Introduction: Newborn jaundice looks in most neonates as “physiological jaundice” in the first limited weeks of life; nevertheless, pathological jaundice is linked with an enlarged hazard of long-term difficulties and death. Only a limited investigation has been done on the predictors of newborn jaundice in Ethiopia. The objective of this investigation was to distinguish the predictors of newborn jaundice among neonates admitted to Ameya primary hospitals. Objectives: To evaluate incidence and its predicators of Neonatal Jaundice amongst Admitted Neonates at Ameya Primary Hospital, South West Shoa Zone, Ethiopia, 2025. Methods: An institutional-based; Retrospective follow-up research design was conducted amongst 414 of neonates. Simple random sampling methods was used to choose study participants. Epidata version 4.62 was used for data entry then exported to STATA version 14.1. Study variables with p-values < 0.25 were moved to multivariable Cox regression models. Adjusted odd ratio with 95% confidence interval was calculated, and the p-value < 0.05 was considered statistically significant in the multivariable model. The findings were stated using text, table and graphs. Results: A data were gathered from 414 and 407 neonates had completed information giving the response rate of 98.3%. The total incidence rate of jaundice among neonates was 20.12 per 1000 person-days (95% CI: 15.33-26.41). Male neonates 2.43 [AHR= 2.43; 95% CI (1.21-4.89, 37-42 weeks of gestational age was 2.8 [AHR = 2.8; 95% CI (1.47-5.36], premature rapture of membrane (PROM) was 2.33 [AHR= 2.33; 95% CI (1.27-4.28)], duration of labor 2.44 [AHR = 2.44; 95% CI (1.275-4.67)] labor onset 3.25 [AHR = 3.25; 95% CI (1.68-6.28)] were predictors. Conclusion and Recommendation: The incidence of jaundice was relatively high in current study than the result of the prior one. Male neonates, prolonged duration of labor, gestational age, premature rapture of membrane (PROM) and labor onset were the significant predictors. Henceforth, an effort has to be considered to reduce the incidence of newborn jaundice via enlightening newborn care and timely interfering meant for neonates with premature rapture of membrane and birth at a elongated period of time as well as the newborn born from induced labor.
| Published in | Science Development (Volume 6, Issue 3) |
| DOI | 10.11648/j.scidev.20250603.28 |
| Page(s) | 197-206 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Neonatal Jaundice, Incidence, Predictor, Ameya Primary Hospital, Ethiopia
Variables | CI | Power | P | HR | Sample Size with 10% withdraw and loss to follow-up | Reference |
|---|---|---|---|---|---|---|
95% | 80% | |||||
Duration of labor | 95% | 80% | 13.04 | 3.5 | 90 | [ 15] |
Sepsis | 95% | 80% | 15.38 | 2.6 | 130 | [ 15] |
Variables | Variables Category | Outcome | Total, N (%) | NDO | IDR per 1000 NDO | |
|---|---|---|---|---|---|---|
Died, N (%) | Censored, N (%) | |||||
Genders of neonates | Male | 38(19.2%) | 160(80.8%) | 198(48.6%) | 1289 | 29.48 |
Female | 14(6.7%) | 195(93.3%) | 209(51.4%) | 1295 | 10.81 | |
Gestational age | <37 | 38(19.2%) | 160(80.8%) | 198(48.6%) | 1247 | 30.47 |
37-42 | 14(6.7%) | 195(93.3%) | 209(51.4%) | 1337 | 10.47 | |
Birth weight (kg) | <2.5 | 51(14.3%) | 305(85.7%) | 356(87.5%) | 2226 | 22.91 |
