Background: Although there are several clinical studies available regarding the management of acid peptic disorders (APD), there is a dearth of studies among clinical experts on their practice. This study aimed to assess clinicians’ perspectives on the management of APD, with particular emphasis on the emerging role of vonoprazan in routine clinical practice in Indian settings. Methodology: This cross-sectional study included 209 clinical experts across India. A validated 22-item questionnaire assessed key aspects of APD management, including epidemiology, diagnostics, treatment practices, challenges related to proton pump inhibitor (PPI) therapy, and perceptions of vonoprazan. Data were analyzed using descriptive statistics. Results: In routine clinical practice, approximately 51% of clinicians reported that about 11–25% of their patients with gastroesophageal reflux disease (GERD) do not respond adequately to PPI therapy, while 49% indicated that nocturnal acid breakthrough is commonly encountered during PPI use. Nearly 63% of respondents emphasized vonoprazan’s unique mechanism of action as its key advantage over PPIs, enabling faster and more prolonged binding to the H⁺/K⁺-ATPase enzyme and providing sustained 24-hour acid suppression. Approximately 42% of clinicians preferred vonoprazan for GERD, while 41.63% favored its use in 11–25% of patients with nonerosive reflux disease, and 38.76% preferred its use across all age groups in PPI-resistant cases. In the setting of NSAID-induced ulcer recurrence, around 55% of respondents reported using vonoprazan in selected cases. Overall, 73% perceived multiple benefits of vonoprazan, including the absence of a requirement for metabolic activation, more rapid intragastric pH elevation, and acid stability with reversible inhibition, allowing meal-independent dosing. Conclusion: This survey highlights important limitations of PPI therapy and strong clinician recognition of vonoprazan’s pharmacological and clinical advantages. The findings suggest strategic use of vonoprazan in patients with an inadequate response to PPIs, particularly in GERD and PPI-resistant cases, positioning it as a valuable therapeutic option for addressing unmet needs in the management of acid-related disorders.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
The global burden of acid peptic diseases (APDs) continues to rise, largely driven by changing lifestyles and dietary habits. In India, gastroesophageal reflux disease (GERD) is particularly prevalent, affecting 39.2% of the population, followed by peptic ulcer disease (PUD) at 37.1% and non-ulcer dyspepsia at 25.2%.
[1]
Juneja HT, Gambhir S, Junaidy KH. Optimizing Proton-pump Inhibitor Therapy in Patients with Comorbidities Receiving Polypharmacy Treatment: Insights from Clinical Practice in India. J Assoc Physicians India. 2025; 73(10): e38–41.
On a global scale, data from the 2021 Global Burden of Disease (GBD) Study estimate that GERD affected approximately 825.6 million individuals in 2021 (95% uncertainty interval: 732.99–925.56 million). Between 1990 and 2021, GERD-related incident cases, prevalence, and years lived with disability increased by 83.16%, 80.06%, and 82.46%, respectively, highlighting the growing public health impact of the disease.
[2]
Mo L, Liu Z, Cao W, Gong H, Wu J, Lin M, et al. Global, regional, and national burden of gastroesophageal reflux disease (1990-2021): age-period-cohort analysis and Bayesian projections. Front Public Health. 2025; 13: 1576527.
The absolute number of PUD cases increased by approximately 50% in regions with a low sociodemographic index, underscoring persistent health inequities and the influence of population growth and limited access to care.
[3]
Zhang T, Zhang B, Tang X. Global Burden of Peptic Ulcer Disease in Adolescents and Young Adults: Trends and Disparities from 1990-2021. Arch Med Res. 2025; 56(8): 103320.
GERD significantly impairs patients’ health-related quality of life due to its chronic and relapsing nature. Its high prevalence translates into a considerable economic burden, affecting patients and their families as well as healthcare systems and society at large. The long-term management of GERD requires substantial healthcare resources and contributes to rising societal costs. Similarly, PUD continues to impose a notable economic burden on healthcare systems worldwide, reinforcing the need for effective prevention and optimized management strategies for acid-related disorders.
[3]
Zhang T, Zhang B, Tang X. Global Burden of Peptic Ulcer Disease in Adolescents and Young Adults: Trends and Disparities from 1990-2021. Arch Med Res. 2025; 56(8): 103320.
Zhang D, Liu S, Li Z, Wang R. Global, regional and national burden of gastroesophageal reflux disease, 1990–2019: update from the GBD 2019 study. Ann Med. 2022; 54(1): 1372–84.
Suppression of gastric acid secretion has long been the cornerstone of therapy for APDs. PPIs have played a central role in their management; however, their clinical effectiveness is limited in a subset of patients. Key challenges include refractoriness or treatment failure due to inadequate acid suppression in some patients with GERD, poor adherence related to complex dosing regimens, interindividual variability in therapeutic response, and phenomena such as nocturnal acid breakthrough.
[5]
Upadhyay R, Soni NK, Vora A, Saraf A, Haldipur D, Mukherjee D, et al. Association of Physicians of India Consensus Recommendations for Vonoprazan in Management of Acid Peptic Disorders. J Assoc Physicians India. 2025; 73(2): 68–77.
Vonoprazan is a novel potassium-competitive acid blocker (P-CAB) developed as an alternative to conventional PPIs for the treatment of acid-related gastrointestinal disorders. Unlike PPIs, which inhibit the H⁺/K⁺-ATPase enzyme in a delayed and sometimes variable manner, vonoprazan directly and competitively blocks the potassium-binding site of the enzyme. This mechanism results in a faster onset of action and more sustained suppression of gastric acid secretion. Owing to its distinctive pharmacological profile, vonoprazan provides more consistent and potent acid control, positioning it as a promising therapeutic option for patients with acid-related conditions.
