Abstract
Background: The first 24 hours following delivery are referred to as the immediate postnatal phase. The first 24 hours following birth account for a significant fraction of mother and newborn fatalities. Regardless of the circumstances surrounding their delivery, providing prompt postnatal care lowers maternal and newborn mortality and morbidity. There was limited evidence on immediate postnatal maternal satisfaction among mothers who gave birth in public hospitals in South West Shoa. Therefore, this study was conducted using a mixed-methods approach to assess maternal satisfaction with immediate postnatal care and to explore underlying factors influencing their experiences. Objectives: To assess women`s satisfaction with immediate postnatal care and associated factors among mothers who gave birth at Public Hospital, in South West Shoa, Ethiopia, 2023. Methods: A facility-based, cross-sectional study design supplemented by a qualitative study / convergent study design/ was conducted among 403 mothers for the quantitative study and 17 women for the qualitative study. Purposive and systematic sampling methods technique was used to select study participants for the qualitative and quantitative study, respectively. EpiData version 3.1 was used for data entry, then exported to statistical package for social science. Multivariable logistic regression models were used for study variables with p-values less than 0.25. In the multivariable model, the adjusted odds ratio and its 95% confidence interval were calculated, and a p-value of less than 0.05 was deemed statistically significant. Thematic analysis was used to examine qualitative data. Graphs, tables, and text were used to display the results. Results: A total of 403 participants were recruited for the study, of whom 394 mothers completed the interview, yielding a response rate of 97.77%. The overall proportion of women satisfied with immediate postnatal care was 242 (61.4%) [95% CI: 57%–66%]. Birth plan (AOR = 2.02; 95% CI: 1.16–3.51). Labor duration (AOR = 1.73; 95% CI: 1.09–2.76). Women who experienced complications (AOR = 2.42; 95% CI: 1.15–5.10), and initiating breastfeeding (AOR = 1.86; 95% CI: 1.12–3.11). Conclusion and Recommendation: Over 50% of women expressed satisfaction with the immediate postnatal care they received. Managers of healthcare institutions and medical professionals collaborate closely to increase postpartum mom satisfaction.
|
Published in
|
Rehabilitation Science (Volume 11, Issue 1)
|
|
DOI
|
10.11648/j.rs.20261101.12
|
|
Page(s)
|
13-28 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2026. Published by Science Publishing Group
|
Keywords
Women Satisfaction, Immediate Postnatal Care, Public Hospital and South West Shoa
1. Introduction
The first 24 hours following delivery are known as the "immediate postnatal period," during which the infant's physiology adjusts and the mother's risks and other serious morbidities are at their maximum
| [1] | Health M. Observation of mother and baby in the immediate postnatal period : consensus statements guiding practice. 2012; (July): 1-4. |
[1]
. The goal of postnatal care services is to give moms and newborns the proper care. Additionally, it guards against issues that could jeopardize their life
| [2] | Tsegaye B, Amare B, Reda M. Prevalence and Factors Associated with Immediate Postnatal Care Utilization in Ethiopia : Analysis of Ethiopian Demographic Health Survey 2016 Prevalence and Factors Associated with Immediate Postnatal Care Utilization in Ethiopia : Analysis of Ethiopian. Published online 2022. https://doi.org/10.2147/IJWH.S294058 |
| [3] | Postnatal care of the mother and newborn 2013. Published online 2013. |
[2, 3]
.
Because satisfaction is influenced by so many different things, it is challenging to conceptually define across the many factors influencing this degree of enjoyment are expectations of mothers, which may range across women due to variations in a context such as their social background, education level, and personal preferences
| [4] | Okonofua F, Ogu R, Agholor K, Okike O, Abdus-salam R, Gana M. Qualitative assessment of women ’ s satisfaction with maternal health care in referral hospitals in Nigeria. Published online 2017: 1-8. https://doi.org/10.1186/s12978-017-0305-6 |
[4]
.
Women's satisfaction with immediate postpartum care is a broad notion that encompasses their level of satisfaction, the postnatal ward's physical setting, and the quality of care provided. The useful reported criterion for assessing the caliber of birth care services is women's contentment during the postpartum period
| [5] | Ilesanmi RE, Akinmeye JA. Evaluation of the quality of postnatal care and mothers ’ satisfaction at the university college hospital Ibadan, Nigeria. 2018; 10(September): 99-108.
https://doi.org/10.5897/IJNM2018.0314 |
[5]
. Maternal satisfaction can be influenced by a number of elements, including the physical environment and infrastructure, the continuity of services offered to mothers, access, knowledge, and attention to psychological difficulties
| [6] | Mehata S, Paudel YR, Dariang M, et al. Factors determining satisfaction among facility-based maternity clients in Nepal. Published online 2017: 1-10.
https://doi.org/10.1186/s12884-017-1532-0 |
| [7] | Lazzerini M, Mariani I, Semenzato C, Valente EP. Association between maternal satisfaction and other indicators of quality of care at childbirth : a cross- sectional study based on the WHO standards. Published online 2020.
https://doi.org/10.1136/bmjopen-2020-037063 |
[6, 7]
.
All mothers and their babies must receive active and ongoing assessment in the immediate postnatal period, regardless of the context around their birth. During this time, the mother and baby should not be left alone – even for a short time. Ongoing assessment is for a minimum of one hour. Assessment will be longer than one hour if the mother or baby has experienced factors that increase their risk of adverse outcomes. Care during this time supports the physiological processes of the mother’s transition to motherhood and the baby’s transition to independent life
| [1] | Health M. Observation of mother and baby in the immediate postnatal period : consensus statements guiding practice. 2012; (July): 1-4. |
[1]
.
At first postnatal contact, giving the woman the opportunity to talk about her birth experience, and provide information about relevant support and birth reflection services makes them happy with their postnatal care
.
Mothers' satisfaction serves as an outcome indication of the effectiveness and caliber of care provided by health care systems, with medical professionals' care being a key determinant of overall client satisfaction
| [9] | Battawi JAA, Hafiz SK. Evaluation of Postnatal Mother ’ s Satisfaction with Nursing Care In El-Shatby Maternity University Hospital. 2017; 6(6): 69-80.
https://doi.org/10.9790/1959-0606026980 |
| [10] | Wolka S, Assegid S, Tantu T, Gunta M, Duko B. Determinants of Maternal Satisfaction with Existing Delivery Care at Wolaita Sodo University Teaching and Referral. 2020; 2020. |
[9, 10]
.
Over 830 women worldwide lost their lives to pregnancy and childbirth-related complications in less than a day. Low- and middle-income nations account for 94% of all maternal deaths
| [11] | WHO. Maternal mortality Evidence brief. 2017; (1): 1-4. |
[11]
. States have pledged to reduce the maternal death ratio to fewer than 70 per 100,000 live births between 2015 and 2030 as part of Sustainable Development Goal 3. Therefore, by 2030, it will be a global priority to address the existing rates of maternal and newborn mortality in low- and middle-income nations
| [12] | WHO, Group WB. Trends in Maternal Mortality : 1990 to 2015. Published online 2015. |
[12]
. The illness is most prevalent in Sub-Saharan Africa, where estimates of severe maternal morbidity can reach 108 per 1,000 live births
| [13] | Geller SE, Koch AR, Garland CE, MacDonald EJ, Storey F, Lawton B. A global view of severe maternal morbidity: Moving beyond maternal mortality. Reprod Health. 2018; 15 (Suppl 1). https://doi.org/10.1186/s12978-018-0527-2 |
[13]
. The first 24 hours following birth account for a significant percentage of mother and newborn deaths
| [14] | Demographic M, Survey H. Ethiopia.; 2019. |
[14]
. Giving immediate postnatal care, regardless of the context around their birth reduce maternal and neonatal deaths and morbidity
| [15] | Mirzaii K, Ghadikolaee SO, Bazzaz MM, Ziaee M. Mother ’ s satisfaction of postpartum care and its relationship with midwifery care at Urban Health Centers, Mashhad, Iran. 2015; (Md). |
[15]
.
A study done in Spain, Iran and India shows that 94.54%, 92% of and vaginal birth 68.7%, and Caesarean section 79.2% of women were satisfied with childbirth and postnatal care services respectively
| [15] | Mirzaii K, Ghadikolaee SO, Bazzaz MM, Ziaee M. Mother ’ s satisfaction of postpartum care and its relationship with midwifery care at Urban Health Centers, Mashhad, Iran. 2015; (Md). |
| [16] | Jha P, Larsson M, Christensson K, Svanberg AS. Satisfaction with childbirth services provided in public health facilities: Results from a cross-sectional survey among postnatal women in Chhattisgarh, India. Glob Health Action. 2017; 10(1).
https://doi.org/10.1080/16549716.2017.1386932 |
| [17] | Mahía LP, López SB, Pillado TS, Díaz SP. Women ’ s satisfaction with childbirth and postpartum care and associated variables. Published online 2021: 1-7. |
[15-17]
. In Egypt, 51.9% of mothers who gave birth in African countries were satisfied with their postpartum treatment
| [18] | El MM, Ahmed A, Hables RM, Mohamed SH. Women Satisfaction Regarding Utilization of Post Natal Care in Alexandria Government. 2020; 7(3): 625-635. |
[18]
, and 26.2% in Zambia
| [19] | Zulu M, Chanda D. IMothers’ satisfaction with immediate postnatal care provided at ndola central hospital, zambia. 2019;(December 2017). |
[19]
. However, in Ethiopia, the proportion of women who were satisfied with immediate postnatal care ranged from 60.9% to 63%
| [20] | Adane D, Wassihun B. Client satisfaction with existing postnatal care and associated factors : A study among mothers in Awi Zone, Amhara region, Ethiopia. Published online 2020.
