Background: Ameloblastic fibrosarcoma (AFS) is a rare malignant odontogenic tumor characterized by benign epithelial components and a malignant mesenchymal stroma. Accurate diagnosis is challenging, especially when initial biopsy samples are limited. Case Presentation: A 35-year-old male presented with a progressively enlarging swelling on the left side of his face. Clinical examination revealed a firm, non-tender mass in the left mandibular region, resulting in mild facial asymmetry. Intraoral evaluation showed buccal cortical expansion in the posterior mandible, accompanied by slight mobility of the adjacent teeth. Panoramic radiograph and cone beam computed tomography (CBCT) revealed an ill-defined, multilocular radiolucent lesion involving the left mandibular body and ramus, with cortical bone perforation and mild soft tissue extension. An incisional biopsy initially diagnosed ameloblastic fibroma (AF). The patient underwent segmental mandibulectomy, and final histopathological evaluation revealed low-grade ameloblastic fibrosarcoma. Reconstruction was performed using a reconstruction plate and autogenous iliac bone graft. The postoperative course was uneventful, with no recurrence observed during a 6-month follow-up. Conclusions: This case underscores the diagnostic challenges of AFS and highlights the importance of comprehensive histopathological evaluation. Early detection, accurate diagnosis, and complete surgical excision with clear margins are critical for best outcomes.
| Published in | International Journal of Clinical Oral and Maxillofacial Surgery (Volume 11, Issue 2) |
| DOI | 10.11648/j.ijcoms.20251102.11 |
| Page(s) | 58-62 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Ameloblastic Fibrosarcoma, Mandible, Odontogenic Tumor, Iliac Bone Graft, Case Report
AF | Ameloblastic Fibroma |
AFS | Ameloblastic Fibrosarcoma |
CBCT | Cone Beam Computed Tomography |
| [1] | Heath C. Lectures on certain diseases of the jaws. Br Med J. 1887; 2(1383): 5-13. |
| [2] | Chrcanovic BR, Brennan PA, Rahimi S, Gomez RS. Ameloblastic fibroma and ameloblastic fibrosarcoma: a systematic review. Journal of Oral Pathology & Medicine. 2018 Apr; 47(4): 315-25. |
| [3] | Munisekhar M, Shylaja S, Kumar RV, Rao KA, Patil SR, Alam MK. Ameloblastic fibrosarcoma - A rarity? JPRAS Open. 2019 Jun 21; 21: 56-62. |
| [4] | WHO Classification of Head and Neck Tumours. 5th ed. Lyon: International Agency for Research on Cancer (IARC); 2022. p. 317-319. |
| [5] | Li LT, Jiang G, Chen Q and Zheng JN: Ki67 is a promising molecular target in the diagnosis of cancer (Review). Mol Med Rep 11: 1566-1572, 2015. |
| [6] | Mohsenifar Z, Behrad S, Abbas FM. Epithelial Dysplasia in Ameloblastic Fibrosarcoma Arising from Recurrent Ameloblastic Fibroma in a 26-Year-Old Iranian Man. Am J Case Rep. 2015 Aug 18; 16: 548-53. |
| [7] |
Gilani SM, Raza A, Al-Khafaji BM. Ameloblastic fibrosarcoma: a rare malignant odontogenic tumor. Eur Ann Otorhinolaryngol Head Neck Dis. 2014 Feb; 131(1): 53-6.
https://doi.org/10.1016/j.anorl.2013.03.001 Epub 2013 Jul 9. |
| [8] | Coletti DP, Ord RA, Liu X. Nonvascularized bone graft reconstruction of the mandible: outcomes and factors influencing success. J Oral Maxillofac Surg. 2009 Feb; 67(2): 400-4. |
| [9] | Carroll C, Gill M, Bowden E, O'Connell JE, Shukla R, Sweet C. Ameloblastic Fibroma of the Mandible Reconstructed with Autogenous Parietal Bone: Report of a Case and Literature Review. Case Rep Dent. 2019 Jun 18; 2019: 5149219. |
APA Style
Motlagh, M. F., Mostafazadhe, S., Motlagh, F. F. (2025). Low-Grade Ameloblastic Fibrosarcoma of the Mandible: A Case Report with Initial Misdiagnosis. International Journal of Clinical Oral and Maxillofacial Surgery, 11(2), 58-62. https://doi.org/10.11648/j.ijcoms.20251102.11
ACS Style
Motlagh, M. F.; Mostafazadhe, S.; Motlagh, F. F. Low-Grade Ameloblastic Fibrosarcoma of the Mandible: A Case Report with Initial Misdiagnosis. Int. J. Clin. Oral Maxillofac. Surg. 2025, 11(2), 58-62. doi: 10.11648/j.ijcoms.20251102.11
@article{10.11648/j.ijcoms.20251102.11,
author = {Masoud Fallahi Motlagh and Samira Mostafazadhe and Farbod Fallahi Motlagh},
title = {Low-Grade Ameloblastic Fibrosarcoma of the Mandible: A Case Report with Initial Misdiagnosis
},
journal = {International Journal of Clinical Oral and Maxillofacial Surgery},
volume = {11},
number = {2},
pages = {58-62},
doi = {10.11648/j.ijcoms.20251102.11},
url = {https://doi.org/10.11648/j.ijcoms.20251102.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcoms.20251102.11},
