Pyopericardium is an uncommon yet potentially fatal paediatric emergency, typically of bacterial origin, but increasingly linked to opportunistic fungal pathogens in immunocompromised individuals. This report delineates the clinical progression of a 2-year-old female with transfusion-dependent Diamond-Blackfan Anaemia (DBA), who exhibited a one-month history of insidious fever, ultimately leading to acute cardiac tamponade. When the patient was admitted to the hospital in an emergency, they had low blood pressure (80/50 mmHg), muffled heart sounds, and severe breathing problems. Laboratory tests showed very low levels of haemoglobin (5.2 g/dL) and very high levls of inflammatory markers. An echocardiogram showed a huge pericardial effusion with right ventricular diastolic collapse and a reduced ejection fraction of 40%. Emergent pericardiocentesis produced 150 mL of purulent fluid, with cultures identifying Candida glabrata as the etiological agent. Management required a multi-faceted approach that included an emergent subxiphoid partial pericardiectomy, inotropic support, and blood transfusions. Antifungal treatment started with liposomal amphotericin B and was successfully switched to oral voriconazole after confirming that the patient was susceptible. Before being discharged on hospital day 19, the patient's heart function had improved so much that their ejection fraction was back to normal at 55%. This case shows how hard it is to diagnose fungal pyopericardium in people with congenital bone marrow failure syndromes. It also shows how important it is to do echocardiographic screening early and use aggressive surgical-pharmacological synergy to lower the high death rates that come with a late diagnosis.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Pyopericardium, which is the buildup of pus-filled fluid in the pericardial sac, is a rare but very serious emergency in paediatric medicine
[4]
Sagristà-Sauleda J, Mercé AS, Soler-Soler J. Diagnosis and management of pericardial effusion. World J Cardiol. 2011; 3(5): 135-143.
[4]
. If this condition isn't treated, it can quickly lead to cardiac tamponade, which can cause unstable blood flow and heart muscle dysfunction through mechanical compression and inflammatory sequelae
[2]
Imazio M, Adler Y, Charron P, et al. Management of pericardial diseases: a position statement of the European Society of Cardiology. Eur Heart J. 2020; 41(7): 1554-1560.
[14]
Jette N, Gebhardt C, Coustinos D. Case report: cardiac tamponade secondary to candida pericarditis. J Surg Case Rep. 2024; 2024(3): rjae150.
[2, 14]
. In kids, the causes are often bacteria that spread from nearby infections, like pneumonia or mediastinitis, or through the blood in the case of bacteremia
[14]
Jette N, Gebhardt C, Coustinos D. Case report: cardiac tamponade secondary to candida pericarditis. J Surg Case Rep. 2024; 2024(3): rjae150.
[14]
. Fungal origins, while less common, make things even more complicated, especially for people with weak immune systems, who are more likely to be attacked by opportunistic invaders like Candida species
[3]
Pappas PG, Kauffman CA, Andes DR, Clancy CJ, Marr KA, Ostrosky-Zeichner L, et al. Clinical practice guideline for the management of candidiasis: 2016 update by the Infectious Diseases Society of America. Clin Infect Dis. 2016; 62(4): e1-e50.
[6]
Jancic P, Milutinovic S, Ward M, Radovanovic M, Jovanovic N, Antic M, et al. Fungal Pericarditis—A Systematic Review of 101 Cases. Microorganisms. 2025; 13(4): 707.
[7]
Dahl C, Johansen HK, Kjaeldgaard P, Helweg-Larsen J. A paediatric case of Candida pericarditis and oesophagus stricture during treatment for acute lymphatic leukaemia. Acta Oncol. 2007; 46(3): 397-399.
[8]
Azhar A. Successful management of fungal pericarditis and endocarditis in a neonate: A case report. J Exp Integr Med. 2012; 2(4): 357-360.
[3, 6-8]
.
Diamond-Blackfan anaemia (DBA) is a classic example of this type of inherited bone marrow failure syndrome
[1]
Da Costa L, Narla A, Mohandas N. Diamond-Blackfan anemia: etiology, pathophysiology, and treatment. Blood Rev. 2018; 32(5): 413-424.
[5]
Vlachos A, Osorio DS, Atsidaftos E, Kang J, Lababidi ML, Seiden HS, Gruber D, Glader BE, Onel K, Farrar JE, Bodine DM, Aspesi A, Dianzani I, Ramenghi U, Ellis SR, Lipton JM. Increased Prevalence of Congenital Heart Disease in Children With Diamond Blackfan Anemia. Circ Genom Precis Med. 2018; 11(5): e002044.
[1, 5]
. DBA shows up early in life as macrocytic anaemia and isolated erythroid hypoplasia. It often needs blood transfusions for the rest of its life
[1]
Da Costa L, Narla A, Mohandas N. Diamond-Blackfan anemia: etiology, pathophysiology, and treatment. Blood Rev. 2018; 32(5): 413-424.
[1]
. People with this condition often have birth defects, like craniofacial dysmorphisms and thumb problems, and they are more likely to get cancer and infections
[1]
Da Costa L, Narla A, Mohandas N. Diamond-Blackfan anemia: etiology, pathophysiology, and treatment. Blood Rev. 2018; 32(5): 413-424.
[5]
Vlachos A, Osorio DS, Atsidaftos E, Kang J, Lababidi ML, Seiden HS, Gruber D, Glader BE, Onel K, Farrar JE, Bodine DM, Aspesi A, Dianzani I, Ramenghi U, Ellis SR, Lipton JM. Increased Prevalence of Congenital Heart Disease in Children With Diamond Blackfan Anemia. Circ Genom Precis Med. 2018; 11(5): e002044.
