Street foods constitute an essential component of urban food access in Guyana. Yet, empirical evidence on consumer food safety knowledge remains scarce, with existing research focused mainly on street food vendors. This study assessed consumer food safety knowledge in Demerara-Mahaica, Guyana, and examined demographic factors associated with high knowledge. A cross-sectional survey was conducted among 104 consumers using a structured questionnaire comprising demographic characteristics and 18 food safety knowledge items. Knowledge scores were derived from correct responses and categorized into low, moderate, and high levels. Descriptive analyses summarized overall and item-level knowledge, while Chi-square tests and odds ratios examined associations between knowledge and demographic variables. A multivariable binary logistic regression model was fitted to identify independent predictors of high food safety knowledge. Overall, most consumers demonstrated moderate food safety knowledge, with persistent deficiencies in technical and pathogen-related concepts despite relatively strong awareness of general hygiene practices. Item-level analyses showed significant associations between overall knowledge classification and understanding of microbial contamination, foodborne pathogens, reheating risks, and adverse health outcomes linked to foodborne disease. Bivariate analyses revealed no statistically significant associations between knowledge level and gender, age group, ethnicity, or place of education. In the multivariable model, educational attainment emerged as the only statistically significant independent predictor of high food safety knowledge (adjusted OR = 2.35), while age showed a positive but borderline association. The modest explanatory power of the model (8.8%, Cox & Snell R², and 12.4% Nagelkerke R²) suggests that factors beyond basic demographics alone shape consumer food safety knowledge. These findings indicate that improving consumer food safety in Guyana will require targeted, context-specific education to address technical knowledge gaps, implemented alongside vendor training, infrastructure support, and regulatory measures within informal food systems.
| Published in | Science Journal of Public Health (Volume 14, Issue 2) |
| DOI | 10.11648/j.sjph.20261402.14 |
| Page(s) | 80-91 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Consumer Food Safety, Food Safety Knowledge, Street Foods, Informal Food Sector, Public Health, Demerara-Mahaica, Guyana
Questionnaire Items | Options | Response n (%) | |
|---|---|---|---|
D1 | Gender | Male | 56 (53.8%) |
Female | 48 (46.2%) | ||
D2 | Age | 18-25 | 26 (25.0%) |
26-35 | 33 (31.7%) | ||
36-45 | 23 (22.1%) | ||
46-55 | 15 (14.4%) | ||
56-60 | 6 (5.8%) | ||
>60 | 1 (1.0%) | ||
D3 | Ethnicity | African | 50 (48.1%) |
Mixed | 28 (26.9%) | ||
East Indian | 17 (16.3%) | ||
Amerindians | 2 (1.9%) | ||
Spanish | 7 (6.7%) | ||
D4 | Education | Nursery | 1 (1.0%) |
Primary | 7 (6.7%) | ||
Secondary | 62 (59.6%) | ||
University | 34 (32.7%) | ||
D5 | Did you receive this education in Guyana? | No | 13 (12.5%) |
Yes | 91 (87.5%) | ||
Questionnaire Items | Response n (%) | |||
|---|---|---|---|---|
Yes | No | Don’t Know | ||
K1 | Abortion in pregnant women can be induced by a food-borne disease. | 52 (50.0%) | 26 (25.0%) | 26 (25.0%) |
K2 | Bloody diarrhea can be transmitted by food. [1 missing] | 78 (75.7%) | 10 (9.7%) | 15 (14.6%) |
K3 | Swollen cans can contain microorganisms. | 74 (71.2%) | 12 (11.5%) | 18 (17.3%) |
K4 | During infectious disease of the skin, it is necessary to take leave from work. | 92 (88.5%) | 8 (7.7%) | 4 (3.8%) |