=>2.5 | 1(2.0%) | 50(98.0%) | 51(12.5%) | 358 | 2.79 | |
Five-minute APGAR score | ≤6 | 27(17.8%) | 125(82.2%) | 152(37.3%) | 986 | 27.38 |
7=10 | 25(9.8%) | 230(90.2%) | 255(62.7%) | 1598 | 15.64 | |
Family history of jaundice | No | 28(11.3%) | 219(88.7%) | 247(59.7%) | 1525 | 18.36 |
Yes | 24(14.4%) | 143(85.6%) | 167(40.3%) | 1059 | 22.66 | |
Birth trauma | No | 33(10.1%) | 293(89.9%) | 326(80.1%) | 2065 | 15.98 |
Yes | 19(23.5%) | 62(76.5%) | 81(19.9%) | 522 | 36.39 | |
Neonatal sepsis | No | 29(9.1%) | 288(90.9%) | 317(77.9%) | 2045 | 14.18 |
Yes | 23(25.6%) | 67(74.4%) | 90(22.1%) | 539 | 23.54 | |
Variables | Variables Category | Outcome | Total, N (%) | NDO | IDR per 1000 NDO | |
|---|---|---|---|---|---|---|
Died, N (%) | Censored, N (%) | |||||
Blood group | A | 5(10.0%) | 45(90.0%) | 50(12.1%) | 321 | 15.58 |
B | 4(3.3%) | 119(96.7%) | 123(29.7%) | 757 | 5.28 | |
AB | 11(8.8%) | 114(91.2%) | 125(30.2%) | 760 | 14.47 | |
O | 32(27.6%) | 84(72.4%) | 116(28.0%) | 746 | 43 | |
RH factor | Negative | 6(30.0%) | 14(70.0%) | 20(4.8%) | 114 | 52.63 |
Positive | 46(11.7%) | 348(96.1%) | 394(95.2%) | 2470 | 18.62 | |
Parity | Single | 21(9.1%) | 210(90.9%) | 231(56.8%) | 1486 | 14.13 |
Multiple | 31(17.6%) | 145(82.4%) | 176(43.2%) | 1098 | 28.23 | |
Premature rapture of membrane | No | 21(7.1%) | 275(92.9%) | 296(72.7%) | 1860 | 11.29 |
Yes | 31(27.9%) | 80(72.1%) | 111(27.3%) | 724 | 42.82 | |
ANC follow-up | No | 17(21.5%) | 62(78.5%) | 79(19.4%) | 485 | 30.05 |
Yes | 35(10.7%) | 293(89.3%) | 328(80.6%) | 2099 | 16.67 | |
Gestational diabetes mellitus | Yes | 33(12.1%) | 240(87.9%) | 273(65.9%) | 1704 | 19.36 |
No | 19(13.5%) | 122(86.5%) | 141(34.1%) | 886 | 21.59 | |
Mode of delivery | Spontaneous vaginal delivery | 24(10.6%) | 203(89.4%) | 227(54.8%) | 1395 | 17.2 |
Instrumental delivery | 20(14.2%) | 121(85.8%) | 141(34.1%) | 877 | 22.8 | |
caesarean section | 8(17.4%) | 38(82.6%) | 46(11.1%) | 312 | 25.64 | |
Gestational hypertension | No | 48(12.1%) | 348(87.9%) | 396(95.7%) | 2479 | 19.36 |
Yes | 4(22.2%) | 14(77.8%) | 18(4.3%) | 105 | 38.09 | |
Obstetrics complication | Yes | 44(12.9%) | 298(87.1%) | 342(82.6%) | 2139 | 20.57 |
No | 8(11.1%) | 64(88.9%) | 72(17.4%) | 445 | 17.97 | |
Duration of labor | Prolonged | 28(36.4%) | 49(63.6%) | 77(18.9%) | 478 | 58.57 |
Normal | 24(7.3%) | 306(92.7%) | 330(81.1%) | 2106 | 11.39 | |
Onset of labor | Spontaneous | 24(7.5%) | 298(92.5%) | 322(79.1%) | 2069 | 11.6 |
Induced | 28(32.9%) | 57(67.1%) | 85(20.9%) | 515 | 54.37 | |
Variables | Log-rank (χ2) | p-Value |
|---|---|---|
Genders of neonates | 15.42 | 0.0001 |
Gestational age | 13.01 | 0.0003 |
Birth weight (kg) | 10.67 | 0.0011 |
Five-minute APGAR score | 4.44 | 0.0351 |
Birth trauma | 7.56 | 0.0060 |
Neonatal sepsis | 17.87 | 0.00001 |
Parity | 6.74 | 0.0094 |
Premature rapture of membrane (PROM) | 20.38 | 0.00001 |
ANC follow-up | 5.97 | 0.0146 |
Duration of labor | 32.17 | 0.00001 |
Onset of labor | 31.48 | 0.00001 |
Variables | Variables Category | Outcome | CHR (CI 95%) | P-value | AHR (CI 95%) | P-value | |
|---|---|---|---|---|---|---|---|
Died, N (%) | Censored, N (%) | ||||||
Genders of neonates | Male | 38(19.2%) | 160(80.8%) | 3.365(1.73-6.55) | 0.0001 | 2.43(1.21-4.89) | 0.013* |
Female | 14(6.7%) | 195(93.3%) | 1 | 1 | |||
