Abstract
Background: Armed conflict in Sudan has severely disrupted healthcare delivery, and access to diagnostic services. Despite the increasing burden of hematological disorders, data on bone marrow examination (BME) findings in such settings remain limited. This study aimed to characterize the spectrum of BME diagnoses in Sudanese patients during a period of ongoing conflict. Methods: A retrospective cross-sectional study was conducted at Al-Mek Nimer University Hospital, including 291 patients who underwent bone marrow examination (aspiration and trephine biopsy) between April 2023 and February 2025. Data were analyzed using SPSS. Results: Hematological malignancies accounting for 64.6% of cases. Leukemia was the most common diagnosis (38.8%), particularly chronic lymphocytic leukemia (17.2%), acute lymphoblastic leukemia (11.7%), and chronic myeloid leukemia (10.3%). Non-malignant conditions represented 35.4% of cases, mainly reactive marrow changes (17.5%) and megaloblastic anemia (7.2%) being the most frequent. Most patients were aged 41–60 years (29.9%), with a slight male predominance (52.9%). Geographically, most cases originated from River Nile State (52.9%) and Khartoum State (33%). A notable proportion of patients were unemployed (58.8%), suggesting socioeconomic vulnerability. Conclusion: There is high burden of advanced hematological malignancies and reactive marrow patterns likely due to delayed access to care during conflict. Bone marrow examination remains essential diagnostic tool in resource-limited settings. Strengthening mobile diagnostic services, promoting early screening among high-risk groups—particularly the elderly and unemployed—and implementing micronutrient supplementation programs may help reduce morbidity and improve outcomes in conflict-affected populations.
|
Published in
|
Journal of Cancer Treatment and Research (Volume 14, Issue 2)
|
|
DOI
|
10.11648/j.jctr.20261402.11
|
|
Page(s)
|
53-65 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2026. Published by Science Publishing Group
|
Keywords
Bone Marrow Examination, Hematological Malignancies, Reactive Marrow Conflict Settings, Sudan
1. Introduction
Bone marrow located within the inner fixed confines of bone and is the primary hematopoietic organ responsible for the production of the blood cellular elements that perform vital functions of oxygen transport, protection against bacterial and viral pathogens, control of inflammatory responses, and participation in endothelial repair as well as clot formation
| [1] | Islam A. Manual of Bone Marrow Examination. 1sted. Dhaka: Anwer Khan Modern Medical College; 2015. |
[1]
.
Examination of the bone marrow is one of the most valuable diagnostic tests used to evaluate hematological disorders. Bone marrow aspiration and biopsy is also used to stage lymph proliferative disorders and for prognostic purposes in chronic lymph proliferative disorders such as chronic lymphocytic leukemia
| [2] | Okinda NA, Riyat MS. Bone marrow examination findings at AgaKhan University Hospital, Nairobi. East Afr Med J. 2010 Jan; 87(1): 11–17. |
[2]
.
Bone marrow aspiration and biopsy is also useful in the diagnostic workup of fever of unknown origin. It may reveal infections, such as tuberculosis mycobacterium avium-intracellulare infections histoplasmosis, leishmaniasis, and other disseminated fungal infections. It may be useful in establishing the diagnosis of storage diseases and diagnosing metastatic non-haemopoietic malignancies that have spread to the bone marrow when all other imaging and diagnostic modalities have failed or when a leucoerythroblastic peripheral blood picture is present
| [3] | Vergidis D. Bone Marrow Aspiration and Biopsy: Overview. In: Medscape [Internet]. New York: Web MD; [updated 2023 May 17; cited 2025 Jul 3]. |
[3]
.
The importance of bone marrow examination in any hematological disorder cannot be overemphasized. In its absence the investigation of any hematopoietic disorder, unless otherwise well defined, documented and prognostic ally evaluated, is incomplete. Even in many cases where the diagnosis is clinically and pathologically established an examination of the bone marrow remains an integral part of the practice of effective, scientific
| [4] | Bashawri LA. Bonemarrow examination. Indications and diagnostic value. Saudi Med J. 2002; 23(2): 191-196. |
[4]
.
Bone marrow examination (aspiration and/or biopsy) is an essential procedure in clinical hematology, widely indicated for the diagnosis, staging, and monitoring of various systemic and hematologic conditions. Bone marrow examination remains a cornerstone in the diagnostic workup of hematologic and systemic diseases. Its value lies not only in diagnosis but also in prognosis, staging, and monitoring response to therapy.
2. Problem Statement
The burden of hematological disorders is rising in conflict-affected regions; there remains a critical lack of published data on bone marrow examination (BME) findings in Sudan, particularly within the Shendi region. The ongoing armed conflict has significantly disrupted healthcare services, delayed diagnostic evaluations, and may have contributed to late-stage disease presentation among patients evidence-base decisions sand hinders effective national health planning. Consequently, a comprehensive investigation of BME patterns is essential to enhance diagnostic accuracy, support clinical decision-making, and guide targeted humanitarian responses in unstable settings.
3. Justification of the Study
Armed conflict in Sudan has significantly disrupted healthcare systems, leading to delayed diagnosis, limited access to specialized investigations, and worsening outcomes for patients with hematological disorders. Bone marrow examination (BME) remains a cornerstone diagnostic tool for a wide range of malignant and non-malignant hematological conditions. However, there is a scarcity of local data describing the spectrum and frequency of bone marrow findings in Sudan, particularly during periods of instability. Generating such data is essential to understand disease patterns, identify high-risk populations, guide resource allocation, and support the development of targeted diagnostic and therapeutic strategies in resource-limited and conflict-affected settings.
4. Objectives
General Objective
To evaluate the pattern and distribution of bone marrow examination findings among Sudanese patients at Al-Mek Nimer University Hospital during the period April 2023 to February 2025.
Specific Objectives
1) To determine the frequency of hematological malignancies diagnosed by BME.
2) To identify the common types of leukemia and other malignancies.
3) To assess the prevalence of non-malignant bone marrow conditions.
4) To analyze the demographic characteristics (age, gender) of patients undergoing BME.
5) To describe the geographic distribution of cases.
6) To explore the association between socioeconomic status (e.g., employment) and disease patterns.
5. Previous Study
1-Findings in Sudan:
Within Sudan, data on BME patterns is limited but provides essential baseline information. Elmadhoun et al. (2015) conducted a pivotal study in Atbara, North Sudan, reviewing 112 bone marrow aspiration (BMA) cases over six years.
| [5] | Elmadhoun WM, Noor SK, Bushara SO, Almobarak AO, Husain NE, Ahmed MH. Bone marrow aspiration in north Sudan: the procedure, indications and the diagnosticvalue. Int J Health Sci (Qassim). 2015 Oct; 9(4): 434-9.
https://doi.org/10.12816/0031233 |
[5]
The primary indications were pancytopenia (38.4%), unexplained anemia (34.8%), and suspected leukemia (11.6%). Crucially, the diagnostic yield was high (76.8%), with aplastic anemia identified as the most common pathological finding.
| [5] | Elmadhoun WM, Noor SK, Bushara SO, Almobarak AO, Husain NE, Ahmed MH. Bone marrow aspiration in north Sudan: the procedure, indications and the diagnosticvalue. Int J Health Sci (Qassim). 2015 Oct; 9(4): 434-9.
https://doi.org/10.12816/0031233 |
[5]
This study underscores the diagnostic value of BMA in Northern Sudan for evaluating cytopenias and suspected hematological malignancies.