K5 | Eating and drinking in the work place increase the risk of food contamination. | 67 (64.4%) | 31 (29.8%) | 6 (5.8%) |
K6 | Hepatitis A virus is a foodborne pathogen. | 33 (31.7%) | 19 (18.3%) | 52 (50.0%) |
K7 | Microbes are in the skin, nose and mouth of healthy food handlers. [1 missing] | 71 (68.9%) | 9 (8.7%) | 23 (22.3%) |
K8 | Salmonella is among the food-borne pathogens. | 59 (56.7%) | 8 (7.7%) | 37 (35.6%) |
K9 | Staphylococcus is among the food-borne pathogens. | 45 (43.3%) | 8 (7.7%) | 51 (49.0%) |
K10 | Influenza can be transmitted by aerosols rather than food. | 73 (70.2%) | 13 (12.5%) | 18 (17.3%) |
K11 | Using gloves while handling food reduces the risk of food contamination. | 94 (90.4%) | 9 (8.7%) | 1 (1.0%) |
K12 | Washing hands before work reduces the risk of food contamination. | 101 (97.1%) | 2 (1.9%) | 1 (1.0%) |
K13 | AIDS can be transmitted by food. | 18 (17.3%) | 62 (59.6%) | 24 (23.1%) |
K14 | Children, healthy adults, pregnant women, and older individuals are at equal risk for food poisoning. | 82 (78.8%) | 13 (12.5%) | 9 (8.7%) |
K15 | Food prepared in advance reduces the risk of food contamination. | 35 (33.7%) | 53 (51.0%) | 16 (15.4%) |
K16 | Proper cleaning and sanitization of utensils decreases the risk of food contamination. | 95 (91.3%) | 7 (6.7%) | 2 (1.9%) |
K17 | Reheating cooked foods can contribute to food contamination. | 59 (56.7%) | 32 (30.8%) | 13 (12.5%) |
K18 | Washing utensils with detergent leaves them free of contamination. | 68 (65.4%) | 31 (29.8%) | 5 (4.8%) |
Knowledge item | Exp. Val. Assumption Satisfied | Pearson Chi-Square (P-value) |
|---|---|---|
K1 | Yes | 0.001 |
K3 | Yes | 0.000 |
K6 | Yes | 0.000 |
K7 | Yes | 0.013 |
K8 | Yes | 0.003 |
K9 | Yes | 0.015 |
K10 | Yes | 0.002 |
K17 | Yes | 0.027 |
KAP | Knowledge, Attitude, and Practice |
ORs | Odds Ratio |
| [1] | K. Abrahale, S. Sousa, G. Albuquerque, P. Padrão, and N. Lunet, “Street food research worldwide: a scoping review,” Journal of Human Nutrition and Dietetics, vol. 32, no. 2, pp. 152-174, Oct. 2018, |
| [2] | Md. Khairuzzaman, F. M. Chowdhury, S. Zaman, A. Al Mamun, and Md. L. Bari, “Food Safety Challenges towards Safe, Healthy, and Nutritious Street Foods in Bangladesh,” International Journal of Food Science, vol. 2014, pp. 1-9, Apr. 2014, |
| [3] | N. P. Steyn et al., “Nutritional contribution of street foods to the diet of people in developing countries: a systematic review,” Public Health Nutrition, vol. 17, no. 6, pp. 1363-1374, May 2013, |
| [4] | N. P. Steyn, D. Labadarios, and J. H. Nel, “Factors which influence the consumption of street foods and fast foods in South Africa-a national survey,” Nutrition Journal, vol. 10, no. 1, Oct. 2011, |
| [5] | B. S. Namugumya and C. Muyanja, “Contribution of street foods to the dietary needs of street food vendors in Kampala, Jinja and Masaka districts, Uganda,” Public Health Nutrition, vol. 15, no. 8, pp. 1503-1511, Oct. 2011, |
| [6] | T. A. Tamenu Abera and M. A. Mogessie Ashenafi, “Food access vs food safety: The case of street food operation around Mexico Square, Addis Ababa, Ethiopia,” SINET: Ethiopian Journal of Science, vol. 46, no. 2, pp. 176-187, Nov. 2023, |
| [7] | J. Hill, Z. Mchiza, T. Puoane, and N. P. Steyn, “The development of an evidence-based street food vending model within a socioecological framework: A guide for African countries,” PLOS ONE, vol. 14, no. 10, pp. 152-174, Oct. 2019, |
| [8] | T. W. Bereda, Y. M. Emerie, M. A. Reta, and H. S. Asfaw, “Microbiological Safety of Street Vended Foods in Jigjiga City, Eastern Ethiopia,” Ethiopian Journal of Health Sciences, vol. 26, no. 2, p. 161, Mar. 2016, |