[12]
Moisa SM, Spoiala EL, Trandafir LM, Butnariu LI, Miron IC, Ciobanu A, Mocanu A, Ivanov A, Ciongradi CI, Sarbu I, Ciubara A, Rusu CD, Luca AC, Burlacu A. Unusual Association of Diamond–Blackfan Anemia and Severe Sinus Bradycardia. Cureus. 2023; 15(2): e34736.
[1, 5, 12]
. People with chronic anaemia, repeated blood transfusions (which can lead to iron overload), and possible corticosteroid treatment for anaemia have weaker immune systems, which makes them more likely to get strange infections like fungal pericarditis
[1]
Da Costa L, Narla A, Mohandas N. Diamond-Blackfan anemia: etiology, pathophysiology, and treatment. Blood Rev. 2018; 32(5): 413-424.
[6]
Jancic P, Milutinovic S, Ward M, Radovanovic M, Jovanovic N, Antic M, et al. Fungal Pericarditis—A Systematic Review of 101 Cases. Microorganisms. 2025; 13(4): 707.
[13]
Bollempalli H, et al. A Rare Case Of Cardiomyopathy With Diamond-Blackfan Anemia? J Am Coll Cardiol. 2024; 83(13_Supplement): 2303.
[1, 6, 13]
.
The link between DBA and infectious complications shows a big problem with diagnosis: symptoms may first look like common febrile illnesses, which makes it hard to tell if the heart is involved
[7]
Dahl C, Johansen HK, Kjaeldgaard P, Helweg-Larsen J. A paediatric case of Candida pericarditis and oesophagus stricture during treatment for acute lymphatic leukaemia. Acta Oncol. 2007; 46(3): 397-399.
[15]
Khillan V, Rathore N, Kathuria S, Chowdhary A. A rare case of breakthrough fungal pericarditis due to fluconazole-resistant Candida auris. JMM Case Rep. 2014; 1(3): e003005.
[7, 15]
. There isn't a lot of writing yet about fungal pyopericardium in DBA. Most of the information out there is case reports that show how hard it is to diagnose and how important it is to use aggressive multimodal therapy
[6]
Jancic P, Milutinovic S, Ward M, Radovanovic M, Jovanovic N, Antic M, et al. Fungal Pericarditis—A Systematic Review of 101 Cases. Microorganisms. 2025; 13(4): 707.
[9]
Sung J, Perez IE, Feinstein A, Stein DK. A case report of purulent pericarditis caused by Candida albicans. Medicine (Baltimore). 2018; 97(28): e11286.
[10]
Matta A, Elenizi K, AlHarthi R, et al. A Rare Case of Candida Pericarditis Associated with Esophagopericardial Fistula. Am J Case Rep. 2019; 20: 1031-1035.
[11]
Neughebauer B, Alvarez V, Harb T, Keefer M. Constrictive pericarditis caused by Candida glabrata in an immunocompetent patient. Scand J Infect Dis. 2002; 34(8): 615-619.
[6, 9-11]
. This report talks about the clinical course of a toddler with DBA who developed extensive pyopericardium due to Candida glabrata, which caused myocardial distress
[6]
Jancic P, Milutinovic S, Ward M, Radovanovic M, Jovanovic N, Antic M, et al. Fungal Pericarditis—A Systematic Review of 101 Cases. Microorganisms. 2025; 13(4): 707.
[11]
Neughebauer B, Alvarez V, Harb T, Keefer M. Constrictive pericarditis caused by Candida glabrata in an immunocompetent patient. Scand J Infect Dis. 2002; 34(8): 615-619.
[6, 11]
. This report goes into great detail about how to handle these cases well by talking about presentation, diagnostics, interventions, and outcomes. It also says that more needs to be done to help kids with blood problems
[2]
Imazio M, Adler Y, Charron P, et al. Management of pericardial diseases: a position statement of the European Society of Cardiology. Eur Heart J. 2020; 41(7): 1554-1560.
[3]
Pappas PG, Kauffman CA, Andes DR, Clancy CJ, Marr KA, Ostrosky-Zeichner L, et al. Clinical practice guideline for the management of candidiasis: 2016 update by the Infectious Diseases Society of America. Clin Infect Dis. 2016; 62(4): e1-e50.
[2, 3]
. By discussing pathophysiological mechanisms, therapeutic rationales, and prognostic insights in more detail, we hope to improve the paediatric literature and help doctors choose the best treatment options
[1]
Da Costa L, Narla A, Mohandas N. Diamond-Blackfan anemia: etiology, pathophysiology, and treatment. Blood Rev. 2018; 32(5): 413-424.
[6]
Jancic P, Milutinovic S, Ward M, Radovanovic M, Jovanovic N, Antic M, et al. Fungal Pericarditis—A Systematic Review of 101 Cases. Microorganisms. 2025; 13(4): 707.
[1, 6]
.
2. Case Presentation
The patient, a 2-year-old female hailing from rural Punjab, India, carried a diagnosis of Diamond-Blackfan anemia established shortly after birth due to persistently low hemoglobin levels necessitating monthly blood transfusions. Her medical history was punctuated by recurrent anemia-related fatigue, pallor, and growth retardation, with her weight stagnating at 10 kg—below the 5th percentile for age. Transfusion dependence had been managed at a local hematology clinic, but no genetic confirmation via ribosomal protein gene sequencing had been pursued owing to resource constraints. Iron studies prior to this admission consistently revealed low serum iron, reflective of chronic disease and transfusion-related hemosiderosis, though chelation therapy had not been initiated.
Approximately one month preceding admission, the child developed an insidious low-grade fever, initially dismissed as a viral prodrome. Over time, this evolved into persistent pyrexia (up to 39°C), accompanied by nonspecific symptoms including irritability, lethargy, and progressive anorexia with markedly decreased oral intake. Parental reports indicated episodic cough without hemoptysis or purulent sputum, and no overt gastrointestinal disturbances. Despite empirical antibiotics from a community practitioner, the fever persisted, culminating in an acute decompensation on November 8, 2025. Suddenly, the child exhibited severe breathlessness, cyanosis around the lips, and a brief episode of unconsciousness lasting minutes, prompting urgent transfer to the pediatric emergency department.