Gestational age | <37 | 38(19.2%) | 160(80.8%) | 1 | 1 | ||
37-42 | 14(6.7%) | 195(93.3%) | 2.89(1.56-5.32) | 0.0003 | 2.8(1.47-5.36) | 0.002* | |
Birth weight (kg) | <2.5 | 51(14.3%) | 305(85.7%) | 9.14(1.26-66.21) | 0.0011 | 4.85(0.66-35.9) | 0.122 |
=>2.5 | 1(2.0%) | 50(98.0%) | 1 | 1 | |||
Five-minute APGAR score | ≤6 | 27(17.8%) | 125(82.2%) | 1.79(1.04-3.10) | 0.0351 | 1.65(0.92-2.97) | 0.092 |
7=10 | 25(9.8%) | 230(90.2%) | 1 | 1 | |||
Birth trauma | No | 33(10.1%) | 293(89.9%) | 1 | 1 | ||
Yes | 19(23.5%) | 62(76.5%) | 2.3(1.31-4.04) | 0.0060 | 0.86(0.43-1.72) | 0.668 | |
Neonatal sepsis | No | 29(9.1%) | 288(90.9%) | 1 | 1 | ||
Yes | 23(25.6%) | 67(74.4%) | 3.5(2.01-6.08) | 0.00001 | 1.79(0.88-3.66) | 0.110 | |
Parity | Singe | 21(9.1%) | 210(90.9%) | 1 | 1 | ||
Multiple | 31(17.6%) | 145(82.4%) | 2.06(1.19-3.6) | 0.0094 | 1.24(0.66-2.32) | 0.508 | |
Premature rapture of membrane (PROM) | No | 21(7.1%) | 275(92.9%) | 1 | 1 | ||
Yes | 31(27.9%) | 80(72.1%) | 3.55(2.04-6.18) | 0.00001 | 2.33(1.27-4.28) | 0.006* | |
ANC follow-up | No | 17(21.5%) | 62(78.5%) | 2.14(1.2-3.82) | 0.0146 | 0.86(0.44-1.69) | 0.658 |
Yes | 35(10.7%) | 293(89.3%) | 1 | 1 | |||
Duration of labor | Prolonged | 28(36.4%) | 49(63.6%) | 5.1(2.95-8.79) | 0.00001 | 2.44(1.275-4.67) | 0.007* |
Normal | 24(7.3%) | 306(92.7%) | 1 | 1 | |||
Onset of labor | Spontaneous | 24(7.5%) | 298(92.5%) | 1 | 1 | ||
Induced | 28(32.9%) | 57(67.1%) | 5(2.9-8.63) | 0.00001 | 3.25(1.68-6.28) | 0.0001* | |
ANC | Antenatal Care |
NICU | Neonatal Intensive Care Unit |
PROM | Premature Rapture of Member |
| [1] | Richard A PC. Lippincott’s Illustrated Review of Biochemistry. New York: Lippincott Williams & Wilkin’s. 2011. |
| [2] | Mitra S RJ. Neonatal jaundice: aetiology, diagnosis and treatment; 78(12): 699-704.. Br J Hosp Med. 2017; from: |
| [3] | Ullah S, Rahman K HM. Hyperbilirubinemia in neonates: types, causes, clinical examinations, preventive measures and treat- ments: a narrative review article. 45(5): 558. Iran J Public Heal. 2016; 32(2): 261-8. |
| [4] |
Brobby NAW et al. ‘Outcomes of neonatal hyperbilirubinemia and associated factors at a tertiary hospital in Ghana’, BMC Pediatrics, 25(1). Available at:
https://doi.org/10.1186/s12887-025-05618-4 BMC Pediatr 25(1). 2025. |
| [5] | Tampubolon CH, Bagus I, Utama E, Pasaribu R. Description of Risk Factors Affecting Neonatal Jaundice. 2024; 9 (December): 175-84. |
| [6] | UNICEF. Neonatal mortality rate. 2024; |
| [7] | Demographic M, Survey H. Mini Demographic and Health Survey 2019. 2019. |
| [8] | Nations U. Transforming our world: the 2030 agenda for sustainable development. 2020; |
| [9] | Scrafford CG, Mullany LC, Katz J et al. Incidence of and risk factors for neonatal jaundice among newborns in southern Nepal. Trop Med Int Heal. 2013; 2 (September). |
| [10] | Gurley ES, Halder AK, Streatfield PK et al. Estimating the burden of maternal and neonatal deaths associated with jaundice in Bangladesh: possible role of hepatitis E infection. Am J Public Health. 2012. |
| [11] | Tette EM, Nartey ET, Nuertey BD et al. The pattern of neonatal admissions and mortality at a regional and district hospital in the Upper West Region of Ghana; a cross sectional study. 2020. PLoS One. 2020; Available from: |
