Abstract
Introduction: Acute Kidney Injury (AKI) is a major cause of mortality and long-term morbidity. It is a very common complication in asphyxiated newborns. Early detection of AKI in these cohort of patients will positively impact outcome. Serum Neutrophil Gelatin-associated lipocalin (NGAL) is a highly sensitive biomarker of AKI. There is paucity of data on the determination of the incidence of AKI in asphyxiated babies using Serum NGAL as a biomarker. Objective: This study was set to evaluate the use of serum NGAL measurement for early detection of AKI in babies with perinatal asphyxia at the Abia State University Teaching Hospital (ABSUTH), Aba. Methods: This was a cross-sectional descriptive study done at the Newborn Special Care Unit of ABSUTH, Aba, Nigeria. Serum NGAL estimation was done within the first six hours of delivery. Also, serum creatinine was done daily for the first week of admission. Results: A total of 155 term neonates with perinatal asphyxia were studied. The male to female ratio was 1.06:1. Among these neonates, 43.9% had mild, 29.0% had moderate and 27.1% had severe perinatal asphyxia respectively. The mean serum NGAL concentration in those with mild, moderate and severe perinatal asphyxia were 345.3ng/ml, 673.1ng/ml, and 866.1ng/ml, respectively. A statistically significant difference was observed in these mean serum NGAL concentrations (p value<0.05). The serum NGAL levels increased with the increasing severity of AKI. There was a higher serum NGAL concentration with a mean of 614.00±22ng/ml in patients with AKI (P<0.05). A cut-off value of 270ng/ml for serum NGAL using the receiver operating curve could detect AKI in asphyxiated neonates, with a sensitivity of 99.3%. The area under the curve of 1.0 was statistically significant. (p = 0.001) Conclusion: Serum NGAL is a highly sensitive biomarker of AKI. Serum NGAL levels measured within the first six hours after birth is elevated in patients with AKI. NGAL estimation in the first 6 hours of the birth of asphyxiated neonates is recommended for early detection of AKI.
|
Published in
|
American Journal of Pediatrics (Volume 11, Issue 3)
|
|
DOI
|
10.11648/j.ajp.20251103.17
|
|
Page(s)
|
156-165 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2025. Published by Science Publishing Group
|
Keywords
AKI, Serum NGAL, Serum Creatinine, Neonatal, Asphyxia, ABSUTH
1. Introduction
As many as 61% of severely asphyxiated infants may develop acute kidney injury (AKI) that is predominantly non-oliguric
| [1] | Agrawal S, Chaudhuri PK, Chaudhary AK, Kumar D. Acute kidney injury in asphyxiated neonates and its correlation to hypoxic ischemic encephalopathy staging. Indian J Child Health. 2016; 3(3): 254-7. |
[1]
. Also, available data suggest that the incidence of AKI in asphyxiated neonates is high, that non-oliguric AKI is common, and that AKI portends poor outcomes
| [2] | Onyiriuka NA. Birth Asphyxia in a mission hospital in Benin City, Nigeria. Trop j Obs. 2006; 23(1): 34-9. |
| [3] | Ogunlesi T, Oseni S. Severe Birth Asphyxia in Wesley Guild Hospital, lesa: A persistent plague! Niger Med Pract. 2008; |
[2, 3]
In critically ill patients, AKI is a major cause of mortality and long-term morbidity
| [4] | Jetton JG, Askenazi DJ. Update on acute kidney injury in the neonate. Curr Opin Pediatr. 2012 Apr; 24(2): 191-6. |
[4]
.
Acute kidney injury (AKI) in the newborn is a common problem in the neonatal intensive care unit (NICU), and the incidence of acute renal failure ranges from 22-67%
| [5] | Hoste EAJ, Clermont G, Kersten A, Venkataraman R, Angus DC, De Bacquer D, et al. RIFLE criteria for acute kidney injury are associated with hospital mortality in critically ill patients: a cohort analysis. Crit Care. 2006; 10(3): R73. |
[5]
.
In Nigeria, there is a paucity of data on AKI in asphyxiated newborns. In a study done in Benin City, Nigeria, 20% of the asphyxiated patients studied had AKI which was defined as serum creatinine greater than 1.0mg/dl
| [6] | Sadoh WE, Eregie CO, Nwaneri DU, Sadoh AE. The diagnostic value of both troponin T and creatinine kinase isoenzyme (CK-MB) in detecting combined renal and myocardial injuries in asphyxiated infants. PLoS One. 2014; 9(3): 9-12. |
[6]
. A similar study done in Port Harcourt identified 35.5% of AKI cases in neonates with severe birth asphyxia
| [7] | Anochie IC, Eke FU. Acute renal failure in Nigerian children: Port Harcourt experience. Pediatr Nephrol. 2005; 20(11): 1610-4. |
[7]
. In a recent cross-sectional descriptive study done on early detection of acute kidney injury using serum neutrophil gelatinase-associated lipocalin in Uyo, Nigeria, it was reported that 11.5% of the subjects had AKI using serum creatinine criteria while sNGAL was able to detect AKI in 48% of the subjects
| [8] | EE Ikpeme MU. early detection of acute kidney injury using serum neutrophil gelatinase-associated lipocalin in asphyxiated term neonates in university of uyo teaching hospital, uyo, Nigeria. african J Paediatr Nephrol. 2018; 5(1): 28-35. |
[8]
. Serum creatinine concentrations are reflective of maternal levels in the first few days of life
| [9] | Askenazi DJ, Ambalavanan N, Goldstein SL. Acute kidney injury in critically ill newborns: What do we know? What do we need to learn? 2008; |
| [10] | A. D, J.-P. G. Renal aspects of the term and preterm infant: A selective update. Curr Opin Pediatr. 2002; |
[9, 10]
. Again, serum creatinine is a poor marker of early renal dysfunction because it is greatly influenced by numerous non-renal factors such as body weight, race, age, and total body volume
| [11] | Lameire N, Van Biesen W, Vanholder R. The changing epidemiology of acute renal failure. Nature Clinical Practice Nephrology. 2006. |
[11]
. Oliguria (i.e. urine output less than 1ml/kg/hr.) is an insensitive marker of renal function in the newborn, as AKI can be seen in the absence of oliguria
| [12] | Karlowicz MG, Adelman RD. Nonoliguric and oliguric acute renal failure in asphyxiated term neonates. Pediatr Nephrol. 1995. |
[12]
These limitations highlight the importance of the use of some novel biomarkers that can be detected early during AKI. These biomarkers can also be detected in easily accessible fluids like urine which is derived from the kidney. The American Society of Nephrology has designated the development of biomarkers for early detection of AKI as a research priority.