https://doi.org/10.1177/1745506520976017 |
| [21] | Bekele SB. Immediate Postnatal Care Satisfaction and Associated Factors Among Postnatal Women in Public Health Facilities at Debre Markos Town,. Published online 2022: 137-147. |
[20, 21]
. Maternal satisfaction with immediate postpartum care is negatively impacted by a number of factors, including lengthy wait times, inappropriate drug and supply availability, disrespectful treatment, invasion of privacy, unclean healthcare facilities, unplanned pregnancies, and complicated feta-maternal birth outcomes
| [22] | Babure ZK, Assefa JF, Weldemarium TD. Maternal Satisfaction and Associated Factors towards Delivery Service among Mothers Who Gave Birth at Nekemte Specialized Hospital, Nekemte Town, East Wollega Zone, Oromia Regional State, Western Ethiopia, 2019 : A Cross- sectional Study Design Journ. Published online 2019: 1-11.
https://doi.org/10.35248/2167-0420.20.9.489.Copyright |
| [23] | Abebe A, Menta AA. Nutrition and Dietetic Practice Mothers ’ Satisfaction with Institutional Delivery Service and Associated Factors among Women Attending Hospitals in. 2018; 2(2): 1-12. |
| [24] | Asres GD. Satisfaction and Associated Factors among Mothers Delivered at Asrade Zewude Memorial Primary Hospital, Bure, West Gojjam, Amhara, Ethiopia: A Cross Sectional Study. Prim Heal Care Open Access. 2018; 08(02).
https://doi.org/10.4172/2167-1079.1000293 |
| [25] | Bishaw KA, Temesgen H, Amha H, et al. A systematic review and meta-analysis of women’s satisfaction with skilled delivery care and the associated factors in Ethiopia. SAGE Open Med. 2022; 10: 205031212110682.
https://doi.org/10.1177/20503121211068249 |
| [26] | Mocumbi S, Högberg U, Lampa E, et al. Mothers ’ satisfaction with care during facility-based childbirth : a cross-sectional survey in southern Mozambique. 2019; 6: 1-14. |
| [27] | Berhe H. Status of Caring, Respectful and Compassionate Health Care Practice in Tigrai Regional State : Patients ’ Perspective. 2017; 10(3): 1118-1128. |
| [28] | Obsa MS. Maternal satisfaction towards childbirth Service in Public Health Facilities at Adama. Published online 2020: 4-11. |
| [29] | Zemenu Yohannes Kassa TA. Maternal Satisfaction and Associated Factors on Delivery Care Service in Gynecology & Obstetrics Maternal Satisfaction and Associated Factors on Delivery Care Service in. 2018; (February 2019).
https://doi.org/10.4172/2161-0932.1000473 |
[22-29]
.
The results of a study conducted in Tanzania, Ethiopia, and Bahir Dar revealed that mothers' unhappiness with childbirth services was a significant deterrent to women preferring institutional delivery
| [30] | Dar B. Compassionate and respectful maternity care during facility based child birth and women ’ s intent to use maternity service in. Published online 2018: 1-9. |
| [31] | Makuka, MD GJ, Sango, MD MM, Mashambo, MD AE, Mashambo, MD AE, Msuya, MD, PhD SE, Mtweve, MD, MSc SP. Clients’ Perspectives on Quality of Delivery Services in a Rural Setting in Tanzania: Findings from a Qualitative Action-Oriented Research. Int J Matern Child Heal AIDS. 2017; 6(1): 60-68. https://doi.org/10.21106/ijma.191 |
[30, 31]
. Traditional birth attendance was chosen by mothers who objected to the healthcare provider's cordial manner during childbirth
| [32] | Zone H, Delibo D, Damena M, Gobena T, Balcha B. Status of Home Delivery and Its Associated Factors among Women Who Gave Birth within the Last 12 Months in East Badawacho. 2020; 2020. |
| [33] | Ngowi AF, Kamazima SR, Kibusi S, Gesase A, Bali T. Women’s determinant factors for preferred place of delivery in Dodoma region Tanzania: A cross sectional study. Reprod Health. 2017; 14(1): 1-8.
https://doi.org/10.1186/s12978-017-0373-7 |
[32, 33]
.
As the results of study conducted in Eritrea and Zambia revealed that mothers who were not pleased with the value of attention during delivery and post-natal care were prefer their future childbirth in-home
| [34] | Kifle MM, Kesete HF, Gaim HT, Angosom GS, Araya MB. Health facility or home delivery ? Factors influencing the choice of delivery place among mothers living in rural communities of Eritrea. 2018; 1: 1-15. |
| [35] | Sacks E, Masvawure TB, Atuyambe LM, Neema S. Postnatal Care Experiences and Barriers to Care Utilization for Home- and Facility-Delivered Newborns in Uganda. Matern Child Health J. Published online 2016.
https://doi.org/10.1007/s10995-016-2144-4 |
[34, 35]
.
Maternal happiness with childbirth offers vital and economical input for enhancing institutional childbearing services.
| [36] | Federal Democratic Republic of Ethiopia Ministry of Health. Health Sector Transformation Plan II 2020/21-2024/25 (2013EFY-2017EFY). 2021; 25(February). |
[36]
. Postpartum care satisfaction has both immediate and long-term benefits for the mother's health, subsequent uptake, and the institution's recommendation to their neighbors and relatives
.
Ethiopia has made impressive strides in increasing the availability of healthcare providers, building infrastructure quickly, allocating more funds, and improving financial management. But just 50% of women gave birth in a hospital. Up until now, it has been quite difficult to maintain and raise service quality. Consequently, delivering high-quality healthcare has emerged as a key transition objective
| [36] | Federal Democratic Republic of Ethiopia Ministry of Health. Health Sector Transformation Plan II 2020/21-2024/25 (2013EFY-2017EFY). 2021; 25(February). |
| [37] | Adnan FI, Mohd N, Id N, Akma N, Junoh M. Associated factors of labor satisfaction and predictor of postnatal satisfaction in the north-east of Peninsular Malaysia. Published online 2020: 1-19. https://doi.org/10.1371/journal.pone.0238310 |
[36, 37]
.
Most studies conducted in Ethiopia on maternal satisfaction with immediate postnatal care have primarily utilized quantitative study designs. However, relying solely on quantitative methods may not adequately capture the detailed factors influencing women’s feelings, expectations, and experiences regarding postnatal care. In the South West Shoa Zone, there is limited evidence from studies that have employed both quantitative and qualitative approaches to assess maternal satisfaction with immediate postnatal care in public hospitals. Therefore, this study aimed to assess the factors associated with women’s satisfaction with immediate postnatal care in public hospitals of South West Shoa Zone, Ethiopia, using a mixed-methods approach.
2. Methods and Materials
2.1. Study Area and Study Period
The study was conducted at a public hospital in Ethiopia's South West Shoa Zone. It is situated 114 kilometers south of Addis Ababa. According to the Central Statistical Agency of Ethiopia's 2007 census, 70321 people are living in this town, of which 35865 are males and 34457 are women out of the 13101 people who are of reproductive age. The Southwest Shoa Zone included one non-government hospital, Lukas Catholic Hospital, located in Waliso, the region's capital, and five government hospitals, Tullu Bollo General Hospital, Waliso General Hospital, Ameya Primary Hospital, Bantu Primary Hospital, and Leman Primary Hospital. Additionally, it has 28 pharmacies, 72 private clinics, 264 health posts, 54 health facilities, and 8 private pharmacies.
The study was conducted at Tullu Bollo General Hospital and Waliso General Hospital. Last year's immediate postnatal cares were 2280 and 2640 in Tullu Bollo general hospital and Waliso General Hospital, respectively. The study was conducted from October 10 – December 10, 2023.
2.2. Study Design
An Institutional-based, cross-sectional study design was supplemented by a qualitative study / convergent parallel study design/ was conducted.
2.3. Source Population
All women who delivered at public hospitals, in south west shoa zone in 2023.
2.4. Study Population
All selected mothers by systematic random sampling at public hospitals, in south west shoa zone during data collection period.
2.5. Eligibility Criteria
2.5.1. Inclusion Criteria
A women who gave birth and received immediate postnatal care and discharged from the hospitals by health care providers were included in the current study.
2.5.2. Exclusion Criteria
1) Women who are critically ill and unable to communicate face-to-face interviews and in-depth interviews at the time of data collection were excluded from this study.
2) Women who were referred to other hospitals were excluded from this study.
3) Women who were delivered at others health facility and referred for post-natal was excluded from the study.
4) Women who were gave stillbirth and IUFD (intra uterine fetal death) was excluded from this study.
2.6. Sample Size Determination and Sampling Technique
2.6.1. Sample Size Determination
Based on a prior study carried out in Public Health Facilities, Debre Markos Town, Northwest Ethiopia, the sample size was determined using the single proportion population formula for the first specific objective, assuming a 95% confidence level with a marginal error of 5%. The proportion of women satisfied with immediate postnatal care was 60.9% (0.609).
| [21] | Bekele SB. Immediate Postnatal Care Satisfaction and Associated Factors Among Postnatal Women in Public Health Facilities at Debre Markos Town,. Published online 2022: 137-147. |
[21]
.
Where n= number of the study subjects
Z= is standardized normal distribution value for the 95% confidence interval (1.96)
P = women satisfaction with immediate postnatal care was (0.609)
q=1-p =1-0.609 =0.0.391, p=0.609 and q =0.391
d = the margin of error taken as 5% = 0.05
By adding 10% (37) non-response rates the final sample size required for the quantitative study was 403.
To Calculate the sample size for the second objective different kinds of literature were reviewed to select the variables, and then the sample size was calculated for those selected variables by using a double population proportion formula for analytic cross-sectional in Epi info version 7.2.5 (see
Table 1).
Table 1. Sample size determination for the second specific objective of women`s satisfaction with immediate post-natal care among mothers who gave birth in public hospital, South West Shoa Zone, Ethiopia, 2024.
