1. Introduction
1.1. Background
Nepal is a country which use to believe in traditional ayurvedic practices which has undergone remarkable transformation over the centuries to a complex modernized health care facility. These services are heavily influenced by politics, socio economic condition and global health impacts
| [3] | Benatar, S. (2016). Politics, power, poverty and global health: systems and frames. International journal of health policy and management, 5(10), 599. |
[3]
. The first known hospital of Nepal was established in 1890 during the rana regime and was named as Bir hospital
| [1] | Acharya, S. P. (2014). Critical care medicine: an emerging super specialty in Nepal. Journal of Society of Anesthesiologists of Nepal, 1(2), 55-58. |
[1]
. Following this history, Nepal has gone significant changes in the improvement of the health sectors. Nepal government has implemented several national health policies, several years plans, targeted programs to address maternal and child health care, communicable diseases, and the expansion of health care services all over the country as a basic need to access the primary healthcare
| [38] | Rokaya, R. B. (2024). Priorities of Health Issues in Periodic Plans of Nepal. Janaprakash Journal of Multidisciplinary Research, 2, 142-155. |
[38]
. Even though, the health service in Nepal is provided by both government and private sectors, they are failing to provide the essential services and quality as per the international standards. It has been found that the prevalence of the diseases in Nepal is higher than other south Asian countries and has very low prognosis
| [17] | Hasan, M., Sutradhar, I., Gupta, R. D., & Sarker, M. (2018). Prevalence of chronic kidney disease in South Asia: a systematic review. BMC nephrology, 19(1), 291. |
[17]
. However, some notable changes can be seen especially in the field of maternal health. One of the most notable achievement is the human development index has increased to 0.602 in 2019 from 0.291 in 1975
| [8] | Doss, C., Meinzen-Dick, R., Pereira, A., & Pradhan, R. (2020). Women’s Empowerment, Extended Families and Male Migration in Nepal. FPRI Discussion Paper, 1977, 41. |
[8]
. Similarly, the child mortality has decreased by 78% from year 1990 to 2017. Life expectancy of Nepali citizen rose to 71.5 years in 2018 from 66 years in 2005
| [36] | Rai, T. R. (2017). A status analysis of nepal's graduation to developing countries. |
[36]
. Health care expenditure from the government is also increasing each year. In 2021, 7.45% of the total budget was allocated for healthcare. In 2002, Nepal government has allocated USD 2.30 for each citizen which gradually increased to USD 137 in 2012 AD
| [35] | Poyck, M. C., Koirala, D. B. N., Aryal, D. P. N., & Sharma, N. K. (2016). Joint Evaluation of Nepal’s School Sector Reform Plan Programmer 2009-16. |
[35]
.
According to the official list, there are 125 governmental hospitals established till 2019. However, these hospitals still fail to maintain the service, facility, nutrition and quality as per the international health standards. Especially in the rural area, there are very limited reproductive healthcare facility for women and also for the marginalized community
| [33] | Pokhrel, R., Knoble, A., Gautam, P., Shah, M. K., Paudel, P., Amatya, A., & Rajbhandari, R. (2025). Minimum service standards assessment tool and the hospital strengthening program: a novel first step towards the quality improvement of Nepal’s national hospital system. The Lancet Regional Health-Southeast Asia, 34. |
[33]
. A huge number of efforts has been made by different national and international organizations to solve the issues of healthcare in the rural areas of Nepal
| [9] | Dumka, N., Gurung, A., Hannah, E., Goel, S., & Kotwal, A. (2024). Understanding key factors for strengthening Nepal’s healthcare needs: health systems perspectives. Journal of Global Health Reports, 8, e2024010. |
[9]
. The major objectives of these organizations are to educate about family planning, communication, safe motherhood practice, skilled birth attendance etc. Similarly, a major factor that contributes towards the health hazards which is nutrition deficiency are wide spread in rural areas with almost half of the women and children malnourished during the pregnancy and post pregnancy period
| [6] | Dangal, G., & Shah, M. K. (2022). Minimum Service Standard: A Hospital Strengthening Program that Facilitates Hospitals’ Attainment of Quality-of-Care Standards. |
[6]
. Nepal has gone significant changes in health care governments after the 2015 constitution where Nepal moved to federal government system with three level of government, a federal level, 7 provinces and 753 local government
| [7] | Devkota, K. L., & Khanal, G. K. (2024, February). Nepal. In The Forum of Federations Handbook on Local Government in Federal Systems (pp. 347-376). Cham: Springer International Publishing. |
[7]
. Health service provided by the ministry of health and population, province and the municipalities are financed by taxes
| [40] | Thapa, R., Bam, K., Tiwari, P., Sinha, T. K., & Dahal, S. (2018). Implementing federalism in the health system of Nepal: opportunities and challenges. International journal of health policy and management, 8(4), 195. |
[40]
. However, external fundings and budget cut from publics also plays role in financing these health service providers. The journey reflects Nepal's socio-political evolution while highlighting both progress and areas requiring sustained attention to achieve universal health coverage. To ensure the highest level of methodological rigor and transparency in this analysis, this study adheres to the PRISMA-P (Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols) and JBI (Joanna Briggs Institute) guidelines. Utilizing the PRISMA-P framework allows for a standardized, pre-defined approach that minimizes bias in study selection and data extraction, while JBI guidelines provided a comprehensive methodology specifically designed for evidence synthesis in complex health systems. These frameworks were essential for this study to accurately map the heterogeneous data spanning Nepal’s transition from traditional practices to a federalized healthcare system, ensuring that the findings are both reproducible and align with international academic standards.