| [13] | Berl T. American Society of Nephrology renal research report. J Am Soc Nephrol. 2005; 16(7): 1886-903. |
[13]
Currently, the more promising early non-invasive biomarkers of AKI are serum and urinary neutrophil gelatinase-associated lipocalin (NGAL), kidney injury molecule-1(KIM-1), urinary interleukin-18(IL-18), and serum cystatin C
| [14] | Mussap M, Degrandi R, Fravega M, Fanos V. Acute kidney injury in critically ill infants: the role of urine Neutrophil Gelatinase-Associated Lipocalin (NGAL). J Matern Fetal Neonatal Med [Internet]. 2010; 23 Suppl 3(October): 70-2. Available from: http://www.ncbi.nlm.nih.gov/pubmed/20807163 |
[14]
. Among these biomarkers, the most promising early non-invasive biomarkers of AKI are serum and urinary neutrophil gelatinase-associated lipocalin (NGAL)
| [15] | Mishra J, Qing MA, Prada A, Mitsnefes M, Zahedi K, Yang J, et al. Identification of neutrophil gelatinase-associated lipocalin as a novel early urinary biomarker for ischemic renal injury. J Am Soc Nephrol. 2003; |
[15]
. The levels of serum and urinary neutrophil gelatinase-associated lipocalin rise in patients 24-48 hours before serum creatinine elevation is detected. This has been shown by several studies
| [16] | Antonucci E, Lippi G, Ticinesi A, Pigna F, Guida L, Morelli I, et al. Neutrophil gelatinase-associated lipocalin (NGAL): A promising biomarker for the early diagnosis of acute kidney injury (AKI). Acta Biomed. 2014; 85(3): 289-94. |
[16]
.
Having in mind the limitations of using serum creatinine to diagnose AKI, this study seeks to determine the incidence of AKI in asphyxiated babies using Serum NGAL as a biomarker.
1.1. Research Questions
1) W hat is the level of serum NGAL in neonates with perinatal asphyxia
2) What is the sensitivity of the use of serum NGAL in identifying AKI in neonates with perinatal asphyxia
3) What is the incidence of AKI in neonates with perinatal asphyxia
1.2. Research Hypothesis
Null hypothesis.
Serum NGAL levels do not rise within the first six hours of delivery in neonates with AKI following perinatal asphyxia.
Alternate hypothesis.
Serum NGAL levels rise within the first six hours of delivery in neonates with AKI following perinatal asphyxia.
2. Method
2.1. Study Period and Setting
A hospital-based cross-sectional study. Conducted from April 2020 to February 2022 on newborns presenting with inability to cry or unsustained cry following delivery at the Special Care Baby Unit of ABSUTH, Aba Abia State, South East, Nigeria.
ABSUTH is the major tertiary health care facility in the state which serves as a referral center for those living in Aba and the surrounding towns as well as some neighboring states.
2.2. Inclusion Criteria
Term newborn babies aged six hours and below with perinatal asphyxia.
2.3. Exclusion Criteria
1) Babies with major congenital anomalies
2) Newborn babies with chromosomal anomalies
3) Premature babies (<37 completed weeks of pregnancy)
4) Newborn of a mother who suffered chronic kidney disease.
2.4. Sample Size
A sample size of 155 term neonates aged six hours and below who met the inclusion criteria were recruited into the study.
2.5. Study Design
Consecutive inborn and outborn neonates aged six hours and below who met the inclusion criteria were enrolled in the study as they presented to the newborn special care unit. This was continued until the sample size of 155 was reached. Informed written consent was obtained from each parent/caregiver before enrolling the subject. Using the study proforma/case record form, the parents/caregivers were interviewed by the researcher, and information about the subject’s age on admission, gender, contact address, phone numbers, presenting complaints, pregnancy, labour, and delivery history was obtained. Gestational age was obtained by calculation from the date of the last menstrual period and/ or possible neonatal ultrasonography to help in excluding preterm newborns from the study. The history of chronic kidney disease in the mother was also excluded. Apgar scores at 1, 5, and 10 minutes were obtained and recorded. Apgar scores of referred subjects were obtained through either their referral notes or if there were no referral notes, phone calls were made to the referring facility to help the researcher estimate the Apgar score of the subject. Asphyxiated neonates were grouped into severe (0-3), moderate (4-5), and mild (6) based on Apgar score at 5 minutes
| [17] | Finster M, Wood M. The Apgar score has survived the test of time. Anesthesiology. 2005; |
[17]
.
2.6. Urine Sample Collection
The urinary output of each of the subjects in the first 24 hours was measured and recorded. With the hand washed, the urine collector bag was held between the thumb and forefinger and applied from the back (perineal area). An adhesive tape was used to secure the urine collector to the skin around the vagina or the scrotum of the female or male neonates respectively. The diaper was loosely fitted to allow unimpeded filling of the bag. The quantity of urine in the urine collector bag was measured and recorded after 24 hours.
2.7. Blood Specimen Collection and Procedures
Two milliliters of venous blood samples were collected by venipuncture through a peripheral vein after cleansing the puncture site with 90% alcohol within six hours of the subjects’ delivery. Collected blood was allowed to clot and centrifuged at 3000 revolutions per minute. The supernatant serum obtained was shared into two, one half was transferred to plain test tubes and stored at -80ﹾC until analysis of serum NGAL was done. The second half was used to analyze serum creatinine. The samples for serum NGAL were pooled and analyzed in batches of 50 tests.