| [9] | K. Alem, “Bacterial Load Assessment of some Food Items Sold in Street in Woldia Town, North-East Ethiopia,” Journal of Pure and Applied Microbiology, vol. 14, no. 3, pp. 1845-1854, Sep. 2020, |
| [10] | B. J. Birgen, L. G. Njue, D. M. Kaindi, F. O. Ogutu, and J. O. Owade, “Determinants of Microbial Contamination of Street-Vended Chicken Products Sold in Nairobi County, Kenya,” International Journal of Food Science, vol. 2020, pp. 1-8, Feb. 2020, |
| [11] | B. J. Birgen, L. G. Njue, D. M. Kaindi, and F. O. Ogutu, “Qualitative Risk Assessment of Campylobacter jejuni in Street Vended Poultry in Informal Settlements of Nairobi County,” European Journal of Nutrition & Food Safety, pp. 28-37, Nov. 2019, |
| [12] | C. Muyanja, L. Nayiga, N. Brenda, and G. Nasinyama, “Practices, knowledge and risk factors of street food vendors in Uganda,” Food Control, vol. 22, no. 10, pp. 1551-1558, Oct. 2011, |
| [13] | B. Huynh-Van et al., “Factors associated with food safety compliance among street food vendors in Can Tho city, Vietnam: implications for intervention activity design and implementation,” BMC Public Health, vol. 22, no. 1, Jan. 2022, |
| [14] | J. K. Hassan and L. W. T. Fweja, “Food Hygienic Practices and Safety Measures among Street Food Vendors in Zanzibar Urban District,” eFood, vol. 1, no. 4, pp. 332-338, Feb. 2020, |
| [15] | J. Mwove, S. Imathiu, I. Orina, and P. Karanja, “Multinomial Logistic Regression Analysis of Factors Influencing Food Safety, Hygiene Awareness and Practices Among Street Food Vendors in Kiambu County, Kenya.,” Current Research in Nutrition and Food Science Journal, vol. 8, no. 3, pp. 988-1000, Dec. 2020, |
| [16] | L. Ma, H. Chen, H. Yan, L. Wu, and W. Zhang, “Food safety knowledge, attitudes, and behavior of street food vendors and consumers in Handan, a third tier city in China,” BMC Public Health, vol. 19, no. 1, Aug. 2019, |
| [17] | A. T. L. Nguyen et al., “Customers’ Knowledge, Attitude, and Practices towards Food Hygiene and Safety Standards of Handlers in Food Facilities in Hanoi, Vietnam,” International Journal of Environmental Research and Public Health, vol. 15, no. 10, p. 2101, Sep. 2018, |
| [18] | Md. H. Rahman, Md. M. Hasan, Md. K. Masud, Md. Moniruzzaman, S. Singha, and Md. S. Palash, “Exploring Consumer Perceptions and Value Addition in Street Cuisine: A Case of Kalai Ruti,” Asian journal of economics, business and accounting, vol. 24, no. 6, pp. 107-119, May 2024, |
| [19] | T. T. A. Ngoc, N. T. M. Hang, D. K. Thanh, and L. V. Hoa, “Evaluation of microbial safety knowledge, attitude and practice of street food vendors and consumers in Can Tho City, Vietnam,” Food Research, vol. 4, no. 5, pp. 1802-1814, Jul. 2020, |
| [20] | S. Mamun, S. Alam, M. A. Zaher, and A. O. Huq, “Food Safety Knowledge, Attitudes and Behavior of Street Food Vendors and Consumers in Dhaka City,” Bangladesh Journal of Microbiology, vol. 37, no. 2, pp. 48-51, Dec. 2020, |
| [21] | N. A. Elsahoryi, A. Olaimat, H. Abu Shaikha, B. Tabib, and R. Holley, “Food safety knowledge, attitudes and practices (KAP) of street vendors: a cross-sectional study in Jordan,” British Food Journal, vol. 126, no. 11, pp. 3870-3887, Oct. 2024, |
| [22] | L. A. Alhashim et al., “Food Safety Knowledge and Attitudes: A Cross-Sectional Study among Saudi Consumers from Food Trucks Owned by Productive Families,” International Journal of Environmental Research and Public Health, vol. 19, no. 7, p. 4322, Apr. 2022, |