2-Findings in Africa:
Studies across Africa demonstrate consistent patterns in BME indications and diagnoses, often reflecting regional burdens of infectious disease, nutritional deficiencies, and resource constraints:
1-Indications:
Anemia and pancytopenia are consistently dominant reasons for BME across the continent. Studies in Nigeria (recurrent anemia 32.2%, presumptive leukemia 27.7%),
| [6] | Yuguda S, Girei AI, Pindiga KM, Dachi RA, Lawan AI, Abdullahi YM. Indications and Diagnostic Utility of Bone Marrow Aspiration Cytology: A 12-year Experience at a Tertiary Health Center in Gombe, Northeastern Nigeria. Ann Trop Pathol. 2020 Jul- Dec; 11(2): 119-122.
https://doi.org/10.4103/atp.atp_33_19 |
[6]
Kenya (anemia predominant),
| [2] | Okinda NA, Riyat MS. Bone marrow examination findings at AgaKhan University Hospital, Nairobi. East Afr Med J. 2010 Jan; 87(1): 11–17. |
[2]
Malawi
, | [2] | Okinda NA, Riyat MS. Bone marrow examination findings at AgaKhan University Hospital, Nairobi. East Afr Med J. 2010 Jan; 87(1): 11–17. |
[2]
and South Africa (suspected malignancies 67%)
| [7] | Hot A, Jaisson I, Girard C, French M, Durand DV, Rousset H, Ninet J. Yield of bone marrow examination in diagnosing the source of fever of unknown origin. Arch Intern Med. 2009 Nov 23; 169(21): 2018-23
https://doi.org/10.1001/archinternmed.2009.384 |
[7]
confirm this trend. Fever of Unknown Origin (FUO) is another significant indication; Hot et al. (2009) found BME had a 23.7% diagnostic yield in immunocompetent FUO patients, primarily identifying hematological malignancies like lymphoma. Anemia and thrombocytopenia were predictive of a positive yield.
| [7] | Hot A, Jaisson I, Girard C, French M, Durand DV, Rousset H, Ninet J. Yield of bone marrow examination in diagnosing the source of fever of unknown origin. Arch Intern Med. 2009 Nov 23; 169(21): 2018-23
https://doi.org/10.1001/archinternmed.2009.384 |
[7]
2-Diagnostic Findings: Non-Malignant Disorders:
Nutritional deficiencies, particularly megaloblastic anemia and combined deficiencies are highly prevalent. They were the most frequent diagnosesin Northeastern Nigeria (20.3% megaloblastic, 9.9% combined deficiency)
| [8] | Ebrahim H, Fisha T, Debash H, Bisetegn H. Patterns of Bone Marrow Confirmed Malignant and Non-Malignant Hematological Disorders in Patients with Abnormal Hematological Parameters in Northeast Ethiopia. J Blood Med. 2022 Feb 15; 13: 51-60. https://doi.org/10.2147/JBM.S345141 |
[8]
and common findings in Kenya (nutritional anemias, especially megaloblastic).
| [2] | Okinda NA, Riyat MS. Bone marrow examination findings at AgaKhan University Hospital, Nairobi. East Afr Med J. 2010 Jan; 87(1): 11–17. |
[2]
In Northeast Ethiopia, non-malignant disorders (57%) like erythroid hyperplasia, aplastic anemia, and combined deficiency anemias significantly out numbered malignancies.
| [8] | Ebrahim H, Fisha T, Debash H, Bisetegn H. Patterns of Bone Marrow Confirmed Malignant and Non-Malignant Hematological Disorders in Patients with Abnormal Hematological Parameters in Northeast Ethiopia. J Blood Med. 2022 Feb 15; 13: 51-60. https://doi.org/10.2147/JBM.S345141 |
[8]
Reactiveor benign changes constituted 60% of diagnoses in Malawi.
| [9] | Edwards Kasonkanji et al. Quality and Diagnostic Characterization of Bone Marrow Biopsies at Kamuzu Central Hospital, Malawi: A Retrospective Study. JCO Glob Oncol. 2024; 10: 155-156. https://doi.org/10.1200/GO.23.00274 |
[9]
Malignant Disorders:
Leukemia's (Acute Lymphoblastic Leukemia-ALL, Acute Myeloid Leukemia-AML), multiple myeloma (MM), and lymphomas are consistently reported. In South Africa (KwaZulu-Natal), leukemia 20%), MM (13%), and lymphoma (11%) were leading diagnoses.
| [10] | Tshabalala WS, Pillay S, Wilson DPK. Diagnostic outcomes of bone marrow aspirate and trephine biopsies performed at a hospital in KwaZulu-Natal, South Africa. Afr J Lab Med. 2020 Feb 25; 9(1): 1028. https://doi.org/10.4102/ajlm.v9i1.1028 |
[10]
In Kenya (Aga Khan, Nairobi), AML was the most frequent malignant disorder.
| [3] | Vergidis D. Bone Marrow Aspiration and Biopsy: Overview. In: Medscape [Internet]. New York: Web MD; [updated 2023 May 17; cited 2025 Jul 3]. |
[3]
Pediatric studies in Kenya found malignancies (27%), predominantly ALL, in a quarter of examinations.
| [11] | Phillips L, Opie J. The utility of bone marrow sampling in the diagnosis and staging of lymphoma in South Africa. Int J Lab Hematol. 2018 Jun; 40(3): 276-283.
https://doi.org/10.1111/ijlh.12801 |
[11]
South African research confirmed the high utility of BME for detecting bone marrow involvement in lymphoma (43.6% NHL, 35.7% HL).
In Ethiopia, malignancies like CML, AML, CLL, MM, and ALL constituted 11.4% of confirmed hematological disorders.
A Saudi Arabian audit noted acute leukemia as a common diagnosis in patients with pancytopenia undergoing BME.
| [13] | Bashawri LA. An audit- indications and diagnosis of bone marrow biopsies at a tertiary care hospital in Saudi Arabia. Med Crave Online J Hematol Transfus. 2016; 1(1): 1–5.
https://doi.org/10.15406/mojht.2016.01.00005 |
[13]
3-Diagnostic Yield:
BME demonstrates high diagnostic utility across Africa. Yields of 76.8% in Sudan,
| [5] | Elmadhoun WM, Noor SK, Bushara SO, Almobarak AO, Husain NE, Ahmed MH. Bone marrow aspiration in north Sudan: the procedure, indications and the diagnosticvalue. Int J Health Sci (Qassim). 2015 Oct; 9(4): 434-9.
https://doi.org/10.12816/0031233 |
[5]
significant diagnostic information in South Africa,
| [10] | Tshabalala WS, Pillay S, Wilson DPK. Diagnostic outcomes of bone marrow aspirate and trephine biopsies performed at a hospital in KwaZulu-Natal, South Africa. Afr J Lab Med. 2020 Feb 25; 9(1): 1028. https://doi.org/10.4102/ajlm.v9i1.1028 |
[10]
and 23.7% specifically for FUO
| [7] | Hot A, Jaisson I, Girard C, French M, Durand DV, Rousset H, Ninet J. Yield of bone marrow examination in diagnosing the source of fever of unknown origin. Arch Intern Med. 2009 Nov 23; 169(21): 2018-23
https://doi.org/10.1001/archinternmed.2009.384 |
[7]
highlight its value. In Iran, BME had the highest yield for suspected leukemia (54%) and MM (30.3%).
| [2] | Okinda NA, Riyat MS. Bone marrow examination findings at AgaKhan University Hospital, Nairobi. East Afr Med J. 2010 Jan; 87(1): 11–17. |
[2]
3-Global studies:
Global studies reinforce the critical role of BME while highlighting specific diagnostic patterns and challenges:
A-Hematological Malignancies:
Studies confirm BME's indispensability for diagnosing and classifying leukemias, myelodysplastic syndromes, myeloproliferative neoplasms, myelomas, and lymphomas. In Uttarakh and, India, leukemia (58%), MM (24.7%), and lymphoma (14.8%) were the predominant hematological malignancies diagnosed via BME, showing age peaks in adolescents/young adults (11-20 years) and older adults (51-60 years), with a male predominance (2.3: 1 ratio).
| [14] | Kusum A, Negi G, Gaur DS, Kishore S, Meena H, Sharma A, Verma SK. Hematological malignancies diagnosed by bone marrow examination in a tertiary hospital at Uttarakh and, India. Indian J Hematol Blood Transfus. 2008 Mar; 24(1): 7-11. https://doi.org/10.1007/s12288-008-0003-6 |
[14]
B-Specific Diagnostic Scenarios:
Fever of unknown origin: As noted in the African context, BME remains valuable globally in FUO, particularly when hematological abnormalities like cytopenias are present.