[6]
Fung S. Vonoprazan: A Review in Erosive Esophagitis and Non-Erosive Gastro-Esophageal Reflux Disease. Drugs. 2025; 85(7): 945-955.
Despite growing evidence supporting vonoprazan's efficacy and safety profile, data on clinician perspectives regarding its role in routine practice remain limited, particularly in the Indian clinical context. Understanding how practicing clinicians perceive the limitations of current PPI therapy and the potential advantages of vonoprazan is essential for optimizing treatment strategies and addressing unmet clinical needs in APD management.
2. Materials and Methods
2.1. Study Settings
A cross-sectional study was carried out among clinicians involved in the management of APD in the major Indian cities from June 2025 to December 2025. The study was performed in accordance with Bangalore Ethics, an Independent Ethics Committee (ECR/355/Indt/KA/2022), which was recognized by the Indian Regulatory Authority, the Drug Controller General of India.
2.2. Study Participants
An invitation was sent to leading clinicians (Gastroenterologists, Consulting Physicians, General Surgeons) in managing APD in the month of March 2025 for participation in this Indian survey. About 209 clinicians from major cities of all Indian states, representing the geographical distribution, shared their willingness to participate and provide necessary data.
2.3. Study Procedure
The questionnaire booklet titled VIVID (Vonoprazan in Potassium Acid Blocker Study) was sent to the clinicians who were interested in participating in the survey. The study questionnaire comprised 22 questions that assessed multiple dimensions of APD management. It covered epidemiology and clinical presentation in routine practice, diagnostic approaches and common comorbidities, current treatment strategies and preferred therapeutic agents, challenges associated with PPI therapy, including treatment resistance and nocturnal acid breakthrough, clinicians’ perceptions of vonoprazan and its advantages, preferred patient populations and clinical scenarios for vonoprazan use, and approaches to patient education. Reliability, as determined by a split-half test (coefficient alpha), was adequate but should be improved in future versions of the questionnaire. A study of criterion validity was undertaken to test the questionnaire and to develop methods of testing the validity of measures of Physicians' Perspectives. However, the extraneous variables in this include the clinician's experience, usage of the newer drugs, etc. The two criteria used were the doctors' perspectives from the clinical practice and the assessment of an external assessor and statistician. Clinicians had the option to skip questions as desired and were instructed to complete the survey independently, without peer consultation. Before participating in the survey, all respondents provided written informed consent.
2.4. Statistical Analysis
The data were analyzed using descriptive statistics. Categorical variables were presented as percentages to provide a clear understanding of their distribution. The frequency of occurrence and the corresponding percentage were used to represent the distribution of each variable. To visualize the distribution of the categorical variables, pie and bar charts were created using Microsoft Excel 2013 (version 2409, build 16.0.18025.20030).
3. Results
The majority of clinicians (88.04%) reported GERD as the most common gastrointestinal condition encountered in their clinical practice. Around 45% reported that 26–40% of their patients have APDs in their clinical practice. The majority of clinicians (66.99%) identified heartburn as the most common presenting symptom of GERD in their clinical practice. Approximately 48% reported diabetes mellitus as the most common comorbid condition associated with APDs in their clinical practice. According to 73% of respondents, patients’ lifestyle is highly influential in the incidence of GERD. Nearly 66% stated GERD as the most common form of APD encountered in their daily clinical practice.
A large proportion of clinicians (62.2%) reported an equal prevalence of APD among male and female patients in their clinical practice. Around 54% indicated that APD is most frequently encountered among patients aged 26–40 years in routine clinical practice. According to 56% of experts, they sometimes encounter H. pylori infection in their routine clinical practice. Nearly 62% identified obesity as the predominant risk factor for GERD in their clinical opinion. Approximately 71% of clinicians most frequently encountered Barrett’s esophagitis as the predominant long-term complication of GERD in their clinical practice. Nearly 59% most commonly relied on upper GI endoscopy as the most dependable diagnostic modality for GERD in routine clinical practice. A predominant proportion of clinicians (50.72%) favored social media as the preferred platform for patient education in their clinical practice.
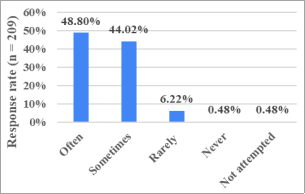
An overwhelming proportion of clinicians (87.08%) preferred PPIs as the primary drug group for the management of APD in their clinical practice. Around 44% indicated that approximately 11–25% of their GERD patients are resistant to treatment in routine clinical practice. Nearly 51% stated that approximately 11–25% of their GERD patients do not respond to PPI therapy in routine clinical practice (Table 1). Approximately 49% of clinicians reported that nocturnal acid breakthrough is often encountered in patients receiving PPIs in their clinical settings (Figure 1).
Table 1. Distribution of responses to the proportion of GERD patients not responding to PPIs in clinical practice.
Figure 1. Distribution of responses to frequency of nocturnal acid breakthrough in patients on PPIs in clinical practice.
A large proportion of clinicians (63.16%) supported vonoprazan’s unique mechanism of action, which allows faster and longer binding to the H⁺/K⁺-ATPase enzyme with sustained 24-hour acid suppression, as its key advantage over PPIs (Table 2). Nearly 42% preferred vonoprazan for patients with GERD, indicating this as the preferred patient group for its use in routine practice (Table 3).
Table 2. Distribution of responses to clinicians’ views on the advantages of vonoprazan compared to PPIs.