Serum creatinine was done daily for the first week of life and the result was documented in the patient’s clinical progress sheet. Subjects enrolled in the study were categorized within 72 hours of admission into the AKI group and no-AKI group and Acute kidney injury was defined as serum creatinine of 133µmol/L and above or a percentage increase in serum creatinine of ≥ 50% (1.5-fold from the baseline
. The non-AKI group was identified by normal serum creatinine values on both day 1 and day 3.
The weight, length, occipitofrontal circumference, and temperatures of each of the subjects were measured and documented:
Babies were weighed naked in a warm environment using a bassinet scale with high sides to ensure the baby’s safety. Three readings were taken for each enrolled subject and an average value was taken to the nearest 0.1 gram (gm).
The length was measured with the help of an assistant using a stadiometer. Three supine measurements were taken, and the average was recorded to the nearest 0.1 centimeters (cm).
Occipitofrontal circumference was measured as the maximum circumference of the head to the nearest 0.1cm with a non-elastic, flexible, measuring tape passing above the supra-orbital ridges and over the maximum occipital prominence as landmarks.
The temperatures of the subjects were taken using clinical mercury-in-glass thermometers. A complete neurological examination which included the subject’s level of consciousness, muscle tone, Moro reflex, pupillary size, and reaction to light was obtained. The stage of HIE was documented using the Sarnat and Sarnat scoring system
| [20] | Sarnat HB, Sarnat MS. Neonatal Encephalopathy Following Fetal Distress: A Clinical and Electroencephalographic Study. Arch Neurol. 1976; 33(10): 696-705. |
[20]
.
Laboratory studies were done by the researcher in collaboration with the chemical pathologist attached to ABSUTH, Aba after the researcher was trained on the laboratory procedures.
Serum creatinine assays were carried out immediately using the modified Jaffe’s method
| [21] | Lolekha PH, Jaruthunyaluck S, Srisawasdi P. Deproteinization of serum: Another best approach to eliminate all forms of bilirubin interference on serum creatinine by the kinetic Jaffe reaction. J Clin Lab Anal. 2001; |
[21]
.
Serum NGAL estimation was done using NGAL ELISA kit 036RUO by Bio Porto diagnostics from Tuborg Havnevej, 15, St. DK-2900 Hellerup Denmark with lot no. NG-1813-03.
Before performing the assay, all specimens and reagents were brought to room temperature (20-25ºc). Specimens were mixed thoroughly by gentle inversion and if necessary clear visible particulate matter by low-speed centrifugation. All samples were prepared before starting the assay. NGAL analysis by ELISA was performed using the commercially available assay, and was run according to the manufacturer’s protocol as stated below:
100µL of NGAL standards, diluted specimens, and any internal laboratory controls were pipetted into the precoated microwells. Microwells were incubated for 60 minutes at room temperature on a shaking platform set at 200 revolutions/minute. The microwells were washed three times with 300µL diluted wash solution.100µL each of Biotinylated NGAL Antibody and HRP-Streptavidin conjugate respectively were incubated in the microwells for 1 hour each with shaking at 200/minute. Washing with buffer solution was also done following the addition of each reagent substrate. The wells were covered and incubated for exactly 10 minutes at room temperature in the dark before the addition of the stop solution. The clock was started when filling the first well. All measurements were run in duplicate to ensure accuracy.
The NGAL concentration was measured at 450nm wavelength using a microplate reader. The mean absorbances for each set of duplicate standards, controls, and samples were calculated. A calibration curve was constructed by plotting the absorbance values obtained for the calibrators on the Y-axis against the corresponding NGAL concentrations on the X-axis. The calibration curve met the validation requirements. The NGAL concentrations of diluted samples were then found by placing their absorbance values on the calibration curve and reading the corresponding concentrations from the X-axis.
The color intensity (optical density) is a function of the NGAL concentration. The NGAL concentration in the samples was calculated from the calibration curve generated by the NGAL calibrators and their corresponding optical densities.
Newborn babies diagnosed with perinatal asphyxia were transferred to the special care newborn unit for observation and treatment. Management was individualized and according to the unit protocol for managing patients with perinatal asphyxia. Immediate clinical assessment was done by recording temperature, respiration, heart rate, capillary refill time, urine output, and oxygen saturation. These parameters were continuously monitored thereafter. Babies with Apgar scores of <4 at 1 minute or <7 at 5 minutes were started on intravenous infusion which was at 2/3rd maintenance. Blood sugar, hematocrit, and electrolyte were monitored and maintained within normal range. Seizures if present were treated with phenobarbital. Out of the 27% of patients with severe perinatal asphyxia, a mortality of 20% was recorded, however, among patients with mild and moderate perinatal asphyxia, no mortality was recorded. Patients were subsequently discharged to the newborn outpatient clinic for follow-up.
3. Data Analysis
The data was recorded on the study proforma and analyzed using IBM SPSS (Statistical Package for the Social Sciences) version 25. Data was appropriately summarized into tables and graphs.
Descriptive statistics were used to summarize quantitative variables while qualitative variables were summarized as proportions. Categorical data/variables were summarized using Chi-Square or Fisher’s exact test.
To determine the sensitivity and specificity of serum NGAL in identifying AKI, a 2X2 contingency table was created. In addition, non-normally distributed data were expressed using the median. A receiver operating characteristic (ROC) curve was generated by plotting the sensitivity against 1-specificity and the area under the curve was calculated. A two-sample t-test was used for continuous variables and Chi-Square or Fisher’s exact test was used for categorical variables. A p-value of ≤0.05 was considered statistically significant.
4. Results
One hundred and fifty-five subjects with perinatal asphyxia were studied of which 80 were males and 75 were females, giving a male: female: ratio of 1.06:1. The mean age of the subjects was 2.85±1.72 hours.
Table 1. Socio-demographic characteristics of study population.