Upon arrival, vital signs were alarming: heart rate 160 beats per minute (tachycardic), respiratory rate 50 breaths per minute (tachypneic), blood pressure 80/50 mmHg (hypotensive), and oxygen saturation 88% on room air. Physical examination disclosed muffled heart sounds, jugular venous distension, and pulsus paradoxus—hallmarks of pericardial tamponade. Respiratory distress was evident with intercostal retractions and nasal flaring. Pallor was profound, consistent with her baseline anemia, but no icterus, lymphadenopathy, or hepatosplenomegaly was noted. Neurological assessment post-resuscitation revealed no focal deficits, though the child remained lethargic.
Initial laboratory investigations corroborated the clinical suspicions. Hemoglobin was critically low at 5.2 g/dL, with a mean corpuscular volume of 102 fL (macrocytic), reticulocyte count <0.5% (indicating aplasia), and serum iron at 35 µg/dL—exacerbated by the ongoing infection. Inflammatory markers were elevated: C-reactive protein 120 mg/L and erythrocyte sedimentation rate 80 mm/hour. Blood cultures drawn on admission were initially sterile, but pericardial fluid aspirated emergently grew Candida glabrata on fungal culture, sensitive to amphotericin B and fluconazole. Echocardiography confirmed massive pericardial effusion with right ventricular diastolic collapse and reduced ejection fraction (40%), signifying myocardial dysfunction.
Chest X-ray demonstrated cardiomegaly with a "water bottle" silhouette, while electrocardiography showed low-voltage complexes and electrical alternans.
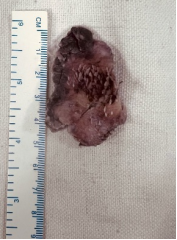
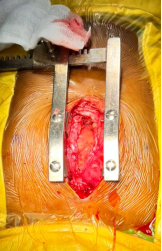
Stabilization ensued with supplemental oxygen, intravenous fluids, and inotropic support (dopamine infusion) to bolster cardiac output. Broad-spectrum antibiotics (vancomycin and ceftriaxone) were initiated empirically, alongside antifungal therapy with liposomal amphotericin B upon fungal suspicion. Given the tamponade physiology, urgent pericardiocentesis yielded 150 mL of purulent, turbid fluid, providing immediate hemodynamic relief. Subsequent surgical consultation led to pericardial drainage and partial pericardiectomy via a subxiphoid approach under general anesthesia, with placement of a single pericardial drain to prevent reaccumulation.
Postoperatively, the child was transferred to the neonatal intensive care unit (NICU) for close monitoring. Over the ensuing 5 days, she received continued inotropic support tapering as ejection fraction improved to 55% on follow-up echocardiography. Antifungal therapy was transitioned to oral voriconazole after susceptibility confirmation, administered for a planned 6-week course. Transfusions elevated hemoglobin to 9.5 g/dL, alleviating anemia symptoms. The single drain output diminished progressively, totaling 200 mL over 6 days, and was removed on postoperative day 6 without rebound effusion. Serial cultures from drain fluid remained sterile, and fever defervesced by day 3. Nutritional support via nasogastric feeds addressed the decreased intake, with gradual resumption of oral feeds. By hospital day 10 in NICU transition, the child exhibited restored consciousness, improved activity, and stable vitals.
Discharge occurred on November 27, 2025, after a total 19-day hospitalization. At follow-up one month later, she was asymptomatic, with normalized cardiac function on echocardiography and stable hemoglobin via ongoing transfusions. Recommendations included genetic testing for DBA confirmation, iron chelation initiation, and infectious disease surveillance to mitigate future risks.
3. Discussion
The child with Diamond Blackfan anemia and fungal pyopericardium grew slowly, which is an example of the "stealthy siege," in which chronic immunosuppression hides aggressive pathology until a crisis happens
[6]
Jancic P, Milutinovic S, Ward M, Radovanovic M, Jovanovic N, Antic M, et al. Fungal Pericarditis—A Systematic Review of 101 Cases. Microorganisms. 2025; 13(4): 707.
[7]
Dahl C, Johansen HK, Kjaeldgaard P, Helweg-Larsen J. A paediatric case of Candida pericarditis and oesophagus stricture during treatment for acute lymphatic leukaemia. Acta Oncol. 2007; 46(3): 397-399.
[6, 7]
. Candida glabrata, a non-albicans species known for azole resistance and biofilm formation, likely established itself during transfusion-induced iron overload and anemia-related immune suppression
[3]
Pappas PG, Kauffman CA, Andes DR, Clancy CJ, Marr KA, Ostrosky-Zeichner L, et al. Clinical practice guideline for the management of candidiasis: 2016 update by the Infectious Diseases Society of America. Clin Infect Dis. 2016; 62(4): e1-e50.
[6]
Jancic P, Milutinovic S, Ward M, Radovanovic M, Jovanovic N, Antic M, et al. Fungal Pericarditis—A Systematic Review of 101 Cases. Microorganisms. 2025; 13(4): 707.
[11]
Neughebauer B, Alvarez V, Harb T, Keefer M. Constrictive pericarditis caused by Candida glabrata in an immunocompetent patient. Scand J Infect Dis. 2002; 34(8): 615-619.
[15]
Khillan V, Rathore N, Kathuria S, Chowdhary A. A rare case of breakthrough fungal pericarditis due to fluconazole-resistant Candida auris. JMM Case Rep. 2014; 1(3): e003005.