Therefore, to critically assess the major changes and continuities in the health policies, program and projects and to identify key achievements and remaining gaps in the health sector and highlight the how past and present interventions have contributed to improving health outcomes and where improvements are still needed, the following review was conducted.
1.2. Problem Statement
The government and several national and international organizations had made significant effort and several health programs to provide easy access to the citizens all across Nepal. However, the peoples from the rural area and marginalized communities continue to face sever challenges in getting timed health care and quality services
| [24] | Marahatta, S. B., Yadav, R. K., Giri, D., Lama, S., Rijal, K. R., Mishra, S. R.,... & Adhikari, B. (2020). Barriers in the access, diagnosis and treatment completion for tuberculosis patients in central and western Nepal: A qualitative study among patients, community members and health care workers. PloS one, 15(1), e0227293. |
[24]
. Moreover, the rules and regulations, plans and policy often suffers from poor condition, lack of proper coordination, resources, unclear objectives and roles of the federal, provincial and local governments. These challenges in the rural area often intervene with the assessment of health care service, very high expenditure due to uneven road ways, very few skilled health care professionals, inadequate infrastructures such as lack of equipment’s, electricity, sterile water at health posts and cultural or religious barriers. The long-term goal and the outcomes are significantly impacted by the current situation of the country
| [39] | Simkhada, B., van Teijlingen, E., Porter, M., & Simkhada, P. (2006). Major problems and key issues in Maternal Health in Nepal. Kathmandu University medical journal, 4(2 (Iss), 258-263. |
[39]
. The developmental history of the medical service is also unclear which is required to critically evaluate the evolution of the health policies and programs in Nepal. The new changes due the the federalization of Nepal have brought new complexities in the health system, with several changes in responsibilities for health service providers. This new fragmentation of development region into federal, provincial and local levels has led to destruction of efforts, unclear objectives, competition for resources and significantly reduce the efficiency of the health care system. Understanding the development of health policies and programs over time requires through knowledge of their historical roots, including the influence of international aid, political transitions, and societal changes on the health sector's development
1.3. Objectives of the Review
The objectives of this review are,
1) To trace the historical development of health services in Nepal,
2) To critically assess the major changes and continuities in health policies, programs, and projects
3) To identify key achievements and remaining gaps in the health sector.
4) To highlight how past and present interventions have contributed to improving health outcomes and where improvements are still needed.
1.4. Rationale of the Study
Understanding the history and the evolution of the health care facility of Nepal is extremely important for effectively implementing and sustainable health care plans and policies. A surface study throughout the history and evolution can help to identify which strategy has worked, which has failed and why this strategy has failed to worked. These knowledge’s can be useful to reform or revise the existing policy regarding the health care which requires a significant attention. By understanding the outcome of this review, the policy makers and health presentational can make quality decisions that can effectively address the current challenges
| [16] | Gurung, G., Derrett, S., Gauld, R., & Hill, P. C. (2017). Why service users do not complain or have ‘voice’: a mixed-methods study from Nepal’s rural primary health care system. BMC health services research, 17(1), 81. |
[16]
. This review also contributes to the broader discourse on health system strengthening in low and middle-income countries undergoing political and administrative transitions.
1.5. Conceptual Framework
The conceptual framework for this review is based on the understanding that the development of Nepal health services is shaped and structured by the historical legacies, political governance and social and economic conditions, international influences and community driven factors. These determinants interact to produce both achievements and persistent gaps in health outcomes. Key inputs include financing, governance, health workforce, infrastructure, and community-level programs such as the Female Community Health Volunteers (FCHVs). These inputs shape processes like health service delivery, decentralization by federal governance and regulation of health policies. The outcomes are reflected in measurable indicators such as maternal and child health improvements, increased life expectancy, and progress toward the Sustainable Development Goals (SDGs). However, systemic problems such as unequal resource distribution, financial instability, and dependence on external fundings limit the utilization of inputs into equitable and high-quality outcomes. By situating Nepal’s experience within the broader regional and international context, the framework emphasizes both the enabling role of community-based initiatives and the structural challenges that impede universal health coverage.