Variables | Frequency (N=155) | Percentage (%) |
Age (Hours) | | |
0 | 7 | 4.5 |
1 | 27 | 17.4 |
2 | 44 | 28.4 |
3 | 29 | 18.7 |
4 | 18 | 11.6 |
5 | 13 | 8.4 |
6 | 17 | 11.0 |
Gender | | |
Male | 80 | 51.6 |
Female | 75 | 48.4 |
(Source: produced by the authors. Aba-Nigeria, 2025)
Table 1 shows the number of subjects having mild, moderate, and severe perinatal asphyxia.
Most of the subjects 68 (43.9%) had mild perinatal asphyxia, 45 (29.0%) had moderate, while 42 (27.1) had severe perinatal asphyxia.
Table 2. Distribution of subjects with Perinatal asphyxia.
APGAR Score at 5 minutes | Frequency | Percentage (%) |
mild (6) | 68 | 43.9 |
moderate (4-5) | 45 | 29.0 |
severe (0-3) | 42 | 27.1 |
Total | 155 | 100.0 |
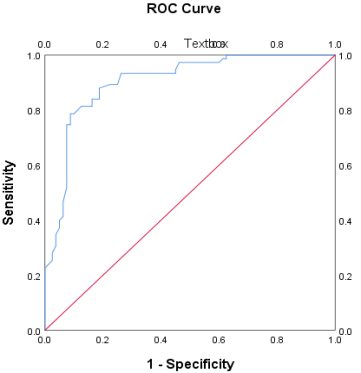
Area Under the Curve |
Test Result Variable: Serum NGAL |
Area |
1.000 |
Figure 1. Receiver operating characteristics curve for serum NGAL.
Figure 1 is a receiver operating characteristic curve (ROC) that was developed to predict the association between the gold standard (serum creatinine) and diagnostic test (sNGAL). The coordinates for the curve; sensitivity at various levels and false positive rate (1- specificity) were generated and plotted on a graph. The point of intersection that gave the best sensitivity and 1- specificity was used as the cutoff point for diagnosis of acute kidney injury (AKI). In this study, the cutoff was determined at 270ng/ml with the highest sensitivity of 99.3%. The area under the curve was 1.0 which was highly significant.
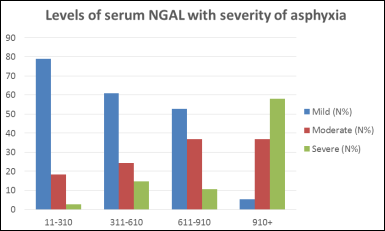
The majority (thirty (78.9%)) of the subjects with mild and moderate perinatal asphyxia had the least serum NGAL levels of between 11-610ng/ml while 33 (57.9%) which constituted the majority of those with severe perinatal asphyxia had levels of NGAL of over 910 ng/ml. All these values were statistically significant with a p value<0.05.
Table 3. Levels of serum NGAL with the severity of asphyxia.
Variable | Mild (N%) | Moderate (N%) | Severe (N%) | ² | P-value |
Serum NGAL (ng/ml) | | | | 76.484(FT) | 0.000* |
11-310 | 30(78.9) | 7(18.4) | 1(2.6) |
311-610 | 25(61.0) | 10(24.4) | 6(14.6) |
611-910 | 10(52.6) | 7(36.8) | 2(10.5) |
>910 | 3(5.3) | 21(36.8) | 33(57.9) |
Mean serum NGAL (ng/ml) | Mild mean±SD 345.3±31 | Moderate mean±SD 673.1±42 | Severe mean±SD 866.1±61 | | 0.000* |
AKI | | | | 81.993(FT) | 0.000* |
Yes | 8(10.7) | 28(37.3) | 39(52.0) |
No | 60(75.0) | 17(21.3) | 3(3.8) |
FT=Fisher’s exact test *Statistically significant
(Source: Produced by the authors. Aba-Nigeria, 2025.)
The mean serum NGAL level in patients with acute kidney injury was found to be 614ng/ml while those with no AKI had a mean serum NGAL level of 357.8ng/ml. These values were statistically significant with p<0.05.
Figure 2. depicts increasing levels of serum NGAL with increasing severity of perinatal asphyxia.
Table 4. Relationship between serum NGAL in neonates with AKI as selected by serum creatinine.
Variables | AKI | No | Mean±SD | Df | T-test | P-value |
Serum NGAL (ng/ml) | Yes | 75 | 614.00±222.624 | 153 | 12.702 | 0.000 |
| No | 80 | 357.84±286.697 | | | |
sCr (μmol/l) | Yes | 75 | 177.94±148.868 | 153 | 3.468 | 0.001 |
| No | 80 | 84.02±152.091 | | | |
(Source: Produced by the authors. Aba-Nigeria, 2025.)
Table 5 shows that the sensitivity of the use of serum NGAL is 97.3% while the specificity is 42.5%. These values were statistically significant.
Table 5. Sensitivity and Specificity of use of Serum NGAL.
Test result (sNGAL) | Yes (%) | No (%) | Total (%) |
Positive | 73 (97.3) | 46 (57.5) | 119 (76.8) |
Negative | 2 (2.7) | 34 (42.5) | 36 (23.2) |
Total | 75 (100.0) | 80 (100.0) | 155 (100.0) |
(Source: Produced by the authors. Aba-Nigeria, 2025)
Table 6 indicates that using serum NGAL as a diagnostic marker, one hundred and thirty-one subjects were found to have AKI. Hence, the incidence of AKI was 84.5% using a cutoff of 270ng/ml.
Table 6. Incidence of AKI.
Serum NGAL Test | n = 155 | % |
Positive (AKI) | 131 | 84.5 |
Negative (No AKI) | 24 | 15.5 |
Total | 155 | 100 |
(Source: Produced by the authors. Aba-Nigeria, 2025)
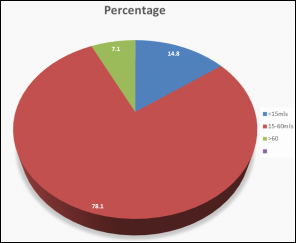
Figure 3. Percentage of subjects and quantity of urine made in the first 24 hours after admission.
Figure 3 shows that 78.1% of the subjects had a urine output of 15-60mls, 14.8% made <15 mls of urine, and 7.1% made >60mls of urine within the first 24 hours of admission.
