Abstract
This research explores healthcare-seeking patterns among residents of Lalgudi Town Panchayat, Tamil Nadu, India, addressing the critical need for equitable access to health services in rural areas. The study aims to understand the factors influencing the utilisation of government health services, given the complex interplay of social, economic, and cultural elements. Using a structured questionnaire, data were collected from 600 hospital visitors and subsequently analysed using factor analysis and structural equation modelling (SEM). The findings highlight several key drivers of healthcare utilisation, including adequate staffing levels, patients' mindsets, service convenience, and the availability of free treatment. Additionally, social and cultural influences, such as patient satisfaction, ease of access, and cost-free services, were found to significantly impact residents' healthcare decisions. Despite generally high levels of trust and satisfaction with local government hospitals, challenges persist, including limited health awareness, resource shortages, and ingrained social barriers. The study concludes with recommendations to enhance healthcare accessibility and equity through sustained investments in healthcare infrastructure, targeted community outreach initiatives, and evidence-based policy planning. These insights are crucial for improving health outcomes in Lalgudi and similar rural contexts in India, ultimately contributing to the broader goal of achieving better health equity.
|
Published in
|
World Journal of Public Health (Volume 11, Issue 2)
|
|
DOI
|
10.11648/j.wjph.20261102.21
|
|
Page(s)
|
197-206 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2026. Published by Science Publishing Group
|
Keywords
Healthcare-seeking Behaviour, Public Health, Rural India, Government Hospital, Factor Analysis, Structural Equation Model
1. Introduction
Social, economic, and cultural factors direct healthcare choices. Residents of Lalgudi Town Panchayat are shaped by these influences when deciding between formal doctors and informal options. Understanding their patterns is key to health policy, and this study specifically examines how residents of Lalgudi Town Panchayat use the government general hospital.
Research on health-seeking behaviour reveals how people in developing countries address illness and access health services, highlighting fairness and health goals. Identifying influences on care-seeking improves programs and reduces the risk of serious illness, thereby directly aligning with this study’s aim.
Health care-seeking behaviour refers to how people seek and accept medical care, influenced by culture, habits, and finances. identify three main factors: a person’s tendency to seek care, the ease of obtaining care, and the seriousness of the illness
| [1] | Andersen, R., & Newman, J. F. (1973). Societal and Individual Determinants of Medical Care Utilization in the United States. The Milbank Memorial Fund Quarterly. Health and Society, 51(1), 95–124. https://doi.org/10.2307/3349613 |
[1]
. describes five levels of health system coverage: availability, accessibility, acceptability, use, and satisfaction
| [2] | Tanahashi, T. (1978). Health service coverage and its evaluation. Bull World Health Organ. 1978; 56(2): 295-303. |
[2]
. highlights that provider options, costs, and waiting times also shape choices
.
Many current models do not capture the full range of personal and external factors that affect care-seeking behaviour. Use a socioecological approach that integrates individual, community, and policy influences
| [4] | Willems, S., De Maesschalck, S., Deveugele, M., Derese, A., & De Maeseneer, J. (2005). Socio-economic status of the patient and doctor–patient communication: Does it make a difference? Patient education and counselling, 56(2), 139–146.
https://doi.org/10.1016/j.pec.2004.02.011 |
[4]
. Whether people seek care depends on their needs, mental and social factors, and provider-related issues. How often people use care also shapes future choices and health results.
2. Overview
The "Health For All" policy and "Primary Health Care" strategy, introduced by WHO in 1978, sought to make healthcare equitable for all, with particular emphasis on poorer countries. PHC prioritised accessible care, illness prevention, and community participation. While approaches varied, the central objective was to enhance basic health services.
Even with these efforts, low-income countries, especially in sub-Saharan Africa, faced significant challenges, including economic difficulties, debt burdens, policy changes, and reduced donor support
. Community involvement was low, and funding systems became weaker. Other problems included the HIV pandemic, changes in population, and ongoing poverty. By 2000, the “Health For All” goal had not been achieved, prompting the WHO to develop new policies
.
Health-seeking behaviour means the steps people take when they notice health problems. Most people with mental illness do not get professional help
| [7] | Alonso, J., Angermeyer, M. C., Bernert, S., Bruffaerts, R., Brugha, T. S., Bryson, H. & Vollebergh, W. A. (2004). Use of mental health services in Europe: results from the European Study of the Epidemiology of Mental Disorders (ESEMeD) project. Acta Psychiatrica Scandinavica, 109(s420), 47-54.
https://doi.org/10.1111/j.1600-0047.2004.00327.x |
[7]
, but their patterns are like those for other illnesses. This process includes noticing symptoms, deciding between self-care and outside help, and choosing what to do next. Recent studies in India show that gender, education, stigma, and access to care are major barriers to seeking help
| [8] | Kumar, S., Dansereau, E., & Murray, C. J. L. (2019). The determinants of healthcare utilisation in India: Evidence from a recent household survey. BMC Public Health, 19, 1189.
https://doi.org/10.1080/00036846.2014.950836 |
| [9] | Chauhan, S., Kumar, S., & Jaiswal, A. (2022). Factors influencing health-seeking behaviour among rural populations in India: A cross-sectional study. Journal of Family Medicine and Primary Care, 11(1), 123–129.
https://doi.org/10.4103/jfmpc.jfmpc_1196_21 |
[8, 9]
.