Ultimately, the framework highlights that Nepal’s health outcomes are not the product of isolated policies but of the intersection between governance, financing, socio-cultural realities, and global influences. Strengthening each dimension in a coordinated way is essential for achieving sustainable, equitable, and high-quality health care.
2. Methodology
This protocol follows the publishing guidelines set forth by the PRISMA-P checklist and the JBI methodology for systematic reviews on prevalence
| [28] | Moher, D., Shamseer, L., Clarke, M., Ghersi, D., Liberati, A., Petticrew, M.,... & Prisma-P Group. (2015). Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Systematic reviews, 4(1), 1. |
[28]
. This review aimed to highlight how past and present interventions have contributed to improving health outcomes and where improvements are still needed.
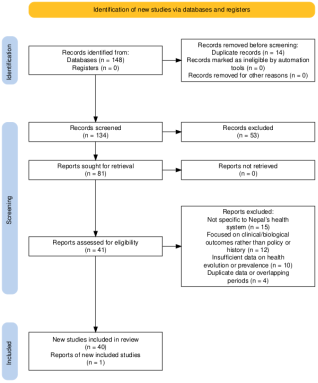
Figure 1. Protocol for systematic review.
2.1. Search Strategy
To achieve this, comprehensive search was conducted across various electronic databases. The articles for this study were searched in different electronic databases (Google Scholar) using the keywords “Nepal”, “Health service”, “History” and “Medicine”. All the articles related to this field were included in this review, regardless of publication year, Journals and Authors.
2.2. Study Selection
Using the PCC (Population, Concept, Context) framework, we included peer-reviewed articles, policy papers, and reports related to Nepal’s health system evolution published in English. We excluded opinion pieces, editorials, and non-scientific blogs. As illustrated in the PRISMA Flow Diagram, total of 148 records were identified through database searches. After removing duplicates, 134 records remained. Following title and abstract screening, 81 records were retained. After assessing full-texts and excluding ineligible articles, 40 studies were finally included in the review.
Inclusion: peer-reviewed articles, policy papers, reports must be related to Nepal’s health system, published in English.
Exclusion: opinion pieces, editorials, non-scientific blogs.
2.3. Data Extraction & Quality Appraisal
After the relevant articles were identified, the full text for these articles were collected in Mendeley and was reviewed. That information is which were relevant to the history of health service and medicine in Nepal were selected and extracted. Additionally, articles with key events, policy changes, development of medical institutions, prevalent diseases, traditional healing methods and the evolution of the health care delivery systems. The collected information’s were then qualitatively synthesized to identify major trends, themes, events and knowledge gaps in the existing literatures. A narrative approach was used for this review to present the findings, summarizing and interpreting the collected information to provide a well-structured historical information.
3. Historical Foundations of Nepal's Health System
3.1. Ancient and Medieval Periods (1st Century - 1768 AD)
During the ancient periods, Nepal first introduces the use of ayurvedic medicines which came in around the period of Lichchhavi dynasty. It was between the period of first to 879 AD. It was known that the king Amshu Verma introduce the ayurvedic medicines to the public. It was first made publicly available in between 605 to 620 AD which was considered as the ground breaking measures in the public health sector. Several of the medicinal herbs were used for treating minor wounds which originate during the war
| [19] | Kharel, L. P. (2023). Role of king in ancient & medieval culture and society of Nepal (Doctoral dissertation, Department of Nepalese History, Culture and Archaeology). |
[19]
. The former king established the Aarohyashalas which translates to health facilities around the Kathmandu valley. The major impactful move was to immediately cut umbilical cord after birth rather than waiting for placenta delivery. Similarly, several protocals for emergency care for women reproductive health, child birth and post mortem cesarean sections were developed by the local health associates. While these accounts highlight the sophisticated early development of public health protocols in Nepal, they originate from historical analyses and secondary sources
| [19] | Kharel, L. P. (2023). Role of king in ancient & medieval culture and society of Nepal (Doctoral dissertation, Department of Nepalese History, Culture and Archaeology). |
[19]
. The JBI appraisal of such literature typically notes challenges in verifying primary evidence from this era. Therefore, these points are best interpreted as illustrating the documented historical narrative of Nepal's medical tradition, rather than as empirically verifiable facts. This underscores the importance of critical source appraisal in historical synthesis.