5. Discussion
In this study, serum NGAL measured in the first 6 hours of life showed significantly higher values in patients with acute kidney injury than in patients without acute kidney injury. This finding is similar to the study done by Krawczeski
et al.
| [22] | Krawczeski CD, Woo JG, Wang Y, Bennett MR, Ma Q, Devarajan P. Neutrophil Gelatinase-Associated Lipocalin Concentrations Predict Development of Acute Kidney Injury in Neonates and Children after Cardiopulmonary Bypass. J Pediatr [Internet]. 2011 Jun 1; 158(6): 1009-1015. e1. Available from: https://doi.org/10.1016/j.jpeds.2010.12.057 |
[22]
, where urine NGAL levels in neonates were significantly increased in the second hour after cardiopulmonary bypass surgery. The bypass surgery caused acute severe hypotension leading to AKI. Also, in agreement with this finding is the study done by Udoh
et al in West Africa, Nigeria which demonstrated elevated levels of serum NGAL in patients with AKI.
| [8] | EE Ikpeme MU. early detection of acute kidney injury using serum neutrophil gelatinase-associated lipocalin in asphyxiated term neonates in university of uyo teaching hospital, uyo, Nigeria. african J Paediatr Nephrol. 2018; 5(1): 28-35. |
[8]
Essajee
et al.
| [23] | Essajee F, Were F, Admani B. Urine neutrophil gelatinase-associated lipocalin in asphyxiated neonates: a prospective cohort study. Pediatr Nephrol. 2015; 30(7): 1189-96. |
[23]
, Pekovic
et al,
| [24] | Pejović B, Erić-Marinković J, Pejović M, Kotur-Stevuljević J, Peco-Antić A. Detection of acute kidney injury in premature asphyxiated neonates by serum neutrophil gelatinase-associated lipocalin (sNGAL) - Sensitivity and specificity of a potential new biomarker. Biochem Medica. 2015; 25(3): 450-9. |
[24]
, Abdel Hady
et al.
| [25] | Abdelhady S, Gawad ERA, Haie OMA, Mansour AI. Usefulness of Serum and Urinary Neutrophil Gelatinase -Associated Lipocalin in Detecting Acute Kidney Injury in Asphyxiated Neonates. Int J Med Heal Sci. 2016; 5(4). |
[25]
, and El Raggal
et al.
| [26] | El Raggal NM, Khafagy SM, Mahmoud NH, El Beltagy SA. Serum neutrophil gelatinase-associated lipocalin as a marker of acute kidney injury in asphyxiated neonates. Indian Pediatr. 2013; 50(5): 459-62. |
[26]
, demonstrated similar findings.
Furthermore, serum NGAL steadily increased with increasing severity of perinatal asphyxia and AKI in this study, corroborating a study done on serum NGAL as a diagnostic marker of AKI in asphyxiated neonates by El Raggal
et al.
| [26] | El Raggal NM, Khafagy SM, Mahmoud NH, El Beltagy SA. Serum neutrophil gelatinase-associated lipocalin as a marker of acute kidney injury in asphyxiated neonates. Indian Pediatr. 2013; 50(5): 459-62. |
[26]
This finding could be attributed to ischemia of renal parenchyma which occurs in AKI. Gupta
et al, in a study on the incidence of renal failure in asphyxiated neonates, showed that the severity of renal failure correlated with Apgar score and HIE grading of the neonates.
| [27] | Gupta BD, Sharma P, Bagla J, Parakh M, Soni JP. Renal failure in asphyxiated neonates. Indian Pediatr. 2005; |
[27]
Also, Kaur
et al and Karlowicz
et al, demonstrated a greater number of patients developing AKI in severe than moderate perinatal asphyxia
| [28] | Kaur S, Jain S, Saha a, Chawla D, Parmar VR, Basu S, et al. Evaluation of glomerular and tubular renal function in neonates with birth asphyxia. Ann Trop Paediatr. 2011; 31(2): 129-34. |
[28]
.
The sensitivity of the use of sNGAL in the early identification of AKI in neonates with perinatal asphyxia was high at 99.3%. This was similar to other studies done on the use of sNGAL as an acute kidney injury biomarker. Studies done by Abdelhady
et al, El Raggal
et al and Essajee
et al found sensitivities of 95%, 83.3%, and 88% respectively
| [23] | Essajee F, Were F, Admani B. Urine neutrophil gelatinase-associated lipocalin in asphyxiated neonates: a prospective cohort study. Pediatr Nephrol. 2015; 30(7): 1189-96. |
| [25] | Abdelhady S, Gawad ERA, Haie OMA, Mansour AI. Usefulness of Serum and Urinary Neutrophil Gelatinase -Associated Lipocalin in Detecting Acute Kidney Injury in Asphyxiated Neonates. Int J Med Heal Sci. 2016; 5(4). |
| [26] | El Raggal NM, Khafagy SM, Mahmoud NH, El Beltagy SA. Serum neutrophil gelatinase-associated lipocalin as a marker of acute kidney injury in asphyxiated neonates. Indian Pediatr. 2013; 50(5): 459-62. |
[23, 25, 26]
. Lower but significant sensitivity of 70% was found by Pejovic
et al.
| [24] | Pejović B, Erić-Marinković J, Pejović M, Kotur-Stevuljević J, Peco-Antić A. Detection of acute kidney injury in premature asphyxiated neonates by serum neutrophil gelatinase-associated lipocalin (sNGAL) - Sensitivity and specificity of a potential new biomarker. Biochem Medica. 2015; 25(3): 450-9. |
[24]
, and this could be attributed to the time of analysis of the ROC curve. Again, premature neonates were the study population enrolled in the study. The high sensitivity of the use of NGAL in both previous and current studies could be attributed to the fact that specimens were collected within 6 hours of life and lends credence to serum NGAL detecting AKI earlier than serum creatinine which is a late marker of acute kidney injury in neonates with perinatal asphyxia.