| [7] | Hot A, Jaisson I, Girard C, French M, Durand DV, Rousset H, Ninet J. Yield of bone marrow examination in diagnosing the source of fever of unknown origin. Arch Intern Med. 2009 Nov 23; 169(21): 2018-23
https://doi.org/10.1001/archinternmed.2009.384 |
[7]
Isolated Thrombocytopenia: The necessity of routine BME for diagnosing Immune Thrombocytopenic Purpura (ITP) is debated. Jubelirer and Harpold (2002) reviewed studies suggesting BME may not be essential for typical ITP, as findings are often consistent and alternative diagnoses rarely emerge during follow-up.
| [15] | Jubelirer SJ, Harpold R. The role of the bone marrow examination in the diagnosis of immune thrombocytopenic purpura: case series and literature review. Clin Appl Thromb Hemost. 2002 Jan; 8(1): 73-6.
https://doi.org/10.1177/107602960200800112 |
[15]
Genetic Susceptibility: Research extends beyond morphology to genetic factors. Elderberry et al. (2023) identified a significant association between the GSTT1 null genotype and increased susceptibility to Philadelphia-negative Chronic Myeloid Leukemia (Ph-ve CML), highlighting the role of detoxification enzyme polymorphisms in hematological malignancies.
| [16] | Elderdery AY, Idris HME, Tebien EM, Diab NA, Hamza SMA, Suliman BA, et al. Impact of GSTT1 and GSTM1 Polymorphisms in the Susceptibility to Philadelphia Negative Chronic Myeloid Leukaemia. Curr Cancer Drug Targets. 2023; 23(4): 319-324.
https://doi.org/10.2174/1568009623666230112104505 |
[16]
C-Unusual Presentations & Complications:
Case report sill lustrates rare but critical findings detectable by BME correlated to underlying conditions/therapies:
1) Chronic Myeloid Leukemia (CML) presenting with spontaneous splenic rupture
| [17] | Jafferbhoy S, Chantry A, Atkey N, Turner D, Wyld L. Spontaneous splenic rupture: an unusual presentation of CML. BMJ Case Rep. 2011 Mar 24; 2011: bcr0220113879.
https://doi.org/10.1136/bcr.02.2011.3879 |
[17]
2) CML complications like sudden bilateral deafness (potentially hyper leukocytosis-related) and hydroxyurea-induced leg ulcers
| [18] | Ugwu NI, Okoye AE, Ugwu CN, Ibiam FA, Nnachi OA, Ugwu GC, Okoh NU. Chronic Myeloid Leukaemia with Sudden Bilateral Deafness and Leg Ulcer Associated with Hydroxyurea Therapy. West Afr J Med. 2021 May 29; 38(5): 502-506. |
[18]
3) Disseminated mucormycosis causing paralysis post-BM Tin AML.
| [19] | Itakusu K, Inoue T, Abe M, Ueda R, Sakurai A, Miyazaki Y, et al. [Acute myeloid leukemia with sudden onset bilateral lower extremity paralysis caused by disseminated mucormycosis following unrelated bone marrow transplantation]. Rinsho Ketsueki. 2019; 60(1): 17-21. Japanese.
https://doi.org/10.11406/rinketsu.60.17 |
[19]
4) Rare primary bone marrow lymphomas mimicking aplastic anemia.
| [20] | Nogami A, Yamamoto M, Yamamoto K, Ito M, Umezawa Y, Tohda S, et al. [Marginal zone lymphoma-like primary bone marrow lymphoma with long-term pancytopenia preceding diagnosis]. Rinsho Ketsueki. 2020; 61(10): 1469-1475. Japanese. https://doi.org/10.11406/rinketsu.61.1469 |
[20]
5) Asymptomatic bone and bone marrow metastases from gastric signet-ring cell carcinoma.
| [21] | Okumura T, Hihara Y, Muraoka S, Nishimura Y, Inoue K, Maruyama A, et al. [Case of Asymptomatic Multiple Bone and Bone Marrow Metastases in Gastric Signet-Ring Cell Carcinoma]. Gan To Kagaku Ryoho. 2020 Jul; 47(7): 1105-1107. Japan. |
[21]
D-Diagnostic Utility:
Globally, BME maintains its status as a definitive test when peripheral blood and routine labs are inconclusive, guiding management and prognosis, especially where advanced diagnostics are limited.
| [8] | Ebrahim H, Fisha T, Debash H, Bisetegn H. Patterns of Bone Marrow Confirmed Malignant and Non-Malignant Hematological Disorders in Patients with Abnormal Hematological Parameters in Northeast Ethiopia. J Blood Med. 2022 Feb 15; 13: 51-60. https://doi.org/10.2147/JBM.S345141 |
| [14] | Kusum A, Negi G, Gaur DS, Kishore S, Meena H, Sharma A, Verma SK. Hematological malignancies diagnosed by bone marrow examination in a tertiary hospital at Uttarakh and, India. Indian J Hematol Blood Transfus. 2008 Mar; 24(1): 7-11. https://doi.org/10.1007/s12288-008-0003-6 |
[8, 14]
6. Methodology
6.1. Study Design
This is a retrospective, Descriptive, cross sectional, hospital based study conducted to assess bone marrow examination finding at Al-Mek Nimir University Hospital in Shendi Sudan.
6.2. Study Area
Shendi town: This study was done in Shendi city, which located in the north of the Sudan. It situated on eastern bank of the Nile River, approximately 150 km northeast of Khartoum. The city covers an area approximately 124000 km squares population estimated between 1787 and 2211. The main tribes living in Shendi are Jaalya, Shwaygia, Hasania and other group. Most of population are Farming. There are several general centers for different service and also there is Shendi University with different colleges. There are many health care and hospital and oncology centre for cancer treatment which is third hospital for oncology in the Sudan.
Al-Mek Nimir University Hospital; which is establish in July 2002, is one of largest hospital in the area which have different department and provide good health service for population Shendi area, there is medicine department, surgery, pediatric, obstetrical, ENT, ICU, ophthalmic, dental unit, minor and major theater, CCU, emergency room, oncology and dialysis unit, there is also blood bank and pharmacy and laboratory.
6.3. Study Population
All patients who underwent bone marrow examination during the study period were included
6.4. Sampling Technique
The population selected by simpler and ohm sample.
6.5. Sampling Size
The total sample size was 292 patients.
6.6. Inclusion and Exclusion Criteria
Inclusion Criteria
1) All patients who underwent bone marrow aspiration and/or trephine biopsy at Al-Mek Nimer University Hospital.
2) Patients of all age groups and both genders
3) Records with complete diagnostic and demographic data
4) Cases performed between April 2023 and February 2025.
5) Exclusion Criteria
6) Incomplete or missing patient records
7) Poor-quality or inadequate bone marrow samples
8) Repeat bone marrow examinations for the same patient (only the first diagnostic sample included).
9) Cases with inconclusive or non-diagnostic results
6.7. Data Collection Tools
Data were collected from patient's files available at the hospital.
6.8. Data Analysis
Data was analyzed by SPAS and presented in figures and tables.
6.9. Ethical Consideration
Ethical approval was obtained from the Department of Community Medicine, Faculty of Medicine, Shendi University. Permission was obtained from hospital administration.
7. Results
A total number 291 of bone marrow examination findings in Al-Mek Nimer University Hospital were enrolled in this study during the period from April 2023 to February 2025, the data obtained explained in tables and figures.
The youngest patient was a 2-month-old female diagnosed with Gaucher disease, while the oldest was a 104-year-old female with megaloblastic anemia.