After the end of the Lichchhavi dynasty, Malla period started. Several improvements were achieved during this period in heath service
| [27] | Mishra, S. R., Ghimire, K., Khanal, V., Aryal, D., Shrestha, B., Khanal, P. & Adhikari, B. (2025). Transforming health in Nepal: a historical and contemporary review on disease burden, health system challenges, and innovations. Health Research Policy and Systems, 23(1), 61. |
[27]
. The Malla period was in around 880 to 1768 AD which was significantly longer than the previous periods. Jayasthiti Malla, a king at that time established a strict rule where there should be no caste-based discrimination during the child birth. Any one was allowed for traditional birth attendance regardless of caste and culture. Similarly, King Pratap Malla established a Ayurvedic dispensary which was completely funded by the state. This dispensary was maintained by the experienced technician from the state and was located at the Hanuman Dhoka palace in 17
th century
| [22] | Lewis, T., & Bajracharya, N. M. (2016). Vajrayāna traditions in Nepal. Tantric Traditions in Transmission and Translation, 87-198. |
[22]
. During this time, several international organizations has begun to provide help to improve health service in Nepal. Christian missionaries introduced allopathic medicines in 1661, whose sole purpose was to provide quality allopathic medicines to the wounded patients. They were successful in establishing new clinics in Kathmandu, Lalitpur and Bhaktapur area. However, unstable kingdom and public pressure led to expel of these services in 1768. The following year, the Malla period ended and new period begun. The description of progressive, equity-focused policies under Malla rulers is compelling, yet it is derived from historical analyses
| [22] | Lewis, T., & Bajracharya, N. M. (2016). Vajrayāna traditions in Nepal. Tantric Traditions in Transmission and Translation, 87-198. |
| [27] | Mishra, S. R., Ghimire, K., Khanal, V., Aryal, D., Shrestha, B., Khanal, P. & Adhikari, B. (2025). Transforming health in Nepal: a historical and contemporary review on disease burden, health system challenges, and innovations. Health Research Policy and Systems, 23(1), 61. |
[22, 27]
that may reflect idealized state records. The claim of non-discriminatory birth attendance, in particular, represents a significant social policy for its time. A critical appraisal using JBI principles would question the extent of its implementation beyond royal decrees and within the complex social fabric of the era. The narrative of missionary expulsion also simplifies a likely multifaceted socio-political conflict, reminding us that historical syntheses must navigate the distinction between documented events and their underlying causes.
Rana period started in 1769 and ended in 1951. During these 104 years of Rana regime, several notable improvements has been made. This period is known for establishing the key foundation of modern healthcare service in Nepal
| [14] | Ghimire, T. N., & Phuyel, S. P. (2022). Tradition, political and legal systems of Nepal. HISAN: Journal of History Association of Nepal, 8(1), 79-87. |
[14]
. Due to the improvement of healthcare service in the world, Nepal also adopted some of the modern techniques to improve the healthcare services. It was the first regime to implement systematic development of modern medical infrastructures
| [13] | Ghimire, D. K. (2024). Economic and Social Development under Rana Regimes in Nepal: A Historical Analysis. Patan Pragya, 13(1), 11-21. |
[13]
. In 1850, vaccination of small pox was first introduced which is the first step for first modern medical intervention. In 1857, the first state health institution was established and was named as Khokana Leprosy Asylum
| [25] | Marasini, B. R. (2003). Health and hospital development in Nepal: past and present. Journal of Nepal Medical Association, 42(149), 306-11. |
[25]
. In 1889, king Bir Shamsher founded a hospital which was named as Prithvi Bir Hospital. This hospital had 15 beds with emergency facility and satellite dispensaries available. Later on, the hospital was named as Bir hospital and is functional till date
| [4] | Bhattarai, A. (2023). Modernization Efforts Undertaken by the Nepali Army. The Journal of Knowledge and Innovation, 9(1), 38-47. |
[4]
. In early 1900, Chandra Shamsher expanded health services to 35 districts, with hospitals and special facilities for tuberculosis, cholera, leprosy and emergency services. In 1925, Tri Chandra Military Hospital was established with an aim to implement western style medical education which became very successful till date
| [30] | Nepal, R. M. (2025). Light in the Dark: Thick and Thin Development during the Rana Period in Nepal. International Journal of Social Sciences and Management, 12(1), 9-17. |
[30]
. Not only there were major revolution in modern medicine but also there was significant shifts in the policy as well. Some of the notable policy shifts were, transition from purely Ayurvedic to dual system, Ayruvedic and allopathic system, introduction of land tax (Birta/Guthi) to fund healthcare services and early specialization with separate male and female hospitals for diseases specific facilities.