[3, 6, 11, 15]
. DBA's pathophysiology, which is based on ribosomal protein haploinsufficiency, makes it harder for red blood cells to form and slightly weakens the body's natural defences, making it easier for opportunistic mycoses to grow
[1]
Da Costa L, Narla A, Mohandas N. Diamond-Blackfan anemia: etiology, pathophysiology, and treatment. Blood Rev. 2018; 32(5): 413-424.
[5]
Vlachos A, Osorio DS, Atsidaftos E, Kang J, Lababidi ML, Seiden HS, Gruber D, Glader BE, Onel K, Farrar JE, Bodine DM, Aspesi A, Dianzani I, Ramenghi U, Ellis SR, Lipton JM. Increased Prevalence of Congenital Heart Disease in Children With Diamond Blackfan Anemia. Circ Genom Precis Med. 2018; 11(5): e002044.
[1, 5]
. The month-long fever shows how long it can take to get a diagnosis in places with few resources, where viral or bacterial infections are the most common
[7]
Dahl C, Johansen HK, Kjaeldgaard P, Helweg-Larsen J. A paediatric case of Candida pericarditis and oesophagus stricture during treatment for acute lymphatic leukaemia. Acta Oncol. 2007; 46(3): 397-399.
[9]
Sung J, Perez IE, Feinstein A, Stein DK. A case report of purulent pericarditis caused by Candida albicans. Medicine (Baltimore). 2018; 97(28): e11286.
[7, 9]
.
Fungi can spread to the pericardium through the blood from a hidden focus (like a catheter, which isn't present here) or by spreading to nearby areas
[6]
Jancic P, Milutinovic S, Ward M, Radovanovic M, Jovanovic N, Antic M, et al. Fungal Pericarditis—A Systematic Review of 101 Cases. Microorganisms. 2025; 13(4): 707.
[9]
Sung J, Perez IE, Feinstein A, Stein DK. A case report of purulent pericarditis caused by Candida albicans. Medicine (Baltimore). 2018; 97(28): e11286.
[10]
Matta A, Elenizi K, AlHarthi R, et al. A Rare Case of Candida Pericarditis Associated with Esophagopericardial Fistula. Am J Case Rep. 2019; 20: 1031-1035.
[6, 9, 10]
. In this case, there aren't any clear risk factors besides DBA, like central lines or immunosuppression. However, it seems possible that endogenous translocation could happen because anaemia weakens the mucosal barrier
[3]
Pappas PG, Kauffman CA, Andes DR, Clancy CJ, Marr KA, Ostrosky-Zeichner L, et al. Clinical practice guideline for the management of candidiasis: 2016 update by the Infectious Diseases Society of America. Clin Infect Dis. 2016; 62(4): e1-e50.
[6]
Jancic P, Milutinovic S, Ward M, Radovanovic M, Jovanovic N, Antic M, et al. Fungal Pericarditis—A Systematic Review of 101 Cases. Microorganisms. 2025; 13(4): 707.
[3, 6]
. The pyopericardium caused tamponade by changing the way fluids move: higher intrapericardial pressure made it harder for the heart to fill with blood during diastole, which made breathing difficult and lowered blood pressure
[2]
Imazio M, Adler Y, Charron P, et al. Management of pericardial diseases: a position statement of the European Society of Cardiology. Eur Heart J. 2020; 41(7): 1554-1560.
[4]
Sagristà-Sauleda J, Mercé AS, Soler-Soler J. Diagnosis and management of pericardial effusion. World J Cardiol. 2011; 3(5): 135-143.
[14]
Jette N, Gebhardt C, Coustinos D. Case report: cardiac tamponade secondary to candida pericarditis. J Surg Case Rep. 2024; 2024(3): rjae150.
[2, 4, 14]
. Simultaneous myocardial dysfunction, evidenced by a reduced ejection fraction, likely stemmed from direct myocarditis, a cytokine storm, or compressive ischaemia, intensifying the crisis to the level of unconsciousness
[2]
Imazio M, Adler Y, Charron P, et al. Management of pericardial diseases: a position statement of the European Society of Cardiology. Eur Heart J. 2020; 41(7): 1554-1560.
[13]
Bollempalli H, et al. A Rare Case Of Cardiomyopathy With Diamond-Blackfan Anemia? J Am Coll Cardiol. 2024; 83(13_Supplement): 2303.
[2, 13]
.
Diagnostic tools were very important. For example, echocardiography's ability to show signs of effusion and tamponade in real time led to immediate treatment, and fungal culture's ability to grow C. glabrata directed therapy
[2]
Imazio M, Adler Y, Charron P, et al. Management of pericardial diseases: a position statement of the European Society of Cardiology. Eur Heart J. 2020; 41(7): 1554-1560.
[4]
Sagristà-Sauleda J, Mercé AS, Soler-Soler J. Diagnosis and management of pericardial effusion. World J Cardiol. 2011; 3(5): 135-143.
[6]
Jancic P, Milutinovic S, Ward M, Radovanovic M, Jovanovic N, Antic M, et al. Fungal Pericarditis—A Systematic Review of 101 Cases. Microorganisms. 2025; 13(4): 707.
[2, 4, 6]
. The low level of serum iron (35 µg/dL) not only showed that the person had chronic anaemia, but it also suggested that the iron was being stored in an infection, since fungi use host iron very well
[1]
Da Costa L, Narla A, Mohandas N. Diamond-Blackfan anemia: etiology, pathophysiology, and treatment. Blood Rev. 2018; 32(5): 413-424.
[3]
Pappas PG, Kauffman CA, Andes DR, Clancy CJ, Marr KA, Ostrosky-Zeichner L, et al. Clinical practice guideline for the management of candidiasis: 2016 update by the Infectious Diseases Society of America. Clin Infect Dis. 2016; 62(4): e1-e50.