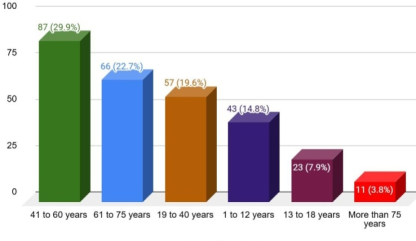
According to the age:
Out of a total of 291 patients' with age distribution ranging from less than 1 year to over 75 years, the estimated mean age was approximately 41.5 years, with an age range of 2 months to 104 years and an estimated standard deviation of 22.9 years, indicating significant age variability within the sample? The largest age group was 41–60 years (29.90%), followed by 61–75 years (22.68%) and 19–40 years (19.59%). The smallest age category was infants under 1 year (1.37%). This distribution reflects a predominantly middle-aged and older adult population. (
Table 1,
Figure 1)
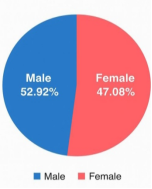
According the gender:
One hindered fixity four were male (52.92%) and 137 were female (47.08%) the male to female ratio was approximately 1.1: 1 with the largest gender disparity in the 61– 75 years group indicating a slight male predominance. (
Figure 2)
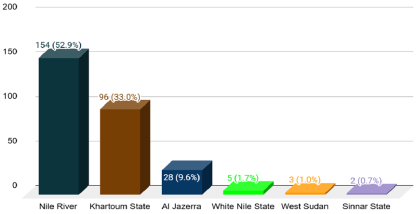
According to the residence:
The majority of individual's residence in River Nile State (52.9%) and Khartoum State (33%), with other regions each representing less than 10% of the sample (
Figure 3)
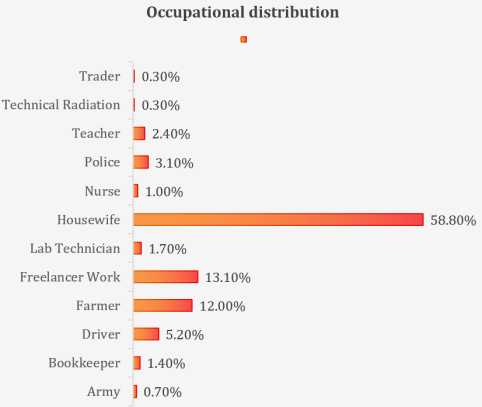
According to the Occupational:
Occupationally, 58.8% report house wife, followed by freelancer work (13.1%) and farmers (12.0%). Other occupations, such as driver (5.2%) and police (3.1%), are less common, with highly specialized roles like technical radiation and trader being rare (0.3% each). (
Table 2,
Figure 4)
According the investigation type:
All 291 individuals underwent aspiration and biopsy. "Finger 5)
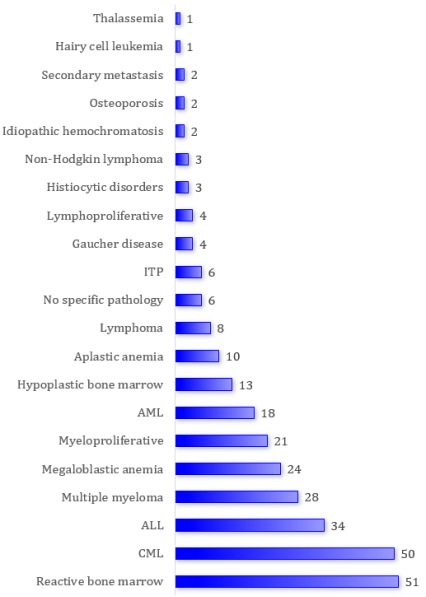
According to the finding:
The most prevalent results were reactive bone marrow (17.5%) and chronic lymphocytic leukemia (17.2%), followed by ALL (11.7%), multiple myeloma (9.6%), and megaloblastic anemia (8.2%). Rare conditions included thalassemia and hairy cell leukemia (0.3%each). The diverse diagnoses, with a significant proportion of reactive bone marrow and leukemias, suggest a population with varied hematological disorders, predominantly non-malignant or chronic conditions. (
Figure 6)
Diagnosis results and AGE Cross tabulation:
Diagnosis results and AGE Cross tabulation Leukemia (113 cases) and non-specific/reactive conditions (53 cases) are the most frequent diagnoses, with leukemia distributed across all age groups, peaking in middle-aged (32) and elderly (30) individuals. Anemia (35) is more common in elderly (13), while lymphomas (15) and myeloma-related disorders (31) are rare in pediatric cases. The chi-square test (χ² = 256.805, df = 120, p <.001) suggests a significant association between age and diagnosis, indicating age influences hematological conditions. (
Table 3)
Diagnosis results and Residence Cross tabulation:
Diagnosis results and Residence Cross tabulation Leukemias (113 cases) and non- specific/reactive conditions (56 cases) dominate, with Nile River showing the highest frequency (63 and 34 cases, respectively), followed by Khartoum State (42 and 15). Anemias (35) and myeloma-related disorders (31) are also notable, particularly in Nile River (19 and 24). Other regions have low case counts, with no dominant diagnosis. The chi-square test (χ²= 281.496, df = 160, p <.001) suggests a significant association between residence and diagnosis, but the high proportion of cells with expected counts below 5 (91.5%) limits reliability. The data indicates regional variations, with Nile River and Khartoum State bearing the majority of hematological cases, particularly leukemias and reactive conditions. (
Table 4)
Distribution of Bone Marrow Diagnosis in Shendi and around:
Distribution of Bone Marrow Diagnosis in Shendi and around Shendi shows the majority of cases coming from Shendi and Hager Alasel. Leukemias were the most commonly reported group of diagnoses, accounting for 51 out of 135 cases (approximately 38%), with a notably high concentration in Shendi. Other common diagnoses included anemias (17 cases) and myeloma-related disorders (20 cases). Meanwhile, rare conditions such as Gaucher disease, histiocytic disorders, and bone marrow fibrosis were reported in only one or two patients. (
Table 5)
Diagnosis results and Occupation Cross tabulation:
Leukemias (113 cases) and non-specific/reactive conditions (57 cases) are the most common diagnoses, predominantly among the unemployed (77 and 36 cases, respectively). Skilled laborers also show notable frequencies for leukemias (29) and non-specific/reactive conditions (19), while professionals have fewer cases across all diagnoses (e.g., 7 for leukemias). Anemias (35) and myeloma-related disorders (31) are less frequent but still significant among the unemployed (22 and 14).The chi-square test (χ²=194.917, df=220, p=.887) indicates no significant association between occupation and diagnosis, likely due to the high proportion of cells with expected counts below 5 (94.8%), which undermines the test’s reliability. The data suggests hematological conditions are most prevalent among the unemployed, with skilled laborers also affected, but no clear occupational pattern emerges. (
Table 6)
Bone Marrow Findings according to Underlying Cause:
Bone Marrow Findings by Underlying Cause among 61 cases, reactive bone marrow is the most prevalent finding (51 cases, 83.6%), predominantly associated with hypersplenism (25 cases, 41.0%) and immune-mediated peripheral destruction (9 cases, 14.8%). Secondary metastasis accounts for 5 cases (8.2%), with 4 linked to reactive marrow and 1 to hypoplastic marrow. No specific pathology was observed in 5 cases (8.2%), mainly tied to excluding multiple myeloma (4 cases). Hypoplastic bone marrow (3 cases, 4.9%) is rare, linked to secondary metastasis and neuroendocrine disorders. Myeloproliferative leukemia is least common (2 cases, 3.3%), exclusively associated with juvenile disorders. These findings suggest reactive marrow changes dominate, driven by systemic conditions like hypersplenism, with other findings being less frequent. (
Table 7)
Classification of Diagnoses into Hematological and Oncological Diseases:
Classification of Diagnoses into Hematological and Oncological Diseases shows the distribution of diagnoses among the 291 patients reveals that oncological diseases are significantly more common than hematological diseases, accounting for 64.6% (188 cases) of all findings. Among the oncological disorders, acute lymphocytic leukemia (ALL) was the most frequent single diagnosis with 34 cases (11.7%), followed closely by chronic myelogenous leukemia (CML) with 30 combined cases (10.3%) and multiple myeloma with 28 cases (9.6%). Other malignant or neoplastic conditions like chronic lymphocytic leukemia (CLL), myeloproliferative disorders (MPL, MPN), lymphomas, and metastatic tumors collectively contribute substantially to the overall cancer burden. In contrast, hematological (non-malignant) disorders made up 35.4% (103 cases) of the total. The most frequent within this group was megaloblastic anemia with 21 cases (7.2%), followed by reactive bone marrow changes in 28 cases (9.6%), indicating a considerable number of patients with reversible or non-neoplastic marrow responses. Aplastic anemia, ITP, Gaucher disease, and other marrow abnormalities such as fibrosis and osteosclerosis appeared in lower frequencies. (
Table 8)
Table 1. AGE and Gender distribution.