Many social and cultural factors affect how people seek health care, including age, gender, education, income, ethnicity, religion, social ties, and place of residence
. In India, caste, place of residence (city or village), and traditional beliefs are important
| [11] | Singh G, Raghav P, Rustagi N (2025). Health Seeking Behaviour among Cancer Patients with the aid of Geographic Information System: A Mixed-Methods Study from Western India. Asian Pac J Cancer Prev. 2025 Jun 1; 26(6): 2205-2213. https://doi.org/10.31557/APJCP.2025.26.6.2205 |
[11]
. Health geographers have shown that distance to health facilities and regional differences matter across Indian states
| [12] | Asadullah, Ritvik Amarchand, Ambuj Roy, Rohit Bhatia, Rakesh Kumar, and Anand Krishnan (2024). Strengthening cardiac services in Faridabad District: A facility mapping exercise to explore implementation of a hub-and-spoke model. 159(3&4); 347-355. https://doi.org/10.25259/IJMR_1789_23 |
| [13] | Joseph, A. E., & Phillips, D. R. (1984). Accessibility and utilisation: Geographical perspectives on health care delivery. London: Harper & Row. urn: lcp: accessibilityuti0000jose: epub: 94752b4a-0105-4890-a843-b6f93a0b57f6. |
| [14] | Singh, N., Patel, R., & Chauhan, S. (2022). Geospatial analysis of utilisation of maternal health care services in India. GeoJournal, 87(4), 3007–3026.
https://www.jstor.org/stable/48754636 |
[12-14]
. People often ask family and friends for advice, which is shaped by those people's beliefs about symptoms. Stigma can stop people from using mental health services
| [15] | Conner KO, Lee B, Mayers V, Robinson D, Reynolds CF, Albert S, Brown C (2010). Attitudes and beliefs about mental health among African American older adults suffering from depression. J Aging Stud. 1; 24(4): 266-277.
https://doi.org/10.1016/j.jaging.2010.05.007 |
| [16] | Aromaa, E., Tolvanen, A., Tuulari, J., & Wahlbeck, K. (2011). Personal stigma and use of mental health services among people with depression in the general population in Finland. BMC Psychiatry, 11, 52.
https://doi.org/10.1186/1471-244X-11-52 |
[15, 16]
. Personal factors may affect health systems, their economic status, available resources, and beliefs about the seriousness of symptoms, all of which influence health-seeking. Other important factors include access, quality, cost, distance, and user fees
.
Chronic and infectious diseases now affect people everywhere
. There is a clear rise in non-communicable diseases, but how people seek care and their access to services still vary, especially between urban and rural areas, due to social and economic differences
.
People’s decisions about seeking health care depend on the availability, quality, and affordability of services, as well as their social group and personal situation
. City residents usually adopt new practices more quickly, while rural residents often stick to traditions. Studies show that health-seeking rates remain low in rural areas, at 44.1% in Mongolia and 8.7% in Ethiopia
.
In short, many social, economic, and cultural factors shape how people seek health care. Understanding how urban and rural areas differ is important for developing effective health policies
| [21] | Van der Hoeven, M., Kruger, A., & Greeff, M. (2012). Differences in health care seeking behaviour between rural and urban communities in South Africa. International Journal for Equity in Health, 11, 31.
https://doi.org/10.1186/1475-9276-11-31 |
[21]
. Comparing different places helps find out what matters most.
Rising disease rates and expensive health care make public health a big challenge for India’s urban poor. In the past decade, policies have become more proactive, such as the National Health Policy 2002, which aimed to improve access; however, uneven resource distribution has led to regional disparities. Growing economic, regional, and gender gaps led to the National Urban and Rural Health Missions, which try to meet the needs of different groups. Recent studies by health geographers, including
| [22] | Kimberly Lakin, Sumit Kane (2022), People’s expectations of healthcare: A conceptual review and proposed analytical framework, Social Science & Medicine, Volume 292,
https://doi.org/10.1016/j.socscimed.2021.114636 |
| [23] | Gupta, G., Rana, T. S., Karun, S (2025). Spatial pattern and correlates of maternal healthcare utilization in the North Eastern Region of India: evidence from the National Family Health Survey, 2019–2021. Discov. Public. Health 22, 365.
https://doi.org/10.1186/s12982-025-00660-0 |
| [24] | Agrawal, R., Chakraborty, M. & Panda, S (2025). Assessing health vulnerability in Indian slums: mapping risks and analyzing contributing factors. GeoJournal 90, 231 (2025).
https://doi.org/10.1007/s10708-025-11484-5 |
[22-24]
, show that disparities in healthcare access persist despite these efforts.
People who need health care most in India often have trouble getting services. Major barriers include limited access, insufficient staff, and low investment. From 2011 to 2015, only 4% of GDP went to health, and just 1.3% to public health, far below levels in developed countries. This lack of funding has led to weak infrastructure and less support since the 1980s, especially after economic liberalisation.
3. Significance of the Present Study
Community health-seeking patterns shape service use and health outcomes. This study focuses on identifying the key physical, social, economic, cultural, and political factors that drive healthcare behaviour in the Lalgudi Town Panchayat. Barriers such as illiteracy, poverty, and funding issues strongly affect access. The research aims to clarify how these factors influence provider choice and service utilisation locally.