[1, 3]
. Streptococci or staphylococci are the main cause of bacterial pyopericardium, and antibiotics are the only treatment. Fungal variants, on the other hand, need antifungals and often surgery because biofilms make drugs useless
[3]
Pappas PG, Kauffman CA, Andes DR, Clancy CJ, Marr KA, Ostrosky-Zeichner L, et al. Clinical practice guideline for the management of candidiasis: 2016 update by the Infectious Diseases Society of America. Clin Infect Dis. 2016; 62(4): e1-e50.
[6]
Jancic P, Milutinovic S, Ward M, Radovanovic M, Jovanovic N, Antic M, et al. Fungal Pericarditis—A Systematic Review of 101 Cases. Microorganisms. 2025; 13(4): 707.
[8]
Azhar A. Successful management of fungal pericarditis and endocarditis in a neonate: A case report. J Exp Integr Med. 2012; 2(4): 357-360.
[3, 6, 8]
.
The main part of the treatment was surgery. First, pericardiocentesis was done to relieve pressure, and then pericardiectomy was done to remove inflamed tissue and stop constriction, which can happen in up to 20% of cases that aren't treated
[2]
Imazio M, Adler Y, Charron P, et al. Management of pericardial diseases: a position statement of the European Society of Cardiology. Eur Heart J. 2020; 41(7): 1554-1560.
[4]
Sagristà-Sauleda J, Mercé AS, Soler-Soler J. Diagnosis and management of pericardial effusion. World J Cardiol. 2011; 3(5): 135-143.
[10]
Matta A, Elenizi K, AlHarthi R, et al. A Rare Case of Candida Pericarditis Associated with Esophagopericardial Fistula. Am J Case Rep. 2019; 20: 1031-1035.
[2, 4, 10]
. The single-drain strategy lowered the chance of infection while still letting drainage happen. The drain was taken out on day 6, which was also the day that the effusion went away
[2]
Imazio M, Adler Y, Charron P, et al. Management of pericardial diseases: a position statement of the European Society of Cardiology. Eur Heart J. 2020; 41(7): 1554-1560.
[8]
Azhar A. Successful management of fungal pericarditis and endocarditis in a neonate: A case report. J Exp Integr Med. 2012; 2(4): 357-360.
[2, 8]
. The Infectious Diseases Society of America says that C. glabrata's susceptibility to fluconazole varies, so the choice of antifungal drugs started with amphotericin B for broad coverage and then switched to voriconazole
[3]
Pappas PG, Kauffman CA, Andes DR, Clancy CJ, Marr KA, Ostrosky-Zeichner L, et al. Clinical practice guideline for the management of candidiasis: 2016 update by the Infectious Diseases Society of America. Clin Infect Dis. 2016; 62(4): e1-e50.
[11]
Neughebauer B, Alvarez V, Harb T, Keefer M. Constrictive pericarditis caused by Candida glabrata in an immunocompetent patient. Scand J Infect Dis. 2002; 34(8): 615-619.
[15]
Khillan V, Rathore N, Kathuria S, Chowdhary A. A rare case of breakthrough fungal pericarditis due to fluconazole-resistant Candida auris. JMM Case Rep. 2014; 1(3): e003005.
[3, 11, 15]
. Inotropes and transfusions were helpful in getting the heart to its lowest point. The time spent in the NICU also allowed for close monitoring for arrhythmias or reaccumulation
[2]
Imazio M, Adler Y, Charron P, et al. Management of pericardial diseases: a position statement of the European Society of Cardiology. Eur Heart J. 2020; 41(7): 1554-1560.
[13]
Bollempalli H, et al. A Rare Case Of Cardiomyopathy With Diamond-Blackfan Anemia? J Am Coll Cardiol. 2024; 83(13_Supplement): 2303.
[2, 13]
.
The results depend on how soon the treatment is given: Delayed fungal pericarditis has a mortality rate exceeding 50%; however, this child's complete recovery and discharge in 19 days demonstrate the efficacy of the treatment
[6]
Jancic P, Milutinovic S, Ward M, Radovanovic M, Jovanovic N, Antic M, et al. Fungal Pericarditis—A Systematic Review of 101 Cases. Microorganisms. 2025; 13(4): 707.
[9]
Sung J, Perez IE, Feinstein A, Stein DK. A case report of purulent pericarditis caused by Candida albicans. Medicine (Baltimore). 2018; 97(28): e11286.
[6, 9]
. Because DBA can cause long-term problems like cancer (like acute myeloid leukaemia) and blood transfusion problems (like hemochromatosis), follow-up care needs to involve more than one field
[1]
Da Costa L, Narla A, Mohandas N. Diamond-Blackfan anemia: etiology, pathophysiology, and treatment. Blood Rev. 2018; 32(5): 413-424.
[5]
Vlachos A, Osorio DS, Atsidaftos E, Kang J, Lababidi ML, Seiden HS, Gruber D, Glader BE, Onel K, Farrar JE, Bodine DM, Aspesi A, Dianzani I, Ramenghi U, Ellis SR, Lipton JM. Increased Prevalence of Congenital Heart Disease in Children With Diamond Blackfan Anemia. Circ Genom Precis Med. 2018; 11(5): e002044.
[1, 5]
. Genetic testing could find mutations like RPS19 that could help with targeted treatments like gene editing or eltrombopag
[1]
Da Costa L, Narla A, Mohandas N. Diamond-Blackfan anemia: etiology, pathophysiology, and treatment. Blood Rev. 2018; 32(5): 413-424.
[5]
Vlachos A, Osorio DS, Atsidaftos E, Kang J, Lababidi ML, Seiden HS, Gruber D, Glader BE, Onel K, Farrar JE, Bodine DM, Aspesi A, Dianzani I, Ramenghi U, Ellis SR, Lipton JM. Increased Prevalence of Congenital Heart Disease in Children With Diamond Blackfan Anemia. Circ Genom Precis Med. 2018; 11(5): e002044.