| [12] | Berhe F, Gebreegziabher L, Mihretu HG, Berhe AH. Prevalence and Factors Associated with Neonatal Mortality at Ayder Comprehensive Specialized Hospital, Northern Ethiopia. A Cross-Sectional. 2020; 29-37. |
| [13] | Mohamed HA, Shiferaw Z, Kedir A, Id R, Id AK. Neonatal mortality and associated factors among neonates admitted to neonatal intensive care unit at public hospitals of Somali Regional State, Eastern Ethiopia : A multicenter retrospective analysis. 2022; 22(Ci): 1-16. Available from: http://dx.doi.org/10.1371/journal.pone.0268648 |
| [14] | Thomas G, Demena M, Hawulte B, Eyeberu A, Heluf H. Neonatal Mortality and Associated Factors Among Neonates Admitted to the Neonatal Intensive Care Unit of Dil Chora Referral Hospital, Dire Dawa City, Ethiopia, 2021 : A Facility-Based Study. 2022; 9(February): 1-7. |
| [15] | Birhanu MY, Workineh AA, Molla Y, Abebaw E, Arora A, Bazezew Y. Rate and predictors of neonatal jaundice in northwest Ethiopia: Prospective cohort study. J Multidiscip Healthc. 2021; 14: 447-57. |
| [16] | Sisay BD, Abebe RF, Kassie AA, Wondimu MG, Kassie GA. Determinants of neonatal jaundice among neonates admitted to neonatal intensive care unit in public hospitals of Sidama Region, Sidama, Ethiopia, 2022: an unmatched case-control study. Pan Afr Med J. 2023; 45. |
| [17] | Ayalew T, Molla A, Kefale B, Alene TD, Abebe GK, Ngusie HS, et al. Factors associated with neonatal jaundice among neonates admitted at referral hospitals in northeast Ethiopia: a facility-based unmatched case-control study. BMC Pregnancy Childbirth. 2024; 24(1): 1-10. |
| [18] | Bante A, Ahmed M, Degefa N, Shibiru S, Yihune M. Neonatal jaundice and associated factors in public hospitals of southern Ethiopia: A multi-center cross-sectional study. Heliyon. 2024; 10(2): e24838. Available from: |
| [19] | Ethiopia FM of H of. Neonatal Intensive Care Unit (NICU) Training Management Protocol. 2021; (November). |
| [20] | Asaye S, Bekele M, Getachew A, Fufa D, Adugna T, Tadasa E. Hyperbilirubinemia and Associated Factors Among Neonates Admitted to the Neonatal Care Unit in Jimma Medical Center. Clin Med Insights Pediatr. 2023; 17. |
| [21] | Azzuqa A WJ. Bilirubin concentrations in jaundiced neo- nates with conjunctival icterus. J Pediatr. 2016. |
| [22] | Tessema M, Mekonnen H, Alemu T, Godie Y, Teklehaimanot WZ, Mengstie LA. Magnitude and its associated factors of neonatal jaundice among neonates admitted to the neonatal intensive care unit of Dessie Town public hospitals, Amhara region, Ethiopia, 2020: a multicenter cross-sectional study. Front Pediatr. 2024; 12(January): 1-8. |
APA Style
Chuko, B. M., Kibrat, F. A., Taye, N., Takele, G., Edea, G., et al. (2025). Incidence and Its Predicators of Neonatal Jaundice Among Admitted Neonates at Ameya Primary Hospital, South West Shoa Zone, Ethiopia, 2025. Science Development, 6(3), 197-206. https://doi.org/10.11648/j.scidev.20250603.28
ACS Style
Chuko, B. M.; Kibrat, F. A.; Taye, N.; Takele, G.; Edea, G., et al. Incidence and Its Predicators of Neonatal Jaundice Among Admitted Neonates at Ameya Primary Hospital, South West Shoa Zone, Ethiopia, 2025. Sci. Dev. 2025, 6(3), 197-206. doi: 10.11648/j.scidev.20250603.28
@article{10.11648/j.scidev.20250603.28,
author = {Bacha Merga Chuko and Fikru Assefa Kibrat and Nebiyu Taye and Girum Takele and Geda Edea and Zufela Sime},