Variables | CI | Power | P1 | P2 | AOR | Ratio | Sample Size | 10% Non-response rate | Final Sample Size | Reference |
95% | 80% |
Mode of delivery | 95% | 80% | 72.19 | 26.2 | 3.14 | 1:1 | 120 | 29 | 319 | | [20] | Adane D, Wassihun B. Client satisfaction with existing postnatal care and associated factors : A study among mothers in Awi Zone, Amhara region, Ethiopia. Published online 2020.
https://doi.org/10.1177/1745506520976017 |
[20] |
Maternal outcome | 95% | 80% | 68.69 | 43.01 | 2.9 | 1:1 | 132 | 12 | 128 | | [20] | Adane D, Wassihun B. Client satisfaction with existing postnatal care and associated factors : A study among mothers in Awi Zone, Amhara region, Ethiopia. Published online 2020.
https://doi.org/10.1177/1745506520976017 |
[20] |
ANC follow up | 95% | 80% | 63.23 | 47.42 | 1.9 | 1:1 | 338 | 20 | 218 | | [21] | Bekele SB. Immediate Postnatal Care Satisfaction and Associated Factors Among Postnatal Women in Public Health Facilities at Debre Markos Town,. Published online 2022: 137-147. |
[21] |
Key
P1 Proportion of outcome among population with the exposure of interest
P2 Proportion of outcome among population without the exposure of interest
By comparing all sample size, large sample was taken; therefore, the final sample size for this study was 403 for quantitative study.
2.6.2. Study Participant Recruitment for Qualitative Study
Homogenous purposive sampling procedure was employed to select participants for qualitative part of the study. Selection was done consciously and purposefully according to certain standards that were pertinent to the goals of the study. Purposive sampling was carried out using the following procedures: Determining the target population: Women who delivered in public hospitals in Ethiopia's Southwest Shoa Zone in 2024 were considered the target population. The selection of participants was guided by well-defined inclusion criteria. Women mothers who delivered at public hospitals via instrumental delivery were included in these criteria, cesarean section spontaneous vaginal delivery. To make sure the sample reflected the intended demographic, exclusion criteria were also established. Individuals who were unable or rejected to participate, had serious comorbidities, or had mental health conditions were omitted. In order to examine the moms who provided birth profiles of possible participants, the lead investigator worked with the hospital administrators. This partnership made it easier to find mothers who fit the study's inclusion requirements and were qualified participants. Participants were chosen with intention and in accordance with the established criteria. The purpose of this study was to guarantee a wide variety of viewpoints and experiences about women's satisfaction with immediate postpartum treatment. Sampling was carried out repeatedly until data saturation was reached. In this instance, after interviewing a total of 17 subjects, the researchers concluded that data saturation had been reached.
2.6.3. Sampling Technique
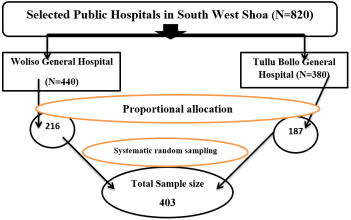
Figure 1. Schematic presentation of sampling procedure on women`s satisfaction with immediate post-natal care among mothers who gave birth Public Hospitals, South West Shoa Zone, Ethiopia 2024.
The number of study participants from each public hospitals were determined by proportional allocation to population size by using an average of two months reports of last year reports was used. Then two months reports of last year immediate postnatal care for both public hospitals (N) were divided by total sample size (n) to obtained the interval (K), K= N/n, K= 820/403, k= 2.034- 2. The first study participant was determined by lottery methods.
Then, by using a systematic random sampling method the data collectors were interviewed mothers every two-interval daily at the time of after finish all service, but before leaving the health facility (exit face to face interview) until the required sample size was obtained.
Proportional allocation: allocating sampling proportional to the total population of each hospital using. The formula: ni = Ni/N * n, where n = total sample size to be selected, N = total population.
Ni = total population of each hospital, ni = sample size from each hospital (see
Figure 1).
2.7. Data Collection Instrument and Technique
2.7.1. Data Collection Instrument
A Structured tool was adapted after reviewing different kinds of literature
| [15] | Mirzaii K, Ghadikolaee SO, Bazzaz MM, Ziaee M. Mother ’ s satisfaction of postpartum care and its relationship with midwifery care at Urban Health Centers, Mashhad, Iran. 2015; (Md). |
| [17] | Mahía LP, López SB, Pillado TS, Díaz SP. Women ’ s satisfaction with childbirth and postpartum care and associated variables. Published online 2021: 1-7. |
| [18] | El MM, Ahmed A, Hables RM, Mohamed SH. Women Satisfaction Regarding Utilization of Post Natal Care in Alexandria Government. 2020; 7(3): 625-635. |
| [21] | Bekele SB. Immediate Postnatal Care Satisfaction and Associated Factors Among Postnatal Women in Public Health Facilities at Debre Markos Town,. Published online 2022: 137-147. |
| [38] | Bulto GA, Demissie DB, Tasu TL, Demisse GA. Mother’s satisfaction with the existing labor and delivery care services at public health facilities in West Shewa zone, Oromia region, Ethiopia. BMC Pregnancy Childbirth. 2020; 20(1): 1-12.
https://doi.org/10.1186/s12884-020-02998-6 |
[15, 17, 18, 21, 38]
. The tool consisted of 7 items of Socio-demographic characteristics, 10 items of Obstetrics related factors, and 25 items of satisfaction assessment questions. The questionnaires contain 3 parts and 42 items.
The qualitative data was collected by using a semi-structured interview guide tools with probing questions linked to women pleasure aspects. During the in-depth interview, voice recorded and notes were taken. The questionnaires contain guiding questions and probing questions.
2.7.2. Data Collection Technique
The data were gathered using a pre-tested structured face-to-face interview tool and guiding question prepared by Afan Oromo. The data was gathered by three BSc midwives who are fluent in the local language and supervised by two MPH.
In-depth interviews (IDIs) were conducted to obtain a more comprehensive picture of women's satisfaction with immediate post-natal care. Using pertinent literature as a resource, a topic guide was created. A team of one seasoned researcher with a solid background in qualitative data collecting conducted in-depth interviews with women on their satisfaction with immediate postpartum care. As a facilitator and data collector, the main investigator (PI) was essential in making sure the interviews went smoothly. For the interviews, the PI carefully chose a setting that would be comfortable and accommodating, such as a quiet, private area at a participant.
These venues sought to establish a secure and encouraging environment that inspired people to freely discuss their experiences. Questions about women's satisfaction with immediate postpartum treatment and their personal experiences were posed to the participants. Participant responses throughout the interviews led to additional investigation and explanation of their experiences.
2.8. Operational Definitions
Women`s satisfaction with immediate post-natal care was measured by using Likert scale and participants was asked to rate their satisfaction level using 5 Likert scale point. The five-point Likert scale was merged into two outcome variables for analysis purposes. These were dissatisfied and satisfied. Strongly disagree, disagree, and neutral responses was considered as dissatisfied. Neutral responses were considered dissatisfied because the women were interviewed at the health facility, they feared and were reluctant when they were dissatisfied. Whereas agree, and strongly agree were considered as satisfied. Then a response was added and converted to give an overall women's satisfaction score.
Satisfied: Women who score 75% and more from the items of women`s' Satisfaction tools were categorized as satisfied with the overall satisfaction.
Unsatisfied: Women`s` who score below75% from the items of women Satisfaction questionnaires, were categorized under unsatisfied for the overall satisfaction
| [28] | Obsa MS. Maternal satisfaction towards childbirth Service in Public Health Facilities at Adama. Published online 2020: 4-11. |
| [29] | Zemenu Yohannes Kassa TA. Maternal Satisfaction and Associated Factors on Delivery Care Service in Gynecology & Obstetrics Maternal Satisfaction and Associated Factors on Delivery Care Service in. 2018; (February 2019).
https://doi.org/10.4172/2161-0932.1000473 |
[28, 29]
.
2.9. Data Quality Control (Assurance) and Data Processing and Analysis
To ensure the quality of tools, tools was adapted from related articles, pre-tested on fifty of the study participants (50 mothers) who gave birth at Holeta primary Hospital. The collected data was entered to EpiData version 3.1 and exported to SPSS version 25 to assess the reliability of satisfaction assessing tool by Cron bach alpha analysis and its value was 0.914. To ensure the consistency of the questionnaires, the English version was translated into Afan Oromo and again retranslated back to English by a language translator expert.
The data collectors and supervisors were recruited from out of the employee of the study hospitals to minimize bias and one day training was given for data collectors and supervisors regarding data collection procedure, tools, the purpose of study, and ethical consideration. Data collectors were strictly supervised. At the end of each day, the questionnaires were reviewed and checked for completeness by the supervisors, and corrections were made.
The collected data were checked for completeness, by the investigator and supervisor before data entry into the application and each questionaries’ approved to enter the application for analysis was correctly coded, and given a specific Identification number.
2.9.1. Trustworthiness of the Qualitative Study
In qualitative study, the researcher implemented various strategies to uphold trustworthiness. First, credibility was enhanced through prolonged engagement with participants, allowing for an in-depth understanding of their experiences. To fully investigate their viewpoints, several trips and interviews were undertaken. The gathered data was validated and corroborated by triangulation, which was accomplished by combining field notes and audio recordings. Second, Transferability was ensured by providing a detailed description of the research setting, including the hospitals and their gynecological and delivery wards. The inclusion and exclusion criteria were detailed in order to ensure that the sample was representative of the intended demographic. This information can be used by readers to assess if the results apply to other groups or situations.