AGE | Female (n,%) | Male (n,%) | Total (n,%) |
Less than 1 year | 2(0.69%) | 2(0.69%) | 4(1.37%) |
1 to 12 years | 19(6.53%) | 24(8.25%) | 43(14.78%) |
13 to 18 years | 11(3.78%) | 12(4.12%) | 23(7.90%) |
19 to 40 years | 28(9.62%) | 29(9.97%) | 57(19.59%) |
41 to 60 years | 48(16.49%) | 39(13.40%) | 87(29.90%) |
61 to 75 years | 25(8.59%) | 41(14.09%) | 66(22.68%) |
more than 75 years | 4(1.37%) | 7(2.41%) | 11(3.78%) |
Total | 137(47.08%) | 154(52.92%) | 291(100.00%) |
Figure 2. Gender distribution.
Figure 3. Residence distribution.
Table 2. Occupation.
Occupation | Frequency | Percent |
Army | 2 | 0.7% |
Bookkeeper | 4 | 1.4% |
Driver | 15 | 5.2% |
Farmer | 35 | 12.0% |
Freelancer Work | 38 | 13.1% |
Lab Technician | 5 | 1.7% |
Housewife | 171 | 58.8% |
Nurse | 3 | 1.0% |
Police | 9 | 3.1% |
Teacher | 7 | 2.4% |
Technical Radiation | 1 | 0.3% |
Trader | 1 | 0.3% |
Total | 291 | 100.0% |
Figure 4. Occupational distribution.
Figure 5. Types of investigations.
Figure 6. Diagnosis results distribution.
Table 3. Diagnosis results and AGE Cross tabulation.
Diagnosis Group | Pediatric (< 1 to 12 years) | Adolescent/Young Adult (13–40 years) | Middle Aged (41–60 years) | Elderly (61–75+ years) | Total |
ALL, AML, CLL, HCL, Myeloproliferative | 24 | 27 | 32 | 30 | 113 |
Aplastic, Megaloblastic, Thalassemia | 5 | 7 | 10 | 13 | 35 |
Lymphoma, NHL, Lymph proliferative | 0 | 7 | 6 | 2 | 15 |
Multiple Myeloma, Gaucher, Histiocytic | 3 | 1 | 15 | 12 | 31 |
Hypoplastic BM, IHC, ITP, Osteoporosis, Secondary Metastasis | 2 | 3 | 9 | 5 | 19 |
Reactive BM, No Specific Pathology | 9 | 18 | 15 | 11 | 53 |
Total | 43 | 80 | 87 | 77 | 291 |
Table 4. Diagnosis results and Residence Cross tabulation.
Diagnosis Group | Al Jazera | Khartoum State | Nile River | Other Regions | Total |
ALL, AML, CLL, HCL, Myeloproliferative | 15 | 42 | 63 | 3 | 113 |
Aplastic, Megaloblastic, Thalassemia | 2 | 13 | 19 | 1 | 35 |
Lymphoma, NHL, Lymphoproliferative | 3 | 6 | 5 | 1 | 15 |
Multiple Myeloma, Gaucher, Histiocytic | 2 | 8 | 24 | 1 | 31 |
Hypoplastic BM, IHC, ITP, Osteoporosis, Secondary Metastasis | 1 | 13 | 10 | 0 | 24 |
Reactive BM, No Specific Pathology | 6 | 15 | 34 | 1 | 56 |
Total | 28 | 96 | 154 | 13 | 291 |
Table 5. Distribution of Bone Marrow Diagnosis in Shendi and around Shendi.
Diagnosis Group | Almahmia | Begrawia | Grii | Hager Alasel | Kaboshia | Shendi | South Shendi | West Shendi | Total |
Leukemias-ALL, AML, CLL, CML, MPL, MPN | 0 | 0 | 4 | 10 | 3 | 26 | 0 | 8 | 51 |
Anemias Aplastic, Megaloblastic, Macrocytic | 1 | 0 | 2 | 3 | 0 | 9 | 0 | 2 | 17 |
-Lymphoma, Related Disorders | 0 | 0 | 1 | 0 | 0 | 2 | 0 | 1 | 4 |
Multiple Myeloma, Gaucher, Histiocytic | 0 | 0 | 2 | 4 | 0 | 12 | 1 | 1 | 20 |
Hypoplastic BM, IHC, ITP, Fibrosis, Osteosclerosis, Secondary Mets | 1 | 0 | 2 | 1 | 0 | 6 | 0 | 3 | 13 |
Reactive BM, No Specific Pathology | 0 | 1 | 0 | 3 | 0 | 12 | 0 | 3 | 19 |
Total | 2 | 1 | 11 | 21 | 3 | 67 | 1 | 18 | 124 |
Table 6. Diagnosis results and Occupation Cross tabulation.
Diagnosis Group | Professional | Skilled Labor | Unemployed | Total |
Leukemias | 7 | 29 | 77 | 113 |
ALL, AML, CLL, HCL, Myeloproliferative | | | | |
| 3 | 9 | 22 | 35 |
Aplastic, Megaloblastic, Thalassemia | | | | |
| 2 | 6 | 7 | 15 |
Lymphoma, NHL, Lymphoproliferative | | | | |
| 4 | 14 | 14 | 31 |
MultipleMyeloma, Gaucher, Histiocytic | | | | |
| 3 | 7 | 11 | 21 |
Hypoplastic BM, IHC, ITP, Osteoporosis, Secondary Metastasis | | | | |
| 2 | 19 | 36 | 57 |
Reactive BM, No Specific Pathology | | | | |
Total | 21 | 84 | 171 | 291 |
Table 7. Bone Marrow Findings by Underlying Cause.
UnderlyingCause | Hypoplastic Bone Marrow | Myeloproliferative Leukemia | No Specific Pathology | Reactive Bone Marrow | Total |
Hypersplenism | 0 | 0 | 0 | 25 | 25 |
Peripheral Destruction (Immune-Mediated) | 0 | 0 | 0 | 9 | 9 |
Peripheral Destruction (Other) | 0 | 0 | 0 | 2 | 2 |
Exclude Multiple Myeloma | 0 | 0 | 4 | 0 | 4 |
Secondary Metastasis | 1 | 0 | 0 | 4 | 5 |
Infection (Tuberculosis/Malaria/Viral) | 0 | 0 | 0 | 4 | 4 |
Lymphoproliferative Disorder (Staging) | 0 | 0 | 0 | 1 | 1 |
Down Syndrome | 0 | 0 | 0 | 1 | 1 |
Cytopenia (Immune, Lung Fibrosis) | 0 | 0 | 1 | 0 | 1 |
Neuroendocrine Disorder | 1 | 0 | 0 | 0 | 1 |
Juvenile Myeloproliferative Disorder | 0 | 2 | 0 | 0 | 2 |
Thalassemia | 0 | 0 | 0 | 1 | 1 |
Mixed Anemia | 0 | 0 | 0 | 1 | 1 |
No Pathology | 0 | 0 | 0 | 1 | 1 |
Total | 3 | 2 | 5 | 51 | 61 |
Table 8. Classification of Diagnoses into Hematological and Oncological Diseases.
Diagnosis Group | ConditionsIncluded | Frequency | Percent |
Hematological Diseases | PRCA, Active bone marrow, Aplastic anemia, Megaloblastic anemia, Macrocytic anemia, Thalassemia, ITP, IHC, Gaucher disease, Bone marrow fibrosis/necrosis/osteosclerosis, Hypercellular BM, Hypocellular BM, Hypoplastic BM, Reactive BM, Osteoporosis, Renal osteodystrophy | 103 | 35.4% |
Oncological Diseases | ALL, AML, CML, CLL, HCL, Lymphoma, NHL, MultipleMyeloma, MPL, MPN, LPD, Secondary metastasis, Tumor, Histiocytic disorders | 188 | 64.6% |
Total | | 291 | 100.0% |
8. Discussion
The present study provides critical insights into the spectrum of bone marrow examination findings among the Sudanese patient during a period of armed conflict, reflecting not only disease patterns but also the broader socio-economic and health disruptions that impact diagnostic outcomes.
