Castleman disease is a rare histopathological entity associated with a variety of lymphoproliferative disorders and autoimmune conditions. The disease can occur in a unicentric form (involving single lymph node group) or multicentric form. While sometimes associated with POEMS syndrome, ascites is not an uncommon association with these disorders. However, the ascites described in association with Castleman disease or POEMS is usually a low SAAG ascites. We report a case with high SAAG ascites as the presenting feature in a patient with POEMS syndrome and multicentric Castleman disease which is quite rare as evidenced by scarcity of literature. Our patient who had presented with ascites, was found to have polyneuropathy, organomegaly (liver and spleen), endocrinopathy (thyroid hormone abnormality), monoclonal gammopathy and skin lesions on evaluation. The scenario was complicated due to a misdiagnosis of tuberculosis from elsewhere and an improper course of antituberculosis treatment. Things fell into place when the diagnosis was confirmed with the histopathological examination of the cervical lymph node biopsy showing hyaline vascular variant of Castleman disease. Thalidomide and its congeners along with steroids have been the mainstay of treatment of this along with stem cell transplantation, while anti IL-6 agents like siltuximab are emerging treatment options. In view of its complexity and the multisystem involvement of this syndrome, it may be easily overlooked or missed if one is not aware or actively looking for the various clinical clues.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
High SAAG Ascites, POEMS Syndrome, Castleman Disease
1. History
53 years old man from a district in north Kerala (a state in India), presented with abdominal pain for 7 months which was generalized, aching pain associated with vomiting. The pain was of moderate intensity and persistent. Vomitus contained recently ingested food and there was no blood or bile staining. The patient was evaluated for the same from nearby hospital, an imaging study CECT was done and he was then started on antituberculosis treatment based on the imaging. There was an initial mild improvement in abdominal pain and vomiting. But within 1 month of treatment, he developed loose stools and there was recurrence of vomiting. There was associated anorexia also. Patient remembers his Bilirubin level was 6.5 at that time. Tuberculosis medications were temporarily stopped and a month later, modified tuberculosis treatment was restarted (Levofloxacin and Ethambutol) from a nearby hospital. Streptomycin was also advised after auditory testing but patient did not follow up, though he kept continuing Levofloxacin and Ethambutol. During the same time, he noticed progressive generalized abdominal distention. One month later, patient was started on Rifampicin (300 mg) and Isoniazid (100 mg) from the same hospital which he was continuing until he visited our hospital.
He presented to the Gastroenterology Department of our hospital, with abdominal distention for 4 months, yellowish discolouration of urine and eyes for 4 months. Bystander had also noted that he was losing weight and had loss of appetite. He also complained of numbness of upper and lower extremities.
2. Physical Examination
On examination, patient was conscious and oriented, moderately built and emaciated. His BMI was 16.24 kg/m2. BP 120/80 mm Hg, Pulse rate 80 per minute. Patient had no pallor or icterus. He had grade 2 clubbing and there was bilateral cervical lymph node enlargement -levels IIB, III and IV A-firm, discrete and movable, largest 2 x 2 cm. Patient also had bilateral pitting pedal edema.
Head to foot examination revealed, hyperpigmentation, hypertrichosis, and multiple papulonodular skin lesions over trunk.
His gastrointestinal examination was remarkable for tense ascites. His neurological examination was unremarkable. Other systems were within normal limits.
With a background history of suboptimal treatment of tuberculosis, our first differential was tuberculosis. With the prominent lymph node enlargement, lymphoma was another possibility. An underlying liver disease had to be ruled out too.
With these considerations, we investigated the patient further. His HIV, HBsAg and Anti HCV were negative. Chest Xray and ECG were normal. Mantoux and IGRA were negative and peripheral smear showed a normocytic, normochromic blood picture. His LDH was 174 and CEA was negative. His TSH was 12, and free T4 was low.
