Abstract
Introduction: Pulmonary embolism (PE) is a major cause of cardiovascular morbidity and mortality. In Africa, limited access to computed tomography pulmonary angiography (CTPA) enhances the clinical value of the electrocardiogram (ECG), a rapid and widely available tool, for early diagnostic orientation and prognostic assessment. Objectives: To describe ECG abnormalities observed in patients with acute pulmonary embolism and to analyze their association with in-hospital mortality and paraclinical markers of severity. Methods: We conducted a retrospective, descriptive, and analytical study including 103 patients hospitalized for confirmed pulmonary embolism in the cardiology department of the National Hospital Center Dalal Jamm, Dakar, Senegal, between January 1, 2021 and December 31, 2023. Clinical characteristics, risk factors, biological parameters, transthoracic echocardiographic findings, and CTPA results were collected. The associations between isolated or cumulative ECG abnormalities and in-hospital mortality were analyzed. Results: The mean age was 53 years, with a female predominance (male-to-female ratio: 0.84). The main risk factors were obesity (36.2%), age >70 years (31.9%), prolonged immobilization (24.6%), underlying heart disease (13%), and gynecological factors (14.5%). The most common symptoms were dyspnea (83.5%), chest pain (67%), and cough (49.5%). The most frequent ECG abnormalities were sinus tachycardia (62.1%), subepicardial ischemia (47.6%), the S1Q3T3 pattern (38.8%), and right-sided conduction disturbances, including right bundle branch block (20.4%). Transthoracic echocardiography revealed right heart chamber dilation (50%), pulmonary hypertension (38.8%), and intracardiac thrombus (6.3%). CTPA showed bilateral PE in 29.1% of cases, right-sided PE in 15.5%, and left-sided PE in 9.7%. All patients received anticoagulation therapy. In-hospital mortality risk was significantly higher in patients presenting with at least two cumulative ECG abnormalities and was strongly associated with right heart dilation and pulmonary hypertension. Conclusion: Pulmonary embolism represents a significant clinical burden in Senegal. Although nonspecific, the ECG provides valuable information for early suspicion and prognostic stratification, particularly in emergency settings with limited resources. The presence of multiple ECG abnormalities identifies patients at high risk of early mortality. Early recognition of these findings, combined with risk factor assessment and evaluation of right ventricular involvement, may facilitate timely management and improve patient outcomes.
Keywords
Pulmonary Embolism, Electrocardiogram, Senegal
1. Introduction
Pulmonary embolism (PE) is a major cardiovascular emergency and, together with deep vein thrombosis, represents one of the main clinical manifestations of venous thromboembolic disease. It remains a significant cause of morbidity and mortality worldwide and ranks among the leading preventable causes of cardiovascular death
| [1] | Goldhaber SZ, Bounameaux H. Pulmonary embolism and deep vein thrombosis. Lancet. 2012; 379(9828): 1835-1846. |
| [2] | Wendelboe AM, Raskob GE. Global burden of thrombosis: epidemiologic aspects. Circ Res. 2016; 118(9): 1340-1347. |
[1, 2]
. Acute PE can rapidly become life-threatening, particularly when associated with right ventricular failure or hemodynamic instability, making early diagnosis and prompt therapeutic management crucial
| [3] | Konstantinides SV, Meyer G, Becattini C, et al. 2019 ESC guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J. 2020; 41(4): 543-603. |
[3]
.
However, the diagnosis of PE remains a clinical challenge due to the nonspecific nature of its presentation. Computed tomography pulmonary angiography (CTPA) is currently considered the reference diagnostic modality because of its high sensitivity and specificity
| [4] | Van der Hulle T, Cheung WY, Kooij S, et al. Simplified diagnostic management of suspected pulmonary embolism (the YEARS study): a prospective, multicentre, cohort study. Lancet. 2017; 390(10091): 289-297. |
[4]
. Nevertheless, access to CTPA remains limited in many low-resource settings, particularly in sub-Saharan Africa, where technical, economic, and logistical constraints restrict its widespread use
| [5] | Kakou Guikahue MK, Soro K, Anzouan-Kacou E, et al. Challenges in the management of pulmonary embolism in sub-Saharan Africa: a perspective. Cardiovasc Diagn Ther. 2020; 10(5): 1514-1521. |
[5]
. In this context, simple, rapidly available, and low-cost diagnostic tools retain particular importance.
The electrocardiogram (ECG), although nonspecific, remains a first-line investigation widely used in patients with suspected PE. It not only helps exclude certain life-threatening differential diagnoses but also reveals indirect signs of acute right ventricular overload
| [6] | Kukla P, McIntyre WF, Fijorek K, et al. Electrocardiographic abnormalities in patients with acute pulmonary embolism. Ann Noninvasive Electrocardiol. 2014; 19(3): 234-241. |
[6]
. ECG abnormalities such as sinus tachycardia, the S₁Q₃T₃ pattern, right bundle branch block, and anterior repolarization abnormalities are classically described in acute PE. However, their frequency and diagnostic and prognostic value vary considerably across studies, and approximately 15–20% of patients may present with a completely normal ECG
| [7] | Stein PD, Dalen JE, McIntyre KM, Sasahara AA, Wenger NK, Willis PW 3rd. The electrocardiogram in acute pulmonary embolism. Prog Cardiovasc Dis. 1975; 17(4): 247-257. |
| [8] | Daniel KR, Courtney DM, Kline JA. Assessment of cardiac stress from massive pulmonary embolism with 12-lead ECG. Chest. 2001; 120(2): 474-481. |
[7, 8]
.