| [23] | O. T. Oladipo‐Adekeye and F. T. Tabit, “The Food Safety Knowledge of Street Food Vendors and the Sanitary Compliance of Their Vending facilities, Johannesburg, South Africa,” Journal of Food Safety, vol. 41, no. 4, May 2021, |
| [24] | T. G. Nguyen Thi, K. Le Tri, T. Hoang Chi, T. Luu Quoc, and T. Hoang Minh, “Food-safety knowledge, attitudes and practices of street-vended food sellers in the city of Kontum, 2018,” Heavy metals and arsenic concentrations in water, agricultural soil, and rice in Ngan Son district, Bac Kan province, Vietnam, vol. 2, no. 3, pp. 90-97, Sep. 2019, |
| [25] | P. J. Letuka, “Nutrition knowledge and attitudes of street food handlers in Mangaung Metro Municipality in free state, South Africa,” Environment social psychology, vol. 9, no. 5, Feb. 2024, |
| [26] | A. H. Subratty, P. Beeharry, and M. Chan Sun, “A survey of hygiene practices among food vendors in rural areas in Mauritius,” Nutrition & Food Science, vol. 34, no. 5, pp. 203-205, Oct. 2004, |
| [27] | O. O. Akinbule, I. H. Omonhinmin, C. A. Oladoyinbo, and A. T. Omidiran, "Food safety and hygiene practice of street food vendors in federal university of agriculture, Abeokuta", Journal of Natural Sciences Engineering and Technology, vol. 18, no. 1, pp. 176-186, Oct. 2020, |
| [28] | R. K. Edeme and N. Nkalu C., “Operations of Street Food Vendors and Their Impact on Sustainable Life in Rural Nigeria,” American Economic & Social Review, vol. 4, no. 1, pp. 1-7, Nov. 2018, |
| [29] | O. W. Alawode and F. T. Tabit, “An Investigation Into the Enforcement and Compliance of Food Safety Regulations at Street Food Vending Sites in Oyo State, Nigeria,” Environmental Health Insights, vol. 19, Oct. 2025, |
| [30] | R. Tayco, V. Cañete, J. D. Bulfa, A. M. Ege, Ellah Noblefranca, and M. A. Remollo, “Assessing Food Safety Knowledge, Attitudes, and Practices of Street Food Vendors,” Journal of interdisciplinary perspectives, vol. 3, no. 7, pp. 376-387 Jun. 2025, |
| [31] | A. B. Esteban, L. A. O, B. M, and A. T, “Food Safety and Hygienic Practices Among Street Food Vendors in Ife East Local Government Area Osun State, Nigeria,” International Journal of Research and Scientific Innovation, vol. XII, no. XV, pp. 468-477, Apr. 2025, |
| [32] | T. Barton, M. O. Tomori, D. Renville, and L. Francois, “Food Safety Knowledge among Street Food Vendors: Case of Demerara-”, Texila Advanced Journal of Multidisciplinary Health Research, vol. 5, no. 1, May. 2025, |
| [33] | W. N. F. Wan Nawawi, V. Ramoo, M. C. Chong, N. H. Zaini, P. L. Chui, and Z. Abdul Mulud, “The Food Safety Knowledge, Attitude and Practice of Malaysian Food Truck Vendors during the COVID-19 Pandemic,” Healthcare, vol. 10, no. 6, p. 998, May 2022, |
| [34] | W.-L. Seow et al., “A Systematic Review on the Usability of Web-Based Applications in Advocating Consumers on Food Safety,” Foods, vol. 11, no. 1, p. 115, Jan. 2022, |
| [35] | T. M. Osaili, B. A. Obeidat, D. O. Abu Jamous, and H. A. Bawadi, “Food safety knowledge and practices among college female students in north of Jordan,” Food Control, vol. 22, no. 2, pp. 269-276, Feb. 2011, |
| [36] | J. Beaudette and T. Koch, “Restaurant Perspectives on the Effects of Point-of-Sale Tip Recommendations on Consumer Patronage,” Journal of Student Research, vol. 12, no. 4, Nov. 2023, |
| [37] | M. L. McHugh, “The Chi-square Test of Independence,” Biochemia Medica, vol. 23, no. 2, pp. 143-149, Jun. 2013, |
| [38] | N. W. Van Hise, R. M. Petrak, K. Shah, M. Diaz, V. Chundi, and M. Redell, "Oritavancin versus daptomycin for osteomyelitis treatment after surgical debridement", Infectious Diseases and Therapy, vol. 13, no. 3, p. 535-547, Feb. 2024, |