4. Study Area
Lalgudi, classified as a Town Panchayat within Tiruchirappalli district, Tamil Nadu, India, covers 10.03 square kilometres and comprises 18 administrative wards. Based on the 2011 Census, the population stands at 23,740, with nearly equal numbers of men and women. The literacy rate is notably high at 91.9%, with male literacy at 95.3% and female literacy at 88.63%. Healthcare services are delivered through the Lalgudi Government Hospital, Primary Health Centres, three private hospitals, and five clinics. As a result, Lalgudi demonstrates elevated literacy levels, a balanced demographic structure, and accessible healthcare, thereby enhancing the quality of life for its residents.
4.1. Objectives
The study aims to identify key factors that affect how residents of the Lalgudi Town Panchayat seek health care. It analyses social and economic backgrounds, prevalent diseases, treatment practices, and attitudes to understand how these factors shape service use and to provide clearer policy guidance.
4.2. Methodology
For this study in Lalgudi Town Panchayat, Tamil Nadu, data were collected from 600 randomly chosen hospital visitors using structured questionnaires during home visits. The researchers also reviewed existing literature on healthcare-seeking behaviour. They used simple percentages and factor analysis to narrow 60 variables down to 17 main factors. All statistical analyses were done with SPSS version 20. The results of the Structural Equation Model (SEM) for the healthcare-seeking behaviours data set meet the fit indices, and the proposed causal model relationships are an acceptable fit according to the recommended values.
5. Results
The application of factor analysis in the present study is particularly useful for distinguishing perceptions of healthcare-seeking behaviour among people in the Lalgudi Town Panchayat. Four dimensions were identified, contributing a total variance of 58.501 per cent.
Table 1. KMO and Bartlett's Test.
Kaiser-Meyer-Olkin Measure of Sampling Adequacy. | 0.868 |
Bartlett's Test of Sphericity | Approx. Chi-Square | 4143.602 |
df | 136 |
Sig. | 0.001 |
An eigenvalue of 1.0 is used as a cutoff to determine how many dimensions to extract. The correlation matrix revealed many coefficients of 0.4 or higher. The Kaiser-Meyer-Oklin (KMO) value was 0.868, exceeding the recommended value of 0.6 (
Table 1), and Barlett's Test of Sphericity was statistically significant (p = 0.001), supporting the factorability of the correlation matrix. Principal component analysis revealed seven components with eigenvalues exceeding 1.0.
5.1. Factor I: Adequate Employee
Table 2. Adequate Employee.
Factor | Variables | Component |
Factor Loadings | Communalities |
Adequate Employee | Sufficient nurses are working | 0.918 | 0.916 |
Adequate menial workers are working | 0.915 | 0.921 |
Sufficient doctors are working | 0.870 | 0.837 |
Eigen value: 2.853 | Percentage of variance: 16.780 |
Having enough staff is crucial for any public organisation to provide good services. In this study, 'Adequate Employee' was the most important factor, with an eigenvalue of 2.853, accounting for 16.780 per cent of the total variance (
Table 2). Three of seventeen variables had high positive factor scores: enough nurses (0.918), enough support staff (0.915), and enough doctors (0.870) in the hospital. This means the Lalgudi Town Panchayat hospital has enough staff to serve the local community.
5.2. Factor II: Mindset
Patient attitude is very important when seeking health care, and satisfaction with treatment is crucial. The second key factor, 'Mindset,' had an eigenvalue of 2.805 and made up 16.498 per cent of the total variance (
Table 3). Five of the seventeen variables scored high on this factor: taking medicine as prescribed (0.765), better health after treatment (0.677), seeing the hospital as clean (0.660), being happy with treatment (0.656), and having a good view of the hospital wards (0.577). These results show that most residents are happy with the services at the Lalgudi Town Panchayat hospital.
Table 3. Mindset.
Factor | Variables | Component |
Factor Loadings | Communalities |
Mindset | I used to take the tablets without fail | 0.765 | 0.635 |
My health is good after taking the treatment | 0.677 | 0.547 |
This hospital is very clean and neat | 0.660 | 0.522 |
I am very happy to receive treatment here | 0.656 | 0.488 |
Hospital wards are looking good | 0.577 | 0.509 |
Eigen value: 2.805 | Percentage of variance: 16.498 |
5.3. Factor III: Convenience
Convenience is a major reason people use healthcare centres. The third factor, 'Convenience,' had an eigenvalue of 2.497 and made up 14.690 per cent of the total variance (
Table 4). High scores for this factor included seeking emergency care (0.691), getting government benefits (0.690), being close to the hospital (0.666), good interactions with doctors (0.619), easy access to staff (0.553), and good personal health care (0.439). This shows that residents find it easy to use the Lalgudi Town Panchayat hospital.
Table 4. Convenience.