Beyond its limited diagnostic role, several studies suggest that certain ECG abnormalities may be associated with PE severity and short-term prognosis, particularly in relation to right ventricular dysfunction and early mortality
| [9] | Kucher N, Walpoth N, Wustmann K, Noveanu M, Gertsch M. QR in V1—an ECG sign associated with right ventricular strain and adverse clinical outcome in pulmonary embolism. Eur Heart J. 2003; 24(12): 1113-1119. |
| [10] | Geibel A, Zehender M, Kasper W, Olschewski M, Klima C, Konstantinides SV. Prognostic value of the ECG on admission in patients with acute major pulmonary embolism. Eur Respir J. 2005; 25(5): 843-848. |
| [11] | Vanni S, Polidori G, Vergara R, et al. Prognostic value of ECG among patients with acute pulmonary embolism and normal blood pressure. Am J Med. 2009; 122(3): 257-264. |
[9-11]
. However, African data on the electrocardiographic features of PE and their correlation with morbidity and mortality remain scarce, fragmented, and often derived from small case series.
In this context, we conducted the present study at the National Hospital Center Dalal Jamm in Dakar, Senegal, to describe the electrocardiographic abnormalities observed in patients hospitalized for pulmonary embolism and to analyze their association with clinical and paraclinical findings, as well as with in-hospital mortality. This study aims to contribute to a better understanding of the role of ECG in the management of pulmonary embolism in African hospital settings.
2. Methods
Study design and setting
This was an observational, retrospective, descriptive, and analytical study conducted in the cardiology department of the National Hospital Center Dalal Jamm (NHCDJ), a tertiary referral hospital located in Dakar, Senegal.
Study period
The study covered a three-year period, from January 1, 2021 to December 31, 2023.
Study population
All patients hospitalized for acute pulmonary embolism confirmed by computed tomography pulmonary angiography during the study period were eligible for inclusion.
Inclusion criteria
Patients aged 18 years or older with pulmonary embolism confirmed by CTPA, who had a standard 12-lead electrocardiogram performed at admission or within the first 24 hours of hospitalization, and whose medical records were complete and exploitable, were included.
Exclusion criteria
Patients with clinically suspected but unconfirmed pulmonary embolism, those with unavailable or uninterpretable ECG recordings, and those with incomplete medical records that did not allow analysis of the studied parameters were excluded.
Data collection
Data were retrospectively collected from hospital medical records, admission registers, and reports of paraclinical investigations, including electrocardiography, laboratory tests, and imaging studies. A standardized data collection form was used.
The collected variables included sociodemographic data (age, sex, marital status, occupation, and socioeconomic level), clinical data such as risk factors for venous thromboembolic disease, functional symptoms (dyspnea, chest pain, syncope, hemoptysis), physical findings, and hemodynamic parameters at admission. Clinical probability of pulmonary embolism was assessed using the Wells score.
Paraclinical data included systematic analysis of a standard 12-lead ECG, focusing on abnormalities suggestive of right ventricular overload, such as sinus tachycardia, right axis deviation, the S₁Q₃T₃ pattern, complete or incomplete right bundle branch block, right ventricular repolarization abnormalities, and atrial fibrillation. The ECG interpretation was performed by two cardiologists in a blinded manner.
Additional investigations included laboratory tests (D-dimer levels, arterial blood gases, and cardiac biomarkers when available), transthoracic echocardiography to assess right ventricular function and pulmonary artery pressure, and CTPA findings.
Outcome data included the occurrence of in-hospital complications, early mortality risk stratification, and in-hospital outcome, defined as survival or death.
Statistical analysis
Data were entered and analyzed using statistical software (SPSS®). Quantitative variables were expressed as mean ± standard deviation or median, depending on their distribution. Qualitative variables were expressed as frequencies and percentages.
Associations between ECG abnormalities and clinical, paraclinical parameters or in-hospital mortality were analyzed using the Chi-square test or Fisher’s exact test, as appropriate. A p-value < 0.05 was considered statistically significant.
Ethical considerations
The study was conducted in accordance with the principles of the Declaration of Helsinki. Patient anonymity and data confidentiality were ensured. Given the retrospective nature of the study, individual informed consent was not required.
3. Results
General characteristics of the study population
During the period from January 1, 2021 to December 31, 2023, a total of 103 patients hospitalized for acute pulmonary embolism confirmed by computed tomography pulmonary angiography were included in the study.
The mean age of the patients was 53 years, with a range from 19 to 82 years. Patients aged over 70 years were the most represented age group (21.4%). A female predominance was observed, with a male-to-female ratio of 0.84.
