Embolism |
PEEP | Positive End Expiratory Pressure |
SpO2 | Peripheral Capillary Oxygen Saturation |
VT | Tidal Volume |
Acknowledgments
We thank the anesthesiology team of West China Tianfu Hospital for clinical support and data collection. We are grateful to the patient and his family for informed consent and cooperation.
Author Contributions
Yong Liu: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing
Mengdie Liang: Data curation, Formal Analysis
Feng Long: Resources, Supervision, Validation
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Wills, J. H., Gaski, G. E. Update on venous thromboembolism in orthopaedic trauma surgery. Journal of the American Academy of Orthopaedic Surgeons. 2024, 32(19), e961-e969.
https://doi.org/10.5435/JAAOS-D-23-06863
|
| [2] |
Woods, B. D., Sladen, R. N. Perioperative considerations for the patient with asthma and bronchospasm. British Journal of Anaesthesia. 2009, 103(Suppl 1), i57-i65.
https://doi.org/10.1093/bja/aep301
|
| [3] |
Lesser, B. A., Leeper, K. V., Jr., Stein, P. D., Saltzman, H. A., Chen, J., Thompson, B. T., Hales, C. A. The diagnosis of acute pulmonary embolism in patients with chronic obstructive pulmonary disease. Chest. 1992, 102(1), 17-22.
https://doi.org/10.1378/chest.102.1.17
|
| [4] |
Bayable, S. D., Melesse, D. Y., Lema, G. F., Ahmed, S. A. Perioperative management of patients with asthma during elective surgery: A systematic review. Annals of Medicine and Surgery. 2021, 70, 102874.
https://doi.org/10.1016/j.amsu.2021.102874
|
| [5] |
Celli, B. R., Fabbri, L. M., Aaron, S. D., Agusti, A., Brook, R. D., Criner, G. J., Han, M. K., Martinez, F. J., Roche, C. M., Wedzicha, J. A. Differential diagnosis of suspected chronic obstructive pulmonary disease exacerbations in the acute care setting: Best practice. American Journal of Respiratory and Critical Care Medicine. 2023, 207(9), 1134-1144.
https://doi.org/10.1164/rccm.202206-1210CI
|
| [6] |
Tillie-Leblond, I., Marquette, C. H., Perez, T., Scherpereel, A., Dehoux, M., Cotte, E., Leroy, S., Weitzenblum, E., Chaouat, A. Pulmonary embolism in patients with unexplained exacerbation of chronic obstructive pulmonary disease: prevalence and risk factors. Annals of Internal Medicine. 2006, 144(6), 390-396.
https://doi.org/10.7326/0003-4819-144-6-390
|
| [7] |
Borowski, B., Haratym, M., Piech, P., Jarecki, J., Staśkiewicz, G. D-dimers or more? Assessing the role of laboratory factors in predicting and confirming pulmonary embolism in high-risk orthopedic patients. Pract Lab Med. 2025, 44, e00452.
https://doi.org/10.1016/j.plabm.2025.e00452
|
| [8] |
Yaghoobpoor, S., Fathi, M., Taher, H. J., Farhood, A. J., Bahrami, A., Eshraghi, R., Hajibeygi, R., Tutunchian, Z., Myers, L., Ahmadi, R., Gholamrezanezhad, A. Computed tomography pulmonary angiography (CTPA) for the detection of pulmonary embolism (PE) among trauma patients: a systematic review and meta-analysis. Emerg Radiol. 2024, 31(4), 567-580.
https://doi.org/10.1007/s10140-024-02249-7
|
| [9] |
Thivaharan, Y., Dayapala, A., Thanushan, M. A case of early pulmonary embolism following blunt trauma to chest and a long bone fracture. Egyptian Journal of Forensic Sciences. 2023, 13(1), 9.
https://doi.org/10.1186/s41935-023-00327-4
|
| [10] |
Di, L., Chen, Z., Wang, X. Y., Zhang, J., Zhang, J., Ding, J. Q. Early diagnosis of occult pulmonary embolism secondary to lower limb fractures: summary of 18 cases. Front Med (Lausanne). 2024, 11, 1355030.