Factor | Variables | Component |
Factor Loadings | Communalities |
Convenience | I am coming here to receive emergency treatment | 0.691 | 0.513 |
I am coming here to receive government benefits | 0.690 | 0.503 |
I am coming because it is near | 0.666 | 0.452 |
I am coming. The physicians are treating me well | 0.619 | 0.521 |
I can access any person in this hospital | 0.553 | 0.365 |
I show much care for my health | 0.439 | 0.500 |
Eigen value: 2.497 | Percentage of variance: 14.690 |
5.4. Factor IV: Free Treatment
Medical treatment at the government general hospital is free. The fourth factor, 'Free Treatment,' had an eigenvalue of 1.790 and made up 10.532 per cent of the total variance (
Table 5). High scores for this factor included seeking care due to a lack of money (0.843), treatment being free (0.789), and not having other caregivers (0.544). This shows that people in Lalgudi Town Panchayat get free medical advice and treatment for their health problems at the local government hospital.
Table 5. Free Treatment.
Factor | Variables | Component |
Factor Loadings | Communalities |
Free Treatment | I am coming because I have no money | 0.843 | 0.715 |
I am coming because of the free treatment | 0.789 | 0.649 |
I am coming here; no one is there to take care of me | 0.544 | 0.353 |
Eigen value: 1.790 | Percentage of variance: 10.532 |
6. Model Fit Assessment-path Analysis with Structural Equation Modelling: Maximum Likelihood Estimates
Path analysis is used to assess whether the model fits the selected variables. Following
| [25] | Anderson, J. C., and Gerbing, D. W. (1988). Structural equation modelling in practice: A review and recommended two-step approach. Psychological Bulletin, 103, 411–423.
https://doi.org/10.1037/0033-2909.103.3.411 |
[25]
, the first step is to assess the survey instrument's reliability and validity. AMOS version 20 is then used to analyse the path model. This method, called SEM, is best for showing cause-and-effect relationships between variables and assessing how well the model fits
.
Structural equation modelling evaluates whether the data fit a hypothetical model. After examining the initial model fit, the chi-square test (P = 0.001) is below the recommended threshold (P < 0.05), indicating a good fit. However, as noted, a large sample size (over 200, with 300 in this research) can yield a significant p-value for the chi-square statistic
| [27] | Byrne, B. M. (2010). Structural Equation Modeling With AMOS: Basic Concepts, Applications, and Programming, Second Edition (2nd ed.). Routledge.
https://doi.org/10.4324/9780203805534 |
[27]
.
Following the initial assessment of model fit, further interpretation is conducted utilising established goodness-of-fit measures
| [27] | Byrne, B. M. (2010). Structural Equation Modeling With AMOS: Basic Concepts, Applications, and Programming, Second Edition (2nd ed.). Routledge.
https://doi.org/10.4324/9780203805534 |
[27]
. Common model-fit indices, including chi-square/degree of freedom (χ
2/df), comparative fit index (CFI), root mean square error of approximation (RMSEA), normated fit index (NFI), incremental fit index (IFI), and Tucker Lewis index (TLI), are employed to evaluate the measurement model.
Table 6 presents the estimates of these indices derived from AMOS structural modelling.
Table 6. Fit statistics of the Measurement Model.
Sl. No. | Fit statistic | Recommended | Obtained |
1 | Chi-Square | - | 9.760 |
2 | df | - | 3 |
3 | Chi-Square significance | P< =0.05 | 0.021 |
4 | Chi-Square ⁄df | <5.0 | 3.253 |
5 | Goodness of Fit Index (GFI) | >0.9 | 0.992 |
6 | Adjusted Goodness of Fit Index (AGFI) | >0.9 | 0.973 |
7 | Normated Fit Index (NFI) | >0.9 | 0.979 |
8 | Relative Fit Index (RFI) | >0.9 | 0.959 |
9 | Comparative Fit Index (CFI) | >0.9 | 0.985 |
10 | Tucker Lewis Index (TLI) | >0.9 | 0.971 |
11 | Incremental Fit Index (IFI) | Approaches 1 | 0.986 |
12 | Root mean square error of approximation (RMSEA) | <0.05 | 0.050 |
13 | Root Mean Square Residual (RMR) | <0.02 | 0.019 |
14 | Parsimony goodness-of-fit index (PGFI) | <5.0 | 0.298 |
Table 7. The Regression Weights for Every Path and Its Significance.
Sl. No. | Construct | Path | Construct | Unstandardized co-efficient | S. E. | Standardized co-efficient | C. R. | P | Label |
1 | Free Treatment | <--- | Mindset | -0.196 | 0.030 | -0.262 | -6.646 | 0.001** | Significant |
2 | Adequate Employee | <--- | Mindset | 0.427 | 0.029 | 0.512 | 14.571 | 0.001** | Significant |
3 | Convenience | <--- | Mindset | 0.573 | 0.034 | 0.572 | 17.068 | 0.001** | Significant |
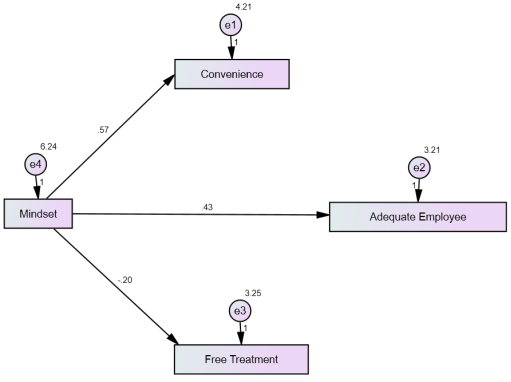
Figure 1. Path Model-Healthcare Seeking Behaviour: Unstandardized.