Third, Careful documenting of the study methodology, data collection techniques, and analysis techniques promoted reliability. Other researchers may be able to replicate or verify this transparency. The reliability of the study's conclusions is further enhanced by the application of a purposive sampling technique and well specified participant selection criteria. Additionally, reflexivity critically analyzing one's own biases and presumptions during the research process was used to increase confirmability. This self-awareness reduced the possibility that assumptions might affect how the evidence was interpreted. Keeping an audit trail, recording decision-making procedures, and guaranteeing impartiality and openness. Finally, one tactic used to increase credibility was member checking. In order to guarantee that their viewpoints were fairly represented in the final analysis, participants were given the chance to examine and comment on the results.
2.9.2. Data Processing and Analysis
Data were entered into Epi data 3.1 to minimize errors, to check double data entered and design skipping pattern. Outlier and missed data were checked before data analysis by exporting to SPSS version 25. Mult co-linearity was checked by using variance inflation factors. The values of variance inflation factors were ranged 1.03-5.43 and tolerance test was ranged 0.18-0.97. Model goodness of fit was checked by Hosmer – Lermeshows, it was 0.89.
Descriptive analysis (like frequencies, percentages, means, and standard deviation) and inferential analysis were done. The bivariate and multivariable logistic regression analyses were done. A p-values < 0.25 association study variables were transferred to multiple logistic regression models. AOR (adjusted odds ratio) with their 95% confidence interval was computed, and the p-value < 0.05 was considered statistically significant in the multivariable. The results were presented using text, tables, and charts.
Qualitative data were analyzed thematically by transcribing recorded audio and notes taken during the Interviews. The recorded audio was first transcribed word by word into Afan Oromo, and then translated into English by the language translator. The transcribed data into English was coded manually (color-coded) with similar ideas with the same code. Then, the narrated qualitative information was organized and categorized according to their similar ideas to form sub-themes. Sub-themes emerged together to form the main themes. Then, the study participant's comment was written in quotes. Ideas related to the objective of the study and commonly indicated by study participants was taken to triangulate with the quantitative results and included in the report.
 2.10. Ethical Consideration
2.10. Ethical Consideration An ethical clearance letter was obtained from Ambo University institutional review board by Ref number AUWC/PG/12/16 on date 07/02/2016 EC and a supportive letter were obtained from the College of Health Science Waliso Campus. Official letters of cooperation were obtained from Zonal Health Bureau and permissions for data collection were obtained from all health facility. Verbal informed consent from study participants before the interview was obtained. The study's goal and the significance of their involvement in providing data that may be used to gauge maternal satisfaction with delivery services were explained to the participants. Additionally, the study participants were advised that they could stop at any moment if they so desired, as well as skip questions or those they did not want to answer completely or in part. The interview took place in a private, separate location. They were given the questionnaire and instructed on how to answer it once their consent and willingness to participate in the study were obtained.
3. Results
A data was gathered among 403 participants, and 394 women were completed the interview giving the response rate of 97.77%. The 9 questionnaires were incomplete and excluded from the analysis.
3.1. Socio-demographic Characteristics of the Respondents
The minimum age of respondents were 18 years while the maximum was 45 years with a mean age of 28.0 (SD± 6.61). Among 394 of the study participants greater than half, 200(50.8%) of women were living in rural area. More than three-fourths, 359(91.1%). of the study participants were married. One hundred forty (35.5%) of women had secondary education by educational level. Regarding occupational status 98(24.9%) of the women were housewife (see
Table 2).
Table 2. Socio-demographics characteristics of mothers who gave birth at public hospitals, South West Shoa, Ethiopia, 2023 (n= 394).
Variables | Variables Categories | Frequency | Percent |
Residency | Urban | 194 | 49.2 |
Rural | 200 | 50.8 |
Marital status | Unmarried | 35 | 8.9 |
Married | 359 | 91.1 |
Educational status | No formal education | 67 | 17.1 |
Primary Education | 123 | 31.2 |
Secondary Education | 140 | 35.5 |
Diploma and above | 64 | 16.2 |
Occupational status | Housewife | 98 | 24.9 |
Farmer | 89 | 22.6 |
Merchant | 87 | 22 |
Government employee | 53 | 13.5 |
Self-Employee | 67 | 17.0 |
Means of come | By referral | 165 | 41.9 |
By friends and relatives | 72 | 18.3 |
By self | 157 | 39.8 |
Types of visit | New | 236 | 59.9 |
Repeat | 158 | 40.1 |
3.2. Maternal Obstetrics Characteristics
In this study among 394 respondents more than half, 228(57.9%) of mothers was multiparous. More than three-fourths, 323(82%) of women were planned their current pregnancy. Among 394 respondents, the majority, 344(87.3%) of them were had ANC follow-ups. However, only 162(47.1%) women had fourth and above four visits (see
Table 3).
Table 3. Obstetrics characteristics of women who gave birth at public hospitals, South West Shoa, Ethiopia, 2023 (n= 394).
Variables | Variables Categories | Frequency | Percent |
Parity | Primiparous | 166 | 42.1 |
Multiparous | 228 | 57.9 |
Status of current Pregnancy | Planned | 323 | 82.0 |
Unplanned | 71 | 18.0 |
ANC follow-up | Yes | 344 | 87.3 |
No | 50 | 12.7 |
Number of ANC visit (n=344) | First visit | 10 | 2.9 |
Second visit | 53 | 15.4 |
Third visit | 119 | 34.6 |
Fourth visit and above | 162 | 47.1 |
Birth plan | Planned | 322 | 81.7 |
Unplanned | 72 | 18.3 |
Labor duration | Less than or equal 12 hour | 206 | 52.3 |
Greater than 12 hour | 188 | 47.7 |
Mode of delivery | Spontaneous vaginal delivery | 202 | 51.3 |
Instrumental delivery | 75 | 19.0 |
cesarean section | 117 | 29.7 |
Maternal outcome | Without complication | 356 | 90.4 |
With complication | 38 | 9.6 |
Mothers with complication (n=38) | Postpartum hemorrhage | 11 | 28.9 |
puerperal sepsis | 22 | 57.9 |
perineal and cervical laceration | 2 | 5.3 |
retained placenta | 3 | 7.9 |
Fetal outcome | Normal | 290 | 73.6 |
With complication | 104 | 26.4 |
Breast feeding | within first hour | 305 | 77.4 |
after first hour | 89 | 22.6 |
3.3. Immediate Postnatal Care Women Satisfaction Related to Interpersonal
The findings of this study showed that 325(82.5%) of the respondents were satisfied with availability of doctors and midwives during postnatal period. Among 394 mothers, 271(68.8%) were satisfied respection given while giving care. Regarding close follow up by health care provider more than two-third, 281 (71.3%) of them were satisfied. More than three-fourths, 318(80.7%) of women were satisfied with monitored maternal BP, PR, RR, temperature, Vaginal bleeding and Newborn`s RR, PR temperature and cord care by health care providers. Concerning assisting in early ambulation 303(76.9%) of moms were satisfied with postnatal care given by health care providers. Greater than two-third, 266(67.5%) of women were satisfied with assistance given by health care providers during perineal care (see
Table 4).
This also supported by the results of the qualitative study women were satisfied when health care providers stay with them during postnatal period and labored along. This was supported by the result from IDI:
“… The midwives were stay with me after I gave birth; they come quickly when I called them to help me. Also, I labored for a long time (one and half days), the way I gave birth was very disgusting [dissatisfied]. Why health professional serves mothers like this are good” (WR2, 26 years old).
“Health caregivers’ stay with me, they gave me care when I wanted, they decided to give birth via surgical operation [cesarean section] after I labored for two days, and I got tired [long labour duration]. After I gave birth by surgical operation, I was sick and stayed one week in this hospital…during this time they help me as sisters” (WR4, 27 years old).
In addition, the respondents were dissatisfied with the care given by health care providers during immediate postnatal period. Women who were helped while breast feed her baby were satisfied with immediate postnatal care. The following were some of the women`s’ sentiments:
“…I got discomfort after I gave my baby. I asked one health profession to feed my newborn my breast. She was not refused me by saying she will feed by herself gave your breast frequently. So, my baby start feeding within hours. For other women its good if assistance continues like this while stayed in hospital” (WR11, 24 years old).
“This was my first birth. so, my breast didn`t expel to feed my baby. I feared to inform this, but I saw that when they push breast of others mother by something (breast sucker) after some time her breast milk start to eject. They asked me and gave that services for me. If they treat every mother equally it would be fantastic” (WR8, 22 years old).
“After I gave birth by reproductive organ (spontaneous vagina delivery) my baby was couldn`t feed my breast timely. I bored with that situation... but they help me more” (WR5, 18 years old).
Table 4. Interpersonal-related of women satisfaction with immediate postnatal care among women who gave birth in public hospitals, South West Shoa Zone, Ethiopia, 2023 (n=394).
Variables | Variables Category | Frequency | Percent |
Available doctors and midwives | Satisfied | 325 | 82.5 |
Dissatisfied | 69 | 17.5 |
Respecting the mother while giving care | Satisfied | 123 | 31.2 |
Dissatisfied | 271 | 68.8 |
Examination after the mother's permission | Satisfied | 315 | 79.9 |
Dissatisfied | 79 | 20.1 |
Assured privacy | Satisfied | 257 | 65.2 |
Dissatisfied | 137 | 34.8 |
Close follow-up by the health care provider | Satisfied | 281 | 71.3 |
Dissatisfied | 113 | 28.7 |
Listen to and answer all mothers’ questions | Satisfied | 300 | 76.1 |
Dissatisfied | 94 | 23.9 |
labour pain management | Satisfied | 298 | 75.6 |
Dissatisfied | 96 | 24.4 |
allowing families to stay with mothers | Satisfied | 304 | 77.2 |
Dissatisfied | 90 | 22.8 |
Monitoring maternal and Newborn | Satisfied | 318 | 80.7 |
Dissatisfied | 76 | 19.3 |
Health care providers stay with mothers | Satisfied | 315 | 79.9 |
Dissatisfied | 79 | 20.1 |
Assisting in early ambulation | Satisfied | 303 | 76.9 |
Dissatisfied | 91 | 23.1 |
Assisting in perineal care | Satisfied | 266 | 67.5 |
Dissatisfied | 128 | 32.5 |
3.4. Immediate Postnatal Care Women Satisfaction Related to Information
According to the result of the current study, 237(60.2%) of women were satisfied with the information given about the result of their examination. Three hundred nine (78.2%), and 301(76.4%) of the respondents were satisfied with the information given by health care providers about postpartum family planning, and about baby’s immunization respectively. Concerning information given about breast-feeding 303(76.9%) of them were satisfied (see
Table 5).