The most represented socio-professional category was the working population (48.5%). Most patients were admitted through inter-hospital transfer (51.5%), followed by referrals from other healthcare facilities (47.6%). A middle socioeconomic level was predominant in 51.5% of cases. The mean length of hospital stay was 8.3 days, ranging from 1 to 32 days.
Etiological and clinical features
The main risk factors for venous thromboembolic disease identified were obesity (36.2%), age over 70 years (31.9%), prolonged immobilization (24.6%), gynecological risk factors (14.5%), underlying heart disease (13%), and prolonged sitting position (10.1%). A history of ischemic stroke and cancer was reported in 8.7% of patients each. No etiological factor was identified in 33% of cases.
From a functional standpoint, symptoms were dominated by dyspnea (83.5%), followed by chest pain (67.0%), cough (49.5%), and hemoptysis (17.5%), as shown in
Table 1.
Table 1. Distribution of patients according to functional symptoms.
Symptoms | Number | Percentage (%) |
Dyspnea | 86 | 83.50 |
Chest pain | 69 | 66.99 |
Cough | 51 | 49.51 |
Painful swollen leg | 18 | 17.48 |
Hemoptysis | 18 | 17.48 |
Fever | 12 | 11.65 |
Palpitations | 7 | 6.80 |
Syncope | 6 | 5.83 |
On clinical examination, the most frequent cardiovascular signs were tachycardia on auscultation (76.6%), spontaneous jugular venous distension (39%), and an accentuated second heart sound (27.3%). Regarding pleuropulmonary findings, tachypnea was observed in 78.5% of patients, crackles in 60.8%, and pulmonary consolidation syndrome in 58.2%.
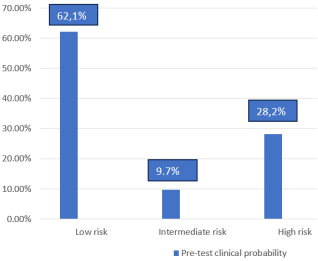
According to the Wells score, the clinical probability of pulmonary embolism was most often low (62.1%), as illustrated in
Figure 1.
Figure 1. Distribution of patients according to the clinical probability of pulmonary embolism based on the Wells score.
Additional paraclinical findings
A complete blood count was performed in all 103 patients. The most frequently observed abnormalities were leukocytosis (47.6%), followed by anemia (38.8%). Regarding inflammatory markers, C-reactive protein was elevated in 91 patients (88.3%), and D-dimer levels were elevated in all patients.
Among the 103 included patients, the electrocardiogram performed at admission revealed sinus tachycardia in 76.6% of cases. This was followed by right ventricular repolarization abnormalities manifested as anterior T-wave inversion in 47.6% of patients, the S₁Q₃T₃ pattern in 38.8%, complete or incomplete right bundle branch block in 20.4%, and right axis deviation in 12.6% of patients (
Table 2).
Table 2. Distribution of patients according to electrocardiographic abnormalities.
Electrocardiographic parameters | Number | Percentage (%) |
Sinus tachycardia | 59 | 76.6 |
Right axis deviation | 13 | 12.6 |
T-wave inversion | 49 | 47.6 |
S₁Q₃T₃ pattern | 40 | 38.8 |
Right bundle branch block | 21 | 20.4 |
Left-ventricular hypertrophy | 17 | 16.5 |
Left atrial enlargement | 14 | 13.6 |
Right atrial enlargement | 10 | 9.7 |
Right-ventricular hypertrophy | 9 | 8.7 |
Atrial arrhythmia | 8 | 7.8 |
Ventricular arrhythmia | 5 | 4.9 |
Transthoracic echocardiography showed right heart chamber dilation in 50% of patients, pulmonary hypertension in 38.8%, intracavitary thrombus in 6.3%, and a visible pulmonary artery thrombus in 1.3% of cases.
Lower limb deep vein thrombosis was detected in 66.7% of patients, with equal involvement of the right and left lower limbs.
Computed tomography pulmonary angiography revealed bilateral pulmonary embolism in 29.1% of cases, isolated right-sided involvement in 15.5%, and isolated left-sided involvement in 9.7% of cases. All patients received anticoagulant therapy.
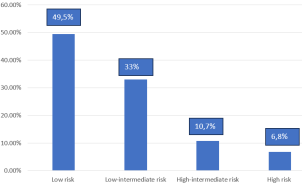
Overall, 49.5% of patients were classified as low-risk for mortality, while 7 patients (6.8%) were classified as high-risk, as illustrated in
Figure 2.
Figure 2. Distribution of patients according to mortality risk.
All patients received anticoagulant therapy. Low-molecular-weight heparin was administered in 88 patients (85.4%), vitamin K antagonists in 63 patients (61.2%), and direct oral anticoagulants in 50 patients (48.5%). Thrombolytic therapy was performed in 18 patients (17.5%).
Clinical outcome
Among the 103 included patients, the mean length of hospital stay was 8.3 days, with a median of 7 days and a standard deviation of 6.1 days. Hospital stays ranged from 1 to 32 days.