Evaluating the fit indices, specify criteria for model suitability: RMSEA of 0.05 or lower; CFI of 0.90 or higher; and NFI of 0.90 or higher. The fit between the collected data and the proposed measurement model can be assessed using the Chi-Square Goodness-of-Fit (GFI) test, with a GFI value of 0.9 or higher indicating a good fit
| [28] | Hu, L., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal, 6(1), 1–55.
https://doi.org/10.1080/10705519909540118 |
[28]
. Referring to
Table 1, the GFI for this study was 0.992, exceeding the recommended value of 0.90. The other measures also fitted satisfactorily: AGFI=0.973, RFI=0.959, CFI=0.985, TLI=0.971, IFI=0.986, NFI=0.979, with χ
2/df= 3.253, RMSEA=0.050
, RMR=0.019, and PGFI=0.298, indicating a good absolute fit. The goodness-of-fit indices together support the model fit, demonstrating the appropriateness of this structural model.
With the model fit established, the following assumptions are made to test the hypothesis.
H1: People's mindset is influenced by the availability of free treatment facilities in government hospitals.
H2: People's mindset is influenced by the adequate number of employees working in the government hospitals.
H3: People's mindset is influenced by the convenience of hospitals.
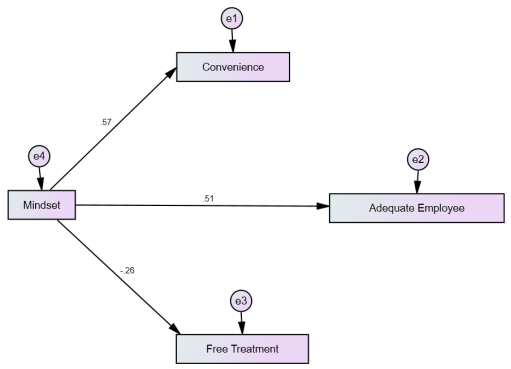
When these hypotheses are examined using SPSS-AMOS, the results include three regression weights and both unstandardized and standardised factor model estimates for each path, with their significance levels presented in
Figures 1 and 2.
Table 2 reports the unstandardized coefficients and relevant test statistics. The unstandardized regression coefficient indicates the magnitude of change in the dependent or mediating variable per unit change in the predictor variable.
Table 7 additionally provides the standardised estimate, standard error (S. E.), and the estimate divided by the standard error (Critical Ratio, C. R.). The column labelled P shows the probability value for the null hypothesis.
Following this, the results of hypothesis testing for the respective paths are shown in
Table 8.
Table 8. The Results of Hypothesis Testing for the Respected Path.
Hypothesis of Path Analysis | Estimate | P-value | Results on Hypothesis |
H1 | -.196 | 0.001** | Significant |
H2 | .427 | 0.001** | Significant |
H3 | .573 | 0.001** | Significant |
Figure 2. QPath Model-Healthcare Seeking Behaviour: Standardised.
6.1. H1: People's Mindset Is Influenced by the Availability of Free Treatment Facilities in Government Hospitals
When people's mindset increases by 1 unit, the availability of free treatment falls by 0.196 units. The score, 0.196, has an error of about 0.030. So, the ratio is 0.196/0.030 = -6.646. This means the score is 6.646 errors above zero. The chance of getting a ratio this large or larger is 0.001. The score is significant at 0.001. This supports the hypothesis (H1) that people's mindset is influenced by free treatment in government hospitals.
6.2. H2: People's Mindset Is Influenced by the Adequate Number of Employees Working in the Government Hospitals
When people's mindset increases by 1 unit, the number of employees in government hospitals rises by 0.427 units. The score, 0.427, has an error of about 0.029. The ratio is 0.427/0.029 = 14.571, meaning the score is 14.571 errors above zero. There is a 0.001 chance of obtaining this ratio by chance, so the score is significant at the 0.001 level. This supports the hypothesis (H2) that the number of employees in government hospitals influences people's mindset.
6.3. H3: People's Mindset Is Influenced by the Convenience of Hospitals
People's mindset is influenced by. When people's mindset increased by 1 unit, the convenience of government hospitals increased by 0.573 units, with an error of about 0.034. The ratio is 0.573/0.034 = 17.068. The result is not significant at the 1% level, as its value is 0.001. Still, the hypothesis (H3) that convenience influences people's mindset is supported in this area.
7. Conclusion
This study provides a detailed look at how people in Lalgudi Town Panchayat, Tamil Nadu, seek health care. It shows that social, cultural, and infrastructure factors all play a role in how people use government health services. Having enough staff, positive attitudes, easy access, and free treatment are key reasons people use these services. High satisfaction with care and staff helps build trust and encourages people to keep using public health services.
The study also highlights the need for sustained investment in infrastructure, regular staff training and hiring, and community programs to address misunderstandings and encourage prevention. Solving transport problems and reaching out to rural areas are important for fair access. Offering free or low-cost care helps remove money barriers for vulnerable groups and supports health equity.