We then proceeded with an ascitic fluid analysis which showed a total count of 88 cells with a lymphocyte predominance. His ascitic fluid protein was 2.8 g with a SAAG of 1.6. ADA was 19, the triglyceride levels in the ascitic fluid was 25 and cytological analysis of the fluid failed to show any malignant cells. Thus, our patient had a high SAAG high protein ascites. Hence, we proceeded with an Ultrasound of the abdomen with splenoportal axis Doppler scan which showed normal IVC and hepatic veins, normal size and echoes of the liver and a spleen size of 15 cm. We also sought a cardiology opinion and Echocardiography -the same was normal A CECT abdomen confirmed these findings and also showed aorto caval and paraaortic nodes. We then did an Upper and lower GI endoscopy which was unremarkable.
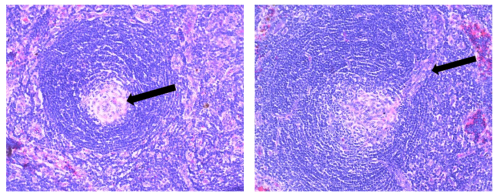
We then proceeded with a lymph node biopsy. The biopsy report clinched the diagnosis. There was “twinning” of germinal centre and “lollipop” appearance suggestive of a hyaline variant of Castleman disease. We then proceeded with HHV-8 serology, which was negative and then did serum protein electrophoresis which showed a prominent M band in the A and lambda region.
Thus, our patient had multicentric castleman disease along with sensory symptoms, organomegaly, sensory symptoms, skin lesions, M band and hypothyroidism completing the criteria for an associated POEMS syndrome.
Figure 3. Histopathological examination of lymph node biopsy showing twinning of germinal centre and lollipop appearance.
4. Discussion
Catleman disease, also called angiofollicular lymph node hyperplasia is a rare, heterogenous group of lymphoproliferative disorders with shared histopathological findings. Castleman disease can broadly be unicentric, when it involves a single lymph node group or multicentric when multiple lymph node groups are involved
[1]
Liu AY, Nabel CS, Finkelman BS, Ruth JR, Kurzrock R, van Rhee F, et al. Idiopathic multicentric Castleman’s disease: a systematic literature review. Lancet Haematol. 2016 Apr; 3(4): e163-175.
. They usually present with enlarged liver and spleen, lymph node enlargement and B symptoms.
The disease is categorized as- unicentric form (UCD), HHV8 associated multicentric Castleman disease (HHV8 associated MCD), POEMS associated MCD and idiopathic multicentric form (iMCD) which is not associated with HHV 8. iMCD can be further classified into iMCD-TAFRO and iMCD not otherwise specified (iMCD-NOS). iMCD may be associated with a wide variety of autoimmune as well as auto inflammatory disease
[3]
Idiopathic multicentric Castleman disease and associated autoimmune and autoinflammatory conditions: practical guidance for diagnosis - PubMed. [cited 2026 Feb 25]. Available from:
Multicentric Castleman disease is known to be associated with POEMS syndrome in about one third of cases. In one study, POEMS was associated with Castleman disease in 11% of cases
[3]
Idiopathic multicentric Castleman disease and associated autoimmune and autoinflammatory conditions: practical guidance for diagnosis - PubMed. [cited 2026 Feb 25]. Available from:
. POEMS syndrome is a rare plasma cell disorder (POEMS being acronym for Polyneuropathy, Organomegaly. Endocrinopathy, Monoclonal gammopathy and Skin changes).
POEMS syndrome is diagnosed using a set of criteria:
[4]
Dispenzieri A, Kyle RA, Lacy MQ, Rajkumar SV, Therneau TM, Larson DR, et al. POEMS syndrome: definitions and long-term outcome. Blood. 2003 Apr 1; 101(7): 2496–506.