| [39] | T. E. S. Charlesworth, M. Navon, Y. Rabinovich, N. Lofaro, and B. Kurdi, “The project implicit international dataset: Measuring implicit and explicit social group attitudes and stereotypes across 34 countries (2009-2019),” Behavior Research Methods, vol. 55, no. 3, pp. 1413-1440, Jun. 2022, |
APA Style
Francois, L., Renville, D. S., Bernard, B., Barton, T. (2026). Statistical Assessment of Food Safety Knowledge Among Consumers in Demerara-Mahaica, Guyana. Science Journal of Public Health, 14(2), 80-91. https://doi.org/10.11648/j.sjph.20261402.14
ACS Style
Francois, L.; Renville, D. S.; Bernard, B.; Barton, T. Statistical Assessment of Food Safety Knowledge Among Consumers in Demerara-Mahaica, Guyana. Sci. J. Public Health 2026, 14(2), 80-91. doi: 10.11648/j.sjph.20261402.14
@article{10.11648/j.sjph.20261402.14,
author = {Linda Francois and Dwayne Shorlon Renville and Bunnel Bernard and Tandeka Barton},
title = {Statistical Assessment of Food Safety Knowledge Among Consumers in Demerara-Mahaica, Guyana},
journal = {Science Journal of Public Health},
volume = {14},
number = {2},
pages = {80-91},
doi = {10.11648/j.sjph.20261402.14},
url = {https://doi.org/10.11648/j.sjph.20261402.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.sjph.20261402.14},
abstract = {Street foods constitute an essential component of urban food access in Guyana. Yet, empirical evidence on consumer food safety knowledge remains scarce, with existing research focused mainly on street food vendors. This study assessed consumer food safety knowledge in Demerara-Mahaica, Guyana, and examined demographic factors associated with high knowledge. A cross-sectional survey was conducted among 104 consumers using a structured questionnaire comprising demographic characteristics and 18 food safety knowledge items. Knowledge scores were derived from correct responses and categorized into low, moderate, and high levels. Descriptive analyses summarized overall and item-level knowledge, while Chi-square tests and odds ratios examined associations between knowledge and demographic variables. A multivariable binary logistic regression model was fitted to identify independent predictors of high food safety knowledge. Overall, most consumers demonstrated moderate food safety knowledge, with persistent deficiencies in technical and pathogen-related concepts despite relatively strong awareness of general hygiene practices. Item-level analyses showed significant associations between overall knowledge classification and understanding of microbial contamination, foodborne pathogens, reheating risks, and adverse health outcomes linked to foodborne disease. Bivariate analyses revealed no statistically significant associations between knowledge level and gender, age group, ethnicity, or place of education. In the multivariable model, educational attainment emerged as the only statistically significant independent predictor of high food safety knowledge (adjusted OR = 2.35), while age showed a positive but borderline association. The modest explanatory power of the model (8.8%, Cox & Snell R², and 12.4% Nagelkerke R²) suggests that factors beyond basic demographics alone shape consumer food safety knowledge. These findings indicate that improving consumer food safety in Guyana will require targeted, context-specific education to address technical knowledge gaps, implemented alongside vendor training, infrastructure support, and regulatory measures within informal food systems.},
year = {2026}
}