This also supported by the results of the qualitative study, women who were informed about the result of their examination, and baby’s condition were very satisfied with immediate postnatal services. The following were some of the women`s ideas:
“...Midwives tells when vaccine my baby, how to keep myself clean, how to breastfeed newborn. I t think the ways they served me is very good [women satisfied with information received] …” (WR5, 18 years old).
“The health care providers inform me the results of my tests [laboratory test], my labour progress, and the condition of my newborn. I was very sick after seven-hour delivery. I was satisfied with their information...” (WR10, 30 years old).
“...Midwives counsel me the advantage of early walking after delivery, how to breastfeed my newborn, and advantage of first milk for the newborn. I am t happy with their counseling.” (WR6, 18 years old).
“…Health care providers tell me the progress of my condition after examination and the condition of my baby`s, they just checked me and not left me alone without any advice.” (WR10, 30 years old).
“As soon as I arrived at the postnatal ward. First midwives assessed me, then they told me saying you are bleeding let we consult the doctor. Then, the doctor came and assessed me, and simply he got out. He tells me about myself. After that, I did feels better…” (WR15, 28 years old).
Table 5. Information-related women satisfaction with immediate postnatal care among women who gave birth in public hospitals, South West Shoa Zone, Ethiopia, 2023(n=394).
Variables | Variables Category | Frequency | Percent |
Information about the results of an examination | Satisfied | 237 | 60.2 |
Dissatisfied | 157 | 39.8 |
Information about postpartum family planning | Satisfied | 309 | 78.4 |
Dissatisfied | 85 | 21.6 |
Information about baby’s immunization | Satisfied | 301 | 76.4 |
Dissatisfied | 93 | 23.6 |
Information about breast-feeding | Satisfied | 303 | 76.9 |
Dissatisfied | 91 | 23.1 |
Information about personal hygiene | Satisfied | 256 | 65.0 |
Dissatisfied | 138 | 35.0 |
Information about newborn care | Satisfied | 260 | 66.0 |
Dissatisfied | 134 | 34.0 |
Information about asked consent before the procedure | Satisfied | 320 | 81.2 |
Dissatisfied | 74 | 18.8 |
3.5. Immediate Postnatal Care Maternal Satisfaction Related to Health Facility Structure
The results of this study showed that 306 (77.7%) of the respondents were satisfied with the cleanliness of the delivery room. Among 394 mothers 300 (76.1%) and 320(81.2%) of them were satisfied with getting prescribed drugs, and laboratory tests in the health facilities respectively. Concerning the availability and cleanliness of toilets less than half, 207(52.5%) of the mothers was satisfied with it (see
Table 6).
This also supported by the results of the qualitative study, women who didn`t get a clean toilet, clean delivery ward, and clean linen were less satisfied with immediate postnatal care. This was narrated:
“… The toilet has water and it was clean, cleaned daily, the postnatal room was also cleaned, and had no bad smell and not soaked with blood, that postnatal room is so good. Some beds of mom’s have linen and night cloth, and mothers who came empty-handed were not exposed to cold. Some…” (WR10, 30 years old).
“…I arrived at this hospital as soon as my labor began. I was subsequently brought to the labor room, but I was slept there as my house. The hospital has linen and blanket at that time. It's good if it gets better always.” (WR2, 28 years old).
“There is water at that day; the postnatal room was cleaned. Bath room was also cleaned ….” (WR4, 27 years old).
Table 6. Structural related women satisfaction with immediate postnatal care among women who gave birth in public hospitals, South West Shoa Zone, Ethiopia, 2023 (n=394).
Variables | Variable Category | Frequency | Percent |
Cleanliness of delivery room | Satisfied | 306 | 77.7 |
Dissatisfied | 88 | 22.3 |
Getting prescribed drugs and supplies | Satisfied | 300 | 76.1 |
Dissatisfied | 94 | 23.9 |
Getting laboratory test | Satisfied | 320 | 81.2 |
Dissatisfied | 74 | 18.8 |
Cleanliness of bed | Satisfied | 315 | 79.9 |
Dissatisfied | 79 | 20.1 |
Availability and Cleanliness of Bathroom | Satisfied | 311 | 78.9 |
Dissatisfied | 83 | 21.1 |
Availability and Cleanliness of toilet | Satisfied | 207 | 52.5 |
Dissatisfied | 187 | 47.5 |
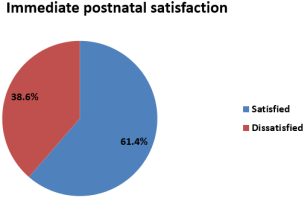
3.6. Over Immediate Postnatal Care Maternal Satisfaction
The finding of this study revealed that the overall immediate postnatal care women satisfaction was 242 (61.4%) [95% CI: 57-66] (See
Figure 2).
Figure 2. Pie chart showed that the overall satisfaction of women with immediate postnatal care among women who gave birth in public hospitals, South West Shoa Zone, Ethiopia, 2023.
3.7. Factors Associated with Immediate Postnatal Care Women Satisfaction
According to this study marital status, educational status, occupational status, labour duration, maternal outcome, fetal outcome, parity, mode of delivery, status of current pregnancy, ANC follow up, birth plan and breastfeeding were identified as candidate variables for multivariable logistic regression analysis. After controlling possible confounding variables by multivariable logistic analysis, labour duration, maternal outcome, birth plan and breast feeding were significantly associated with immediate postnatal care women satisfaction at a p-value <0.05(see
Table 7).
The finding of this study revealed that women who planned their birth were 2.02 times more likely satisfied with immediate postnatal care compared to women who not planned their birth (AOR=2.02(95% CI:1.16-3.51)). Women whose labour persist for 12 hours and less were 1.73 times more likely satisfied with immediate postnatal care compared to women whose labour persist more than 12 hours (AOR=1.73 (95% CI: 1.09-2.76). This was also supported by qualitative study. “… The midwives were stayed with me after I gave birth; they come quickly when I called them to help me. Also, I labored for a long time (one and half days), the way I gave birth was very disgusting [dissatisfied]. Why health professional serves mothers like this good” (WR2, 26 years old).
In addition, respondents who were normal during immediate postnatal period were 2.42 times more likely satisfied with immediate postnatal care compared to mothers who had complications during immediate postnatal period (AOR = 2.42 (95%CI: 1.15-5.1). This was also supported by qualitative study. “…They [health care providers] treat me anything when pain suffered me, they. Finally, they saw that my reproductive organ [perineal] was lacerated when I gave birth …this made me happy to give birth at this hospital, but they helped me more” (WR12, 23 years old).
Women who started breast feeding of their newborn within one hour were 1.86 times more likely satisfied with immediate postnatal care compared to women who were started breast feeding of their newborn after one hour (AOR = 1.86 (95%CI: 1.12-3.11). This was also supported by qualitative study. “…I got discomfort after I gave my baby. I asked one health profession to feed my newborn my breast. She was not refused me by saying she will feed by herself gave your breast frequently. So, my baby start feeding within hours. For other women its good if assistance continues like this while stayed in hospital” (WR11, 24 years old).
“After I gave birth by reproductive organ (spontaneous vagina delivery) my baby was couldn`t feed my breast timely. I bored with that situation. but they help.” (WR5, 18 years old).
Table 7. Multivariable logistics regression analysis for women satisfaction with immediate postnatal care among women who gave birth in public hospitals, South West Shoa, Ethiopia, 2023 (n=394).
Variables | Variables Category | Satisfaction | P-value | AOR 95% CI | P-value | AOR 95% CI |
Satisfied N(%) | Dissatisfied N(%) |
Marital status | Unmarried | 27(77.1%) | 8(22.9%) | 0.05 | 2.26(1-5.115) | 0.06 | 2.32(0.96-5.61) |
Married | 215(59.9%) | 144(40.1%) | | 1 | | 1 |
Occupational status | Housewife | 71(72.4%) | 27(27.6%) | 0.186 | 1.56(0.8-3.04) | 0.207 | 1.6(0.77-3.33) |
Farmer | 59(66.3%) | 30(33.7%) | 0.641 | 1.17(0.6-2.27) | 0.610 | 1.21(0.58-2.5) |
Merchant | 44(50.6%) | 43(49.1%) | 0.135 | 0.61(0.32-1.17) | 0.263 | 0.67(0.33-1.35) |
Gov`t employee | 26(49.1%) | 27(50.9%) | 0.136 | 0.57(0.28-1.19) | 0.421 | 0.71(0.31-1.63) |
Self-Employee | 42(62.7%) | 25(37.3%) | | 1 | | 1 |
Parity | Primiparous | 110(66.3%) | 56(33.7%) | 0.092 | 1.43(0.94-2.16) | 0.056 | 1.62(0.99-2.67) |
Multiparous | 132(57.9%) | 96(42.1%) | | 1 | | 1 |
Birth plan | Planned | 208(64.6%) | 114(35.4%) | 0.007 | 2.04(1.22-3.42) | 0.012* | 2.02(1.16-3.51) |
Unplanned | 34(47.2%) | 38(52.8%) | | 1 | | 1 |
Labour duration |  12 hour 12 hour
| 140(68%) | 66(32%) | 0.005 | 1.79(1.19-2.69) | 0.02* | 1.73(1.09-2.76) |
>12 hour | 102(54.3%) | 86(45.7%) | | 1 | | 1 |
Maternal outcome | Without complication | 228(64%) | 128(36%) | 0.002 | 3.05(1.53-6.11) | 0.02* | 2.42(1.15-5.1) |
With complication | 14(36.8%) | 24(63.2%) | | 1 | | 1 |
Fetal outcome | Normal | 191(65.9%) | 99(34.1%) | 0.003 | 2(1.27-3.16) | 0.073 | 1.57(0.95-2.59) |
With complication | 51(49.0%) | 53(51.0%) | | 1 | | 1 |
Breast feeding | within first hour | 198(64.9%) | 107(35.1%) | 0.009 | 1.89(1.17-3.05) | 0.017* | 1.86(1.12-3.11) |
after first hour | 44(49.4%) | 45(50.6%) | | 1 | | 1 |
Key: *= statistically significant,1= Reference COR= Crude odd ratio, AOR= Adjusted odd ratio, CI= confidence interval
4. Discussion
Women’s satisfaction with immediate postnatal care serves as a key indicator of the quality of healthcare services and overall service delivery. This study was conducted to evaluate the level of women’s satisfaction with immediate postnatal care in selected public hospitals of South West Shoa. The findings revealed that 61.4% of women were satisfied with the care they received (95% CI: 57%–66%).