Clinical outcome was favorable in 80.6% of patients. An unfavorable outcome was observed in 19.4% of cases, including 17 in-hospital deaths.
Analytical study
Correlation between ECG abnormalities and mortality risk
Analytical analysis showed no statistically significant correlation between isolated electrocardiographic abnormalities and in-hospital mortality.
However, analysis of cumulative ECG abnormalities demonstrated that patients presenting with multiple associated ECG abnormalities had a significantly higher risk of mortality compared with those presenting with one or no abnormality (p < 0.001).
Correlation between ECG findings and right ventricular dysfunction
Transthoracic echocardiography revealed right heart chamber dilation in 50% of cases and pulmonary hypertension in 38.8%.
Patients presenting with the S₁Q₃T₃ pattern, right bundle branch block, or anterior T-wave inversion on ECG more frequently exhibited right heart chamber dilation and pulmonary hypertension, indicating a significant correlation between ECG abnormalities and right ventricular dysfunction. In addition, a significant association was observed between cardiac rhythm disturbances and the presence of intracavitary thrombus (p < 0.001), as well as between the S₁Q₃T₃ pattern and pulmonary hypertension (p = 0.026).
Table 3. Correlation between electrocardiographic abnormalities and echocardiographic findings.
ECG abnormalities | RV dilation (%) | RA dilation (%) | Intracavitary thrombus (%) | Pulmonary artery thrombus (%) | Pulmonary hypertension (%) |
Sinus tachycardia | 60 (p=0.82) | 58.06 (p=0.921) | 100 (p=0.053) | 0 (p=0.23) | 74.19 (p=0.026) |
Rhythm disturbances | 7.5 (p=0.288) | 16.13 (p=0.272) | 60 (p<0.001) | 0 (p=0.72) | 9.68 (p=0.723) |
Conduction disorders | 22.5 (p=0.239) | 25.81 (p=0.12) | 40 (p=0.171) | 0 (p=0.643) | 22.58 (p=0.341) |
Right atrial enlargement | 12.5 (p=0.456) | 12.9 (p=0.491) | 20 (p=0.441) | 0 (p=0.737) | 12.9 (p=0.491) |
Right ventricular hypertrophy | 15 (p=0.048) | 12.9 (p=0.296) | 0 (p=0.475) | 0 (p=0.755) | 12.9 (p=0.296) |
S₁Q₃T₃ pattern | 55 (p=0.116) | 51.61 (p=0.444) | 60 (p=0.524) | 100 (p=0.278) | 67.74 (p=0.002) |
T-wave inversion | 60 (p=0.025) | 54.84 (p=0.296) | 40 (p=0.729) | 100 (p=0.29) | 51.61 (p=0.558) |
RA: right atrium; RV: right ventricle.
Correlation between ECG findings and CT angiography features
Proximal pulmonary embolism was significantly correlated with sinus tachycardia (p = 0.003) and the presence of T-wave inversion (p = 0.018). In addition, T-wave inversion was also significantly associated with segmental pulmonary embolism (p = 0.023).
4. Discussion
Epidemiological and clinical characteristics
The mean age of 53 years observed in our series, with a female predominance (male-to-female ratio = 0.84), is comparable to that reported in several African studies, particularly from Senegal, but lower than that observed in European cohorts, where pulmonary embolism predominantly affects older patients. This difference may be explained by earlier exposure to thromboembolic risk factors in our setting, particularly gynecological factors and obesity.
The main risk factors identified are obesity (36.2%), age over 70 years (31.9%), prolonged immobilization (24.6%), and underlying heart disease (13%) are consistent with data from the international literature and support the ongoing epidemiological transition of venous thromboembolic disease in Africa.
Clinically, dyspnea (83.5%) and chest pain (67%) were the most frequent presenting symptoms, reflecting the nonspecific nature of pulmonary embolism presentation. This finding highlights the need for readily available complementary diagnostic tools, such as the electrocardiogram, in routine clinical practice
| [6] | Kukla P, McIntyre WF, Fijorek K, et al. Electrocardiographic abnormalities in patients with acute pulmonary embolism. Ann Noninvasive Electrocardiol. 2014; 19(3): 234-241. |
| [7] | Stein PD, Dalen JE, McIntyre KM, Sasahara AA, Wenger NK, Willis PW 3rd. The electrocardiogram in acute pulmonary embolism. Prog Cardiovasc Dis. 1975; 17(4): 247-257. |
| [8] | Daniel KR, Courtney DM, Kline JA. Assessment of cardiac stress from massive pulmonary embolism with 12-lead ECG. Chest. 2001; 120(2): 474-481. |
[6-8]
.
Frequency and nature of electrocardiographic abnormalities
In our study, ECG findings were heterogeneous, with a predominance of sinus tachycardia (76.6%), right ventricular repolarization abnormalities manifested as anterior T-wave inversion (47.6%), the S₁Q₃T₃ pattern (38.8%), and right-sided conduction abnormalities, including right bundle branch block (20.4%).