Mandatory major criteria: Polyradiculoneuropathy, Monoclonal plasma cell disorder
Other major criteria: Castleman disease, Sclerotic bone lesions, Elevated VEGF
Minor criteria: Organomegaly, Extravascular volume overload, Endocrinopathy, Skin changes, Papilledema, Thrombocytosis or polycythemia
Here we present a case of idiopathic MCD associated with POEMS syndrome which presented with a high SAAG, high protein ascites. Literature reports various presentations of POEMS associated with Castleman syndrome. Congcong Min etal reports a case presenting with polyserositis and renal impairment
[6]
A case report of Castleman disease variant of POEMS syndrome presenting with prominent polyserositis and renal impairment - PMC. [cited 2026 Feb 25]. Available from:
Lee etal reports a case that presented with inguinal lymphadenopathy
[7]
Lee YM, Choi YS, Kim JM. POEMS Syndrome: Presented as Idiopathic Multicentric Castleman Disease of Plasma Cell Variant for Eight Years and Dramatic Treatment with Siltuximab Followed by Autologous Peripheral Blood Stem Cell Transplantation. Diagnostics (Basel). 2022 Apr 15; 12(4): 998.
Hang Yu etal describes the case of a 24 years old male with this syndrome who also had multiple cerebral infarctions
[8]
Castleman disease variant of POEMS syndrome complicated with multiple cerebral infarction: a rare case report and review of literature - PMC. [cited 2026 Feb 25]. Available from:
Extravascular volume overload has been described in about 29% of patients with POEMS syndrome with ascites seen in about 7%.
[3]
Idiopathic multicentric Castleman disease and associated autoimmune and autoinflammatory conditions: practical guidance for diagnosis - PubMed. [cited 2026 Feb 25]. Available from:
involving 106 POEMS patients, ascites was seen in 42 (39.6%) of patients. Of these, 31 patients underwent ascitic fluid study, all had low SAAG ascites. A few case reports describing ascites as the presenting feature are available for both POEMS syndrome
[9]
The characteristics of ascites in patients with POEMS syndrome - PubMed. [cited 2023 Apr 26]. Available from:
Frontiers | Refractory ascites: unveiling POEMS syndrome as the underlying cause: a case report and literature review. [cited 2026 Feb 25]. Available from:
SciELO - Brazil - Ascites as a presenting sign of multicentric mixed-type Castleman disease variant of POEMS syndrome Ascites as a presenting sign of multicentric mixed-type Castleman disease variant of POEMS syndrome. [cited 2023 Apr 27]. Available from:
Al-Mayoof O, Sughaiyer HA, Abuomar W, Khan M. POEMS syndrome: a rare cause of exudative ascites and chronic peripheral neuropathy. Case Reports. 2017 Jun 21; 2017: bcr.
as well as multicentric Castleman disease, with the type of ascites being low SAAG ascites again. A case report by Lina Wu etal
[14]
Wu L, Li Y, Yao F, Lu C, Li J, Zhou W, et al. Portal hypertension as the initial manifestation of POEMS syndrome: a case report. BMC Hematol. 2017 May 11; 17: 9.
describes a patient with POEMS syndrome who presented with features of idiopathic portal hypertension. Their patient also had Castleman disease similar to our case. His portal hypertension was successfully treated with dexamethasone and lenalidomide. Mechanisms for the development of portal hypertension descibed are progressive fibrosis of the portal veins and VEGF induced microvascular changes.
Our patient had a high SAAG high protein ascites without features of liver cirrhosis. He had skin changes suggestive of POEMS- hyperpigmentation, hypertrichosis and multiple glomerular hemangiomas. He was also newly detected to have hypothyroidism and was started on thyroxine supplementation. There was splenomegaly and lymph node enlargement and a monoclonal plasma cell disorder suggested by an M band in the IgA and lambda region all fitting into the classical description of POEMS syndrome. Our patient was started on steroids and lenalidomide and is on follow up. Emerging treatments for the condition include IL -6 inhibitors, considering its pivotal role in the disease pathology. Lee etal in his case report describes successful treatment with Siltuximab (monoclonal antibody against IL 6) followed by autologous peripheral blood stem cell transplantation
[7]
Lee YM, Choi YS, Kim JM. POEMS Syndrome: Presented as Idiopathic Multicentric Castleman Disease of Plasma Cell Variant for Eight Years and Dramatic Treatment with Siltuximab Followed by Autologous Peripheral Blood Stem Cell Transplantation. Diagnostics (Basel). 2022 Apr 15; 12(4): 998.