While the Rana period undeniably institutionalized modern biomedical infrastructure in Nepal, a critical reading of these developments
| [4] | Bhattarai, A. (2023). Modernization Efforts Undertaken by the Nepali Army. The Journal of Knowledge and Innovation, 9(1), 38-47. |
| [14] | Ghimire, T. N., & Phuyel, S. P. (2022). Tradition, political and legal systems of Nepal. HISAN: Journal of History Association of Nepal, 8(1), 79-87. |
| [25] | Marasini, B. R. (2003). Health and hospital development in Nepal: past and present. Journal of Nepal Medical Association, 42(149), 306-11. |
| [30] | Nepal, R. M. (2025). Light in the Dark: Thick and Thin Development during the Rana Period in Nepal. International Journal of Social Sciences and Management, 12(1), 9-17. |
[4, 14, 25, 30]
must consider their primary beneficiaries. The establishment of hospitals like Bir and Tri Chandra, while foundational, was largely concentrated in the Kathmandu Valley and aimed primarily at serving the Rana elite, military, and the urban populace. The expansion to 35 districts under Chandra Shamsher represents a significant scaling of state health apparatus, yet the extent to which these services were accessible to the rural poor remains a critical question. This synthesis highlights a pattern where the foundations of a modern system were laid, but its equitable implementation was a challenge deferred to future eras.
3.2. Post-Democracy Health System Expansion (1951-1990)
From 1950, autocracy ended and the period of democracy started which led to the exponential growth in health service, quality care, infrastructures and programs. In 1954, the international organization called as United Mission to Nepal established the Tansen Mission Hospital which current has 200 beds and is mostly functional for acute services located in palpa district. In 1956, a national project for the eradication of Malaria in all over Nepal was launched with aim to prevent high morbidity of malaria
| [11] | Gautam, U. (2019). Aid Effectiveness in Nepal: A Case of Malaria Program. |
[11]
. In 1958, a policy to establish one health center for each 105 electoral constituencies. In 1972, institute of Medicine established the beginning of domestic medical education in Nepal
| [18] | Khanal, D. P. (2017). History of pharmaceutical development in Nepal. Journal of Manmohan Memorial Institute of Health Sciences, 3(1), 86-93. |
[18]
. In 1978, the primary healthcare system was adopted for the strategy to improve health. Some of the programs launched during this period were, vertical disease control programs for small pox in 1962, leprosy in 1963 and family planning in 1962. In 1988, female community health volunteer program and mothers’ group was launched
| [34] | Pokhrel, S., & Sauerborn, R. (2004). Household decision-making on child health care in developing countries: the case of Nepal. Health policy and planning, 19(4), 218-233. |
[34]
. Following this year, expansion of immunization programs of smallpox was launched to eradicate it. The narrative of exponential, post-autocracy growth captures a period of ambitious institution-building. However, a critical synthesis must examine the inherent tensions within this expansion. The co-existence of a domestic medical education system
| [18] | Khanal, D. P. (2017). History of pharmaceutical development in Nepal. Journal of Manmohan Memorial Institute of Health Sciences, 3(1), 86-93. |
[18]
with heavy reliance on international missions, and the parallel launch of comprehensive primary healthcare (PHC) with numerous vertical disease programs, reveals a fragmented strategic vision. While the Female Community Health Volunteer (FCHV) program
| [34] | Pokhrel, S., & Sauerborn, R. (2004). Household decision-making on child health care in developing countries: the case of Nepal. Health policy and planning, 19(4), 218-233. |
[34]
became a cornerstone of community-based care, its creation also highlights the state's reliance on an unpaid (and later minimally compensated) female workforce to achieve national health goals a model with significant equity and sustainability implications that would be scrutinized in a contemporary policy appraisal.