These abnormalities reflect acute right ventricular overload caused by a sudden increase in pulmonary vascular resistance, which represents the central pathophysiological mechanism of acute pulmonary embolism. The relatively high frequency of these findings confirms that the ECG appears to reflect the hemodynamic consequences of pulmonary embolism rather than directly measure them, despite its limited specificity for diagnosis
| [12] | Ndiaye EO, Ngaide A, Faye S, Kane A, Mbaye A, Diack B. Pulmonary embolism: epidemiological, diagnostic, therapeutic and outcome aspects in the cardiology department of Idrissa Pouye Hospital, Dakar (about 89 cases). Rev Mal Respir Actual. 2023; 15(1): 212. |
[12]
.
Electrocardiogram and mortality risk
Our analytical analysis did not demonstrate a statistically significant association between isolated electrocardiographic abnormalities and in-hospital mortality. This finding is consistent with several international studies that emphasize the limited independent prognostic value of a single ECG abnormality.
However, a major finding of our study is that the presence of at least two cumulative electrocardiographic abnormalities was strongly associated with a significantly increased risk of mortality (p < 0.001). This result suggests that ECG interpretation should be global and integrative rather than focused on individual abnormalities, in order to identify patients at high risk of early death
| [8] | Daniel KR, Courtney DM, Kline JA. Assessment of cardiac stress from massive pulmonary embolism with 12-lead ECG. Chest. 2001; 120(2): 474-481. |
| [12] | Ndiaye EO, Ngaide A, Faye S, Kane A, Mbaye A, Diack B. Pulmonary embolism: epidemiological, diagnostic, therapeutic and outcome aspects in the cardiology department of Idrissa Pouye Hospital, Dakar (about 89 cases). Rev Mal Respir Actual. 2023; 15(1): 212. |
[8, 12]
.
Correlation between electrocardiographic abnormalities and right ventricular dysfunction
Transthoracic echocardiography demonstrated right heart chamber dilation in 50% of cases and pulmonary hypertension in 38.8%, indicating frequent right ventricular involvement.
Several ECG abnormalities were significantly associated with these echocardiographic parameters. Anterior T-wave inversion was correlated with right ventricular dilation (p = 0.025), electrical right ventricular hypertrophy was associated with right ventricular dilation (p = 0.048), and the S₁Q₃T₃ pattern was significantly correlated with pulmonary hypertension (p = 0.002). In addition, cardiac rhythm disturbances were strongly associated with the presence of intracavitary thrombus (p < 0.001).
These findings confirm that certain electrocardiographic abnormalities reliably reflect right ventricular dysfunction, which is a key determinant of pulmonary embolism severity
| [12] | Ndiaye EO, Ngaide A, Faye S, Kane A, Mbaye A, Diack B. Pulmonary embolism: epidemiological, diagnostic, therapeutic and outcome aspects in the cardiology department of Idrissa Pouye Hospital, Dakar (about 89 cases). Rev Mal Respir Actual. 2023; 15(1): 212. |
| [13] | Konaté M, Sako M, Sonfo B, Sidibé S, Mariko S, Sow DS, et al. Pulmonary embolism: epidemiological, clinical, therapeutic and outcome aspects in the medicine department of the Hospital of Mali, Bamako. World J Cardiovasc Dis. 2021; 11(4): 242-248. |
| [14] | Oger E; EPI-GETBP Study Group. Incidence of venous thromboembolism: a community-based study in Western France. Thromb Haemost. 2000; 83(5): 657-660. |
| [15] | Miniati M, Monti S, Pratali L, Di Ricco G, Tonelli L, Giuntini C, et al. Value of the electrocardiogram in acute pulmonary embolism. Chest. 2005; 128(3): 1241-1247. |
[12-15]
.
Correlation between electrocardiogram and CT angiographic findings
CT angiographic analysis revealed significant associations between specific ECG abnormalities and the anatomical extent of pulmonary embolism. Sinus tachycardia was significantly correlated with proximal pulmonary embolism (p = 0.003), as was the presence of T-wave inversion (p = 0.018). Moreover, T-wave inversion was also associated with segmental pulmonary embolism (p = 0.023).
These correlations suggest that the ECG may serve as an indirect marker of thrombotic burden, particularly in clinical settings where immediate access to CT pulmonary angiography is limited.
In the African context, characterized by restricted access to advanced imaging modalities, our findings emphasize that the ECG although non specific represents a simple, low-cost, and widely available tool that can contribute to early prognostic stratification of pulmonary embolism. Early identification of patients presenting with multiple ECG abnormalities, signs of electrical right heart strain, or anterior repolarization abnormalities may allow earlier therapeutic decision-making and prioritization of access to specialized investigations and intensive management
| [12] | Ndiaye EO, Ngaide A, Faye S, Kane A, Mbaye A, Diack B. Pulmonary embolism: epidemiological, diagnostic, therapeutic and outcome aspects in the cardiology department of Idrissa Pouye Hospital, Dakar (about 89 cases). Rev Mal Respir Actual. 2023; 15(1): 212. |
| [13] | Konaté M, Sako M, Sonfo B, Sidibé S, Mariko S, Sow DS, et al. Pulmonary embolism: epidemiological, clinical, therapeutic and outcome aspects in the medicine department of the Hospital of Mali, Bamako. World J Cardiovasc Dis. 2021; 11(4): 242-248. |
| [14] | Oger E; EPI-GETBP Study Group. Incidence of venous thromboembolism: a community-based study in Western France. Thromb Haemost. 2000; 83(5): 657-660. |
| [15] | Miniati M, Monti S, Pratali L, Di Ricco G, Tonelli L, Giuntini C, et al. Value of the electrocardiogram in acute pulmonary embolism. Chest. 2005; 128(3): 1241-1247. |
[12-15]
.