[1, 5]
. This story says that people with febrile DBA should get echocardiograms on a regular basis and that antifungals should be given as a precaution in high-risk situations to avoid such sieges
[2]
Imazio M, Adler Y, Charron P, et al. Management of pericardial diseases: a position statement of the European Society of Cardiology. Eur Heart J. 2020; 41(7): 1554-1560.
[3]
Pappas PG, Kauffman CA, Andes DR, Clancy CJ, Marr KA, Ostrosky-Zeichner L, et al. Clinical practice guideline for the management of candidiasis: 2016 update by the Infectious Diseases Society of America. Clin Infect Dis. 2016; 62(4): e1-e50.
[12]
Moisa SM, Spoiala EL, Trandafir LM, Butnariu LI, Miron IC, Ciobanu A, Mocanu A, Ivanov A, Ciongradi CI, Sarbu I, Ciubara A, Rusu CD, Luca AC, Burlacu A. Unusual Association of Diamond–Blackfan Anemia and Severe Sinus Bradycardia. Cureus. 2023; 15(2): e34736.
[2, 3, 12]
.
In Punjab's farming context, things get worse when people have to wait for care. This shows the need for telemedicine and subsidised diagnostics
[7]
Dahl C, Johansen HK, Kjaeldgaard P, Helweg-Larsen J. A paediatric case of Candida pericarditis and oesophagus stricture during treatment for acute lymphatic leukaemia. Acta Oncol. 2007; 46(3): 397-399.
[7]
. This has a bigger effect on health around the world. A 2018 Paediatric Cardiology series on 12 pyopericardium cases indicates that fungi are the aetiology in fewer than 10% of instances, with DBA being even rarer. This report adds to what we already know
[6]
Jancic P, Milutinovic S, Ward M, Radovanovic M, Jovanovic N, Antic M, et al. Fungal Pericarditis—A Systematic Review of 101 Cases. Microorganisms. 2025; 13(4): 707.
[13]
Bollempalli H, et al. A Rare Case Of Cardiomyopathy With Diamond-Blackfan Anemia? J Am Coll Cardiol. 2024; 83(13_Supplement): 2303.
[6, 13]
.
4. Conclusion
In surmounting fungal pyopericardium's assault amid Diamond-Blackfan anemia, this case epitomizes resilience forged through astute recognition and integrated care. From fever's subtle harbinger to cardiac precipice, the trajectory underscores infectious vigilance's paramountcy in congenital anemias. Clinicians must heed such lessons, championing proactive strategies to shield vulnerable hearts from similar encroachments.
Da Costa L, Narla A, Mohandas N. Diamond-Blackfan anemia: etiology, pathophysiology, and treatment. Blood Rev. 2018; 32(5): 413-424.
[2]
Imazio M, Adler Y, Charron P, et al. Management of pericardial diseases: a position statement of the European Society of Cardiology. Eur Heart J. 2020; 41(7): 1554-1560.
[3]
Pappas PG, Kauffman CA, Andes DR, Clancy CJ, Marr KA, Ostrosky-Zeichner L, et al. Clinical practice guideline for the management of candidiasis: 2016 update by the Infectious Diseases Society of America. Clin Infect Dis. 2016; 62(4): e1-e50.
[4]
Sagristà-Sauleda J, Mercé AS, Soler-Soler J. Diagnosis and management of pericardial effusion. World J Cardiol. 2011; 3(5): 135-143.
[5]
Vlachos A, Osorio DS, Atsidaftos E, Kang J, Lababidi ML, Seiden HS, Gruber D, Glader BE, Onel K, Farrar JE, Bodine DM, Aspesi A, Dianzani I, Ramenghi U, Ellis SR, Lipton JM. Increased Prevalence of Congenital Heart Disease in Children With Diamond Blackfan Anemia. Circ Genom Precis Med. 2018; 11(5): e002044.
[6]
Jancic P, Milutinovic S, Ward M, Radovanovic M, Jovanovic N, Antic M, et al. Fungal Pericarditis—A Systematic Review of 101 Cases. Microorganisms. 2025; 13(4): 707.
[7]
Dahl C, Johansen HK, Kjaeldgaard P, Helweg-Larsen J. A paediatric case of Candida pericarditis and oesophagus stricture during treatment for acute lymphatic leukaemia. Acta Oncol. 2007; 46(3): 397-399.
[8]
Azhar A. Successful management of fungal pericarditis and endocarditis in a neonate: A case report. J Exp Integr Med. 2012; 2(4): 357-360.
[9]
Sung J, Perez IE, Feinstein A, Stein DK. A case report of purulent pericarditis caused by Candida albicans. Medicine (Baltimore). 2018; 97(28): e11286.
[10]
Matta A, Elenizi K, AlHarthi R, et al. A Rare Case of Candida Pericarditis Associated with Esophagopericardial Fistula. Am J Case Rep. 2019; 20: 1031-1035.
[11]
Neughebauer B, Alvarez V, Harb T, Keefer M. Constrictive pericarditis caused by Candida glabrata in an immunocompetent patient. Scand J Infect Dis. 2002; 34(8): 615-619.
[12]
Moisa SM, Spoiala EL, Trandafir LM, Butnariu LI, Miron IC, Ciobanu A, Mocanu A, Ivanov A, Ciongradi CI, Sarbu I, Ciubara A, Rusu CD, Luca AC, Burlacu A. Unusual Association of Diamond–Blackfan Anemia and Severe Sinus Bradycardia. Cureus. 2023; 15(2): e34736.