Previously, the long term prognosis for patients with POEMS syndrome was generally poor (median survival being about 12-33 months
[3]
Idiopathic multicentric Castleman disease and associated autoimmune and autoinflammatory conditions: practical guidance for diagnosis - PubMed. [cited 2026 Feb 25]. Available from:
Idiopathic multicentric Castleman disease and associated autoimmune and autoinflammatory conditions: practical guidance for diagnosis - PubMed. [cited 2026 Feb 25]. Available from:
A case report of Castleman disease variant of POEMS syndrome presenting with prominent polyserositis and renal impairment - PMC. [cited 2026 Feb 25]. Available from:
Lee YM, Choi YS, Kim JM. POEMS Syndrome: Presented as Idiopathic Multicentric Castleman Disease of Plasma Cell Variant for Eight Years and Dramatic Treatment with Siltuximab Followed by Autologous Peripheral Blood Stem Cell Transplantation. Diagnostics (Basel). 2022 Apr 15; 12(4): 998.
Castleman disease variant of POEMS syndrome complicated with multiple cerebral infarction: a rare case report and review of literature - PMC. [cited 2026 Feb 25]. Available from:
Frontiers | Refractory ascites: unveiling POEMS syndrome as the underlying cause: a case report and literature review. [cited 2026 Feb 25]. Available from:
SciELO - Brazil - Ascites as a presenting sign of multicentric mixed-type Castleman disease variant of POEMS syndrome Ascites as a presenting sign of multicentric mixed-type Castleman disease variant of POEMS syndrome. [cited 2023 Apr 27]. Available from:
Al-Mayoof O, Sughaiyer HA, Abuomar W, Khan M. POEMS syndrome: a rare cause of exudative ascites and chronic peripheral neuropathy. Case Reports. 2017 Jun 21; 2017: bcr.
Wu L, Li Y, Yao F, Lu C, Li J, Zhou W, et al. Portal hypertension as the initial manifestation of POEMS syndrome: a case report. BMC Hematol. 2017 May 11; 17: 9.
Veetil, R. P., Balagopal, S. K., Kandiyil, S. K. (2026). An Unusual Case of Ascites: Multicentric Castleman Disease Associated with Poems Syndrome Presenting as High Saag Ascites. International Journal of Gastroenterology, 10(1), 5-8. https://doi.org/10.11648/j.ijg.20261001.12
Veetil, R. P.; Balagopal, S. K.; Kandiyil, S. K. An Unusual Case of Ascites: Multicentric Castleman Disease Associated with Poems Syndrome Presenting as High Saag Ascites. Int. J. Gastroenterol.2026, 10(1), 5-8. doi: 10.11648/j.ijg.20261001.12
Veetil RP, Balagopal SK, Kandiyil SK. An Unusual Case of Ascites: Multicentric Castleman Disease Associated with Poems Syndrome Presenting as High Saag Ascites. Int J Gastroenterol. 2026;10(1):5-8. doi: 10.11648/j.ijg.20261001.12
@article{10.11648/j.ijg.20261001.12,
author = {Remya Puthiya Veetil and Sithara Kodapally Balagopal and Sunil Kumar Kandiyil},
title = {An Unusual Case of Ascites: Multicentric Castleman Disease Associated with Poems Syndrome Presenting as High Saag Ascites},
journal = {International Journal of Gastroenterology},
volume = {10},
number = {1},
pages = {5-8},
doi = {10.11648/j.ijg.20261001.12},
url = {https://doi.org/10.11648/j.ijg.20261001.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijg.20261001.12},