Advantages
Response rate (n = 209)
Vonoprazan rapidly accumulates in the canalicular membranes of parietal cells
13 (6.22%)
Vonoprazan stably accumulates in the acidic secretory canaliculus
7 (3.35%)
Vonoprazan does not require any activation and is stable in the acidic environment
49 (23.44%)
Unique mechanism of action results in vonoprazan binding faster and longer to H+ K+ -ATPases enzyme, resulting in 24-hour acid control activity
132 (63.16%)
All of the above
6 (2.87%)
Efficacy highly acceptable
1 (0.48%)
Not attempted
1 (0.48%)
Table 3. Distribution of responses to preferred patient groups for vonoprazan use in clinical practice.
Patient groups
Response rate (n = 209)
Gastroesophageal reflux disease
87 (41.63%)
Gastric ulcer
27 (12.92%)
Duodenal ulcer
9 (4.31%)
Prevention of recurrence of gastric ulcer, duodenal ulcer, and NSAID administration
53 (25.36%)
Adjunct to Helicobacter pylori eradication
22 (10.53%)
All of the above
10 (4.78%)
Not attempted
1 (0.48%)
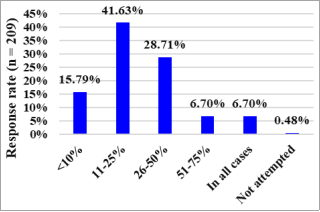
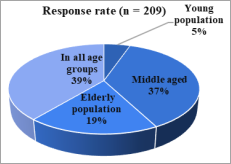
Around 42% of experts indicated a preference for using vonoprazan in 11–25% of patients with NERD (Figure 2). Nearly 39% expressed a preference for using vonoprazan across all age groups in PPI-resistant cases (Figure 3). According to 55% of clinicians, they would use vonoprazan in a few selected cases of NSAID-induced ulcer recurrence, reflecting a cautious and individualized approach in routine practice (Table 4). Approximately 73% of clinicians perceived that vonoprazan offers multiple benefits, including the absence of a requirement for metabolic activation, a more rapid increase in intragastric pH compared with PPIs, and acid stability with reversible inhibition that allows dosing independent of mealtimes (Table 5).
Figure 3. Distribution of responses to preferred age group for using vonoprazan in PPI-resistant cases.
Table 4. Distribution of responses to the use of vonoprazan in NSAID-induced ulcer recurrence in clinical practice.
Response
Response rate (n = 209)
Yes, in all cases
60 (28.71%)
Yes, in a few selected cases
114 (54.55%)
Need more data
31 (14.83%)
Especially in renal-compromised patients
3 (1.44%)
Not attempted
1 (0.48%)
Table 5. Distribution of Responses to Perceived Benefits of Vonoprazan According to Clinicians.
Benefit
Response rate (n = 209)
Not require transformation (active drug)
5 (2.39%)
More rapidly increases intragastric pH when compared with PPIs
16 (7.66%)
In contrast to PPIs, vonoprazan is acid-stable and facilitates reversible inhibition and can be dosed independent of mealtimes
34 (16.27%)
All the above
153 (73.21%)
Not attempted
1 (0.48%)
4. Discussion
This survey provides valuable insight into clinicians’ perceptions of the limitations of PPI therapy and the emerging role of vonoprazan in routine practice. More than half of the respondents (51.20%) indicated that 11–25% of their patients do not respond adequately to PPIs. This treatment gap, coupled with the high prevalence of nocturnal acid breakthrough (48.80% of clinicians reporting frequent encounters) in patients receiving PPIs, underscores persistent clinical challenges in achieving adequate acid suppression with conventional therapy. Although PPIs are well established to markedly suppress gastric acid secretion, leading to high rates of esophageal mucosal healing and rapid relief of GERD-related symptoms
[6]
Fung S. Vonoprazan: A Review in Erosive Esophagitis and Non-Erosive Gastro-Esophageal Reflux Disease. Drugs. 2025; 85(7): 945-955.
Dickman R, Boaz M, Aizic S, Beniashvili Z, Fass R, Niv Y. Comparison of clinical characteristics of patients with gastroesophageal reflux disease who failed proton pump inhibitor therapy versus those who fully responded. J Neurogastroenterol Motil. 2011; 17(4): 387–94.
, increasing evidence over recent years highlights a substantial proportion of treatment failures. It is now estimated that nearly 10–40% of patients with GERD continue to experience persistent symptoms despite standard-dose PPI therapy.
[7]
Dickman R, Boaz M, Aizic S, Beniashvili Z, Fass R, Niv Y. Comparison of clinical characteristics of patients with gastroesophageal reflux disease who failed proton pump inhibitor therapy versus those who fully responded. J Neurogastroenterol Motil. 2011; 17(4): 387–94.
A healthcare provider survey conducted by the International Working Group for the Classification of Oesophagitis (IWGCO) steering committee, involving 113 clinicians, reported incomplete symptom control with once-daily PPI therapy in more than 20% of patients, as noted by 64.6% of gastroenterologists and 14.7% of non-gastroenterologists. Even with twice-daily dosing, an inadequate response in over 20% of patients was still reported by 31.6% of gastroenterologists and 11.8% of non-gastroenterologists.
[8]
Armstrong D, Hungin AP, Kahrilas PJ, Sifrim D, Sinclair P, Vaezi MF, et al. Knowledge gaps in the management of refractory reflux‐like symptoms: Healthcare provider survey. Neurogastroenterol Motil. 2022; 34(10): e14387.
Nocturnal acid breakthrough has been reported in over 70% of H. pylori–negative patients receiving PPI therapy and is clinically significant, particularly among individuals with complicated GERD, Barrett’s esophagus, and underlying esophageal motility disorders.