The predominance of leukemia (38.8%) and non-specific reactive marrow changes (19.6%) is consistent with findings from previous studies in both Sudan and broader African contexts, For example, in North Sudan, Elmadhoun et al. identified aplastic anemia as the leading pathology in bone marrow aspirations conducted in Atbara, with a diagnostic yield of 76.8%
| [5] | Elmadhoun WM, Noor SK, Bushara SO, Almobarak AO, Husain NE, Ahmed MH. Bone marrow aspiration in north Sudan: the procedure, indications and the diagnosticvalue. Int J Health Sci (Qassim). 2015 Oct; 9(4): 434-9.
https://doi.org/10.12816/0031233 |
[5]
.
In contrast, our data show a more prominent presence of leukemias and chronic lymphoproliferative conditions, possibly reflecting delays in healthcare access and diagnosis, leading to more advanced disease presentation.
Leukemia widespread presence across all age groups in our sample with peaks in middle-aged and elderly populations mirrors pan-African findings where both acute and chronic leukemia consistently feature as top malignant diagnoses
| [2] | Okinda NA, Riyat MS. Bone marrow examination findings at AgaKhan University Hospital, Nairobi. East Afr Med J. 2010 Jan; 87(1): 11–17. |
| [6] | Yuguda S, Girei AI, Pindiga KM, Dachi RA, Lawan AI, Abdullahi YM. Indications and Diagnostic Utility of Bone Marrow Aspiration Cytology: A 12-year Experience at a Tertiary Health Center in Gombe, Northeastern Nigeria. Ann Trop Pathol. 2020 Jul- Dec; 11(2): 119-122.
https://doi.org/10.4103/atp.atp_33_19 |
| [10] | Tshabalala WS, Pillay S, Wilson DPK. Diagnostic outcomes of bone marrow aspirate and trephine biopsies performed at a hospital in KwaZulu-Natal, South Africa. Afr J Lab Med. 2020 Feb 25; 9(1): 1028. https://doi.org/10.4102/ajlm.v9i1.1028 |
[2, 6, 10]
.
This broad age distribution reinforces the role of bone marrow biopsy in diagnosing hematological malignancies across the life span.
Notably, the higher prevalence of chronic lymphocytic leukemia (CLL) and acute lymphoblastic leukemia (ALL) in our data aligns with trends reported in South Africa and Kenya
| [2] | Okinda NA, Riyat MS. Bone marrow examination findings at AgaKhan University Hospital, Nairobi. East Afr Med J. 2010 Jan; 87(1): 11–17. |
| [10] | Tshabalala WS, Pillay S, Wilson DPK. Diagnostic outcomes of bone marrow aspirate and trephine biopsies performed at a hospital in KwaZulu-Natal, South Africa. Afr J Lab Med. 2020 Feb 25; 9(1): 1028. https://doi.org/10.4102/ajlm.v9i1.1028 |
[2, 10]
.
Furthermore, the concentration of leukemia cases in the River Nile and Khartoum States may reflect not only regional population densities but also varying degrees of health care infrastructure and accessibility.
The burden of non-malignant hematological disorders, including megaloblastic anemia and aplastic anemia, is also evident, albeit to a lesser extent. These findings are in line with studies from Nigeria and Ethiopia that emphasize nutritional deficiency anemias and bone marrow suppression due to infections, poor nutrition, or environmental exposures
| [6] | Yuguda S, Girei AI, Pindiga KM, Dachi RA, Lawan AI, Abdullahi YM. Indications and Diagnostic Utility of Bone Marrow Aspiration Cytology: A 12-year Experience at a Tertiary Health Center in Gombe, Northeastern Nigeria. Ann Trop Pathol. 2020 Jul- Dec; 11(2): 119-122.
https://doi.org/10.4103/atp.atp_33_19 |
| [8] | Ebrahim H, Fisha T, Debash H, Bisetegn H. Patterns of Bone Marrow Confirmed Malignant and Non-Malignant Hematological Disorders in Patients with Abnormal Hematological Parameters in Northeast Ethiopia. J Blood Med. 2022 Feb 15; 13: 51-60. https://doi.org/10.2147/JBM.S345141 |
[6, 8]
.
Given the known impacts of conflict on food security, sanitation, and healthcare availability, our findings of 12% non-malignant anemia may underestimate the true prevalence, particularly considering the diagnostic limitations inherent to conflict settings.
The relatively high occurrence of reactive or non-specific bone marrow findings (19.6%) highlights another dimension of conflict-related health challenges. Such findings are often linked to infections, inflammatory processes, or general physiological stress all likely exacerbated by displacement, malnutrition, and psychosocial strain during conflict Similar trends were observed in Malawi, where benign and reactive marrow changes constituted over 60% of findings, especially in immunocompromised populations
| [9] | Edwards Kasonkanji et al. Quality and Diagnostic Characterization of Bone Marrow Biopsies at Kamuzu Central Hospital, Malawi: A Retrospective Study. JCO Glob Oncol. 2024; 10: 155-156. https://doi.org/10.1200/GO.23.00274 |
[9]
.
The diagnostic profile of multiple myeloma, lymphomas, and histiocytic disorders in this study further demonstrates the importance of BME in identifying chronic and often late- stage malignancies. As in studies from India and South Africa, multiple myeloma showed a preference for older adults and was more frequently identified in urban centers with better healthcare access
| [10] | Tshabalala WS, Pillay S, Wilson DPK. Diagnostic outcomes of bone marrow aspirate and trephine biopsies performed at a hospital in KwaZulu-Natal, South Africa. Afr J Lab Med. 2020 Feb 25; 9(1): 1028. https://doi.org/10.4102/ajlm.v9i1.1028 |
| [14] | Kusum A, Negi G, Gaur DS, Kishore S, Meena H, Sharma A, Verma SK. Hematological malignancies diagnosed by bone marrow examination in a tertiary hospital at Uttarakh and, India. Indian J Hematol Blood Transfus. 2008 Mar; 24(1): 7-11. https://doi.org/10.1007/s12288-008-0003-6 |
[10, 14]
The relative under representation of pediatric lymphomas, especially when compared to African pediatric studies where up to 27%of BME yielded malignancies
| [20] | Nogami A, Yamamoto M, Yamamoto K, Ito M, Umezawa Y, Tohda S, et al. [Marginal zone lymphoma-like primary bone marrow lymphoma with long-term pancytopenia preceding diagnosis]. Rinsho Ketsueki. 2020; 61(10): 1469-1475. Japanese. https://doi.org/10.11406/rinketsu.61.1469 |
[20]
, may reflect referral patterns, survival bias, or limitations in pediatric oncology services in Shendi.
Demographically, the preponderance of hematological abnormalities among unemployed individuals is noteworthy. While the study’s chi-square test did not show a statistically significant association between occupation and diagnosis, the clear clustering of leukemia and anemia cases among those without formal employment suggests a potential social determinant of health. Similar findings have been reported in conflict zones, where economic instability correlates with higher disease burdens due to limited nutrition, healthcare access, and health literacy
| [7] | Hot A, Jaisson I, Girard C, French M, Durand DV, Rousset H, Ninet J. Yield of bone marrow examination in diagnosing the source of fever of unknown origin. Arch Intern Med. 2009 Nov 23; 169(21): 2018-23
https://doi.org/10.1001/archinternmed.2009.384 |
| [22] | Mirzai AZ, Hosseini N, Sadeghipour A. Indications and diagnostic utility of bone marrow examination in different bone marrow disorders in Iran. Lab Hematol. 2009; 15(4): 38-44. https://doi.org/10.1532/LH96.09009 |
[7, 22]
.
The study’s retrospective design, while necessary due to operational constraints during conflict, limits causal inference. Nonetheless, the statistically significant association between age and diagnosis (χ² = 256.805, p <.001) reinforces known age-related disease trends, while the weak association with occupation (p =.887) may reflect limitations in occupational data classification
Importantly, the elevated proportion of expected counts below 5 in chi-square tests for occupation and residence (over 87% and 91%, respectively) suggests that larger, prospective studies with better stratification are needed to clarify these trends. The implications of these findings are profound.