https://doi.org/10.3389/fmed.2024.1355030
|
| [11] |
Ayad, M., Ikram, J., Husnain, A. R., Anis, H., Tandon, S., Padubidri, A., Ayad, S. Acute Intraoperative Saddle Pulmonary Embolus in a Trauma Patient Undergoing Repair of Tibial Fracture: A Case Report. Clin Case Rep. 2025, 13(11), e71422.
https://doi.org/10.1002/ccr3.71422
|
| [12] |
Konstantinides, S. V., Meyer, G., Becattini, C., Bueno, H., Geersing, G. J., Harjola, V. P., Huisman, M. V., Humbert, M., Jennings, C. S., Jiménez, D., Kucher, N., Lang, I. M., Lankeit, M., Lorusso, R., Mazzolai, L., Meneveau, N., Ní Áinle, F., Prandoni, P., Pruszczyk, P., Righini, M., Torbicki, A., Van Belle, E., Zamorano, J. L. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J. 2020, 41(4), 543-603.
https://doi.org/10.1093/eurheartj/ehz405
|
| [13] |
Hou, R. X., Miao, F. F., Jin, D., Duan, Q. F., Yin, C., Feng, Q. P., Wang, T. L. General Anesthesia for Patients With Chronic Obstructive Pulmonary Disease and Postoperative Respiratory Failure: A Retrospective Analysis of 120 Patients. Front Physiol. 2022, 13, 842784.
https://doi.org/10.3389/fphys.2022.842784
|
| [14] |
Maddah, S. A., Barzegari, A. The Effect of Albuterol Spray on Hypoxia and Bronchospasm in Patients with Chronic Obstructive Pulmonary Disease (COPD) under General Anesthesia: A double-blind Randomized Clinical Trial. Ethiopian Journal of Health Sciences. 2023, 33(3), 491-498.
https://doi.org/10.4314/ejhs.v33i3.12
|
| [15] |
Lee, M., So, J. Y., Woo, Y. H., Jung, J. W., Chung, Y. H., Koo, B. S. Intraoperative use of noninvasive ventilation during spinal anaesthesia in patients with severe chronic obstructive pulmonary disease undergoing orthopaedic surgery: A case report. J Int Med Res. 2022, 50(5), 3000605221103968.
https://doi.org/10.1177/03000605221103968
|
| [16] |
Tu, J. H., Peng, P., Xiong, Z. D. General anesthesia with spontaneous breathing and laryngeal mask airway intubation combined with peripheral nerve block in orthopaedic surgery: a retrospective study. Front Med (Lausanne). 2025, 12, 1584437.
https://doi.org/10.3389/fmed.2025.1584437
|
Cite This Article
-
APA Style
Liu, Y., Liang, M., Long, F. (2026). Anesthetic Management for Emergency Orthopedic Surgery in a Patient with COPD and Asthma: A Case Report. International Journal of Anesthesia and Clinical Medicine, 14(1), 110-114. https://doi.org/10.11648/j.ijacm.20261401.27
 Copy
|
Copy
|
 Download
Download
ACS Style
Liu, Y.; Liang, M.; Long, F. Anesthetic Management for Emergency Orthopedic Surgery in a Patient with COPD and Asthma: A Case Report. Int. J. Anesth. Clin. Med. 2026, 14(1), 110-114. doi: 10.11648/j.ijacm.20261401.27
Copy
|
Download
AMA Style
Liu Y, Liang M, Long F. Anesthetic Management for Emergency Orthopedic Surgery in a Patient with COPD and Asthma: A Case Report. Int J Anesth Clin Med. 2026;14(1):110-114. doi: 10.11648/j.ijacm.20261401.27
Copy
|
Download
-
@article{10.11648/j.ijacm.20261401.27,
author = {Yong Liu and Mengdie Liang and Feng Long},
title = {Anesthetic Management for Emergency Orthopedic Surgery in a Patient with COPD and Asthma: A Case Report},
journal = {International Journal of Anesthesia and Clinical Medicine},
volume = {14},
number = {1},
pages = {110-114},
doi = {10.11648/j.ijacm.20261401.27},
url = {https://doi.org/10.11648/j.ijacm.20261401.27},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijacm.20261401.27},