Study limitations
This study has several limitations, including its retrospective and single-center design, the relatively small sample size, and the lack of systematic availability of certain prognostic biomarkers such as troponin and B-type natriuretic peptide. Nevertheless, it provides important and context-specific data that remain scarce in the African literature. Moreover, it highlights the additive prognostic value of the electrocardiogram in patients with pulmonary embolism.
Conclusion
Pulmonary embolism is a frequent and potentially life-threatening condition in our setting. In resource-limited environments, the electrocardiogram, although nonspecific, remains a readily available and useful tool for the initial assessment of patients with suspected pulmonary embolism. Our study demonstrates that electrocardiographic abnormalities are common and that their cumulative presence is significantly associated with increased in-hospital mortality and right ventricular dysfunction. The ECG therefore allows early prognostic stratification, complementary to clinical and echocardiographic findings.
Early identification of patients presenting with multiple ECG abnormalities may help optimize management strategies and improve the prognosis of pulmonary embolism in African hospital settings.
Abbreviations
AASI | Ambulatory Arterial Stiffness Index |
AIx | Augmentation Index |
aPWV | Aortic Pulse Wave Velocity |
ACEI | Angiotensin-Converting Enzyme Inhibitors |
ARB | Angiotensin II Receptor Blockers |
BMI | Body Mass Index |
BP | Blood Pressure |
cfPWV | Carotid-Femoral Pulse Wave Velocity |
CV | Cardiovascular |
CVD | Cardiovascular Diseases |
DBP | Diastolic Blood Pressure |
ESC | European Society of Cardiology |
ESH | European Society of Hypertension |
FDR | Cardiovascular Risk Factors |
HbA1c | Glycated Hemoglobin |
HF | Heart Failure |
HTN | Hypertension (Arterial Hypertension) |
LVH | Left Ventricular Hypertrophy |
MAPA/ABPM | Ambulatory Blood Pressure Monitoring |
NO | Nitric Oxide |
PP | Pulse Pressure |
PWV | Pulse Wave Velocity |
PWVtf | Toe-Finger Pulse Wave Velocity |
SBP | Systolic Blood Pressure |
RAAS | Renin–Angiotensin–Aldosterone System |
TTE | Transthoracic Echocardiography |
VOP | Pulse Wave Velocity |
VOPcf | Carotid-Femoral Pulse Wave Velocity |
VOPdo | Toe-Finger Pulse Wave Velocity |
Author Contributions
Mingou Joseph Salvador: Conceptualization, Funding acquisition, Investigation, Supervision, Writing – original draft, Writing – review & editing
Diallo Ramatoulaye: Data curation, Formal Analysis, Methodology, Resources
Diao Maboury: Project administration, Software, Validation
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Goldhaber SZ, Bounameaux H. Pulmonary embolism and deep vein thrombosis. Lancet. 2012; 379(9828): 1835-1846.
|
| [2] |
Wendelboe AM, Raskob GE. Global burden of thrombosis: epidemiologic aspects. Circ Res. 2016; 118(9): 1340-1347.
|
| [3] |
Konstantinides SV, Meyer G, Becattini C, et al. 2019 ESC guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J. 2020; 41(4): 543-603.
|
| [4] |
Van der Hulle T, Cheung WY, Kooij S, et al. Simplified diagnostic management of suspected pulmonary embolism (the YEARS study): a prospective, multicentre, cohort study. Lancet. 2017; 390(10091): 289-297.
|
| [5] |
Kakou Guikahue MK, Soro K, Anzouan-Kacou E, et al. Challenges in the management of pulmonary embolism in sub-Saharan Africa: a perspective. Cardiovasc Diagn Ther. 2020; 10(5): 1514-1521.
|
| [6] |
Kukla P, McIntyre WF, Fijorek K, et al. Electrocardiographic abnormalities in patients with acute pulmonary embolism. Ann Noninvasive Electrocardiol. 2014; 19(3): 234-241.
|
| [7] |
Stein PD, Dalen JE, McIntyre KM, Sasahara AA, Wenger NK, Willis PW 3rd. The electrocardiogram in acute pulmonary embolism. Prog Cardiovasc Dis. 1975; 17(4): 247-257.
|
| [8] |
Daniel KR, Courtney DM, Kline JA. Assessment of cardiac stress from massive pulmonary embolism with 12-lead ECG. Chest. 2001; 120(2): 474-481.