The heavy burden of leukemia and reactive conditions amidst a backdrop of conflict underscores both a high diagnostic need and the fragility of health systems under duress. Studies from South Africa and Ethiopia highlight how limited diagnostics and delayed presentation compromise care, and these concerns are magnified in the context of active conflict
| [22] | Mirzai AZ, Hosseini N, Sadeghipour A. Indications and diagnostic utility of bone marrow examination in different bone marrow disorders in Iran. Lab Hematol. 2009; 15(4): 38-44. https://doi.org/10.1532/LH96.09009 |
[22]
.
Furthermore, operational challenges such as lack of pathologists, disrupted supply chains, and infrastructural damage—as outlined in the literature—likely affected both the performance and interpretation of BME in Shendi.
In conclusion, the data reveals a complex hematological landscape shaped by both biological disease processes and socio-political turmoil. The dominance of leukemias, the presence of significant non-malignant pathology, and the regional and occupational variations observed highlight the urgent need for improved diagnostic capacity, public health surveillance, and conflict-sensitive healthcare planning.
This study provides a critical evidence base for national health policy and offers a foundation for future research into the intersection between armed conflict and hematological disease burden in Sudan.
9. Conclusion
This study highlights a high burden of hematological malignancies and significant proportions of reactive and nutritional bone marrow disorders among Sudanese patients in a conflict-affected setting. The findings reflect delayed healthcare access, socioeconomic challenges, and limited diagnostic resources. Bone marrow examination remains an indispensable diagnostic tool in such environments. Addressing gaps in early detection, expanding diagnostic capacity, and implementing targeted public health interventions are essential to improving patient outcomes and reducing disease-related morbidity and mortality.
10. Recommendations
1) Strengthen early diagnostic services through mobile and outreach hematology units in underserved and conflict-affected areas.
2) Implement targeted screening programs for high-risk groups, particularly older adults and socioeconomically vulnerable populations.
3) Improve access to advanced diagnostic modalities such as flow cytometry and molecular testing.
4) Enhance training of healthcare providers in early recognition and referral of hematological disorders.
5) Establish a national registry for hematological diseases to support surveillance and research.
6) Promote nutritional support programs, including micronutrient supplementation, to reduce preventable hematological conditions.
7) Improve medical record systems and data documentation for better research and clinical decision-making.
11. Limitations of the Study
1) Retrospective design limits the ability to establish causality.
2) Single-center study, which may limit generalizability to other regions of Sudan.
3) Possible selection biases, as only patients who reached the hospital and underwent BME were included.
4) Incomplete clinical data due to documentation challenges during conflict.
5) Lack of advanced diagnostic tools (e.g., flow cytometry, cytogenetics, and molecular studies) may have affected diagnostic accuracy and sub-classification.
6) Socioeconomic variables may not have been fully captured or standardized.
Abbreviations
BME | Bone Marrow Examination |
ALL | Acute Lymphocytic Leukemia |
CLL | Chronic Lymphocytic Leukemia |
AML | Acute Myelogenous Leukemia |
CML | Chronic Myelogenous Leukemia |
ITP | Idiopathic Thrombocytopenic |
MPL | Myelo Proliferative Leukemia |
IHC | Idiopathic Hemochromatosis |
HCL | Hairy Cell Leukemia |
NHL | Nonhodgkin Lymphoma |
PRCA | Pure Red Cell Aplasia |
Acknowledgments
The authors would like to thank the staff of Al-Mek Nimer University Hospital for their support in data collection.
Author Contributions
Motwakil Imam Awadelkareim Imam: Conceptualization, Supervision, Writing – review & editing
Baker Mohammed Saleh Hadi Gahaf: Data curation, Investigation, Writing – original draft
Muayid Abdullah Ahmed Mohammed: Formal Analysis, Methodology, Visualization
Funding
This research did not receive any specific grant from any funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of Interest
The authors declared no conflict of interest.
References
| [1] |
Islam A. Manual of Bone Marrow Examination. 1sted. Dhaka: Anwer Khan Modern Medical College; 2015.
|
| [2] |
Okinda NA, Riyat MS. Bone marrow examination findings at AgaKhan University Hospital, Nairobi. East Afr Med J. 2010 Jan; 87(1): 11–17.
|
| [3] |
Vergidis D. Bone Marrow Aspiration and Biopsy: Overview. In: Medscape [Internet]. New York: Web MD; [updated 2023 May 17; cited 2025 Jul 3].
|
| [4] |
Bashawri LA. Bonemarrow examination. Indications and diagnostic value. Saudi Med J. 2002; 23(2): 191-196.
|
| [5] |
Elmadhoun WM, Noor SK, Bushara SO, Almobarak AO, Husain NE, Ahmed MH. Bone marrow aspiration in north Sudan: the procedure, indications and the diagnosticvalue. Int J Health Sci (Qassim). 2015 Oct; 9(4): 434-9.
https://doi.org/10.12816/0031233
|
| [6] |
Yuguda S, Girei AI, Pindiga KM, Dachi RA, Lawan AI, Abdullahi YM. Indications and Diagnostic Utility of Bone Marrow Aspiration Cytology: A 12-year Experience at a Tertiary Health Center in Gombe, Northeastern Nigeria. Ann Trop Pathol. 2020 Jul- Dec; 11(2): 119-122.
https://doi.org/10.4103/atp.atp_33_19
|
| [7] |
Hot A, Jaisson I, Girard C, French M, Durand DV, Rousset H, Ninet J. Yield of bone marrow examination in diagnosing the source of fever of unknown origin. Arch Intern Med. 2009 Nov 23; 169(21): 2018-23
https://doi.org/10.1001/archinternmed.2009.384
|
| [8] |
Ebrahim H, Fisha T, Debash H, Bisetegn H. Patterns of Bone Marrow Confirmed Malignant and Non-Malignant Hematological Disorders in Patients with Abnormal Hematological Parameters in Northeast Ethiopia. J Blood Med. 2022 Feb 15; 13: 51-60.
https://doi.org/10.2147/JBM.S345141
|
| [9] |
Edwards Kasonkanji et al. Quality and Diagnostic Characterization of Bone Marrow Biopsies at Kamuzu Central Hospital, Malawi: A Retrospective Study. JCO Glob Oncol. 2024; 10: 155-156.
https://doi.org/10.1200/GO.23.00274
|
| [10] |
Tshabalala WS, Pillay S, Wilson DPK. Diagnostic outcomes of bone marrow aspirate and trephine biopsies performed at a hospital in KwaZulu-Natal, South Africa. Afr J Lab Med. 2020 Feb 25; 9(1): 1028.
https://doi.org/10.4102/ajlm.v9i1.1028
|
| [11] |
Phillips L, Opie J. The utility of bone marrow sampling in the diagnosis and staging of lymphoma in South Africa. Int J Lab Hematol. 2018 Jun; 40(3): 276-283.
https://doi.org/10.1111/ijlh.12801
|
| [12] |
BainBJ, Clark DM, Wilkins BS. Bone marrow pathology. 4thed. Wiley-Blackwell; 2010.
https://doi.org/10.1002/9781444305943
|
| [13] |
Bashawri LA. An audit- indications and diagnosis of bone marrow biopsies at a tertiary care hospital in Saudi Arabia. Med Crave Online J Hematol Transfus. 2016; 1(1): 1–5.
https://doi.org/10.15406/mojht.2016.01.00005
|
| [14] |
Kusum A, Negi G, Gaur DS, Kishore S, Meena H, Sharma A, Verma SK. Hematological malignancies diagnosed by bone marrow examination in a tertiary hospital at Uttarakh and, India. Indian J Hematol Blood Transfus. 2008 Mar; 24(1): 7-11.
https://doi.org/10.1007/s12288-008-0003-6
|
| [15] |
Jubelirer SJ, Harpold R. The role of the bone marrow examination in the diagnosis of immune thrombocytopenic purpura: case series and literature review. Clin Appl Thromb Hemost. 2002 Jan; 8(1): 73-6.