Even with these good results, there are still problems, such as limited health knowledge, sometimes insufficient staff or resources, and social or cultural barriers to getting care quickly. These issues show that policies need to keep improving, feedback systems should be in place, and planning should be based on evidence to meet people’s changing needs.
In short, this study provides new insights into health-seeking behaviour in small Indian towns and offers practical guidance for policymakers and health leaders. Tackling both system and personal factors can help create a more inclusive, efficient, and responsive public health system in Lalgudi Town Panchayat and similar places.
In addition, this study also demonstrates that the measurement and structural models fit the data well, as evidenced by multiple indices exceeding recommended thresholds. The findings from the SEM path analysis confirm that the availability of free treatment, staffing adequacy, and service convenience significantly influence people's mindsets regarding utilisation of government hospitals. Each hypothesis was tested, highlighting the importance of these factors in shaping healthcare-seeking behaviour. Together, these insights provide valuable implications for policymakers and healthcare administrators aiming to enhance the effectiveness and public perception of government healthcare facilities.
8. Research Gaps
Even though there is extensive research on health-seeking behaviour in India and worldwide, there are few detailed, community-based studies examining the factors affecting healthcare use in small towns such as Lalgudi Town Panchayat. Most research focuses on big cities or rural areas, overlooking the unique issues in smaller towns. There is also little work on how patient attitudes, convenience, free treatment, and satisfaction with government care interact in these places. This study helps fill these gaps by giving real-world data from Lalgudi Town Panchayat and adds to our understanding of health-seeking in semi-urban areas.
9. Policy Implications
The results of this study offer important policy lessons for health care in small towns such as Lalgudi Town Panchayat. Ensuring there are enough staff, investing in buildings and equipment, and running health education campaigns are key to improving access and quality. Improving transport, reaching out to more people, offering free or low-cost programs, and setting up patient feedback systems will help make access and service quality fairer. Regularly collecting and studying data on how services are used can help health leaders make better decisions and build a more responsive public health system.
10. Recommendations for Future Research
Future research should compare small towns, rural areas, and urban areas to understand better the factors that affect health-seeking behaviour across settings. Long-term studies can show how changes in health care, policies, and economic conditions affect people's use of services over time. Talking with patients and providers can help explain why access to care is easier or harder, especially for vulnerable groups. Researchers could also examine how digital health and community programs improve access to care and health knowledge. Including private providers, traditional healers, and informal care would give a fuller picture of health care choices in small towns like Lalgudi Town Panchayat.
11. Ethical Issues and Standards
This study was conducted in strict accordance with established ethical standards for research involving human participants. Informed consent was obtained from all respondents before data collection commenced, ensuring that participation was entirely voluntary and based on a clear understanding of the study's objectives and procedures. The confidentiality and anonymity of participants were maintained throughout the research process, with all personal information securely protected and used solely for academic purposes. The research design, data collection, and analysis were carried out with full respect for participants' rights and dignity, in accordance with recognised guidelines for social science research. Approval was obtained from the relevant institutional ethics committee prior to fieldwork, and every effort was made to minimise any potential harm or discomfort to participants.
Abbreviations
SEM | Structural Equation Model |
HIV | Human Immunodeficiency Virus |
WHO | World Health Organization |
SPSS | Statistical Package for Social Sciences |
KMO | Kaiser-Meyer-Oklin |
AMOS | Analysis of Moment Structures |
Author Contributions
Pavendar Tamilarasan: Conceptualization, Data curation, Formal Analysis, Methodology, Project administration, Software, Supervision, Validation, Writing – original draft, Writing – review & editing
Vadivel Sivalingam: Conceptualization, Data curation, Investigation, Methodology, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing
Data Availability Statement
The datasets generated and analysed during the current study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Andersen, R., & Newman, J. F. (1973). Societal and Individual Determinants of Medical Care Utilization in the United States. The Milbank Memorial Fund Quarterly. Health and Society, 51(1), 95–124.
https://doi.org/10.2307/3349613
|
| [2] |
Tanahashi, T. (1978). Health service coverage and its evaluation. Bull World Health Organ. 1978; 56(2): 295-303.
|
| [3] |
Kroeger, A. (1983). Anthropological and socio-medical health care research in developing countries. Social Science & Medicine, 17(3), 147–161.
https://doi.org/10.1016/0277-9536(83)90248-4
|
| [4] |
Willems, S., De Maesschalck, S., Deveugele, M., Derese, A., & De Maeseneer, J. (2005). Socio-economic status of the patient and doctor–patient communication: Does it make a difference? Patient education and counselling, 56(2), 139–146.
https://doi.org/10.1016/j.pec.2004.02.011
|
| [5] |
United Nations Research Institute for Social Development. (2007).
https://cdn.unrisd.org/assets/library/papers/pdf-files/razavi-paper.pdf
|
| [6] |
World Health Organisation. (1997). Declaration of Alma-Ata. International Conference on Primary Health Care, Alma-Ata, USSR.
https://archive.org/details/World_Health_Organization_Report_English_1997
|
| [7] |
Alonso, J., Angermeyer, M. C., Bernert, S., Bruffaerts, R., Brugha, T. S., Bryson, H. & Vollebergh, W. A. (2004). Use of mental health services in Europe: results from the European Study of the Epidemiology of Mental Disorders (ESEMeD) project. Acta Psychiatrica Scandinavica, 109(s420), 47-54.