abstract = {Castleman disease is a rare histopathological entity associated with a variety of lymphoproliferative disorders and autoimmune conditions. The disease can occur in a unicentric form (involving single lymph node group) or multicentric form. While sometimes associated with POEMS syndrome, ascites is not an uncommon association with these disorders. However, the ascites described in association with Castleman disease or POEMS is usually a low SAAG ascites. We report a case with high SAAG ascites as the presenting feature in a patient with POEMS syndrome and multicentric Castleman disease which is quite rare as evidenced by scarcity of literature. Our patient who had presented with ascites, was found to have polyneuropathy, organomegaly (liver and spleen), endocrinopathy (thyroid hormone abnormality), monoclonal gammopathy and skin lesions on evaluation. The scenario was complicated due to a misdiagnosis of tuberculosis from elsewhere and an improper course of antituberculosis treatment. Things fell into place when the diagnosis was confirmed with the histopathological examination of the cervical lymph node biopsy showing hyaline vascular variant of Castleman disease. Thalidomide and its congeners along with steroids have been the mainstay of treatment of this along with stem cell transplantation, while anti IL-6 agents like siltuximab are emerging treatment options. In view of its complexity and the multisystem involvement of this syndrome, it may be easily overlooked or missed if one is not aware or actively looking for the various clinical clues.},
year = {2026}
}
TY - JOUR
T1 - An Unusual Case of Ascites: Multicentric Castleman Disease Associated with Poems Syndrome Presenting as High Saag Ascites
AU - Remya Puthiya Veetil
AU - Sithara Kodapally Balagopal
AU - Sunil Kumar Kandiyil
Y1 - 2026/03/12
PY - 2026
N1 - https://doi.org/10.11648/j.ijg.20261001.12
DO - 10.11648/j.ijg.20261001.12
T2 - International Journal of Gastroenterology
JF - International Journal of Gastroenterology
JO - International Journal of Gastroenterology
SP - 5
EP - 8
PB - Science Publishing Group
SN - 2640-169X
UR - https://doi.org/10.11648/j.ijg.20261001.12
AB - Castleman disease is a rare histopathological entity associated with a variety of lymphoproliferative disorders and autoimmune conditions. The disease can occur in a unicentric form (involving single lymph node group) or multicentric form. While sometimes associated with POEMS syndrome, ascites is not an uncommon association with these disorders. However, the ascites described in association with Castleman disease or POEMS is usually a low SAAG ascites. We report a case with high SAAG ascites as the presenting feature in a patient with POEMS syndrome and multicentric Castleman disease which is quite rare as evidenced by scarcity of literature. Our patient who had presented with ascites, was found to have polyneuropathy, organomegaly (liver and spleen), endocrinopathy (thyroid hormone abnormality), monoclonal gammopathy and skin lesions on evaluation. The scenario was complicated due to a misdiagnosis of tuberculosis from elsewhere and an improper course of antituberculosis treatment. Things fell into place when the diagnosis was confirmed with the histopathological examination of the cervical lymph node biopsy showing hyaline vascular variant of Castleman disease. Thalidomide and its congeners along with steroids have been the mainstay of treatment of this along with stem cell transplantation, while anti IL-6 agents like siltuximab are emerging treatment options. In view of its complexity and the multisystem involvement of this syndrome, it may be easily overlooked or missed if one is not aware or actively looking for the various clinical clues.