abstract = {Background: Ameloblastic fibrosarcoma (AFS) is a rare malignant odontogenic tumor characterized by benign epithelial components and a malignant mesenchymal stroma. Accurate diagnosis is challenging, especially when initial biopsy samples are limited. Case Presentation: A 35-year-old male presented with a progressively enlarging swelling on the left side of his face. Clinical examination revealed a firm, non-tender mass in the left mandibular region, resulting in mild facial asymmetry. Intraoral evaluation showed buccal cortical expansion in the posterior mandible, accompanied by slight mobility of the adjacent teeth. Panoramic radiograph and cone beam computed tomography (CBCT) revealed an ill-defined, multilocular radiolucent lesion involving the left mandibular body and ramus, with cortical bone perforation and mild soft tissue extension. An incisional biopsy initially diagnosed ameloblastic fibroma (AF). The patient underwent segmental mandibulectomy, and final histopathological evaluation revealed low-grade ameloblastic fibrosarcoma. Reconstruction was performed using a reconstruction plate and autogenous iliac bone graft. The postoperative course was uneventful, with no recurrence observed during a 6-month follow-up. Conclusions: This case underscores the diagnostic challenges of AFS and highlights the importance of comprehensive histopathological evaluation. Early detection, accurate diagnosis, and complete surgical excision with clear margins are critical for best outcomes.},
year = {2025}
}
TY - JOUR T1 - Low-Grade Ameloblastic Fibrosarcoma of the Mandible: A Case Report with Initial Misdiagnosis AU - Masoud Fallahi Motlagh AU - Samira Mostafazadhe AU - Farbod Fallahi Motlagh Y1 - 2025/07/24 PY - 2025 N1 - https://doi.org/10.11648/j.ijcoms.20251102.11 DO - 10.11648/j.ijcoms.20251102.11 T2 - International Journal of Clinical Oral and Maxillofacial Surgery JF - International Journal of Clinical Oral and Maxillofacial Surgery JO - International Journal of Clinical Oral and Maxillofacial Surgery SP - 58 EP - 62 PB - Science Publishing Group SN - 2472-1344 UR - https://doi.org/10.11648/j.ijcoms.20251102.11 AB - Background: Ameloblastic fibrosarcoma (AFS) is a rare malignant odontogenic tumor characterized by benign epithelial components and a malignant mesenchymal stroma. Accurate diagnosis is challenging, especially when initial biopsy samples are limited. Case Presentation: A 35-year-old male presented with a progressively enlarging swelling on the left side of his face. Clinical examination revealed a firm, non-tender mass in the left mandibular region, resulting in mild facial asymmetry. Intraoral evaluation showed buccal cortical expansion in the posterior mandible, accompanied by slight mobility of the adjacent teeth. Panoramic radiograph and cone beam computed tomography (CBCT) revealed an ill-defined, multilocular radiolucent lesion involving the left mandibular body and ramus, with cortical bone perforation and mild soft tissue extension. An incisional biopsy initially diagnosed ameloblastic fibroma (AF). The patient underwent segmental mandibulectomy, and final histopathological evaluation revealed low-grade ameloblastic fibrosarcoma. Reconstruction was performed using a reconstruction plate and autogenous iliac bone graft. The postoperative course was uneventful, with no recurrence observed during a 6-month follow-up. Conclusions: This case underscores the diagnostic challenges of AFS and highlights the importance of comprehensive histopathological evaluation. Early detection, accurate diagnosis, and complete surgical excision with clear margins are critical for best outcomes. VL - 11 IS - 2 ER -
Department of Oral & Maxillofacial, Private Practitioner and Consultant in Maxillofacial Surgery, Azarbayjan Hospital, Urmia, Iran
Department of Oral and Maxillofacial Pathology, Urmia University of Medical Sciences, Urmia, Iran
Dental School of Islamic Azad, University of Tehran, Tehran, Iran

Figure 1. The image shows a firm, non-tender swelling on the left side of the mandible.
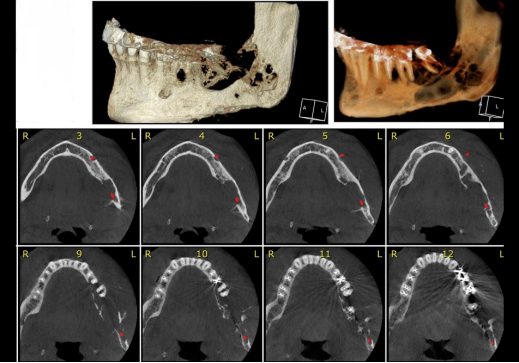
Figure 2. CBCT images showed cortical bone thinning and areas of perforation.
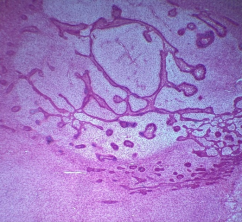
Figure 3. H&E sections (10×10) show epithelial islands and strands within a loose, cellular fibroblastic stroma resembling primitive dental papilla. Peripheral epithelial cells are low columnar. Hyaline-like material is present adjacent to the epithelial structures.

Figure 4. The postoperative panoramic view demonstrates the tumor resection site and reconstruction with a reconstruction plate.
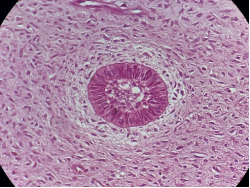
Figure 5. H&E stain (40×10 magnification) shows a mesenchymal area composed of spindle and stellate cells exhibiting mild to moderate nuclear pleomorphism, cytologic atypia, vesicular hyperchromatic nuclei, and numerous mitotic figures.
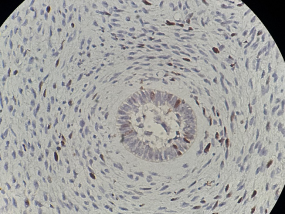
Figure 6. Immunohistochemical staining with Ki-67 (40×10 magnification) shows that approximately 15% of mesenchymal cells express the marker. Most epithelial cells exhibited only a small number of Ki-67-positive cells.
Information