[9]
Tutuian R, Castell DO. Nocturnal Acid Breakthrough -- Approach to Management. MedGenMed. 2004; 6(4): 11.
[9]
In a study by Karyampudi et al., nocturnal acid breakthrough was observed in 72.4% of patients with GERD receiving PPI therapy.
[10]
Karyampudi A, Ghoshal UC, Singh R, Verma A, Misra A, Saraswat VA. Esophageal Acidification During Nocturnal Acid-breakthrough with Ilaprazole Versus Omeprazole in Gastroesophageal Reflux Disease. J Neurogastroenterol Motil. 2017; 23(2): 208–17.
The strong recognition of vonoprazan's mechanism of action as its primary advantage (63.16%) suggests clinicians appreciate the pharmacological distinctions between potassium-competitive acid blockers and traditional PPIs. The widespread recognition of vonoprazan's multiple clinical benefits (73.21%), including acid stability, meal-independent dosing, and elimination of metabolic activation requirements, highlights appreciation for practical advantages that may improve treatment adherence and outcomes.
Vonoprazan differs from PPIs in its mechanism of action by reversibly inhibiting the H⁺/K⁺-ATPase through competitive blockade of potassium ion binding, whereas PPIs act irreversibly on the proton pump. This reversible inhibition leads to a marked reduction in gastric acid secretion, with vonoprazan demonstrating substantially greater potency than PPIs. Owing to its reversible binding, vonoprazan has a faster onset of action and provides more sustained acid suppression compared with conventional PPIs. In addition, vonoprazan inhibits the proton pump across all phases of its catalytic cycle without requiring acid activation, further contributing to its strong and prolonged acid-suppressive effect. Clinical studies have shown that vonoprazan achieves rapid and robust acid suppression, reaching peak plasma levels within a short time. Its slower dissociation from the proton pump results in a prolonged duration of acid inhibition, supported by a relatively long plasma half-life. Furthermore, vonoprazan exhibits stable plasma concentrations and consistent antisecretory effects, with its efficacy remaining largely unaffected by food intake or genetic polymorphisms that commonly influence the performance of PPIs.
[11]
Padwale V, Kirnake V, Daswani R, Kodmalwar A, Gupta A. A Comprehensive Review on the Efficacy and Safety of Vonoprazan in the Management of Gastric Acid-Related Diseases. Cureus. 2024; 16(7): e64777.
Tian L, Xiang D, Yue F, Li R, Zhou Y. Efficacy and safety of vonoprazan versus proton pump inhibitors in the treatment of peptic ulcer disease: a systematic review and network meta-analysis for randomized controlled trails. Front Nutr. 2024; 11: 1436993.
Perception mapping research underscores the importance of evaluating vonoprazan’s clinical role in the Indian setting, particularly in overcoming the limitations of conventional PPIs. The Vonoprazan Advisory Strategy Team (VAST-1) consensus, involving 850 gastrointestinal experts with extensive cumulative clinical experience, demonstrated a strong preference for vonoprazan across multiple acid-related disorders. Vonoprazan was consistently rated superior to PPIs due to its rapid onset of action, pH-independent mechanism, effective nocturnal acid control, and efficacy in refractory and PPI-resistant GERD. It also showed comparable ulcer healing with shorter treatment durations and a favorable safety profile. Overall, the findings highlight vonoprazan as a transformative and superior acid suppressant, well-positioned to address unmet clinical needs in routine Indian practice.
[13]
Chandrasekhar TS, Puri R, Dhawan P, Abraham P, Appasani S, Pratap N, et al. Perception mapping of vonoprazan: expert consensus on its efficacy and clinical utility in acid-related disorders in India. Gut. 2025; 74(Suppl 1): P130.
[13]
This understanding of its mechanism is perceived to be translating into clinical decision-making, with GERD emerging as the predominant indication (41.63%) in the present survey, likely driven by the need for more robust acid suppression in patients with inadequate PPI response. The preference for vonoprazan in 11–25% of NERD patients (41.63%) in the current survey reflects a measured approach to adoption, suggesting that clinicians are selectively targeting cases where conventional therapy has proven insufficient.
As per the consensus of the Association of Physicians of India, vonoprazan, with its superior efficacy and favorable safety profile across mild to severe acid peptic disorders, including GERD, erosive esophagitis, NERD, and H. pylori infection, shows strong potential to emerge as a frontline therapy in the management of APDs.
[5]
Upadhyay R, Soni NK, Vora A, Saraf A, Haldipur D, Mukherjee D, et al. Association of Physicians of India Consensus Recommendations for Vonoprazan in Management of Acid Peptic Disorders. J Assoc Physicians India. 2025; 73(2): 68–77.
A systematic review by Silva et al. reported that, in GERD, vonoprazan was a superior treatment option compared with PPIs in half of the included studies, while the remaining studies found the two therapies to be equally effective.
[14]
Silva GA, Figueiredo JS, Gonçalves RJ, Barbosa MG, Chehter EZ. Vonoprazan: A systematic review of an alternative to proton pump inhibitors. GHOA. 2022; 13(6): 221–31.
A randomized trial by Laine et al. demonstrated that vonoprazan reduced heartburn symptoms in subjects diagnosed with NERD, with benefits appearing as early as the first day of therapy. The treatment effect persisted after the initial 4-week placebo-controlled period throughout the 20-week extension period.
[15]
Laine L, Spechler S, Yadlapati R, Schnoll-Sussman F, Smith N, Leifke E, et al. Vonoprazan is Efficacious for Treatment of Heartburn in Non-erosive Reflux Disease: A Randomized Trial. Clin Gastroenterol Hepatol. 2024; 22(11): 2211-2220.e10.