[13]
Bollempalli H, et al. A Rare Case Of Cardiomyopathy With Diamond-Blackfan Anemia? J Am Coll Cardiol. 2024; 83(13_Supplement): 2303.
[14]
Jette N, Gebhardt C, Coustinos D. Case report: cardiac tamponade secondary to candida pericarditis. J Surg Case Rep. 2024; 2024(3): rjae150.
[15]
Khillan V, Rathore N, Kathuria S, Chowdhary A. A rare case of breakthrough fungal pericarditis due to fluconazole-resistant Candida auris. JMM Case Rep. 2014; 1(3): e003005.
Satpathy, A. S., Pavan, M., Pramanik, B., Sangdup, T. (2026). A Rare Case of Fungal Pyopericardium with Myocardial Dysfunction in a Child with Diamond-Blackfan Anemia. International Journal of Cardiovascular and Thoracic Surgery, 12(2), 80-84. https://doi.org/10.11648/j.ijcts.20261202.20
Satpathy, A. S.; Pavan, M.; Pramanik, B.; Sangdup, T. A Rare Case of Fungal Pyopericardium with Myocardial Dysfunction in a Child with Diamond-Blackfan Anemia. Int. J. Cardiovasc. Thorac. Surg.2026, 12(2), 80-84. doi: 10.11648/j.ijcts.20261202.20
Satpathy AS, Pavan M, Pramanik B, Sangdup T. A Rare Case of Fungal Pyopericardium with Myocardial Dysfunction in a Child with Diamond-Blackfan Anemia. Int J Cardiovasc Thorac Surg. 2026;12(2):80-84. doi: 10.11648/j.ijcts.20261202.20
@article{10.11648/j.ijcts.20261202.20,
author = {Abhishek Soham Satpathy and Mallikarjuna Pavan and Biswarup Pramanik and Tsering Sangdup},
title = {A Rare Case of Fungal Pyopericardium with Myocardial Dysfunction in a Child with Diamond-Blackfan Anemia},
journal = {International Journal of Cardiovascular and Thoracic Surgery},
volume = {12},
number = {2},
pages = {80-84},
doi = {10.11648/j.ijcts.20261202.20},
url = {https://doi.org/10.11648/j.ijcts.20261202.20},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcts.20261202.20},
abstract = {Pyopericardium is an uncommon yet potentially fatal paediatric emergency, typically of bacterial origin, but increasingly linked to opportunistic fungal pathogens in immunocompromised individuals. This report delineates the clinical progression of a 2-year-old female with transfusion-dependent Diamond-Blackfan Anaemia (DBA), who exhibited a one-month history of insidious fever, ultimately leading to acute cardiac tamponade. When the patient was admitted to the hospital in an emergency, they had low blood pressure (80/50 mmHg), muffled heart sounds, and severe breathing problems. Laboratory tests showed very low levels of haemoglobin (5.2 g/dL) and very high levls of inflammatory markers. An echocardiogram showed a huge pericardial effusion with right ventricular diastolic collapse and a reduced ejection fraction of 40%. Emergent pericardiocentesis produced 150 mL of purulent fluid, with cultures identifying Candida glabrata as the etiological agent. Management required a multi-faceted approach that included an emergent subxiphoid partial pericardiectomy, inotropic support, and blood transfusions. Antifungal treatment started with liposomal amphotericin B and was successfully switched to oral voriconazole after confirming that the patient was susceptible. Before being discharged on hospital day 19, the patient's heart function had improved so much that their ejection fraction was back to normal at 55%. This case shows how hard it is to diagnose fungal pyopericardium in people with congenital bone marrow failure syndromes. It also shows how important it is to do echocardiographic screening early and use aggressive surgical-pharmacological synergy to lower the high death rates that come with a late diagnosis.},
year = {2026}
}
TY - JOUR
T1 - A Rare Case of Fungal Pyopericardium with Myocardial Dysfunction in a Child with Diamond-Blackfan Anemia
AU - Abhishek Soham Satpathy
AU - Mallikarjuna Pavan
AU - Biswarup Pramanik
AU - Tsering Sangdup
Y1 - 2026/04/15
PY - 2026
N1 - https://doi.org/10.11648/j.ijcts.20261202.20
DO - 10.11648/j.ijcts.20261202.20
T2 - International Journal of Cardiovascular and Thoracic Surgery
JF - International Journal of Cardiovascular and Thoracic Surgery
JO - International Journal of Cardiovascular and Thoracic Surgery
SP - 80
EP - 84
PB - Science Publishing Group
SN - 2575-4882
UR - https://doi.org/10.11648/j.ijcts.20261202.20
AB - Pyopericardium is an uncommon yet potentially fatal paediatric emergency, typically of bacterial origin, but increasingly linked to opportunistic fungal pathogens in immunocompromised individuals. This report delineates the clinical progression of a 2-year-old female with transfusion-dependent Diamond-Blackfan Anaemia (DBA), who exhibited a one-month history of insidious fever, ultimately leading to acute cardiac tamponade. When the patient was admitted to the hospital in an emergency, they had low blood pressure (80/50 mmHg), muffled heart sounds, and severe breathing problems. Laboratory tests showed very low levels of haemoglobin (5.2 g/dL) and very high levls of inflammatory markers. An echocardiogram showed a huge pericardial effusion with right ventricular diastolic collapse and a reduced ejection fraction of 40%. Emergent pericardiocentesis produced 150 mL of purulent fluid, with cultures identifying Candida glabrata as the etiological agent. Management required a multi-faceted approach that included an emergent subxiphoid partial pericardiectomy, inotropic support, and blood transfusions. Antifungal treatment started with liposomal amphotericin B and was successfully switched to oral voriconazole after confirming that the patient was susceptible. Before being discharged on hospital day 19, the patient's heart function had improved so much that their ejection fraction was back to normal at 55%. This case shows how hard it is to diagnose fungal pyopericardium in people with congenital bone marrow failure syndromes. It also shows how important it is to do echocardiographic screening early and use aggressive surgical-pharmacological synergy to lower the high death rates that come with a late diagnosis.