3.3. Health System Reforms in the Federal Era (1990-Present)
After the year of 1990, there was major policy shifts and health system restructuring. The major policy framework evolution is, in 1991, first national health policy was established with major emphasizing in PHC expansion to all the four thousand village development communities. In 1993, decentralization began with health management favoring the municipalities. In 2015, sub health posts were upgraded to health posts as a part of federalization
| [5] | Chettry, L. K., Bohara, P., Bohara, R. C., Rijal, R., Khadha, S., Subedi, H. & Anderson, D. M. (2024). Budgeting and advocacy to improve water, sanitation, and hygiene in health care facilities: a case study in Nepal. Global Health: Science and Practice, 12(3). |
[5]
. Following the same year in 2016, health system restructuring was done under the federal government. Along with the policy changes, several key programmatic achievements were seen. In the maternal and child health program, the maternal mortality ratio was reduced by 55% from 1996 to 2016
| [21] | Lampard, R., Hogan, D. B., Stahnisch, F. W., & Wright Jr, J. R. (2021). Creating the Future of Health: The History of the Cumming School of Medicine at the University of Calgary, 1967-2012 (p. 420). University of Calgary Press. |
[21]
. Previously it was 539 live births per lakh which improved to 239 deaths. Similarly, the neonatal mortality rate was reduced to half from 40 to 20 per thousand live births from 1996 to 2016. Similarly, 94% antenatal care were covered and 93% neonatal tetanus protection was achieved by 2025. The diseases such as small pox and polio were successfully eradicated. The DOTS strategy was implemented for TB control. Due to the improvement in healthcare service, universal health coverage index improved from 48 in 2017 to 53 in 2019. Similarly, human development index rose from 0.395 in 1990 to 0.601 in 2019. In 2025, the use of modern technology was implemented which uses a mobile app called as Nagarik App for the expansion of health insurance and digital integration
| [29] | Najar, P. A. (2024). Adopting Global Health Insurance Models for Medical Tourists in India: Implications for Stakeholders in Digitalized Era. |
[29]
.
The post-1990 period illustrates a persistent theme in Nepal's health system evolution: the tension between progressive policy aspirations and complex ground-level realities. While the policy trajectory from the 1991 National Health Policy to federalization
| [5] | Chettry, L. K., Bohara, P., Bohara, R. C., Rijal, R., Khadha, S., Subedi, H. & Anderson, D. M. (2024). Budgeting and advocacy to improve water, sanitation, and hygiene in health care facilities: a case study in Nepal. Global Health: Science and Practice, 12(3). |
[5]
demonstrates a consistent rhetorical commitment to decentralization and Primary Health Care (PHC), the actual devolution of authority, resources, and management capacity has been uneven and fraught. The impressive gains in maternal and child health metrics
| [21] | Lampard, R., Hogan, D. B., Stahnisch, F. W., & Wright Jr, J. R. (2021). Creating the Future of Health: The History of the Cumming School of Medicine at the University of Calgary, 1967-2012 (p. 420). University of Calgary Press. |
[21]
are testament to successful vertical programming and donor investment. However, a critical synthesis must note that these national aggregates often mask severe sub-national disparities, particularly in mountainous and remote regions, revealing that the reach of the system expanded faster than its equitable depth. The introduction of digital tools like the Nagarik App
| [29] | Najar, P. A. (2024). Adopting Global Health Insurance Models for Medical Tourists in India: Implications for Stakeholders in Digitalized Era. |
[29]
represents a modern solution, but its success is contingent on the very infrastructure and literacy gaps that historical inequities have created.
3.4. Impact of Federalization on Health Care System
There was a major change in the country after 2015 where the country was divided into different level of tiers. The structural and governance changes include the Nepal health care system now runs under federal, provincial and local governments each with distinct responsibilities. The local government can make their own decisions and have full control over the primary health care services. Similarly, provincial government controls the secondary hospitals whereas, the federal government focus on policy making, standards and tertiary health cares. Due to this division, instead of ease, there was more of confusion in roles and responsibilities, leading to challenges in coordination and service gaps. Some of the local government has taken leap ahead on this new governmental system however, some local bodies in rural areas stills struggles due to the limited supply of infrastructures and finances.
The budget allocated for the health care significantly rose from 1.5% to 2.4% with government now contributing 64% of health expenditures. The impact on health care workforce is, hospitals can now recruit and train local workers according to their need and demands. However, due to the low number of health care workers in the rural areas, there are shortage of skilled manpower’s in rural areas as compared to the urban areas. The distribution of the hospitals with the local bodies has led to decrease of salaries from 24.3% to 13.8% which has a major impact on the daily lives of the citizens. Similarly, many hospitals at the local level lacks planning and efficient management of the finance. The federalization has improved the local responsiveness through efficient planning and management, but the lack of coordination between the government levels has disturbed the referral systems and created health service gaps. Many local health workers lack skills in management, procurement, and planning required for their new responsibilities. The gaps of skills, equipment’s and knowledge still persists among the specific region even though, federalization was aimed to reduce these disparities. This was seen during the covid pandemics where there were difficulties in running the minor health care but some of the local bodies adapted quickly.
The most important advantage of federalization in health care system is the emergences of strengths. Which means, there is greater community participation in health planning, there is greater potential for better resources planning and distribution, increased innovation from the local levels and increasing amount of allocated budget for each individual hospitals and health posts. However, some of the persistent challenges includes, complex division of roles between the federal, provisional and the local bodies. The weak monitoring and low-quality supply of equipment’s has made the health service access more complex. The most important drawbacks are the influence of politics in every decision making.