title = {Incidence and Its Predicators of Neonatal Jaundice Among Admitted Neonates at Ameya Primary Hospital, South West Shoa Zone, Ethiopia, 2025
},
journal = {Science Development},
volume = {6},
number = {3},
pages = {197-206},
doi = {10.11648/j.scidev.20250603.28},
url = {https://doi.org/10.11648/j.scidev.20250603.28},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.scidev.20250603.28},
abstract = {Introduction: Newborn jaundice looks in most neonates as “physiological jaundice” in the first limited weeks of life; nevertheless, pathological jaundice is linked with an enlarged hazard of long-term difficulties and death. Only a limited investigation has been done on the predictors of newborn jaundice in Ethiopia. The objective of this investigation was to distinguish the predictors of newborn jaundice among neonates admitted to Ameya primary hospitals. Objectives: To evaluate incidence and its predicators of Neonatal Jaundice amongst Admitted Neonates at Ameya Primary Hospital, South West Shoa Zone, Ethiopia, 2025. Methods: An institutional-based; Retrospective follow-up research design was conducted amongst 414 of neonates. Simple random sampling methods was used to choose study participants. Epidata version 4.62 was used for data entry then exported to STATA version 14.1. Study variables with p-values Results: A data were gathered from 414 and 407 neonates had completed information giving the response rate of 98.3%. The total incidence rate of jaundice among neonates was 20.12 per 1000 person-days (95% CI: 15.33-26.41). Male neonates 2.43 [AHR= 2.43; 95% CI (1.21-4.89, 37-42 weeks of gestational age was 2.8 [AHR = 2.8; 95% CI (1.47-5.36], premature rapture of membrane (PROM) was 2.33 [AHR= 2.33; 95% CI (1.27-4.28)], duration of labor 2.44 [AHR = 2.44; 95% CI (1.275-4.67)] labor onset 3.25 [AHR = 3.25; 95% CI (1.68-6.28)] were predictors. Conclusion and Recommendation: The incidence of jaundice was relatively high in current study than the result of the prior one. Male neonates, prolonged duration of labor, gestational age, premature rapture of membrane (PROM) and labor onset were the significant predictors. Henceforth, an effort has to be considered to reduce the incidence of newborn jaundice via enlightening newborn care and timely interfering meant for neonates with premature rapture of membrane and birth at a elongated period of time as well as the newborn born from induced labor.},
year = {2025}
}
TY - JOUR T1 - Incidence and Its Predicators of Neonatal Jaundice Among Admitted Neonates at Ameya Primary Hospital, South West Shoa Zone, Ethiopia, 2025 AU - Bacha Merga Chuko AU - Fikru Assefa Kibrat AU - Nebiyu Taye AU - Girum Takele AU - Geda Edea AU - Zufela Sime Y1 - 2025/08/15 PY - 2025 N1 - https://doi.org/10.11648/j.scidev.20250603.28 DO - 10.11648/j.scidev.20250603.28 T2 - Science Development JF - Science Development JO - Science Development SP - 197 EP - 206 PB - Science Publishing Group SN - 2994-7154 UR - https://doi.org/10.11648/j.scidev.20250603.28 AB - Introduction: Newborn jaundice looks in most neonates as “physiological jaundice” in the first limited weeks of life; nevertheless, pathological jaundice is linked with an enlarged hazard of long-term difficulties and death. Only a limited investigation has been done on the predictors of newborn jaundice in