VL - 12
IS - 2
ER -
Satpathy, A. S., Pavan, M., Pramanik, B., Sangdup, T. (2026). A Rare Case of Fungal Pyopericardium with Myocardial Dysfunction in a Child with Diamond-Blackfan Anemia. International Journal of Cardiovascular and Thoracic Surgery, 12(2), 80-84. https://doi.org/10.11648/j.ijcts.20261202.20
Satpathy, A. S.; Pavan, M.; Pramanik, B.; Sangdup, T. A Rare Case of Fungal Pyopericardium with Myocardial Dysfunction in a Child with Diamond-Blackfan Anemia. Int. J. Cardiovasc. Thorac. Surg.2026, 12(2), 80-84. doi: 10.11648/j.ijcts.20261202.20
Satpathy AS, Pavan M, Pramanik B, Sangdup T. A Rare Case of Fungal Pyopericardium with Myocardial Dysfunction in a Child with Diamond-Blackfan Anemia. Int J Cardiovasc Thorac Surg. 2026;12(2):80-84. doi: 10.11648/j.ijcts.20261202.20
@article{10.11648/j.ijcts.20261202.20,
author = {Abhishek Soham Satpathy and Mallikarjuna Pavan and Biswarup Pramanik and Tsering Sangdup},
title = {A Rare Case of Fungal Pyopericardium with Myocardial Dysfunction in a Child with Diamond-Blackfan Anemia},
journal = {International Journal of Cardiovascular and Thoracic Surgery},
volume = {12},
number = {2},
pages = {80-84},
doi = {10.11648/j.ijcts.20261202.20},
url = {https://doi.org/10.11648/j.ijcts.20261202.20},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcts.20261202.20},
abstract = {Pyopericardium is an uncommon yet potentially fatal paediatric emergency, typically of bacterial origin, but increasingly linked to opportunistic fungal pathogens in immunocompromised individuals. This report delineates the clinical progression of a 2-year-old female with transfusion-dependent Diamond-Blackfan Anaemia (DBA), who exhibited a one-month history of insidious fever, ultimately leading to acute cardiac tamponade. When the patient was admitted to the hospital in an emergency, they had low blood pressure (80/50 mmHg), muffled heart sounds, and severe breathing problems. Laboratory tests showed very low levels of haemoglobin (5.2 g/dL) and very high levls of inflammatory markers. An echocardiogram showed a huge pericardial effusion with right ventricular diastolic collapse and a reduced ejection fraction of 40%. Emergent pericardiocentesis produced 150 mL of purulent fluid, with cultures identifying Candida glabrata as the etiological agent. Management required a multi-faceted approach that included an emergent subxiphoid partial pericardiectomy, inotropic support, and blood transfusions. Antifungal treatment started with liposomal amphotericin B and was successfully switched to oral voriconazole after confirming that the patient was susceptible. Before being discharged on hospital day 19, the patient's heart function had improved so much that their ejection fraction was back to normal at 55%. This case shows how hard it is to diagnose fungal pyopericardium in people with congenital bone marrow failure syndromes. It also shows how important it is to do echocardiographic screening early and use aggressive surgical-pharmacological synergy to lower the high death rates that come with a late diagnosis.},
year = {2026}
}
TY - JOUR
T1 - A Rare Case of Fungal Pyopericardium with Myocardial Dysfunction in a Child with Diamond-Blackfan Anemia
AU - Abhishek Soham Satpathy
AU - Mallikarjuna Pavan
AU - Biswarup Pramanik
AU - Tsering Sangdup
Y1 - 2026/04/15
PY - 2026
N1 - https://doi.org/10.11648/j.ijcts.20261202.20
DO - 10.11648/j.ijcts.20261202.20
T2 - International Journal of Cardiovascular and Thoracic Surgery
JF - International Journal of Cardiovascular and Thoracic Surgery
JO - International Journal of Cardiovascular and Thoracic Surgery
SP - 80
EP - 84
PB - Science Publishing Group
SN - 2575-4882
UR - https://doi.org/10.11648/j.ijcts.20261202.20
AB - Pyopericardium is an uncommon yet potentially fatal paediatric emergency, typically of bacterial origin, but increasingly linked to opportunistic fungal pathogens in immunocompromised individuals. This report delineates the clinical progression of a 2-year-old female with transfusion-dependent Diamond-Blackfan Anaemia (DBA), who exhibited a one-month history of insidious fever, ultimately leading to acute cardiac tamponade. When the patient was admitted to the hospital in an emergency, they had low blood pressure (80/50 mmHg), muffled heart sounds, and severe breathing problems. Laboratory tests showed very low levels of haemoglobin (5.2 g/dL) and very high levls of inflammatory markers. An echocardiogram showed a huge pericardial effusion with right ventricular diastolic collapse and a reduced ejection fraction of 40%. Emergent pericardiocentesis produced 150 mL of purulent fluid, with cultures identifying Candida glabrata as the etiological agent. Management required a multi-faceted approach that included an emergent subxiphoid partial pericardiectomy, inotropic support, and blood transfusions. Antifungal treatment started with liposomal amphotericin B and was successfully switched to oral voriconazole after confirming that the patient was susceptible. Before being discharged on hospital day 19, the patient's heart function had improved so much that their ejection fraction was back to normal at 55%. This case shows how hard it is to diagnose fungal pyopericardium in people with congenital bone marrow failure syndromes. It also shows how important it is to do echocardiographic screening early and use aggressive surgical-pharmacological synergy to lower the high death rates that come with a late diagnosis.
VL - 12
IS - 2
ER -