Another study by Hoshikawa et al. demonstrated that on-demand therapy with vonoprazan 20 mg was as effective as continuous PPI maintenance therapy in patients with NERD.
[16]
Hoshikawa Y, Kawami N, Hoshino S, Tanabe T, Umezawa M, Kaise M, et al. Efficacy of on-demand therapy using 20-mg vonoprazan for non-erosive reflux disease. Esophagus. 2019; 16(2): 201–6.
Similarly, the current survey, revealing age-agnostic utilization in PPI-resistant cases (38.76%), indicates that treatment decisions are guided more by therapeutic response than by demographic factors. A systematic review and meta-analysis by Simadibrata et al. showed that vonoprazan has high efficacy in the healing and maintenance of PPI-resistant erosive esophagitis and provides moderate improvement in Frequency Scale for Symptoms of GERD (FSSG) scores. Vonoprazan was also well tolerated in patients with PPI-resistant GERD.
[17]
Simadibrata DM, Lesmana E, Fass R. A systematic review and meta-analysis of the efficacy of vonoprazan for proton pump inhibitor-resistant gastroesophageal reflux disease. J Gastroenterol Hepatol. 2024; 39(5): 796–805.
A study by Niikura et al. reported that switching therapy from a PPI to vonoprazan was significantly associated with improvement in gastroesophageal reflux symptoms. These findings highlight vonoprazan as a highly promising therapeutic option for patients with PPI-resistant GERD.
[18]
Niikura R, Yamada A, Hirata Y, Hayakawa Y, Takahashi A, Shinozaki T, et al. Efficacy of Vonoprazan for Gastroesophageal Reflux Symptoms in Patients with Proton Pump Inhibitor-resistant Non-erosive Reflux Disease. Intern Med. 2018; 57(17): 2443–50.
The majority of clinicians in the current survey preferred vonoprazan in a few selected cases of NSAID-induced ulcer recurrence. Kawai et al. reported no new safety concerns with vonoprazan when used for the prevention of secondary ulcers or bleeding in patients receiving long-term NSAID therapy. In this real-world study, vonoprazan was also effective in preventing the recurrence of NSAID-associated peptic ulcers.
[19]
Kawai T, Suzuki C, Honda Y, Fernandez JL. Long-term safety and effectiveness of vonoprazan for prevention of gastric and duodenal ulcer recurrence in patients on nonsteroidal anti-inflammatory drugs in Japan: a 12-month post-marketing surveillance study. Expert Opin Drug Saf. 2023; 22(5): 425–31.
In a phase 3 randomized study with a long-term extension, vonoprazan demonstrated non-inferiority to lansoprazole for the secondary prevention of NSAID-induced peptic ulcers in patients receiving long-term NSAID therapy. Both vonoprazan doses (10 mg and 20 mg) were associated with lower or comparable rates of ulcer recurrence over 24 weeks compared with lansoprazole, with no new or significant safety concerns.
[20]
Mizokami Y, Oda K, Funao N, Nishimura A, Soen S, Kawai T, et al. Vonoprazan prevents ulcer recurrence during long-term NSAID therapy: randomised, lansoprazole-controlled non-inferiority and single-blind extension study. Gut. 2018; 67(6): 1042–51.
This survey highlights a significant therapeutic gap in the management of acid-related disorders, with over half of clinicians reporting inadequate PPI response in 11–25% of their patients. The high frequency of nocturnal acid breakthrough further emphasizes substantial unmet clinical needs. Clinicians strongly recognized vonoprazan’s distinct mechanism as a potassium-competitive acid blocker and its practical advantages, including acid stability, meal-independent dosing, and consistent efficacy irrespective of genetic polymorphisms. These findings collectively indicate the strategic adoption of vonoprazan for PPI-resistant GERD and selected patient subgroups, positioning it as a potentially transformative option to overcome key limitations of conventional acid-suppressive therapy in the Indian clinical context.
A major strength of the study is the use of a carefully designed and validated questionnaire to capture expert perspectives. However, the reliance on clinician perceptions rather than objective patient outcome data introduces potential recall and subjective bias. Limited reporting on sample size, geographic distribution, and practice settings restricts generalizability. The absence of longitudinal outcome data, real-world comparative effectiveness analyses, and evaluation of adoption barriers such as cost and availability are additional limitations. Furthermore, long-term safety data and identification of patient subgroups deriving the greatest benefit remain unaddressed, and response bias cannot be excluded.
5. Conclusions
This survey underscores significant treatment gaps in current PPI therapy and reveals strong clinician appreciation for vonoprazan's pharmacological and clinical advantages. The findings suggest vonoprazan is being adopted strategically for patients with inadequate PPI response, particularly in GERD and PPI-resistant cases, positioning it as a valuable therapeutic option to address unmet clinical needs in acid-related disorder management.
Abbreviations
APDs
Acid Peptic Disorders
GERD
Gastroesophageal Reflux Disease
PUD
Peptic Ulcer Disease
GBD
Global Burden of Disease
PPIs
Proton Pump Inhibitors
P-CAB
Potassium-Competitive Acid Blocker
H⁺/K⁺-ATPase
Hydrogen/Potassium Adenosine Triphosphatase
NERD
Nonerosive Reflux Disease
NSAID
Nonsteroidal Anti-Inflammatory Drug
H. pylori
Helicobacter Pylori
GI
Gastrointestinal
IWGCO
International Working Group for the Classification of Oesophagitis
FSSG
Frequency Scale for Symptoms of Gastroesophageal Reflux Disease
DCGI
Drug Controller General of India
UI
Uncertainty Interval
Acknowledgments
We would like to thank all the clinicians who participated in this study.