This study was in line with the study conducted in Awi Zone, Ethiopia 63%
| [20] | Adane D, Wassihun B. Client satisfaction with existing postnatal care and associated factors : A study among mothers in Awi Zone, Amhara region, Ethiopia. Published online 2020.
https://doi.org/10.1177/1745506520976017 |
[20]
, Debre Markos Town, Northwest Ethiopia, 60.9%
| [21] | Bekele SB. Immediate Postnatal Care Satisfaction and Associated Factors Among Postnatal Women in Public Health Facilities at Debre Markos Town,. Published online 2022: 137-147. |
[21]
, and West Shewa zone, Central Ethiopia 60.8%
| [38] | Bulto GA, Demissie DB, Tasu TL, Demisse GA. Mother’s satisfaction with the existing labor and delivery care services at public health facilities in West Shewa zone, Oromia region, Ethiopia. BMC Pregnancy Childbirth. 2020; 20(1): 1-12.
https://doi.org/10.1186/s12884-020-02998-6 |
[38]
. The similarity in findings may be attributed to comparable study designs and settings, as all were facility-based cross-sectional studies conducted at hospital level.
Nevertheless, the finding of this study was higher than the study done in Zambia 26.2%
| [19] | Zulu M, Chanda D. IMothers’ satisfaction with immediate postnatal care provided at ndola central hospital, zambia. 2019;(December 2017). |
[19]
. This discrepancy could be explained by differences in study settings and the socio-cultural characteristics of the study populations. Additionally, variations in the year of study and sampling techniques may have contributed to the difference. The Zambian study was conducted several years earlier and used a purposive sampling method, which may have underestimated the true level of satisfaction, whereas the current study employed a random sampling technique, potentially providing a more representative estimate.
Accordingly, this study was also higher than the study done at Alexandria Government, Egypt 51.9%
| [18] | El MM, Ahmed A, Hables RM, Mohamed SH. Women Satisfaction Regarding Utilization of Post Natal Care in Alexandria Government. 2020; 7(3): 625-635. |
[18]
. This difference may be attributed to variations in study settings and women’s expectations of healthcare services. For instance, mothers in Egypt may have higher expectations for standardized and comprehensive care, which could influence their level of satisfaction.
The result of this study was higher than the study carried out in Haramaya District, Eastern Ethiopia 22.6%
| [39] | Kifle D, Azale T, Gelaw YA, Melsew YA. Maternal health care service seeking behaviors and associated factors among women in rural Haramaya District, Eastern Ethiopia: a triangulated community-based cross-sectional study. Reprod Health. 2017; 14(1): 1-11. https://doi.org/10.1186/s12978-016-0270-5 |
[39]
. This discrepancy could be due to differences in the types of health facilities included in the studies. The current study was conducted in hospital settings, where relatively better resources and services may be available, whereas the study in Haramaya District was conducted at the district level, where health facilities may be less equipped to meet women’s expectations.
On the contrary, this study was lower than the study conducted in Spain 94.54%
| [17] | Mahía LP, López SB, Pillado TS, Díaz SP. Women ’ s satisfaction with childbirth and postpartum care and associated variables. Published online 2021: 1-7. |
[17]
. This variation may be explained by differences in healthcare systems and resource availability between developing and developed countries. Facilities in Spain are more likely to provide high-quality, standardized care that meets women’s expectations during the immediate postnatal period. Additionally, differences in study populations and socio-cultural contexts may also contribute to the observed variation.
Similarly, the finding of this study was lower than the study conducted in Wolaita Sodo University teaching and referral hospital in Ethiopia, 67.3%
| [10] | Wolka S, Assegid S, Tantu T, Gunta M, Duko B. Determinants of Maternal Satisfaction with Existing Delivery Care at Wolaita Sodo University Teaching and Referral. 2020; 2020. |
[10]
. The observed difference may be attributed to variations in study settings. Women who delivered at a specialized referral hospital may receive more comprehensive and higher-quality services that better meet their expectations during the immediate postnatal period. Additionally, differences in infrastructure such as the availability of clean delivery wards, water supply, and essential medical equipment may contribute to higher satisfaction levels. Improvements in hospital services over time could also play a role in fulfilling women’s expectations.
This study found that women who were normal during the immediate postnatal period were more likely to be satisfied with immediate postnatal care. The qualitative study also supports this finding, women who delivered without complications were very happy with immediate postnatal. It is similar to a study conducted in Awi Zone hospitals, Ethiopia
| [20] | Adane D, Wassihun B. Client satisfaction with existing postnatal care and associated factors : A study among mothers in Awi Zone, Amhara region, Ethiopia. Published online 2020.
https://doi.org/10.1177/1745506520976017 |
[20]
. A possible explanation is that women without complications are more likely to have positive birth experiences, which enhances their overall satisfaction. In contrast, women who experience complications may attribute their condition to the quality of care received, leading to dissatisfaction and reduced trust in healthcare providers.
The present study revealed that mothers whose labour persists for 12 hours and less were more likely satisfied with immediate postnatal care compared with women whose labour persisted for >12 hours. This was supported by the results of the qualitative study; mothers who were laboring for a long time were dissatisfied with immediate postnatal care. This was similar to the previous study conducted in Wolaita Sodo University Teaching and Referral Hospital, Ethiopia
| [10] | Wolka S, Assegid S, Tantu T, Gunta M, Duko B. Determinants of Maternal Satisfaction with Existing Delivery Care at Wolaita Sodo University Teaching and Referral. 2020; 2020. |
[10]
and in Nekemte Specialized Hospital in Western Ethiopia
| [22] | Babure ZK, Assefa JF, Weldemarium TD. Maternal Satisfaction and Associated Factors towards Delivery Service among Mothers Who Gave Birth at Nekemte Specialized Hospital, Nekemte Town, East Wollega Zone, Oromia Regional State, Western Ethiopia, 2019 : A Cross- sectional Study Design Journ. Published online 2019: 1-11.
https://doi.org/10.35248/2167-0420.20.9.489.Copyright |
[22]
. This may be because prolonged labor can be physically exhausting and emotionally stressful, often involving repeated clinical procedures and increased anxiety about delivery outcomes, thereby reducing satisfaction. Additionally, women may expect shorter labor durations after arriving at a health facility; when this expectation is not met, dissatisfaction may arise.
Furthermore, the finding of this study showed that birth plan had a positive association with women satisfaction with immediate postnatal care. Women who were plan their birth were happier with immediate postnatal care than women didn`t plan their birth. This was similar with study conducted in Spain
| [17] | Mahía LP, López SB, Pillado TS, Díaz SP. Women ’ s satisfaction with childbirth and postpartum care and associated variables. Published online 2021: 1-7. |
[17]
. A possible explanation is that birth planning enhances preparedness, promotes better self-care, and reduces unexpected complications, thereby improving the overall childbirth experience and satisfaction.
Similarly, women who started breast feeding of their newborn within one hour were more likely satisfied with immediate postnatal care compared to women who were started breast feeding of their newborn after one hour. The qualitative study supports this finding, women who were started feeding of their newborn was happier with immediate postnatal care. This was similar with study conducted in Greek
, in Mashhad, Iran
| [15] | Mirzaii K, Ghadikolaee SO, Bazzaz MM, Ziaee M. Mother ’ s satisfaction of postpartum care and its relationship with midwifery care at Urban Health Centers, Mashhad, Iran. 2015; (Md). |
[15]
, and Porto Alegre, southern Brazil
| [41] | Francis A, Senna K De, Giugliani C, et al. Maternal satisfaction with breastfeeding in the first month postpartum and associated factors. Published online 2020: 1-11. |
[41]
. This association may be explained by the benefits of early skin-to-skin contact, which enhances maternal–infant bonding, stimulates hormonal responses, improves breastfeeding practices, and reduces postnatal complications. Additionally, mothers who initiate breastfeeding early may perceive that they and their newborn received attentive and high-quality care from healthcare providers, thereby increasing their satisfaction.
5. Strengths
This study has several important strengths it employed a mixed-methods approach, combining both quantitative and qualitative data, which provided a more comprehensive understanding of women’s satisfaction with immediate postnatal care. The qualitative findings complemented the quantitative results by exploring women’s experiences, expectations, and perceptions in greater depth. The study used a relatively large sample size with a high response rate (97.77%), which enhances the reliability and generalizability of the findings within similar settings. The use of random sampling techniques minimized selection bias and improved the representativeness of the study population. Additionally, the inclusion of multiple public hospitals increased the external validity of the study.