The synthesis of evidence on federalization reveals its fundamental paradox: it is simultaneously a reform designed to reduce inequity by empowering local bodies, and a process that risks exacerbating inequity due to varying local capacity. The documented confusion in roles and service gaps is not merely a teething problem but a structural feature of a rapid, top-down decentralization where responsibilities were devolved faster than the corresponding managerial, technical, and financial capabilities could be built at the sub-national level. The COVID-19 pandemic served as a critical stress test, exposing this fragility. Therefore, the ultimate success of federalization in health will be measured not by the initial increase in budget or community participation, but by the system's ability to institutionalize mechanisms such as equalization grants, standardized management training, and robust inter-governmental platforms that proactively bridge the growing capacity chasm between high- and low-performing local governments.
3.5. Evolution of Health Care System in Panchayat, Multiparty and Federal Republic Eras
The health care system of Nepal has gone several changes due to the political changes which is seen in three different eras. The first one is the panchayat era which is estimated to be started from 1960 and ended in 1990
| [14] | Ghimire, T. N., & Phuyel, S. P. (2022). Tradition, political and legal systems of Nepal. HISAN: Journal of History Association of Nepal, 8(1), 79-87. |
[14]
. This era is the long than other eras and had a significant impact in the health care system of Nepal. In this system, there was absolute monarchy, with no political party system. All the health services and access were entirely controlled by the central government which was located in the Kathmandu. There were village panchayats as well but had very limited access to the administrative department of health care system
| [10] | Gaenszle, M. (2021). History, Locality and Culture in East Nepal During much of Nepal's modern history, especially under the party-less Panchayat system (1961-1990), the diversity of ethnic and local. A Place in the World: New Local Historiographies in Africa and South Asia, 2, 331. |
[10]
.
After the end of monarchy, multiparty system started after 1990 till 2008
| [12] | Gellner, D. N. (2022). The last Hindu king: How Nepal desanctified its monarchy. In Sacred kingship in world history: Between immanence and transcendence (pp. 271-298). Columbia University Press. |
[12]
. This era made the change of monarch controlling the entire parliament and constitution to the democracy controlling the parliament. This led to political instability but the development of health policy was advancing forward. There was introduction of Nepal national health policy in 1991 which focus more on the public health of the rural areas. During this era, several health post and sub health post were created in village development committees and across the country. Also, there was greater involvement of private sector than before.
After the year 2008, monarchy completed ended and new system was introduced where the country was divided into three tiers, federal, provisional and local government in 2015. There are total of 753 local governments where significant health responsibilities were assigned to them. A synthesis of the 40 included reports highlights a common theme: the governance transition in 2015 created a coordination gap. Due to this division, instead of ease, there was more of confusion in roles and responsibilities, leading to challenges in coordination and service gaps
| [32] | Paudel, N. R., & Pahari, S. (2024). Open Government in Federal Nepal: Challenges, Constraints, and Opportunities. In Mapping Governance Innovations (pp. 188-209). Routledge India. |
[32]
. Some of the local government has taken leap ahead on this new governmental system however, some local bodies in rural areas stills struggles due to the limited supply of infrastructures and finances. Major initiatives during this era were, free universal health insurance program in 2012, complete revision of National health policy in 2014 and 2019 focusing on federal system, recommending primary health care and compulsory at least two years of governmental service for receiving governmental medical scholarships. As Nepal continues its federal health system development, learning from both past successes and limitations of previous systems will be important for future health system strengthening.
Table 1. Comparative Analysis of the Key indicators of each governing era of Nepal.
Indicator | Panchayat era | Multiparty era | Federal republic |
Governance | Highly centralize | Partial decentralization | Three tier federal system |
Health Expenditure (% GDP) | ~1.5% | ~2-3% | More than 4% |
Maternal Mortality | 850 per 100,000 | 539 per 100,000 | 186 per 100,000 |
Under-5 Mortality | 162 per 1000 | 61.5 per 1000 | 32.2 per 1000 |
Life Expectancy | ~50 years | ~66 years | 71.5 years |
Institutional Deliveries | Very low | 18% to 39% | 79% above |
Primary Focus | Disease treatment | Maternal and child health | Universal health standards |
Viewing these three eras through a critical historical lens reveals a tension between political rupture and systemic continuity. While the Panchayat, Multiparty, and Federal Republic periods are defined by distinct political contracts, the health system demonstrates a persistent, underlying struggle to balance central control with local needs. The Panchayat's centralized model
| [10] | Gaenszle, M. (2021). History, Locality and Culture in East Nepal During much of Nepal's modern history, especially under the party-less Panchayat system (1961-1990), the diversity of ethnic and local. A Place in the World: New Local Historiographies in Africa and South Asia, 2, 331. |
[10]
created a uniform but rigid skeleton. The Multiparty era expanded coverage but grafted new programs and private actors onto this skeleton without fundamentally reforming its core governance
| [12] | Gellner, D. N. (2022). The last Hindu king: How Nepal desanctified its monarchy. In Sacred kingship in world history: Between immanence and transcendence (pp. 271-298). Columbia University Press. |
[12]
. Federalization
| [32] | Paudel, N. R., & Pahari, S. (2024). Open Government in Federal Nepal: Challenges, Constraints, and Opportunities. In Mapping Governance Innovations (pp. 188-209). Routledge India. |
[32]
then attempted a radical dismantling of that central skeleton, but in doing so, it inherited and often magnified the pre-existing inequities in capacity and resources. Thus, the "coordination gap" of the federal era is not a new problem but the latest manifestation of Nepal's enduring challenge: administering an equitable health system across formidable geographic and social gradients through a governance structure that has oscillated between over-centralization and fragmented decentralization.