Krishna Kumar Manjunath: Data curation, Formal Analysis, Investigation, Visualization, Writing – original draft, Writing – review & editing
Data Availability Statement
The data is available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
Juneja HT, Gambhir S, Junaidy KH. Optimizing Proton-pump Inhibitor Therapy in Patients with Comorbidities Receiving Polypharmacy Treatment: Insights from Clinical Practice in India. J Assoc Physicians India. 2025; 73(10): e38–41.
Mo L, Liu Z, Cao W, Gong H, Wu J, Lin M, et al. Global, regional, and national burden of gastroesophageal reflux disease (1990-2021): age-period-cohort analysis and Bayesian projections. Front Public Health. 2025; 13: 1576527.
Zhang T, Zhang B, Tang X. Global Burden of Peptic Ulcer Disease in Adolescents and Young Adults: Trends and Disparities from 1990-2021. Arch Med Res. 2025; 56(8): 103320.
Zhang D, Liu S, Li Z, Wang R. Global, regional and national burden of gastroesophageal reflux disease, 1990–2019: update from the GBD 2019 study. Ann Med. 2022; 54(1): 1372–84.
Upadhyay R, Soni NK, Vora A, Saraf A, Haldipur D, Mukherjee D, et al. Association of Physicians of India Consensus Recommendations for Vonoprazan in Management of Acid Peptic Disorders. J Assoc Physicians India. 2025; 73(2): 68–77.
Dickman R, Boaz M, Aizic S, Beniashvili Z, Fass R, Niv Y. Comparison of clinical characteristics of patients with gastroesophageal reflux disease who failed proton pump inhibitor therapy versus those who fully responded. J Neurogastroenterol Motil. 2011; 17(4): 387–94.
Tutuian R, Castell DO. Nocturnal Acid Breakthrough -- Approach to Management. MedGenMed. 2004; 6(4): 11.
[10]
Karyampudi A, Ghoshal UC, Singh R, Verma A, Misra A, Saraswat VA. Esophageal Acidification During Nocturnal Acid-breakthrough with Ilaprazole Versus Omeprazole in Gastroesophageal Reflux Disease. J Neurogastroenterol Motil. 2017; 23(2): 208–17.
Padwale V, Kirnake V, Daswani R, Kodmalwar A, Gupta A. A Comprehensive Review on the Efficacy and Safety of Vonoprazan in the Management of Gastric Acid-Related Diseases. Cureus. 2024; 16(7): e64777.
Tian L, Xiang D, Yue F, Li R, Zhou Y. Efficacy and safety of vonoprazan versus proton pump inhibitors in the treatment of peptic ulcer disease: a systematic review and network meta-analysis for randomized controlled trails. Front Nutr. 2024; 11: 1436993.
Chandrasekhar TS, Puri R, Dhawan P, Abraham P, Appasani S, Pratap N, et al. Perception mapping of vonoprazan: expert consensus on its efficacy and clinical utility in acid-related disorders in India. Gut. 2025; 74(Suppl 1): P130.
[14]
Silva GA, Figueiredo JS, Gonçalves RJ, Barbosa MG, Chehter EZ. Vonoprazan: A systematic review of an alternative to proton pump inhibitors. GHOA. 2022; 13(6): 221–31.
Laine L, Spechler S, Yadlapati R, Schnoll-Sussman F, Smith N, Leifke E, et al. Vonoprazan is Efficacious for Treatment of Heartburn in Non-erosive Reflux Disease: A Randomized Trial. Clin Gastroenterol Hepatol. 2024; 22(11): 2211-2220.e10.
Hoshikawa Y, Kawami N, Hoshino S, Tanabe T, Umezawa M, Kaise M, et al. Efficacy of on-demand therapy using 20-mg vonoprazan for non-erosive reflux disease. Esophagus. 2019; 16(2): 201–6.
Simadibrata DM, Lesmana E, Fass R. A systematic review and meta-analysis of the efficacy of vonoprazan for proton pump inhibitor-resistant gastroesophageal reflux disease. J Gastroenterol Hepatol. 2024; 39(5): 796–805.
Niikura R, Yamada A, Hirata Y, Hayakawa Y, Takahashi A, Shinozaki T, et al. Efficacy of Vonoprazan for Gastroesophageal Reflux Symptoms in Patients with Proton Pump Inhibitor-resistant Non-erosive Reflux Disease. Intern Med. 2018; 57(17): 2443–50.
Kawai T, Suzuki C, Honda Y, Fernandez JL. Long-term safety and effectiveness of vonoprazan for prevention of gastric and duodenal ulcer recurrence in patients on nonsteroidal anti-inflammatory drugs in Japan: a 12-month post-marketing surveillance study. Expert Opin Drug Saf. 2023; 22(5): 425–31.
Mizokami Y, Oda K, Funao N, Nishimura A, Soen S, Kawai T, et al. Vonoprazan prevents ulcer recurrence during long-term NSAID therapy: randomised, lansoprazole-controlled non-inferiority and single-blind extension study. Gut. 2018; 67(6): 1042–51.