6. Limitations
Despite these strengths, the study has some limitations. The cross-sectional nature of the study limits the ability to establish causal relationships between independent variables and women’s satisfaction. Second, since the data were collected through interviewer-administered questionnaires, there is a possibility of social desirability bias, where participants may have over reported their level of satisfaction and a low sample size for the qualitative study. The study was conducted in public hospitals only, which may limit the generalizability of the findings to private health facilities or other settings. Furthermore, recall bias might have occurred, as mothers were asked to report their experiences shortly after delivery.
7. Conclusion
The result of current study was concluded that more than half of women were satisfied with immediate postnatal care. Women’s satisfaction was significantly associated with having a birth plan, shorter duration of labor (≤12 hours), absence of complications during the immediate postnatal period, and early initiation of breastfeeding within one hour. These findings emphasize the importance of promoting birth preparedness, improving labor management, and encouraging early breastfeeding practices to enhance maternal satisfaction.
However, barriers such as inadequate care provision, insufficient information and counseling, poor cleanliness and infrastructure, and shortages of laboratory services, drugs, and medical supplies negatively affected women’s satisfaction.
8. Recommendation
Based on the findings of the current study, the following recommendations are forwarded to relevant stakeholders to improve women’s satisfaction with immediate postnatal care, thereby enhancing institutional childbirth services:
For Health Facility (Hospital) Managers:
1) Ensure cleanliness of delivery wards and provide adequate linen for women who deliver at the facility.
2) Maintain a reliable supply of essential drugs, water, and medical equipment to improve the quality of care.
3) Strengthen immediate postnatal care services to meet women’s expectations and enhance satisfaction.
For Healthcare Providers:
1) Work to prevent and manage maternal complications effectively to improve women’s satisfaction with postnatal care.
2) Closely monitor laboring mothers and provide timely interventions for prolonged labor.
3) Support and encourage early initiation of breastfeeding within the first hour after birth.
For Women:
Plan their birth in advance to enhance preparedness and increase the likelihood of a positive postnatal care experience.
For Researchers:
Conduct in-depth qualitative studies, including focus group discussions with both mothers and their partners, to better understand the factors influencing immediate postnatal care satisfaction and guide targeted interventions.
Author Contributions
Bacha Merga Chuko: Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing
Zufela Sime: Investigation, Methodology, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing, Formal Analysis
Fikru Assefa: Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing
Gada Edea: Investigation, Methodology, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing
Tilahun Fufa Debela: Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing
Nebiyu Taye: Investigation, Methodology, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing, Formal Analysis
Derara Kebata: Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing
Funding
The authors declare that no financial support was received for the study, authorship, and/or publication of this article.
Data Availability Statement
The original contributions presented in the study were included in the articles. Material; further inquiries can be directed to the corresponding author based upon reasonable request.
Conflicts of Interest
The authors declare that the study was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
| [1] |
Health M. Observation of mother and baby in the immediate postnatal period : consensus statements guiding practice. 2012; (July): 1-4.
|
| [2] |
Tsegaye B, Amare B, Reda M. Prevalence and Factors Associated with Immediate Postnatal Care Utilization in Ethiopia : Analysis of Ethiopian Demographic Health Survey 2016 Prevalence and Factors Associated with Immediate Postnatal Care Utilization in Ethiopia : Analysis of Ethiopian. Published online 2022.
https://doi.org/10.2147/IJWH.S294058
|
| [3] |
Postnatal care of the mother and newborn 2013. Published online 2013.
|
| [4] |
Okonofua F, Ogu R, Agholor K, Okike O, Abdus-salam R, Gana M. Qualitative assessment of women ’ s satisfaction with maternal health care in referral hospitals in Nigeria. Published online 2017: 1-8.
https://doi.org/10.1186/s12978-017-0305-6
|
| [5] |
Ilesanmi RE, Akinmeye JA. Evaluation of the quality of postnatal care and mothers ’ satisfaction at the university college hospital Ibadan, Nigeria. 2018; 10(September): 99-108.
https://doi.org/10.5897/IJNM2018.0314
|
| [6] |
Mehata S, Paudel YR, Dariang M, et al. Factors determining satisfaction among facility-based maternity clients in Nepal. Published online 2017: 1-10.
https://doi.org/10.1186/s12884-017-1532-0
|
| [7] |
Lazzerini M, Mariani I, Semenzato C, Valente EP. Association between maternal satisfaction and other indicators of quality of care at childbirth : a cross- sectional study based on the WHO standards. Published online 2020.
https://doi.org/10.1136/bmjopen-2020-037063
|
| [8] |
Guideline N. Postnatal care Guideline 2022; (64).
www.nice.org.uk/guidance/ng194
|
| [9] |
Battawi JAA, Hafiz SK. Evaluation of Postnatal Mother ’ s Satisfaction with Nursing Care In El-Shatby Maternity University Hospital. 2017; 6(6): 69-80.
https://doi.org/10.9790/1959-0606026980
|
| [10] |
Wolka S, Assegid S, Tantu T, Gunta M, Duko B. Determinants of Maternal Satisfaction with Existing Delivery Care at Wolaita Sodo University Teaching and Referral. 2020; 2020.
|
| [11] |
WHO. Maternal mortality Evidence brief. 2017; (1): 1-4.
|
| [12] |
WHO, Group WB. Trends in Maternal Mortality : 1990 to 2015. Published online 2015.
|
| [13] |
Geller SE, Koch AR, Garland CE, MacDonald EJ, Storey F, Lawton B. A global view of severe maternal morbidity: Moving beyond maternal mortality. Reprod Health. 2018; 15 (Suppl 1).
https://doi.org/10.1186/s12978-018-0527-2
|
| [14] |
Demographic M, Survey H. Ethiopia.; 2019.
|
| [15] |
Mirzaii K, Ghadikolaee SO, Bazzaz MM, Ziaee M. Mother ’ s satisfaction of postpartum care and its relationship with midwifery care at Urban Health Centers, Mashhad, Iran. 2015; (Md).
|
| [16] |
Jha P, Larsson M, Christensson K, Svanberg AS. Satisfaction with childbirth services provided in public health facilities: Results from a cross-sectional survey among postnatal women in Chhattisgarh, India. Glob Health Action. 2017; 10(1).
https://doi.org/10.1080/16549716.2017.1386932
|
| [17] |
Mahía LP, López SB, Pillado TS, Díaz SP. Women ’ s satisfaction with childbirth and postpartum care and associated variables. Published online 2021: 1-7.
|
| [18] |
El MM, Ahmed A, Hables RM, Mohamed SH. Women Satisfaction Regarding Utilization of Post Natal Care in Alexandria Government. 2020; 7(3): 625-635.
|
| [19] |
Zulu M, Chanda D. IMothers’ satisfaction with immediate postnatal care provided at ndola central hospital, zambia. 2019;(December 2017).
|
| [20] |
Adane D, Wassihun B. Client satisfaction with existing postnatal care and associated factors : A study among mothers in Awi Zone, Amhara region, Ethiopia. Published online 2020.
https://doi.org/10.1177/1745506520976017
|
| [21] |
Bekele SB. Immediate Postnatal Care Satisfaction and Associated Factors Among Postnatal Women in Public Health Facilities at Debre Markos Town,. Published online 2022: 137-147.
|
| [22] |
Babure ZK, Assefa JF, Weldemarium TD. Maternal Satisfaction and Associated Factors towards Delivery Service among Mothers Who Gave Birth at Nekemte Specialized Hospital, Nekemte Town, East Wollega Zone, Oromia Regional State, Western Ethiopia, 2019 : A Cross- sectional Study Design Journ. Published online 2019: 1-11.
https://doi.org/10.35248/2167-0420.20.9.489.Copyright
|
| [23] |
Abebe A, Menta AA. Nutrition and Dietetic Practice Mothers ’ Satisfaction with Institutional Delivery Service and Associated Factors among Women Attending Hospitals in. 2018; 2(2): 1-12.
|
| [24] |
Asres GD. Satisfaction and Associated Factors among Mothers Delivered at Asrade Zewude Memorial Primary Hospital, Bure, West Gojjam, Amhara, Ethiopia: A Cross Sectional Study. Prim Heal Care Open Access. 2018; 08(02).
https://doi.org/10.4172/2167-1079.1000293
|
| [25] |
Bishaw KA, Temesgen H, Amha H, et al. A systematic review and meta-analysis of women’s satisfaction with skilled delivery care and the associated factors in Ethiopia. SAGE Open Med. 2022; 10: 205031212110682.
https://doi.org/10.1177/20503121211068249
|
| [26] |
Mocumbi S, Högberg U, Lampa E, et al. Mothers ’ satisfaction with care during facility-based childbirth : a cross-sectional survey in southern Mozambique. 2019; 6: 1-14.
|
| [27] |
Berhe H. Status of Caring, Respectful and Compassionate Health Care Practice in Tigrai Regional State : Patients ’ Perspective. 2017; 10(3): 1118-1128.
|
| [28] |
Obsa MS. Maternal satisfaction towards childbirth Service in Public Health Facilities at Adama. Published online 2020: 4-11.
|
| [29] |
Zemenu Yohannes Kassa TA. Maternal Satisfaction and Associated Factors on Delivery Care Service in Gynecology & Obstetrics Maternal Satisfaction and Associated Factors on Delivery Care Service in. 2018; (February 2019).
https://doi.org/10.4172/2161-0932.1000473
|
| [30] |
Dar B. Compassionate and respectful maternity care during facility based child birth and women ’ s intent to use maternity service in. Published online 2018: 1-9.
|
| [31] |
Makuka, MD GJ, Sango, MD MM, Mashambo, MD AE, Mashambo, MD AE, Msuya, MD, PhD SE, Mtweve, MD, MSc SP. Clients’ Perspectives on Quality of Delivery Services in a Rural Setting in Tanzania: Findings from a Qualitative Action-Oriented Research. Int J Matern Child Heal AIDS. 2017; 6(1): 60-68.