The incidence of AKI in neonates with perinatal asphyxia using serum NGAL in this index study was 84.5% which is comparable with studies done in Belgrade, Serbia where 67.6% of the patients developed AKI
| [24] | Pejović B, Erić-Marinković J, Pejović M, Kotur-Stevuljević J, Peco-Antić A. Detection of acute kidney injury in premature asphyxiated neonates by serum neutrophil gelatinase-associated lipocalin (sNGAL) - Sensitivity and specificity of a potential new biomarker. Biochem Medica. 2015; 25(3): 450-9. |
[24]
. It is however higher than a Kenyan study with a prevalence of 56%
| [23] | Essajee F, Were F, Admani B. Urine neutrophil gelatinase-associated lipocalin in asphyxiated neonates: a prospective cohort study. Pediatr Nephrol. 2015; 30(7): 1189-96. |
[23]
, and another study done in Egypt with a prevalence of 55%
| [26] | El Raggal NM, Khafagy SM, Mahmoud NH, El Beltagy SA. Serum neutrophil gelatinase-associated lipocalin as a marker of acute kidney injury in asphyxiated neonates. Indian Pediatr. 2013; 50(5): 459-62. |
[26]
. Another study which is the only published study on the incidence of AKI in neonates with perinatal asphyxia in Nigeria found an incidence of 48%
| [29] | Emmanuel IE, Tony DO, Paulinus UM, J UJ. Incidence of acute kidney injury in asphyxiated babies in university of Uyo teaching hospital, Uyo, Nigeria. 2020; 8(7): 2477-81. |
[29]
. The high prevalence in the above studies could be explained by the use of serum NGAL which is known to detect AKI earlier in the course of the disease and rises significantly in blood and urine soon after AKI
| [30] | Zappitelli M, Washburn KK, Arikan AA, Loftis L, Ma Q, Devarajan P, et al. Urine neutrophil gelatinase-associated lipocalin is an early marker of acute kidney injury in critically ill children: a prospective cohort study. Crit Care [Internet]. 2007; 11(4): R84. Available from: https://doi.org/10.1186/cc6089 |
[30]
. This further indicates that NGAL expression increases significantly in the presence of injury to the renal epithelia.
Urine output criteria were not used in the diagnosis of AKI in this study. However, 78.1% of the study subjects had adequate urine output while oliguria was found in 14.8% of the study population indicating that oliguria is an insensitive marker of renal function, and that AKI can be seen in the absence of oliguria
| [31] | Alaro D, Bashir A, Musoke R, Wanaiana L, Bashir A. Prevalence and outcomes of acute kidney injury in term neonates with perinatal asphyxia. Afr Health Sci. 2014; |
[31]
.
6. Conclusion
The level of serum NGAL rise early during AKI following perinatal asphyxia. This rise increases with the increasing severity of perinatal asphyxia. The sensitivity using serum NGAL as a diagnostic marker in this study was very high. It is therefore, a plausible step to recommend new biomarkers like SNGAL for the early diagnosis of AKI in neonates with perinatal asphyxia.
Limitations of the Study
One of the key limitations of this study was loss to follow-up of the study participants. Majority of the patients were lost to follow-up; hence long-term follow-up was difficult.
Abbreviations
ABSUTH | Abia State University Teaching Hospital |
AKI | Acute Kidney Injury |
ELISA | Enzyme- Linked Immunosorbent Assay |
KIM-1 | Kidney Injury Molecule-1 |
NGAL | Neutrophil Gelatin-Associated Lipocalin |
NBSCU | Newborn Special Care Unit |
ROC | Receiver Operating Curve |
Acknowledgments
This study was carried out due to the untiring efforts and hard work of many individuals. I would like to express my sincere gratitude and appreciation to everyone that helped to make this work a success. I am grateful to all the babies and their parents for their support and consent. My heartfelt gratitude goes to members of staff of the NBSCU, ABSUTH, Aba.
Author Contributions
Ijeoma Umeh Stella: conceptualization of the study, writing, funding acquisition, project administration
Nneka Okoronkwo: conceptualization, supervision, and writing
Felicia Eke: Supervision, and writing
Assumpta Chapp-Jumbo: Supervision
Ngozichukwu Cynthia Ekeleme: Data curation, Formal analysis, software
Carol Iwuoha: Validation, Formal analysis, methodology
Funding
This work is not supported by any external funding.
Conflicts of Interest
The authors declare no conflicts of interests.
References
| [1] |
Agrawal S, Chaudhuri PK, Chaudhary AK, Kumar D. Acute kidney injury in asphyxiated neonates and its correlation to hypoxic ischemic encephalopathy staging. Indian J Child Health. 2016; 3(3): 254-7.
|
| [2] |
Onyiriuka NA. Birth Asphyxia in a mission hospital in Benin City, Nigeria. Trop j Obs. 2006; 23(1): 34-9.
|
| [3] |
Ogunlesi T, Oseni S. Severe Birth Asphyxia in Wesley Guild Hospital, lesa: A persistent plague! Niger Med Pract. 2008;
|
| [4] |
Jetton JG, Askenazi DJ. Update on acute kidney injury in the neonate. Curr Opin Pediatr. 2012 Apr; 24(2): 191-6.
|
| [5] |
Hoste EAJ, Clermont G, Kersten A, Venkataraman R, Angus DC, De Bacquer D, et al. RIFLE criteria for acute kidney injury are associated with hospital mortality in critically ill patients: a cohort analysis. Crit Care. 2006; 10(3): R73.
|
| [6] |
Sadoh WE, Eregie CO, Nwaneri DU, Sadoh AE. The diagnostic value of both troponin T and creatinine kinase isoenzyme (CK-MB) in detecting combined renal and myocardial injuries in asphyxiated infants. PLoS One. 2014; 9(3): 9-12.
|
| [7] |
Anochie IC, Eke FU. Acute renal failure in Nigerian children: Port Harcourt experience. Pediatr Nephrol. 2005; 20(11): 1610-4.
|
| [8] |
EE Ikpeme MU. early detection of acute kidney injury using serum neutrophil gelatinase-associated lipocalin in asphyxiated term neonates in university of uyo teaching hospital, uyo, Nigeria. african J Paediatr Nephrol. 2018; 5(1): 28-35.