3.6. Assessment of Policy Changes and Challenges
Primary healthcare was of major focus at the year of 1978 which was controlled by National health policy and the current federal policies. Similarly, government has worked with different national organizations to establish Mothers grow ups through community participation which remain cornerstone strategies since 1988. Government has also invested in the immunization programs all across the country for major fatal diseases such as small pox and polio and go beyond these diseases
| [26] | Millard, C. (2005). sMan and Glud: Standard Tibetan Medicine and Ritual Medicine in a Bon Medical School and Clinic in Nepal. The Tibet Journal, 30(4/1), 3-30. |
[26]
. Major transformative policy shifts include the decentralization of the governmental controlled system into three tier federal structure from centralized Rana regime system. The financial structure for supporting the insurance based system was from the land taxes which changed to fully funded by government and other donor organizations. Similarly, first private medical service which includes medical colleges and hospitals was established from 1991.
Even though, several notable changes have been made, 80% of women in urban areas delivers under the supervision of skilled attendance but the percentage still remains worst in the remote areas of Nepal. This disparities between the urban and rural areas are still persistent and needs immediate attention of the appropriate authority
| [2] | Afsana, K. (2025). Global health and sustainable development: successes and challenges in maternal health in South Asian countries. In The Intersection of Global Health and Sustainable Development (pp. 11-33). Edward Elgar Publishing. |
[2]
. Nepal has a huge problem of brain drain where skilled personal leaves the country for better opportunities. Several areas including the health service lacks the skilled manpower such as nurse and proper training programs and reservation policies which is limiting the growth of these services. Similarly, in 2025 around 3 billion Nepalese rupees has been reduced for health care which might be a potential threat to maternal health care’s especially in rural areas
| [20] | Khatri, R. B., Khanal, P., Thakuri, D. S., Ghimire, P., & Jakovljevic, M. (2025). Navigating Nepal’s health financing system: A road to universal health coverage amid epidemiological and demographic transitions. PloS one, 20(5), e0324880. |
[20]
. Epidemiological studies shows that non communicable diseases account for 66% deaths in Nepal but systems remain oriented to infectious diseases only.
This synthesis reveals the emergence of a persistent "two-track" health system in Nepal. One track, forged through policies like PHC (1978) and community-based programs (1988), represents the public, primary care-oriented, and equity-seeking vision. The other track, accelerated by the entry of private medical colleges (1991) and shaped by donor priorities, leans towards a curative, urban-centric, and market-influenced model. The current challenges rural-urban disparities, brain drain, and a disease burden misaligned with system orientation
| [2] | Afsana, K. (2025). Global health and sustainable development: successes and challenges in maternal health in South Asian countries. In The Intersection of Global Health and Sustainable Development (pp. 11-33). Edward Elgar Publishing. |
| [20] | Khatri, R. B., Khanal, P., Thakuri, D. S., Ghimire, P., & Jakovljevic, M. (2025). Navigating Nepal’s health financing system: A road to universal health coverage amid epidemiological and demographic transitions. PloS one, 20(5), e0324880. |
| [26] | Millard, C. (2005). sMan and Glud: Standard Tibetan Medicine and Ritual Medicine in a Bon Medical School and Clinic in Nepal. The Tibet Journal, 30(4/1), 3-30. |
[2, 20, 26]
are not accidental failures but logical outcomes of these competing tracks operating without sufficient integration. The federal structure, intended to unify the system, may instead risk further entrenching this divide if local governments lack the capacity to manage this complexity. Therefore, the core policy challenge is no longer merely expanding access but consciously integrating these tracks to ensure that the benefits of private investment and global health agendas serve, rather than undermine, the foundational equity goals of the public PHC system.