https://doi.org/10.21106/ijma.191
|
| [32] |
Zone H, Delibo D, Damena M, Gobena T, Balcha B. Status of Home Delivery and Its Associated Factors among Women Who Gave Birth within the Last 12 Months in East Badawacho. 2020; 2020.
|
| [33] |
Ngowi AF, Kamazima SR, Kibusi S, Gesase A, Bali T. Women’s determinant factors for preferred place of delivery in Dodoma region Tanzania: A cross sectional study. Reprod Health. 2017; 14(1): 1-8.
https://doi.org/10.1186/s12978-017-0373-7
|
| [34] |
Kifle MM, Kesete HF, Gaim HT, Angosom GS, Araya MB. Health facility or home delivery ? Factors influencing the choice of delivery place among mothers living in rural communities of Eritrea. 2018; 1: 1-15.
|
| [35] |
Sacks E, Masvawure TB, Atuyambe LM, Neema S. Postnatal Care Experiences and Barriers to Care Utilization for Home- and Facility-Delivered Newborns in Uganda. Matern Child Health J. Published online 2016.
https://doi.org/10.1007/s10995-016-2144-4
|
| [36] |
Federal Democratic Republic of Ethiopia Ministry of Health. Health Sector Transformation Plan II 2020/21-2024/25 (2013EFY-2017EFY). 2021; 25(February).
|
| [37] |
Adnan FI, Mohd N, Id N, Akma N, Junoh M. Associated factors of labor satisfaction and predictor of postnatal satisfaction in the north-east of Peninsular Malaysia. Published online 2020: 1-19.
https://doi.org/10.1371/journal.pone.0238310
|
| [38] |
Bulto GA, Demissie DB, Tasu TL, Demisse GA. Mother’s satisfaction with the existing labor and delivery care services at public health facilities in West Shewa zone, Oromia region, Ethiopia. BMC Pregnancy Childbirth. 2020; 20(1): 1-12.
https://doi.org/10.1186/s12884-020-02998-6
|
| [39] |
Kifle D, Azale T, Gelaw YA, Melsew YA. Maternal health care service seeking behaviors and associated factors among women in rural Haramaya District, Eastern Ethiopia: a triangulated community-based cross-sectional study. Reprod Health. 2017; 14(1): 1-11.
https://doi.org/10.1186/s12978-016-0270-5
|
| [40] |
Panagopoulou V, Kalokairinou A, Tzavella F, Tziaferi S. A survey of Greek women’s satisfaction of postnatal care. AIMS Public Heal. 2018; 5(2): 158-172.
https://doi.org/10.3934/publichealth.2018.2.158
|
| [41] |
Francis A, Senna K De, Giugliani C, et al. Maternal satisfaction with breastfeeding in the first month postpartum and associated factors. Published online 2020: 1-11.
|
Cite This Article
-
APA Style
Chuko, B. M., Sime, Z., Assefa, F., Edea, G., Debela, T. F., et al. (2026). Women’s Satisfaction with Immediate Postnatal Care and Associated Factors Among Mothers Who Gave Birth at Public Hospital, in South West Shoa, Ethiopia, 2023:
Mixed-method Study. Rehabilitation Science, 11(1), 13-28. https://doi.org/10.11648/j.rs.20261101.12
 Copy
|
Copy
|
 Download
Download
ACS Style
Chuko, B. M.; Sime, Z.; Assefa, F.; Edea, G.; Debela, T. F., et al. Women’s Satisfaction with Immediate Postnatal Care and Associated Factors Among Mothers Who Gave Birth at Public Hospital, in South West Shoa, Ethiopia, 2023:
Mixed-method Study. Rehabil. Sci. 2026, 11(1), 13-28. doi: 10.11648/j.rs.20261101.12
Copy
|
Download
AMA Style
Chuko BM, Sime Z, Assefa F, Edea G, Debela TF, et al. Women’s Satisfaction with Immediate Postnatal Care and Associated Factors Among Mothers Who Gave Birth at Public Hospital, in South West Shoa, Ethiopia, 2023:
Mixed-method Study. Rehabil Sci. 2026;11(1):13-28. doi: 10.11648/j.rs.20261101.12
Copy
|
Download
-
@article{10.11648/j.rs.20261101.12,
author = {Bacha Merga Chuko and Zufela Sime and Fikru Assefa and Gada Edea and Tilahun Fufa Debela and Nebiyu Taye and Derara Kebata},
title = {Women’s Satisfaction with Immediate Postnatal Care and Associated Factors Among Mothers Who Gave Birth at Public Hospital, in South West Shoa, Ethiopia, 2023:
Mixed-method Study},
journal = {Rehabilitation Science},
volume = {11},
number = {1},
pages = {13-28},
doi = {10.11648/j.rs.20261101.12},
url = {https://doi.org/10.11648/j.rs.20261101.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.rs.20261101.12},
abstract = {Background: The first 24 hours following delivery are referred to as the immediate postnatal phase. The first 24 hours following birth account for a significant fraction of mother and newborn fatalities. Regardless of the circumstances surrounding their delivery, providing prompt postnatal care lowers maternal and newborn mortality and morbidity. There was limited evidence on immediate postnatal maternal satisfaction among mothers who gave birth in public hospitals in South West Shoa. Therefore, this study was conducted using a mixed-methods approach to assess maternal satisfaction with immediate postnatal care and to explore underlying factors influencing their experiences. Objectives: To assess women`s satisfaction with immediate postnatal care and associated factors among mothers who gave birth at Public Hospital, in South West Shoa, Ethiopia, 2023. Methods: A facility-based, cross-sectional study design supplemented by a qualitative study / convergent study design/ was conducted among 403 mothers for the quantitative study and 17 women for the qualitative study. Purposive and systematic sampling methods technique was used to select study participants for the qualitative and quantitative study, respectively. EpiData version 3.1 was used for data entry, then exported to statistical package for social science. Multivariable logistic regression models were used for study variables with p-values less than 0.25. In the multivariable model, the adjusted odds ratio and its 95% confidence interval were calculated, and a p-value of less than 0.05 was deemed statistically significant. Thematic analysis was used to examine qualitative data. Graphs, tables, and text were used to display the results. Results: A total of 403 participants were recruited for the study, of whom 394 mothers completed the interview, yielding a response rate of 97.77%. The overall proportion of women satisfied with immediate postnatal care was 242 (61.4%) [95% CI: 57%–66%]. Birth plan (AOR = 2.02; 95% CI: 1.16–3.51). Labor duration (AOR = 1.73; 95% CI: 1.09–2.76). Women who experienced complications (AOR = 2.42; 95% CI: 1.15–5.10), and initiating breastfeeding (AOR = 1.86; 95% CI: 1.12–3.11). Conclusion and Recommendation: Over 50% of women expressed satisfaction with the immediate postnatal care they received. Managers of healthcare institutions and medical professionals collaborate closely to increase postpartum mom satisfaction.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Women’s Satisfaction with Immediate Postnatal Care and Associated Factors Among Mothers Who Gave Birth at Public Hospital, in South West Shoa, Ethiopia, 2023:
Mixed-method Study
AU - Bacha Merga Chuko
AU - Zufela Sime
AU - Fikru Assefa
AU - Gada Edea
AU - Tilahun Fufa Debela
AU - Nebiyu Taye
AU - Derara Kebata
Y1 - 2026/06/10
PY - 2026
N1 - https://doi.org/10.11648/j.rs.20261101.12
DO - 10.11648/j.rs.20261101.12
T2 - Rehabilitation Science
JF - Rehabilitation Science
JO - Rehabilitation Science
SP - 13
EP - 28
PB - Science Publishing Group
SN - 2637-594X
UR - https://doi.org/10.11648/j.rs.20261101.12
AB - Background: The first 24 hours following delivery are referred to as the immediate postnatal phase. The first 24 hours following birth account for a significant fraction of mother and newborn fatalities. Regardless of the circumstances surrounding their delivery, providing prompt postnatal care lowers maternal and newborn mortality and morbidity. There was limited evidence on immediate postnatal maternal satisfaction among mothers who gave birth in public hospitals in South West Shoa. Therefore, this study was conducted using a mixed-methods approach to assess maternal satisfaction with immediate postnatal care and to explore underlying factors influencing their experiences. Objectives: To assess women`s satisfaction with immediate postnatal care and associated factors among mothers who gave birth at Public Hospital, in South West Shoa, Ethiopia, 2023. Methods: A facility-based, cross-sectional study design supplemented by a qualitative study / convergent study design/ was conducted among 403 mothers for the quantitative study and 17 women for the qualitative study. Purposive and systematic sampling methods technique was used to select study participants for the qualitative and quantitative study, respectively. EpiData version 3.1 was used for data entry, then exported to statistical package for social science. Multivariable logistic regression models were used for study variables with p-values less than 0.25. In the multivariable model, the adjusted odds ratio and its 95% confidence interval were calculated, and a p-value of less than 0.05 was deemed statistically significant. Thematic analysis was used to examine qualitative data. Graphs, tables, and text were used to display the results. Results: A total of 403 participants were recruited for the study, of whom 394 mothers completed the interview, yielding a response rate of 97.77%. The overall proportion of women satisfied with immediate postnatal care was 242 (61.4%) [95% CI: 57%–66%]. Birth plan (AOR = 2.02; 95% CI: 1.16–3.51). Labor duration (AOR = 1.73; 95% CI: 1.09–2.76). Women who experienced complications (AOR = 2.42; 95% CI: 1.15–5.10), and initiating breastfeeding (AOR = 1.86; 95% CI: 1.12–3.11). Conclusion and Recommendation: Over 50% of women expressed satisfaction with the immediate postnatal care they received. Managers of healthcare institutions and medical professionals collaborate closely to increase postpartum mom satisfaction.
VL - 11
IS - 1
ER -
Copy
|
Download