https://doi.org/10.1111/j.1600-0047.2004.00327.x
|
| [8] |
Kumar, S., Dansereau, E., & Murray, C. J. L. (2019). The determinants of healthcare utilisation in India: Evidence from a recent household survey. BMC Public Health, 19, 1189.
https://doi.org/10.1080/00036846.2014.950836
|
| [9] |
Chauhan, S., Kumar, S., & Jaiswal, A. (2022). Factors influencing health-seeking behaviour among rural populations in India: A cross-sectional study. Journal of Family Medicine and Primary Care, 11(1), 123–129.
https://doi.org/10.4103/jfmpc.jfmpc_1196_21
|
| [10] |
Young, J. T. (2004). Illness behaviour: a selective review and synthesis. Sociology of Health & Illness, 26(1), 1-31.
https://doi.org/10.1111/j.1467-9566.2004.00376.x
|
| [11] |
Singh G, Raghav P, Rustagi N (2025). Health Seeking Behaviour among Cancer Patients with the aid of Geographic Information System: A Mixed-Methods Study from Western India. Asian Pac J Cancer Prev. 2025 Jun 1; 26(6): 2205-2213.
https://doi.org/10.31557/APJCP.2025.26.6.2205
|
| [12] |
Asadullah, Ritvik Amarchand, Ambuj Roy, Rohit Bhatia, Rakesh Kumar, and Anand Krishnan (2024). Strengthening cardiac services in Faridabad District: A facility mapping exercise to explore implementation of a hub-and-spoke model. 159(3&4); 347-355.
https://doi.org/10.25259/IJMR_1789_23
|
| [13] |
Joseph, A. E., & Phillips, D. R. (1984). Accessibility and utilisation: Geographical perspectives on health care delivery. London: Harper & Row. urn: lcp: accessibilityuti0000jose: epub: 94752b4a-0105-4890-a843-b6f93a0b57f6.
|
| [14] |
Singh, N., Patel, R., & Chauhan, S. (2022). Geospatial analysis of utilisation of maternal health care services in India. GeoJournal, 87(4), 3007–3026.
https://www.jstor.org/stable/48754636
|
| [15] |
Conner KO, Lee B, Mayers V, Robinson D, Reynolds CF, Albert S, Brown C (2010). Attitudes and beliefs about mental health among African American older adults suffering from depression. J Aging Stud. 1; 24(4): 266-277.
https://doi.org/10.1016/j.jaging.2010.05.007
|
| [16] |
Aromaa, E., Tolvanen, A., Tuulari, J., & Wahlbeck, K. (2011). Personal stigma and use of mental health services among people with depression in the general population in Finland. BMC Psychiatry, 11, 52.
https://doi.org/10.1186/1471-244X-11-52
|
| [17] |
Shaikh, B. T., & Hatcher, J. (2007). Health-seeking behaviour and health service utilisation in Pakistan: challenging policymakers. Journal of Public Health, 27(1), 49-54. Available at:
https://ecommons.aku.edu/pakistan_fhs_mc_chs_chs/474
|
| [18] |
Green, J. (2012). Health-seeking behaviour in Pakistan: A narrative review of the existing literature. Public Health.
https://doi.org/10.1016/J.PUHE.2012.02.006
|
| [19] |
Engels, D., & Savioli, L. (2006). Reconsidering the underestimated burden caused by neglected tropical diseases. Trends in Parasitology, 22(8), 363-366.
https://doi.org/10.1016/j.pt.2006.06.004
|
| [20] |
World Health Organisation. (1978). Declaration of Alma-Ata. International Conference on Primary Health Care, Alma-Ata, USSR.
https://cdn.who.int/media/docs/default-source/documents/almaata-declaration-en.pdf?sfvrsn=7b3c2167_2
|
| [21] |
Van der Hoeven, M., Kruger, A., & Greeff, M. (2012). Differences in health care seeking behaviour between rural and urban communities in South Africa. International Journal for Equity in Health, 11, 31.
https://doi.org/10.1186/1475-9276-11-31
|
| [22] |
Kimberly Lakin, Sumit Kane (2022), People’s expectations of healthcare: A conceptual review and proposed analytical framework, Social Science & Medicine, Volume 292,
https://doi.org/10.1016/j.socscimed.2021.114636
|
| [23] |
Gupta, G., Rana, T. S., Karun, S (2025). Spatial pattern and correlates of maternal healthcare utilization in the North Eastern Region of India: evidence from the National Family Health Survey, 2019–2021. Discov. Public. Health 22, 365.
https://doi.org/10.1186/s12982-025-00660-0
|
| [24] |
Agrawal, R., Chakraborty, M. & Panda, S (2025). Assessing health vulnerability in Indian slums: mapping risks and analyzing contributing factors. GeoJournal 90, 231 (2025).
https://doi.org/10.1007/s10708-025-11484-5
|
| [25] |
Anderson, J. C., and Gerbing, D. W. (1988). Structural equation modelling in practice: A review and recommended two-step approach. Psychological Bulletin, 103, 411–423.
https://doi.org/10.1037/0033-2909.103.3.411
|
| [26] |
Peter T (2011). Adoption of Mobile Money Technology: Structural Equation Modelling Approach. Eur. J. Bus. Manage. 3(7).