|
| [9] |
Askenazi DJ, Ambalavanan N, Goldstein SL. Acute kidney injury in critically ill newborns: What do we know? What do we need to learn? 2008;
|
| [10] |
A. D, J.-P. G. Renal aspects of the term and preterm infant: A selective update. Curr Opin Pediatr. 2002;
|
| [11] |
Lameire N, Van Biesen W, Vanholder R. The changing epidemiology of acute renal failure. Nature Clinical Practice Nephrology. 2006.
|
| [12] |
Karlowicz MG, Adelman RD. Nonoliguric and oliguric acute renal failure in asphyxiated term neonates. Pediatr Nephrol. 1995.
|
| [13] |
Berl T. American Society of Nephrology renal research report. J Am Soc Nephrol. 2005; 16(7): 1886-903.
|
| [14] |
Mussap M, Degrandi R, Fravega M, Fanos V. Acute kidney injury in critically ill infants: the role of urine Neutrophil Gelatinase-Associated Lipocalin (NGAL). J Matern Fetal Neonatal Med [Internet]. 2010; 23 Suppl 3(October): 70-2. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/20807163
|
| [15] |
Mishra J, Qing MA, Prada A, Mitsnefes M, Zahedi K, Yang J, et al. Identification of neutrophil gelatinase-associated lipocalin as a novel early urinary biomarker for ischemic renal injury. J Am Soc Nephrol. 2003;
|
| [16] |
Antonucci E, Lippi G, Ticinesi A, Pigna F, Guida L, Morelli I, et al. Neutrophil gelatinase-associated lipocalin (NGAL): A promising biomarker for the early diagnosis of acute kidney injury (AKI). Acta Biomed. 2014; 85(3): 289-94.
|
| [17] |
Finster M, Wood M. The Apgar score has survived the test of time. Anesthesiology. 2005;
|
| [18] |
Aliyu I, Lawal T, Onankpa B. Hypoxic-ischemic encephalopathy and the Apgar scoring system: The experience in a resource-limited setting YR - 2018/1/1. J Clin Sci. (1 UL-
https://www.jcsjournal.org/article.asp?issn=2468-6859;year=2018;volume=15;issue=1;spage=18;epage=21;aulast=Aliyu;t=5):18 OP-21 VO - 15
|
| [19] |
Mathur NB, Agarwal HS, Maria A. Acute renal failure in neonatal sepsis. Indian J Pediatr [Internet]. 2006; 73(6): 499-502. Available from:
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=16816511
|
| [20] |
Sarnat HB, Sarnat MS. Neonatal Encephalopathy Following Fetal Distress: A Clinical and Electroencephalographic Study. Arch Neurol. 1976; 33(10): 696-705.
|
| [21] |
Lolekha PH, Jaruthunyaluck S, Srisawasdi P. Deproteinization of serum: Another best approach to eliminate all forms of bilirubin interference on serum creatinine by the kinetic Jaffe reaction. J Clin Lab Anal. 2001;
|
| [22] |
Krawczeski CD, Woo JG, Wang Y, Bennett MR, Ma Q, Devarajan P. Neutrophil Gelatinase-Associated Lipocalin Concentrations Predict Development of Acute Kidney Injury in Neonates and Children after Cardiopulmonary Bypass. J Pediatr [Internet]. 2011 Jun 1; 158(6): 1009-1015. e1. Available from:
https://doi.org/10.1016/j.jpeds.2010.12.057
|
| [23] |
Essajee F, Were F, Admani B. Urine neutrophil gelatinase-associated lipocalin in asphyxiated neonates: a prospective cohort study. Pediatr Nephrol. 2015; 30(7): 1189-96.
|
| [24] |
Pejović B, Erić-Marinković J, Pejović M, Kotur-Stevuljević J, Peco-Antić A. Detection of acute kidney injury in premature asphyxiated neonates by serum neutrophil gelatinase-associated lipocalin (sNGAL) - Sensitivity and specificity of a potential new biomarker. Biochem Medica. 2015; 25(3): 450-9.
|
| [25] |
Abdelhady S, Gawad ERA, Haie OMA, Mansour AI. Usefulness of Serum and Urinary Neutrophil Gelatinase -Associated Lipocalin in Detecting Acute Kidney Injury in Asphyxiated Neonates. Int J Med Heal Sci. 2016; 5(4).
|
| [26] |
El Raggal NM, Khafagy SM, Mahmoud NH, El Beltagy SA. Serum neutrophil gelatinase-associated lipocalin as a marker of acute kidney injury in asphyxiated neonates. Indian Pediatr. 2013; 50(5): 459-62.
|
| [27] |
Gupta BD, Sharma P, Bagla J, Parakh M, Soni JP. Renal failure in asphyxiated neonates. Indian Pediatr. 2005;
|
| [28] |
Kaur S, Jain S, Saha a, Chawla D, Parmar VR, Basu S, et al. Evaluation of glomerular and tubular renal function in neonates with birth asphyxia. Ann Trop Paediatr. 2011; 31(2): 129-34.
|
| [29] |
Emmanuel IE, Tony DO, Paulinus UM, J UJ. Incidence of acute kidney injury in asphyxiated babies in university of Uyo teaching hospital, Uyo, Nigeria. 2020; 8(7): 2477-81.