TY - JOUR T1 - Statistical Assessment of Food Safety Knowledge Among Consumers in Demerara-Mahaica, Guyana AU - Linda Francois AU - Dwayne Shorlon Renville AU - Bunnel Bernard AU - Tandeka Barton Y1 - 2026/04/02 PY - 2026 N1 - https://doi.org/10.11648/j.sjph.20261402.14 DO - 10.11648/j.sjph.20261402.14 T2 - Science Journal of Public Health JF - Science Journal of Public Health JO - Science Journal of Public Health SP - 80 EP - 91 PB - Science Publishing Group SN - 2328-7950 UR - https://doi.org/10.11648/j.sjph.20261402.14 AB - Street foods constitute an essential component of urban food access in Guyana. Yet, empirical evidence on consumer food safety knowledge remains scarce, with existing research focused mainly on street food vendors. This study assessed consumer food safety knowledge in Demerara-Mahaica, Guyana, and examined demographic factors associated with high knowledge. A cross-sectional survey was conducted among 104 consumers using a structured questionnaire comprising demographic characteristics and 18 food safety knowledge items. Knowledge scores were derived from correct responses and categorized into low, moderate, and high levels. Descriptive analyses summarized overall and item-level knowledge, while Chi-square tests and odds ratios examined associations between knowledge and demographic variables. A multivariable binary logistic regression model was fitted to identify independent predictors of high food safety knowledge. Overall, most consumers demonstrated moderate food safety knowledge, with persistent deficiencies in technical and pathogen-related concepts despite relatively strong awareness of general hygiene practices. Item-level analyses showed significant associations between overall knowledge classification and understanding of microbial contamination, foodborne pathogens, reheating risks, and adverse health outcomes linked to foodborne disease. Bivariate analyses revealed no statistically significant associations between knowledge level and gender, age group, ethnicity, or place of education. In the multivariable model, educational attainment emerged as the only statistically significant independent predictor of high food safety knowledge (adjusted OR = 2.35), while age showed a positive but borderline association. The modest explanatory power of the model (8.8%, Cox & Snell R², and 12.4% Nagelkerke R²) suggests that factors beyond basic demographics alone shape consumer food safety knowledge. These findings indicate that improving consumer food safety in Guyana will require targeted, context-specific education to address technical knowledge gaps, implemented alongside vendor training, infrastructure support, and regulatory measures within informal food systems. VL - 14 IS - 2 ER -
Department of Mathematics, Physics and Statistics, University of Guyana, Georgetown, Guyana
Department of Mathematics, Physics and Statistics, University of Guyana, Georgetown, Guyana
Department of Mathematics, Physics and Statistics, University of Guyana, Georgetown, Guyana
Department of Public Health, Texila American University, Georgetown, Guyana
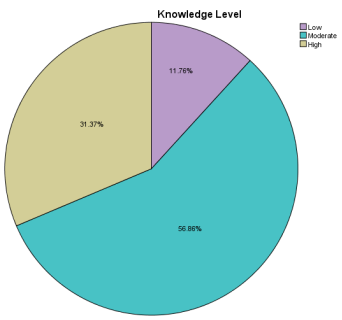
Figure 1. Distribution of overall food safety knowledge levels among consumers.
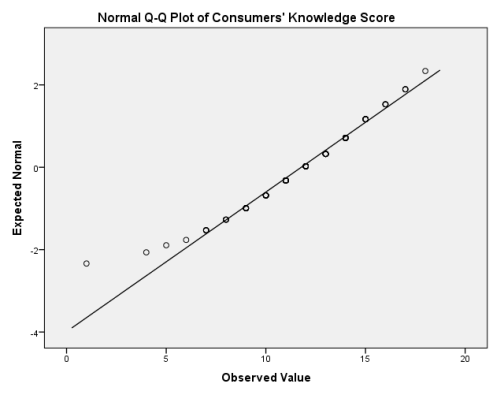
Figure 2. Normal Q-Q plot of the total food safety knowledge score among consumers.
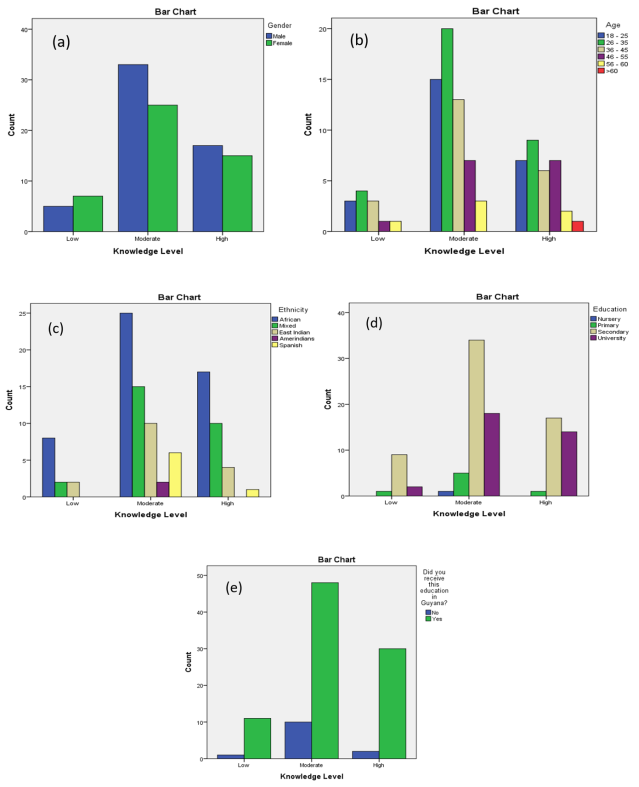
Figure 3. Distribution of food safety knowledge levels across demographic characteristics, (a) gender, (b) age, (c) ethnicity, (d) education, and (e) whether education was received in Guyana.
Figure 4. Institutional Review Board (IRB) approval letter granting ethical clearance for the study.
Information