abstract = {Orthopedic trauma patients with limited mobility and prolonged bed rest are at high risk of venous thromboembolism and pulmonary embolism (PE). When acute hypoxemia and respiratory dysfunction occur in such patients, it is clinically challenging to distinguish PE from acute exacerbation of underlying chronic obstructive pulmonary disease (COPD) or asthma, which directly affects perioperative safety. This study aimed to summarize the diagnostic thinking and standardized anesthetic management strategies for this type of high-risk emergency patient. We reported a 68-year-old male patient diagnosed with L2 burst fracture, who presented with severe hypoxemia (room-air SpO2 75%) before emergency surgery. Combined with the patient’s medical history, lung auscultation, arterial blood gas analysis and chest computed tomography (CT) findings, we rapidly confirmed that hypoxemia was caused by acute airway obstruction rather than PE. Pre-intubation interventions including bronchodilators, corticosteroids and airway surface anesthesia were applied to prevent intraoperative bronchospasm. Intraoperative lung-protective ventilation was implemented, and stepwise respiratory support was adopted after extubation. The patient had an uneventful perioperative course and was discharged on the 5th postoperative day. In conclusion, for immobilized orthopedic trauma patients complicated with chronic airway diseases and acute respiratory abnormalities, comprehensive differential diagnosis combining clinical manifestations and auxiliary examinations is the premise of safe treatment. Targeted pre-operative prevention, standardized intraoperative ventilation and graded postoperative respiratory care can effectively reduce perioperative respiratory complications.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Anesthetic Management for Emergency Orthopedic Surgery in a Patient with COPD and Asthma: A Case Report
AU - Yong Liu
AU - Mengdie Liang
AU - Feng Long
Y1 - 2026/06/26
PY - 2026
N1 - https://doi.org/10.11648/j.ijacm.20261401.27
DO - 10.11648/j.ijacm.20261401.27
T2 - International Journal of Anesthesia and Clinical Medicine
JF - International Journal of Anesthesia and Clinical Medicine
JO - International Journal of Anesthesia and Clinical Medicine
SP - 110
EP - 114
PB - Science Publishing Group
SN - 2997-2698
UR - https://doi.org/10.11648/j.ijacm.20261401.27
AB - Orthopedic trauma patients with limited mobility and prolonged bed rest are at high risk of venous thromboembolism and pulmonary embolism (PE). When acute hypoxemia and respiratory dysfunction occur in such patients, it is clinically challenging to distinguish PE from acute exacerbation of underlying chronic obstructive pulmonary disease (COPD) or asthma, which directly affects perioperative safety. This study aimed to summarize the diagnostic thinking and standardized anesthetic management strategies for this type of high-risk emergency patient. We reported a 68-year-old male patient diagnosed with L2 burst fracture, who presented with severe hypoxemia (room-air SpO2 75%) before emergency surgery. Combined with the patient’s medical history, lung auscultation, arterial blood gas analysis and chest computed tomography (CT) findings, we rapidly confirmed that hypoxemia was caused by acute airway obstruction rather than PE. Pre-intubation interventions including bronchodilators, corticosteroids and airway surface anesthesia were applied to prevent intraoperative bronchospasm. Intraoperative lung-protective ventilation was implemented, and stepwise respiratory support was adopted after extubation. The patient had an uneventful perioperative course and was discharged on the 5th postoperative day. In conclusion, for immobilized orthopedic trauma patients complicated with chronic airway diseases and acute respiratory abnormalities, comprehensive differential diagnosis combining clinical manifestations and auxiliary examinations is the premise of safe treatment. Targeted pre-operative prevention, standardized intraoperative ventilation and graded postoperative respiratory care can effectively reduce perioperative respiratory complications.
VL - 14
IS - 1
ER -
Copy
|
Download