Suresh, M., Manjunath, K. K. (2026). Expert Perspectives on Acid Peptic Disease Management and the Role of Vonoprazan in Indian Settings. International Journal of Gastroenterology, 10(1), 59-66. https://doi.org/10.11648/j.ijg.20261001.20
Suresh, M.; Manjunath, K. K. Expert Perspectives on Acid Peptic Disease Management and the Role of Vonoprazan in Indian Settings. Int. J. Gastroenterol.2026, 10(1), 59-66. doi: 10.11648/j.ijg.20261001.20
Suresh M, Manjunath KK. Expert Perspectives on Acid Peptic Disease Management and the Role of Vonoprazan in Indian Settings. Int J Gastroenterol. 2026;10(1):59-66. doi: 10.11648/j.ijg.20261001.20
@article{10.11648/j.ijg.20261001.20,
author = {Manjula Suresh and Krishna Kumar Manjunath},
title = {Expert Perspectives on Acid Peptic Disease Management and the Role of Vonoprazan in Indian Settings},
journal = {International Journal of Gastroenterology},
volume = {10},
number = {1},
pages = {59-66},
doi = {10.11648/j.ijg.20261001.20},
url = {https://doi.org/10.11648/j.ijg.20261001.20},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijg.20261001.20},
abstract = {Background: Although there are several clinical studies available regarding the management of acid peptic disorders (APD), there is a dearth of studies among clinical experts on their practice. This study aimed to assess clinicians’ perspectives on the management of APD, with particular emphasis on the emerging role of vonoprazan in routine clinical practice in Indian settings. Methodology: This cross-sectional study included 209 clinical experts across India. A validated 22-item questionnaire assessed key aspects of APD management, including epidemiology, diagnostics, treatment practices, challenges related to proton pump inhibitor (PPI) therapy, and perceptions of vonoprazan. Data were analyzed using descriptive statistics. Results: In routine clinical practice, approximately 51% of clinicians reported that about 11–25% of their patients with gastroesophageal reflux disease (GERD) do not respond adequately to PPI therapy, while 49% indicated that nocturnal acid breakthrough is commonly encountered during PPI use. Nearly 63% of respondents emphasized vonoprazan’s unique mechanism of action as its key advantage over PPIs, enabling faster and more prolonged binding to the H⁺/K⁺-ATPase enzyme and providing sustained 24-hour acid suppression. Approximately 42% of clinicians preferred vonoprazan for GERD, while 41.63% favored its use in 11–25% of patients with nonerosive reflux disease, and 38.76% preferred its use across all age groups in PPI-resistant cases. In the setting of NSAID-induced ulcer recurrence, around 55% of respondents reported using vonoprazan in selected cases. Overall, 73% perceived multiple benefits of vonoprazan, including the absence of a requirement for metabolic activation, more rapid intragastric pH elevation, and acid stability with reversible inhibition, allowing meal-independent dosing. Conclusion: This survey highlights important limitations of PPI therapy and strong clinician recognition of vonoprazan’s pharmacological and clinical advantages. The findings suggest strategic use of vonoprazan in patients with an inadequate response to PPIs, particularly in GERD and PPI-resistant cases, positioning it as a valuable therapeutic option for addressing unmet needs in the management of acid-related disorders.},
year = {2026}
}
TY - JOUR
T1 - Expert Perspectives on Acid Peptic Disease Management and the Role of Vonoprazan in Indian Settings
AU - Manjula Suresh
AU - Krishna Kumar Manjunath
Y1 - 2026/06/29
PY - 2026
N1 - https://doi.org/10.11648/j.ijg.20261001.20
DO - 10.11648/j.ijg.20261001.20
T2 - International Journal of Gastroenterology
JF - International Journal of Gastroenterology
JO - International Journal of Gastroenterology
SP - 59
EP - 66
PB - Science Publishing Group
SN - 2640-169X
UR - https://doi.org/10.11648/j.ijg.20261001.20
AB - Background: Although there are several clinical studies available regarding the management of acid peptic disorders (APD), there is a dearth of studies among clinical experts on their practice. This study aimed to assess clinicians’ perspectives on the management of APD, with particular emphasis on the emerging role of vonoprazan in routine clinical practice in Indian settings. Methodology: This cross-sectional study included 209 clinical experts across India. A validated 22-item questionnaire assessed key aspects of APD management, including epidemiology, diagnostics, treatment practices, challenges related to proton pump inhibitor (PPI) therapy, and perceptions of vonoprazan. Data were analyzed using descriptive statistics. Results: In routine clinical practice, approximately 51% of clinicians reported that about 11–25% of their patients with gastroesophageal reflux disease (GERD) do not respond adequately to PPI therapy, while 49% indicated that nocturnal acid breakthrough is commonly encountered during PPI use. Nearly 63% of respondents emphasized vonoprazan’s unique mechanism of action as its key advantage over PPIs, enabling faster and more prolonged binding to the H⁺/K⁺-ATPase enzyme and providing sustained 24-hour acid suppression. Approximately 42% of clinicians preferred vonoprazan for GERD, while 41.63% favored its use in 11–25% of patients with nonerosive reflux disease, and 38.76% preferred its use across all age groups in PPI-resistant cases. In the setting of NSAID-induced ulcer recurrence, around 55% of respondents reported using vonoprazan in selected cases. Overall, 73% perceived multiple benefits of vonoprazan, including the absence of a requirement for metabolic activation, more rapid intragastric pH elevation, and acid stability with reversible inhibition, allowing meal-independent dosing. Conclusion: This survey highlights important limitations of PPI therapy and strong clinician recognition of vonoprazan’s pharmacological and clinical advantages. The findings suggest strategic use of vonoprazan in patients with an inadequate response to PPIs, particularly in GERD and PPI-resistant cases, positioning it as a valuable therapeutic option for addressing unmet needs in the management of acid-related disorders.