|
| [9] |
Kucher N, Walpoth N, Wustmann K, Noveanu M, Gertsch M. QR in V1—an ECG sign associated with right ventricular strain and adverse clinical outcome in pulmonary embolism. Eur Heart J. 2003; 24(12): 1113-1119.
|
| [10] |
Geibel A, Zehender M, Kasper W, Olschewski M, Klima C, Konstantinides SV. Prognostic value of the ECG on admission in patients with acute major pulmonary embolism. Eur Respir J. 2005; 25(5): 843-848.
|
| [11] |
Vanni S, Polidori G, Vergara R, et al. Prognostic value of ECG among patients with acute pulmonary embolism and normal blood pressure. Am J Med. 2009; 122(3): 257-264.
|
| [12] |
Ndiaye EO, Ngaide A, Faye S, Kane A, Mbaye A, Diack B. Pulmonary embolism: epidemiological, diagnostic, therapeutic and outcome aspects in the cardiology department of Idrissa Pouye Hospital, Dakar (about 89 cases). Rev Mal Respir Actual. 2023; 15(1): 212.
|
| [13] |
Konaté M, Sako M, Sonfo B, Sidibé S, Mariko S, Sow DS, et al. Pulmonary embolism: epidemiological, clinical, therapeutic and outcome aspects in the medicine department of the Hospital of Mali, Bamako. World J Cardiovasc Dis. 2021; 11(4): 242-248.
|
| [14] |
Oger E; EPI-GETBP Study Group. Incidence of venous thromboembolism: a community-based study in Western France. Thromb Haemost. 2000; 83(5): 657-660.
|
| [15] |
Miniati M, Monti S, Pratali L, Di Ricco G, Tonelli L, Giuntini C, et al. Value of the electrocardiogram in acute pulmonary embolism. Chest. 2005; 128(3): 1241-1247.
|
Cite This Article
-
APA Style
Salvador, M. J., Ramatoulaye, D., Issa, Y., Tening, D. M., Antoine, S. S., et al. (2026). Electrocardiographic Characteristics of Pulmonary Embolism in Patients Hospitalized at Dalal Jamm National Hospital Center (2021–2023). International Journal of Cardiovascular and Thoracic Surgery, 12(2), 33-39. https://doi.org/10.11648/j.ijcts.20261202.13
 Copy
|
Copy
|
 Download
Download
ACS Style
Salvador, M. J.; Ramatoulaye, D.; Issa, Y.; Tening, D. M.; Antoine, S. S., et al. Electrocardiographic Characteristics of Pulmonary Embolism in Patients Hospitalized at Dalal Jamm National Hospital Center (2021–2023). Int. J. Cardiovasc. Thorac. Surg. 2026, 12(2), 33-39. doi: 10.11648/j.ijcts.20261202.13
Copy
|
Download
AMA Style
Salvador MJ, Ramatoulaye D, Issa Y, Tening DM, Antoine SS, et al. Electrocardiographic Characteristics of Pulmonary Embolism in Patients Hospitalized at Dalal Jamm National Hospital Center (2021–2023). Int J Cardiovasc Thorac Surg. 2026;12(2):33-39. doi: 10.11648/j.ijcts.20261202.13
Copy
|
Download
-
@article{10.11648/j.ijcts.20261202.13,
author = {Mingou Joseph Salvador and Diallo Ramatoulaye and Yakusu Issa and Diouf Marguerite Tening and Sarr Simon Antoine and Aw Fatou and Gaye Ngone Diaba and Ngaide Aliou Alassane and Ndiaye Malick and Dioum Momar and Bodian Malick and Ndiaye Mouhamadou Bamba and Diao Maboury and Kane Abdoul},
title = {Electrocardiographic Characteristics of Pulmonary Embolism in Patients Hospitalized at Dalal Jamm National Hospital Center (2021–2023)},
journal = {International Journal of Cardiovascular and Thoracic Surgery},
volume = {12},
number = {2},
pages = {33-39},
doi = {10.11648/j.ijcts.20261202.13},
url = {https://doi.org/10.11648/j.ijcts.20261202.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcts.20261202.13},
abstract = {Introduction: Pulmonary embolism (PE) is a major cause of cardiovascular morbidity and mortality. In Africa, limited access to computed tomography pulmonary angiography (CTPA) enhances the clinical value of the electrocardiogram (ECG), a rapid and widely available tool, for early diagnostic orientation and prognostic assessment. Objectives: To describe ECG abnormalities observed in patients with acute pulmonary embolism and to analyze their association with in-hospital mortality and paraclinical markers of severity. Methods: We conducted a retrospective, descriptive, and analytical study including 103 patients hospitalized for confirmed pulmonary embolism in the cardiology department of the National Hospital Center Dalal Jamm, Dakar, Senegal, between January 1, 2021 and December 31, 2023. Clinical characteristics, risk factors, biological parameters, transthoracic echocardiographic findings, and CTPA results were collected. The associations between isolated or cumulative ECG abnormalities and in-hospital mortality were analyzed. Results: The mean age was 53 years, with a female predominance (male-to-female ratio: 0.84). The main risk factors were obesity (36.2%), age >70 years (31.9%), prolonged immobilization (24.6%), underlying heart disease (13%), and gynecological factors (14.5%). The most common symptoms were dyspnea (83.5%), chest pain (67%), and cough (49.5%). The most frequent ECG abnormalities were sinus tachycardia (62.1%), subepicardial ischemia (47.6%), the S1Q3T3 pattern (38.8%), and right-sided conduction disturbances, including right bundle branch block (20.4%). Transthoracic echocardiography revealed right heart chamber dilation (50%), pulmonary hypertension (38.8%), and intracardiac thrombus (6.3%). CTPA showed bilateral PE in 29.1% of cases, right-sided PE in 15.5%, and left-sided PE in 9.7%. All patients received anticoagulation therapy. In-hospital mortality risk was significantly higher in patients presenting with at least two cumulative ECG abnormalities and was strongly associated with right heart dilation and pulmonary hypertension. Conclusion: Pulmonary embolism represents a significant clinical burden in Senegal. Although nonspecific, the ECG provides valuable information for early suspicion and prognostic stratification, particularly in emergency settings with limited resources. The presence of multiple ECG abnormalities identifies patients at high risk of early mortality. Early recognition of these findings, combined with risk factor assessment and evaluation of right ventricular involvement, may facilitate timely management and improve patient outcomes.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Electrocardiographic Characteristics of Pulmonary Embolism in Patients Hospitalized at Dalal Jamm National Hospital Center (2021–2023)
AU - Mingou Joseph Salvador
AU - Diallo Ramatoulaye
AU - Yakusu Issa
AU - Diouf Marguerite Tening
AU - Sarr Simon Antoine
AU - Aw Fatou
AU - Gaye Ngone Diaba
AU - Ngaide Aliou Alassane
AU - Ndiaye Malick
AU - Dioum Momar
AU - Bodian Malick
AU - Ndiaye Mouhamadou Bamba
AU - Diao Maboury
AU - Kane Abdoul
Y1 - 2026/03/10
PY - 2026
N1 - https://doi.org/10.11648/j.ijcts.20261202.13
DO - 10.11648/j.ijcts.20261202.13
T2 - International Journal of Cardiovascular and Thoracic Surgery
JF - International Journal of Cardiovascular and Thoracic Surgery
JO - International Journal of Cardiovascular and Thoracic Surgery
SP - 33
EP - 39
PB - Science Publishing Group
SN - 2575-4882
UR - https://doi.org/10.11648/j.ijcts.20261202.13
AB - Introduction: Pulmonary embolism (PE) is a major cause of cardiovascular morbidity and mortality. In Africa, limited access to computed tomography pulmonary angiography (CTPA) enhances the clinical value of the electrocardiogram (ECG), a rapid and widely available tool, for early diagnostic orientation and prognostic assessment. Objectives: To describe ECG abnormalities observed in patients with acute pulmonary embolism and to analyze their association with in-hospital mortality and paraclinical markers of severity. Methods: We conducted a retrospective, descriptive, and analytical study including 103 patients hospitalized for confirmed pulmonary embolism in the cardiology department of the National Hospital Center Dalal Jamm, Dakar, Senegal, between January 1, 2021 and December 31, 2023. Clinical characteristics, risk factors, biological parameters, transthoracic echocardiographic findings, and CTPA results were collected. The associations between isolated or cumulative ECG abnormalities and in-hospital mortality were analyzed. Results: The mean age was 53 years, with a female predominance (male-to-female ratio: 0.84). The main risk factors were obesity (36.2%), age >70 years (31.9%), prolonged immobilization (24.6%), underlying heart disease (13%), and gynecological factors (14.5%). The most common symptoms were dyspnea (83.5%), chest pain (67%), and cough (49.5%). The most frequent ECG abnormalities were sinus tachycardia (62.1%), subepicardial ischemia (47.6%), the S1Q3T3 pattern (38.8%), and right-sided conduction disturbances, including right bundle branch block (20.4%). Transthoracic echocardiography revealed right heart chamber dilation (50%), pulmonary hypertension (38.8%), and intracardiac thrombus (6.3%). CTPA showed bilateral PE in 29.1% of cases, right-sided PE in 15.5%, and left-sided PE in 9.7%. All patients received anticoagulation therapy. In-hospital mortality risk was significantly higher in patients presenting with at least two cumulative ECG abnormalities and was strongly associated with right heart dilation and pulmonary hypertension. Conclusion: Pulmonary embolism represents a significant clinical burden in Senegal. Although nonspecific, the ECG provides valuable information for early suspicion and prognostic stratification, particularly in emergency settings with limited resources. The presence of multiple ECG abnormalities identifies patients at high risk of early mortality. Early recognition of these findings, combined with risk factor assessment and evaluation of right ventricular involvement, may facilitate timely management and improve patient outcomes.
VL - 12
IS - 2
ER -
Copy
|
Download