VL - 10
IS - 1
ER -
Veetil, R. P., Balagopal, S. K., Kandiyil, S. K. (2026). An Unusual Case of Ascites: Multicentric Castleman Disease Associated with Poems Syndrome Presenting as High Saag Ascites. International Journal of Gastroenterology, 10(1), 5-8. https://doi.org/10.11648/j.ijg.20261001.12
Veetil, R. P.; Balagopal, S. K.; Kandiyil, S. K. An Unusual Case of Ascites: Multicentric Castleman Disease Associated with Poems Syndrome Presenting as High Saag Ascites. Int. J. Gastroenterol.2026, 10(1), 5-8. doi: 10.11648/j.ijg.20261001.12
Veetil RP, Balagopal SK, Kandiyil SK. An Unusual Case of Ascites: Multicentric Castleman Disease Associated with Poems Syndrome Presenting as High Saag Ascites. Int J Gastroenterol. 2026;10(1):5-8. doi: 10.11648/j.ijg.20261001.12
@article{10.11648/j.ijg.20261001.12,
author = {Remya Puthiya Veetil and Sithara Kodapally Balagopal and Sunil Kumar Kandiyil},
title = {An Unusual Case of Ascites: Multicentric Castleman Disease Associated with Poems Syndrome Presenting as High Saag Ascites},
journal = {International Journal of Gastroenterology},
volume = {10},
number = {1},
pages = {5-8},
doi = {10.11648/j.ijg.20261001.12},
url = {https://doi.org/10.11648/j.ijg.20261001.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijg.20261001.12},
abstract = {Castleman disease is a rare histopathological entity associated with a variety of lymphoproliferative disorders and autoimmune conditions. The disease can occur in a unicentric form (involving single lymph node group) or multicentric form. While sometimes associated with POEMS syndrome, ascites is not an uncommon association with these disorders. However, the ascites described in association with Castleman disease or POEMS is usually a low SAAG ascites. We report a case with high SAAG ascites as the presenting feature in a patient with POEMS syndrome and multicentric Castleman disease which is quite rare as evidenced by scarcity of literature. Our patient who had presented with ascites, was found to have polyneuropathy, organomegaly (liver and spleen), endocrinopathy (thyroid hormone abnormality), monoclonal gammopathy and skin lesions on evaluation. The scenario was complicated due to a misdiagnosis of tuberculosis from elsewhere and an improper course of antituberculosis treatment. Things fell into place when the diagnosis was confirmed with the histopathological examination of the cervical lymph node biopsy showing hyaline vascular variant of Castleman disease. Thalidomide and its congeners along with steroids have been the mainstay of treatment of this along with stem cell transplantation, while anti IL-6 agents like siltuximab are emerging treatment options. In view of its complexity and the multisystem involvement of this syndrome, it may be easily overlooked or missed if one is not aware or actively looking for the various clinical clues.},
year = {2026}
}
TY - JOUR
T1 - An Unusual Case of Ascites: Multicentric Castleman Disease Associated with Poems Syndrome Presenting as High Saag Ascites
AU - Remya Puthiya Veetil
AU - Sithara Kodapally Balagopal
AU - Sunil Kumar Kandiyil
Y1 - 2026/03/12
PY - 2026
N1 - https://doi.org/10.11648/j.ijg.20261001.12
DO - 10.11648/j.ijg.20261001.12
T2 - International Journal of Gastroenterology
JF - International Journal of Gastroenterology
JO - International Journal of Gastroenterology
SP - 5
EP - 8
PB - Science Publishing Group
SN - 2640-169X
UR - https://doi.org/10.11648/j.ijg.20261001.12
AB - Castleman disease is a rare histopathological entity associated with a variety of lymphoproliferative disorders and autoimmune conditions. The disease can occur in a unicentric form (involving single lymph node group) or multicentric form. While sometimes associated with POEMS syndrome, ascites is not an uncommon association with these disorders. However, the ascites described in association with Castleman disease or POEMS is usually a low SAAG ascites. We report a case with high SAAG ascites as the presenting feature in a patient with POEMS syndrome and multicentric Castleman disease which is quite rare as evidenced by scarcity of literature. Our patient who had presented with ascites, was found to have polyneuropathy, organomegaly (liver and spleen), endocrinopathy (thyroid hormone abnormality), monoclonal gammopathy and skin lesions on evaluation. The scenario was complicated due to a misdiagnosis of tuberculosis from elsewhere and an improper course of antituberculosis treatment. Things fell into place when the diagnosis was confirmed with the histopathological examination of the cervical lymph node biopsy showing hyaline vascular variant of Castleman disease. Thalidomide and its congeners along with steroids have been the mainstay of treatment of this along with stem cell transplantation, while anti IL-6 agents like siltuximab are emerging treatment options. In view of its complexity and the multisystem involvement of this syndrome, it may be easily overlooked or missed if one is not aware or actively looking for the various clinical clues.
VL - 10
IS - 1
ER -