VL - 10
IS - 1
ER -
Suresh, M., Manjunath, K. K. (2026). Expert Perspectives on Acid Peptic Disease Management and the Role of Vonoprazan in Indian Settings. International Journal of Gastroenterology, 10(1), 59-66. https://doi.org/10.11648/j.ijg.20261001.20
Suresh, M.; Manjunath, K. K. Expert Perspectives on Acid Peptic Disease Management and the Role of Vonoprazan in Indian Settings. Int. J. Gastroenterol.2026, 10(1), 59-66. doi: 10.11648/j.ijg.20261001.20
Suresh M, Manjunath KK. Expert Perspectives on Acid Peptic Disease Management and the Role of Vonoprazan in Indian Settings. Int J Gastroenterol. 2026;10(1):59-66. doi: 10.11648/j.ijg.20261001.20
@article{10.11648/j.ijg.20261001.20,
author = {Manjula Suresh and Krishna Kumar Manjunath},
title = {Expert Perspectives on Acid Peptic Disease Management and the Role of Vonoprazan in Indian Settings},
journal = {International Journal of Gastroenterology},
volume = {10},
number = {1},
pages = {59-66},
doi = {10.11648/j.ijg.20261001.20},
url = {https://doi.org/10.11648/j.ijg.20261001.20},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijg.20261001.20},
abstract = {Background: Although there are several clinical studies available regarding the management of acid peptic disorders (APD), there is a dearth of studies among clinical experts on their practice. This study aimed to assess clinicians’ perspectives on the management of APD, with particular emphasis on the emerging role of vonoprazan in routine clinical practice in Indian settings. Methodology: This cross-sectional study included 209 clinical experts across India. A validated 22-item questionnaire assessed key aspects of APD management, including epidemiology, diagnostics, treatment practices, challenges related to proton pump inhibitor (PPI) therapy, and perceptions of vonoprazan. Data were analyzed using descriptive statistics. Results: In routine clinical practice, approximately 51% of clinicians reported that about 11–25% of their patients with gastroesophageal reflux disease (GERD) do not respond adequately to PPI therapy, while 49% indicated that nocturnal acid breakthrough is commonly encountered during PPI use. Nearly 63% of respondents emphasized vonoprazan’s unique mechanism of action as its key advantage over PPIs, enabling faster and more prolonged binding to the H⁺/K⁺-ATPase enzyme and providing sustained 24-hour acid suppression. Approximately 42% of clinicians preferred vonoprazan for GERD, while 41.63% favored its use in 11–25% of patients with nonerosive reflux disease, and 38.76% preferred its use across all age groups in PPI-resistant cases. In the setting of NSAID-induced ulcer recurrence, around 55% of respondents reported using vonoprazan in selected cases. Overall, 73% perceived multiple benefits of vonoprazan, including the absence of a requirement for metabolic activation, more rapid intragastric pH elevation, and acid stability with reversible inhibition, allowing meal-independent dosing. Conclusion: This survey highlights important limitations of PPI therapy and strong clinician recognition of vonoprazan’s pharmacological and clinical advantages. The findings suggest strategic use of vonoprazan in patients with an inadequate response to PPIs, particularly in GERD and PPI-resistant cases, positioning it as a valuable therapeutic option for addressing unmet needs in the management of acid-related disorders.},
year = {2026}
}
TY - JOUR
T1 - Expert Perspectives on Acid Peptic Disease Management and the Role of Vonoprazan in Indian Settings
AU - Manjula Suresh
AU - Krishna Kumar Manjunath
Y1 - 2026/06/29
PY - 2026
N1 - https://doi.org/10.11648/j.ijg.20261001.20
DO - 10.11648/j.ijg.20261001.20
T2 - International Journal of Gastroenterology
JF - International Journal of Gastroenterology
JO - International Journal of Gastroenterology
SP - 59
EP - 66
PB - Science Publishing Group
SN - 2640-169X
UR - https://doi.org/10.11648/j.ijg.20261001.20
AB - Background: Although there are several clinical studies available regarding the management of acid peptic disorders (APD), there is a dearth of studies among clinical experts on their practice. This study aimed to assess clinicians’ perspectives on the management of APD, with particular emphasis on the emerging role of vonoprazan in routine clinical practice in Indian settings. Methodology: This cross-sectional study included 209 clinical experts across India. A validated 22-item questionnaire assessed key aspects of APD management, including epidemiology, diagnostics, treatment practices, challenges related to proton pump inhibitor (PPI) therapy, and perceptions of vonoprazan. Data were analyzed using descriptive statistics. Results: In routine clinical practice, approximately 51% of clinicians reported that about 11–25% of their patients with gastroesophageal reflux disease (GERD) do not respond adequately to PPI therapy, while 49% indicated that nocturnal acid breakthrough is commonly encountered during PPI use. Nearly 63% of respondents emphasized vonoprazan’s unique mechanism of action as its key advantage over PPIs, enabling faster and more prolonged binding to the H⁺/K⁺-ATPase enzyme and providing sustained 24-hour acid suppression. Approximately 42% of clinicians preferred vonoprazan for GERD, while 41.63% favored its use in 11–25% of patients with nonerosive reflux disease, and 38.76% preferred its use across all age groups in PPI-resistant cases. In the setting of NSAID-induced ulcer recurrence, around 55% of respondents reported using vonoprazan in selected cases. Overall, 73% perceived multiple benefits of vonoprazan, including the absence of a requirement for metabolic activation, more rapid intragastric pH elevation, and acid stability with reversible inhibition, allowing meal-independent dosing. Conclusion: This survey highlights important limitations of PPI therapy and strong clinician recognition of vonoprazan’s pharmacological and clinical advantages. The findings suggest strategic use of vonoprazan in patients with an inadequate response to PPIs, particularly in GERD and PPI-resistant cases, positioning it as a valuable therapeutic option for addressing unmet needs in the management of acid-related disorders.
VL - 10
IS - 1
ER -