Ethiopia. The objective of this investigation was to distinguish the predictors of newborn jaundice among neonates admitted to Ameya primary hospitals. Objectives: To evaluate incidence and its predicators of Neonatal Jaundice amongst Admitted Neonates at Ameya Primary Hospital, South West Shoa Zone, Ethiopia, 2025. Methods: An institutional-based; Retrospective follow-up research design was conducted amongst 414 of neonates. Simple random sampling methods was used to choose study participants. Epidata version 4.62 was used for data entry then exported to STATA version 14.1. Study variables with p-values Results: A data were gathered from 414 and 407 neonates had completed information giving the response rate of 98.3%. The total incidence rate of jaundice among neonates was 20.12 per 1000 person-days (95% CI: 15.33-26.41). Male neonates 2.43 [AHR= 2.43; 95% CI (1.21-4.89, 37-42 weeks of gestational age was 2.8 [AHR = 2.8; 95% CI (1.47-5.36], premature rapture of membrane (PROM) was 2.33 [AHR= 2.33; 95% CI (1.27-4.28)], duration of labor 2.44 [AHR = 2.44; 95% CI (1.275-4.67)] labor onset 3.25 [AHR = 3.25; 95% CI (1.68-6.28)] were predictors. Conclusion and Recommendation: The incidence of jaundice was relatively high in current study than the result of the prior one. Male neonates, prolonged duration of labor, gestational age, premature rapture of membrane (PROM) and labor onset were the significant predictors. Henceforth, an effort has to be considered to reduce the incidence of newborn jaundice via enlightening newborn care and timely interfering meant for neonates with premature rapture of membrane and birth at a elongated period of time as well as the newborn born from induced labor. VL - 6 IS - 3 ER -
Department of Maternity and Neonatology, Ameya Primary Hospital, Waliso, Ethiopia
Department of Anesthesia, Waliso General Hospital, Waliso, Ethiopia
Department of Laboratory, Waliso Health Center, Waliso, Ethiopia
Department of Pharmacy, Waliso Health Center, Waliso, Ethiopia
Department of Nursing, Ambo University, Ambo, Ethiopia
Department of Midwifery, Waliso General Hospital, Waliso, Ethiopia
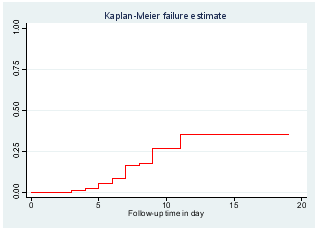
Figure 1. Kaplan Meier survival estimate of cumulative failure status of the jaundice neonates during follow- up time at Ameya Primary Hospital, Ethiopia, 2025.
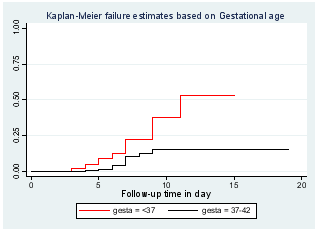
Figure 2. Kaplan Meier survival estimate neonatal jaundice based on gestational age at Ameya Primary Hospital, Ethiopia, 2025.
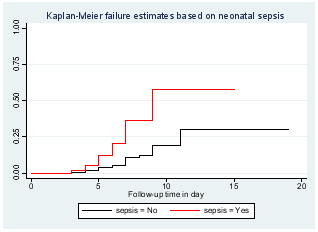
Figure 3. Kaplan Meier survival estimate neonatal jaundice based on neonatal sepsis at Ameya Primary Hospital, Ethiopia, 2025.
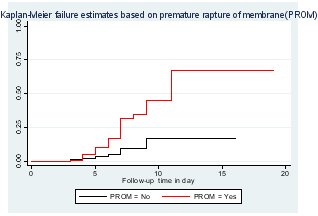
Figure 4. Kaplan Meier survival estimate neonatal jaundice based on PROM at Ameya Primary Hospital, Ethiopia, 2025.
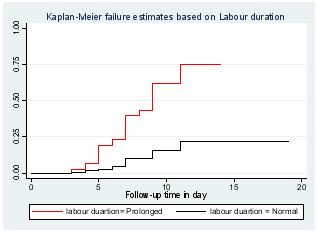
Figure 5. Kaplan Meier survival estimate neonatal jaundice based on labor duration at Ameya Primary Hospital, Ethiopia, 2025.
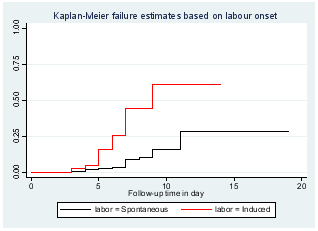
Figure 6. Kaplan Meier survival estimate neonatal jaundice based on labor onset at Ameya Primary Hospital, Ethiopia, 2025.
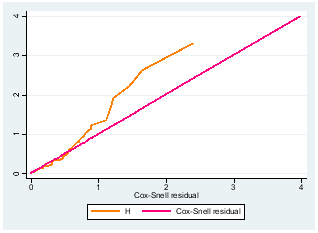
Figure 7. Test of goodness of fitting of the model by Cox-Snell residual Nelson-Alen cumulative hazard plot.
Information