https://www.researchgate.net/publication/265987570_Adoption_of_Mobile_Money_Transfer_Technology_Structural_Equation_Modeling_Approach
|
| [27] |
Byrne, B. M. (2010). Structural Equation Modeling With AMOS: Basic Concepts, Applications, and Programming, Second Edition (2nd ed.). Routledge.
https://doi.org/10.4324/9780203805534
|
| [28] |
Hu, L., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal, 6(1), 1–55.
https://doi.org/10.1080/10705519909540118
|
| [29] |
Bagozzi RP, Yi Y (1988). On the evaluation of structural equation models. J. Acad. Mark. Sci. 16(1): 74-94.
https://doi.org/10.1007/BF02723327
|
Cite This Article
-
APA Style
Tamilarasan, P., Sivalingam, V. (2026). A Study of Healthcare-seeking Patterns Among Residents in Lalgudi Town Panchayat, Tamil Nadu, India. World Journal of Public Health, 11(2), 197-206. https://doi.org/10.11648/j.wjph.20261102.21
 Copy
|
Copy
|
 Download
Download
ACS Style
Tamilarasan, P.; Sivalingam, V. A Study of Healthcare-seeking Patterns Among Residents in Lalgudi Town Panchayat, Tamil Nadu, India. World J. Public Health 2026, 11(2), 197-206. doi: 10.11648/j.wjph.20261102.21
Copy
|
Download
AMA Style
Tamilarasan P, Sivalingam V. A Study of Healthcare-seeking Patterns Among Residents in Lalgudi Town Panchayat, Tamil Nadu, India. World J Public Health. 2026;11(2):197-206. doi: 10.11648/j.wjph.20261102.21
Copy
|
Download
-
@article{10.11648/j.wjph.20261102.21,
author = {Pavendar Tamilarasan and Vadivel Sivalingam},
title = {A Study of Healthcare-seeking Patterns Among Residents in Lalgudi Town Panchayat, Tamil Nadu, India},
journal = {World Journal of Public Health},
volume = {11},
number = {2},
pages = {197-206},
doi = {10.11648/j.wjph.20261102.21},
url = {https://doi.org/10.11648/j.wjph.20261102.21},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.wjph.20261102.21},
abstract = {This research explores healthcare-seeking patterns among residents of Lalgudi Town Panchayat, Tamil Nadu, India, addressing the critical need for equitable access to health services in rural areas. The study aims to understand the factors influencing the utilisation of government health services, given the complex interplay of social, economic, and cultural elements. Using a structured questionnaire, data were collected from 600 hospital visitors and subsequently analysed using factor analysis and structural equation modelling (SEM). The findings highlight several key drivers of healthcare utilisation, including adequate staffing levels, patients' mindsets, service convenience, and the availability of free treatment. Additionally, social and cultural influences, such as patient satisfaction, ease of access, and cost-free services, were found to significantly impact residents' healthcare decisions. Despite generally high levels of trust and satisfaction with local government hospitals, challenges persist, including limited health awareness, resource shortages, and ingrained social barriers. The study concludes with recommendations to enhance healthcare accessibility and equity through sustained investments in healthcare infrastructure, targeted community outreach initiatives, and evidence-based policy planning. These insights are crucial for improving health outcomes in Lalgudi and similar rural contexts in India, ultimately contributing to the broader goal of achieving better health equity.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - A Study of Healthcare-seeking Patterns Among Residents in Lalgudi Town Panchayat, Tamil Nadu, India
AU - Pavendar Tamilarasan
AU - Vadivel Sivalingam
Y1 - 2026/06/18
PY - 2026
N1 - https://doi.org/10.11648/j.wjph.20261102.21
DO - 10.11648/j.wjph.20261102.21
T2 - World Journal of Public Health
JF - World Journal of Public Health
JO - World Journal of Public Health
SP - 197
EP - 206
PB - Science Publishing Group
SN - 2637-6059
UR - https://doi.org/10.11648/j.wjph.20261102.21
AB - This research explores healthcare-seeking patterns among residents of Lalgudi Town Panchayat, Tamil Nadu, India, addressing the critical need for equitable access to health services in rural areas. The study aims to understand the factors influencing the utilisation of government health services, given the complex interplay of social, economic, and cultural elements. Using a structured questionnaire, data were collected from 600 hospital visitors and subsequently analysed using factor analysis and structural equation modelling (SEM). The findings highlight several key drivers of healthcare utilisation, including adequate staffing levels, patients' mindsets, service convenience, and the availability of free treatment. Additionally, social and cultural influences, such as patient satisfaction, ease of access, and cost-free services, were found to significantly impact residents' healthcare decisions. Despite generally high levels of trust and satisfaction with local government hospitals, challenges persist, including limited health awareness, resource shortages, and ingrained social barriers. The study concludes with recommendations to enhance healthcare accessibility and equity through sustained investments in healthcare infrastructure, targeted community outreach initiatives, and evidence-based policy planning. These insights are crucial for improving health outcomes in Lalgudi and similar rural contexts in India, ultimately contributing to the broader goal of achieving better health equity.
VL - 11
IS - 2
ER -
Copy
|
Download