|
| [30] |
Zappitelli M, Washburn KK, Arikan AA, Loftis L, Ma Q, Devarajan P, et al. Urine neutrophil gelatinase-associated lipocalin is an early marker of acute kidney injury in critically ill children: a prospective cohort study. Crit Care [Internet]. 2007; 11(4): R84. Available from:
https://doi.org/10.1186/cc6089
|
| [31] |
Alaro D, Bashir A, Musoke R, Wanaiana L, Bashir A. Prevalence and outcomes of acute kidney injury in term neonates with perinatal asphyxia. Afr Health Sci. 2014;
|
Cite This Article
-
APA Style
Ijeoma, S., Okoronkwo, N., Eke, F., Chapp-Jumbo, A., Ekeleme, N., et al. (2025). Serum Neutrophil Gelatinase-Associated Lipocalin as a Biomarker of Acute Kidney Injury in Babies with Perinatal Asphyxia in Abia State, South-East Nigeria. American Journal of Pediatrics, 11(3), 156-165. https://doi.org/10.11648/j.ajp.20251103.17
 Copy
|
Copy
|
 Download
Download
ACS Style
Ijeoma, S.; Okoronkwo, N.; Eke, F.; Chapp-Jumbo, A.; Ekeleme, N., et al. Serum Neutrophil Gelatinase-Associated Lipocalin as a Biomarker of Acute Kidney Injury in Babies with Perinatal Asphyxia in Abia State, South-East Nigeria. Am. J. Pediatr. 2025, 11(3), 156-165. doi: 10.11648/j.ajp.20251103.17
Copy
|
Download
AMA Style
Ijeoma S, Okoronkwo N, Eke F, Chapp-Jumbo A, Ekeleme N, et al. Serum Neutrophil Gelatinase-Associated Lipocalin as a Biomarker of Acute Kidney Injury in Babies with Perinatal Asphyxia in Abia State, South-East Nigeria. Am J Pediatr. 2025;11(3):156-165. doi: 10.11648/j.ajp.20251103.17
Copy
|
Download
-
@article{10.11648/j.ajp.20251103.17,
author = {Stella Ijeoma and Nneka Okoronkwo and Felicia Eke and Assumpta Chapp-Jumbo and Ngozichukwu Ekeleme and Carol Iwuoha},
title = {Serum Neutrophil Gelatinase-Associated Lipocalin as a Biomarker of Acute Kidney Injury in Babies with Perinatal Asphyxia in Abia State, South-East Nigeria
},
journal = {American Journal of Pediatrics},
volume = {11},
number = {3},
pages = {156-165},
doi = {10.11648/j.ajp.20251103.17},
url = {https://doi.org/10.11648/j.ajp.20251103.17},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajp.20251103.17},
abstract = {Introduction: Acute Kidney Injury (AKI) is a major cause of mortality and long-term morbidity. It is a very common complication in asphyxiated newborns. Early detection of AKI in these cohort of patients will positively impact outcome. Serum Neutrophil Gelatin-associated lipocalin (NGAL) is a highly sensitive biomarker of AKI. There is paucity of data on the determination of the incidence of AKI in asphyxiated babies using Serum NGAL as a biomarker. Objective: This study was set to evaluate the use of serum NGAL measurement for early detection of AKI in babies with perinatal asphyxia at the Abia State University Teaching Hospital (ABSUTH), Aba. Methods: This was a cross-sectional descriptive study done at the Newborn Special Care Unit of ABSUTH, Aba, Nigeria. Serum NGAL estimation was done within the first six hours of delivery. Also, serum creatinine was done daily for the first week of admission. Results: A total of 155 term neonates with perinatal asphyxia were studied. The male to female ratio was 1.06:1. Among these neonates, 43.9% had mild, 29.0% had moderate and 27.1% had severe perinatal asphyxia respectively. The mean serum NGAL concentration in those with mild, moderate and severe perinatal asphyxia were 345.3ng/ml, 673.1ng/ml, and 866.1ng/ml, respectively. A statistically significant difference was observed in these mean serum NGAL concentrations (p valueConclusion: Serum NGAL is a highly sensitive biomarker of AKI. Serum NGAL levels measured within the first six hours after birth is elevated in patients with AKI. NGAL estimation in the first 6 hours of the birth of asphyxiated neonates is recommended for early detection of AKI.},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Serum Neutrophil Gelatinase-Associated Lipocalin as a Biomarker of Acute Kidney Injury in Babies with Perinatal Asphyxia in Abia State, South-East Nigeria
AU - Stella Ijeoma
AU - Nneka Okoronkwo
AU - Felicia Eke
AU - Assumpta Chapp-Jumbo
AU - Ngozichukwu Ekeleme
AU - Carol Iwuoha
Y1 - 2025/07/28
PY - 2025
N1 - https://doi.org/10.11648/j.ajp.20251103.17
DO - 10.11648/j.ajp.20251103.17
T2 - American Journal of Pediatrics
JF - American Journal of Pediatrics
JO - American Journal of Pediatrics
SP - 156
EP - 165
PB - Science Publishing Group
SN - 2472-0909
UR - https://doi.org/10.11648/j.ajp.20251103.17
AB - Introduction: Acute Kidney Injury (AKI) is a major cause of mortality and long-term morbidity. It is a very common complication in asphyxiated newborns. Early detection of AKI in these cohort of patients will positively impact outcome. Serum Neutrophil Gelatin-associated lipocalin (NGAL) is a highly sensitive biomarker of AKI. There is paucity of data on the determination of the incidence of AKI in asphyxiated babies using Serum NGAL as a biomarker. Objective: This study was set to evaluate the use of serum NGAL measurement for early detection of AKI in babies with perinatal asphyxia at the Abia State University Teaching Hospital (ABSUTH), Aba. Methods: This was a cross-sectional descriptive study done at the Newborn Special Care Unit of ABSUTH, Aba, Nigeria. Serum NGAL estimation was done within the first six hours of delivery. Also, serum creatinine was done daily for the first week of admission. Results: A total of 155 term neonates with perinatal asphyxia were studied. The male to female ratio was 1.06:1. Among these neonates, 43.9% had mild, 29.0% had moderate and 27.1% had severe perinatal asphyxia respectively. The mean serum NGAL concentration in those with mild, moderate and severe perinatal asphyxia were 345.3ng/ml, 673.1ng/ml, and 866.1ng/ml, respectively. A statistically significant difference was observed in these mean serum NGAL concentrations (p valueConclusion: Serum NGAL is a highly sensitive biomarker of AKI. Serum NGAL levels measured within the first six hours after birth is elevated in patients with AKI. NGAL estimation in the first 6 hours of the birth of asphyxiated neonates is recommended for early detection of AKI.
VL - 11
IS - 3
ER -
Copy
|
Download