https://doi.org/10.1177/107602960200800112
|
| [16] |
Elderdery AY, Idris HME, Tebien EM, Diab NA, Hamza SMA, Suliman BA, et al. Impact of GSTT1 and GSTM1 Polymorphisms in the Susceptibility to Philadelphia Negative Chronic Myeloid Leukaemia. Curr Cancer Drug Targets. 2023; 23(4): 319-324.
https://doi.org/10.2174/1568009623666230112104505
|
| [17] |
Jafferbhoy S, Chantry A, Atkey N, Turner D, Wyld L. Spontaneous splenic rupture: an unusual presentation of CML. BMJ Case Rep. 2011 Mar 24; 2011: bcr0220113879.
https://doi.org/10.1136/bcr.02.2011.3879
|
| [18] |
Ugwu NI, Okoye AE, Ugwu CN, Ibiam FA, Nnachi OA, Ugwu GC, Okoh NU. Chronic Myeloid Leukaemia with Sudden Bilateral Deafness and Leg Ulcer Associated with Hydroxyurea Therapy. West Afr J Med. 2021 May 29; 38(5): 502-506.
|
| [19] |
Itakusu K, Inoue T, Abe M, Ueda R, Sakurai A, Miyazaki Y, et al. [Acute myeloid leukemia with sudden onset bilateral lower extremity paralysis caused by disseminated mucormycosis following unrelated bone marrow transplantation]. Rinsho Ketsueki. 2019; 60(1): 17-21. Japanese.
https://doi.org/10.11406/rinketsu.60.17
|
| [20] |
Nogami A, Yamamoto M, Yamamoto K, Ito M, Umezawa Y, Tohda S, et al. [Marginal zone lymphoma-like primary bone marrow lymphoma with long-term pancytopenia preceding diagnosis]. Rinsho Ketsueki. 2020; 61(10): 1469-1475. Japanese.
https://doi.org/10.11406/rinketsu.61.1469
|
| [21] |
Okumura T, Hihara Y, Muraoka S, Nishimura Y, Inoue K, Maruyama A, et al. [Case of Asymptomatic Multiple Bone and Bone Marrow Metastases in Gastric Signet-Ring Cell Carcinoma]. Gan To Kagaku Ryoho. 2020 Jul; 47(7): 1105-1107. Japan.
|
| [22] |
Mirzai AZ, Hosseini N, Sadeghipour A. Indications and diagnostic utility of bone marrow examination in different bone marrow disorders in Iran. Lab Hematol. 2009; 15(4): 38-44.
https://doi.org/10.1532/LH96.09009
|
Cite This Article
-
APA Style
Imam, M. I. A., Gahaf, B. M. S. H., Mohammed, M. A. A. (2026). Bone Marrow Examination Findings Among Sudanese Patients During the Sudanese Armed Conflict (April 2023 to February 2025). Journal of Cancer Treatment and Research, 14(2), 53-65. https://doi.org/10.11648/j.jctr.20261402.11
 Copy
|
Copy
|
 Download
Download
ACS Style
Imam, M. I. A.; Gahaf, B. M. S. H.; Mohammed, M. A. A. Bone Marrow Examination Findings Among Sudanese Patients During the Sudanese Armed Conflict (April 2023 to February 2025). J. Cancer Treat. Res. 2026, 14(2), 53-65. doi: 10.11648/j.jctr.20261402.11
Copy
|
Download
AMA Style
Imam MIA, Gahaf BMSH, Mohammed MAA. Bone Marrow Examination Findings Among Sudanese Patients During the Sudanese Armed Conflict (April 2023 to February 2025). J Cancer Treat Res. 2026;14(2):53-65. doi: 10.11648/j.jctr.20261402.11
Copy
|
Download
-
@article{10.11648/j.jctr.20261402.11,
author = {Motwakil Imam Awadelkareim Imam and Baker Mohammed Saleh Hadi Gahaf and Muayid Abdullah Ahmed Mohammed},
title = {Bone Marrow Examination Findings Among Sudanese Patients During the Sudanese Armed Conflict (April 2023 to February 2025)},
journal = {Journal of Cancer Treatment and Research},
volume = {14},
number = {2},
pages = {53-65},
doi = {10.11648/j.jctr.20261402.11},
url = {https://doi.org/10.11648/j.jctr.20261402.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.jctr.20261402.11},
abstract = {Background: Armed conflict in Sudan has severely disrupted healthcare delivery, and access to diagnostic services. Despite the increasing burden of hematological disorders, data on bone marrow examination (BME) findings in such settings remain limited. This study aimed to characterize the spectrum of BME diagnoses in Sudanese patients during a period of ongoing conflict. Methods: A retrospective cross-sectional study was conducted at Al-Mek Nimer University Hospital, including 291 patients who underwent bone marrow examination (aspiration and trephine biopsy) between April 2023 and February 2025. Data were analyzed using SPSS. Results: Hematological malignancies accounting for 64.6% of cases. Leukemia was the most common diagnosis (38.8%), particularly chronic lymphocytic leukemia (17.2%), acute lymphoblastic leukemia (11.7%), and chronic myeloid leukemia (10.3%). Non-malignant conditions represented 35.4% of cases, mainly reactive marrow changes (17.5%) and megaloblastic anemia (7.2%) being the most frequent. Most patients were aged 41–60 years (29.9%), with a slight male predominance (52.9%). Geographically, most cases originated from River Nile State (52.9%) and Khartoum State (33%). A notable proportion of patients were unemployed (58.8%), suggesting socioeconomic vulnerability. Conclusion: There is high burden of advanced hematological malignancies and reactive marrow patterns likely due to delayed access to care during conflict. Bone marrow examination remains essential diagnostic tool in resource-limited settings. Strengthening mobile diagnostic services, promoting early screening among high-risk groups—particularly the elderly and unemployed—and implementing micronutrient supplementation programs may help reduce morbidity and improve outcomes in conflict-affected populations.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Bone Marrow Examination Findings Among Sudanese Patients During the Sudanese Armed Conflict (April 2023 to February 2025)
AU - Motwakil Imam Awadelkareim Imam
AU - Baker Mohammed Saleh Hadi Gahaf
AU - Muayid Abdullah Ahmed Mohammed
Y1 - 2026/05/13
PY - 2026
N1 - https://doi.org/10.11648/j.jctr.20261402.11
DO - 10.11648/j.jctr.20261402.11
T2 - Journal of Cancer Treatment and Research
JF - Journal of Cancer Treatment and Research
JO - Journal of Cancer Treatment and Research
SP - 53
EP - 65
PB - Science Publishing Group
SN - 2376-7790
UR - https://doi.org/10.11648/j.jctr.20261402.11
AB - Background: Armed conflict in Sudan has severely disrupted healthcare delivery, and access to diagnostic services. Despite the increasing burden of hematological disorders, data on bone marrow examination (BME) findings in such settings remain limited. This study aimed to characterize the spectrum of BME diagnoses in Sudanese patients during a period of ongoing conflict. Methods: A retrospective cross-sectional study was conducted at Al-Mek Nimer University Hospital, including 291 patients who underwent bone marrow examination (aspiration and trephine biopsy) between April 2023 and February 2025. Data were analyzed using SPSS. Results: Hematological malignancies accounting for 64.6% of cases. Leukemia was the most common diagnosis (38.8%), particularly chronic lymphocytic leukemia (17.2%), acute lymphoblastic leukemia (11.7%), and chronic myeloid leukemia (10.3%). Non-malignant conditions represented 35.4% of cases, mainly reactive marrow changes (17.5%) and megaloblastic anemia (7.2%) being the most frequent. Most patients were aged 41–60 years (29.9%), with a slight male predominance (52.9%). Geographically, most cases originated from River Nile State (52.9%) and Khartoum State (33%). A notable proportion of patients were unemployed (58.8%), suggesting socioeconomic vulnerability. Conclusion: There is high burden of advanced hematological malignancies and reactive marrow patterns likely due to delayed access to care during conflict. Bone marrow examination remains essential diagnostic tool in resource-limited settings. Strengthening mobile diagnostic services, promoting early screening among high-risk groups—particularly the elderly and unemployed—and implementing micronutrient supplementation programs may help reduce morbidity and improve outcomes in conflict-affected populations.
VL - 14
IS - 2
ER -
Copy
|
Download