Abstract
Sexual and reproductive health rights (SRHRs) are fundamental human rights that underpin gender equality, health, and sustainable development, yet violations remain widespread among women in many low- and middle-income settings due to entrenched socio-cultural norms, gender inequality, and unequal power relations within marriage. This study assessed both the violations and the exercise of SRHRs among ever-married women in Ibadan metropolis, Nigeria, using a community-based cross-sectional mixed-methods design. A total of 423 ever-married women aged 15–49 years were selected through multistage sampling from two Local Government Areas, with quantitative data collected via semi-structured interviewer-administered questionnaires and qualitative insights obtained from five focus group discussions; quantitative data were analysed using descriptive statistics and logistic regression, while qualitative data were subjected to thematic analysis. Overall, 25.1% of respondents reported experiencing violations of SRHRs, with the most common being violations of the right to freedom from sexual violence (29.3%), and husbands identified as the primary perpetrators (38.7%). Despite this, 90.1% of respondents reported exercising at least one SRHR, most commonly the right to marriage (27.9%) and the right to family planning (25.1%), and among those who experienced violations, 57.5% reported taking some form of action against the violation, the perpetrator, or both. Qualitative findings further highlighted intimate partner violence, coercive childbearing, and socio-cultural expectations as key drivers of SRHR violations. These findings indicate that SRHR violations remain prevalent among married women in Ibadan, underscoring the need to strengthen awareness, legal protections, and community support mechanisms to enhance women’s capacity to exercise their sexual and reproductive health rights.
|
Published in
|
European Journal of Preventive Medicine (Volume 14, Issue 2)
|
|
DOI
|
10.11648/j.ejpm.20261402.12
|
|
Page(s)
|
25-33 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2026. Published by Science Publishing Group
|
Keywords
Sexual and Reproductive Health Rights, Gender-Based Violence, Married Women, Reproductive Autonomy, Nigeria
1. Introduction
Sexual and reproductive health rights (SRHRs) are an essential component of the universal human right to the highest attainable standard of health. These rights encompass access to reproductive health services, autonomy in reproductive decision-making, and protection from discrimination, coercion, and violence. They are grounded in broader human rights principles, including equality, non-discrimination, privacy, bodily autonomy, access to information, and the right to seek redress when rights are violated
| [1] | Amnesty International USA: Sexual and Reproductive Health Rights. What is sexual and reproductive health? 2015. |
| [2] | World Health Organization: WHO working definition. Geneva; 2010. |
[1, 2]
.
The global recognition of SRHRs was strengthened during the International Conference on Population and Development (ICPD) held in Cairo in 1994, which marked a shift toward a rights-based approach to reproductive health emphasising gender equality, reproductive autonomy, and individual dignity
| [3] | Guttmacher Institute: A Time to Lead: A Roadmap for Progress on Sexual and Reproductive Health and Rights Worldwide. 2018. |
[3]
. Since then, SRHRs have become central to global development priorities, particularly within the Sustainable Development Goals (SDGs), which emphasise universal access to sexual and reproductive healthcare services and the elimination of gender-based violence
| [4] | International Planned Parenthood Federation: Sexual and reproductive health and rights are the key to gender equality and sustainable development | IPPF. 2015. |
[4]
.
Despite global commitments, violations of SRHRs remain widespread. The World Health Organisation estimates that approximately 30% of women globally have experienced physical or sexual violence by an intimate partner during their lifetime
| [5] | World Health Organization: Global and regional estimates of violence against women Prevalence and health effects of intimate partner violence and non-partner sexual violence. World Health Organization: Geneva; 2013. |
[5]
. In sub-Saharan Africa, the prevalence of intimate partner violence is estimated at approximately 44%
| [6] | Muluneh MD, Stulz V, Francis L, Agho K: Gender Based Violence against Women in Sub-Saharan Africa: A Systematic Review and Meta-Analysis of Cross-Sectional Studies. Int J Environ Res Public Health. 2020, 17: 903.
https://doi.org/10.3390/ijerph17030903 |
[6]
. Such violations often manifest in the form of forced marriage, denial of reproductive autonomy, gender-based violence, and harmful traditional practices such as female genital mutilation and early marriage
| [7] | United Nations Human Rights: Sexual and reproductive health and rights. 2015. |
[7]
.
Nigeria continues to face significant challenges in protecting women’s sexual and reproductive rights. Harmful cultural practices, gender inequality, and weak enforcement of protective laws contribute to violations of SRHRs among women of reproductive age
. National survey data indicate that approximately 36% of Nigerian women have experienced spousal violence, while female genital mutilation remains prevalent in several communities
| [9] | National Population Commission: Nigeria Demographic and Health Survey. 2019. |
[9]
. These violations have significant consequences for women’s physical, mental, and reproductive health.
Married women are particularly vulnerable to SRHR violations because patriarchal norms and unequal power dynamics often shape marital relationships. Cultural expectations and economic dependency may limit women’s ability to make independent reproductive decisions or seek help when violations occur
| [10] | World Health Organization: Promoting sexual and reproductive health for persons with disabilities. 2009. |
[10]
.
Although several studies in Nigeria have examined knowledge and perceptions of SRHRs among women
, limited research has focused on the actual exercise of these rights and women’s experiences of violations, particularly among married women at the community level. Understanding both the occurrence of violations and how women respond to them is essential for designing effective interventions that promote women’s autonomy and protect their reproductive rights.
This study, therefore, assessed the violation and exercise of sexual and reproductive health rights among ever-married women in Ibadan metropolis using a mixed-methods approach, providing new evidence on both the prevalence of SRHR violations and the strategies women employ to respond to them in a community setting.
2. Methods
2.1. Study Design
A community-based cross-sectional study using a mixed-methods approach (quantitative and qualitative components) was conducted to assess the violation and exercise of sexual and reproductive health rights among ever-married women of reproductive age.
2.2. Study Area
The study was conducted in Ibadan metropolis, Oyo State, southwestern Nigeria. Two Local Government Areas (LGAs) were selected for the study: Ibadan South-West and Ibadan North-East LGAs. These areas comprise both urban and peri-urban communities with diverse socioeconomic and cultural characteristics.
2.3. Study Population
The study population consisted of ever-married women aged 15–49 years residing in the selected communities within the study LGAs.
2.3.1. Inclusion Criteria
Women who had lived in the study area for at least six months before the study were eligible to participate.
2.3.2. Exclusion Criteria
Women who were severely ill or mentally incapacitated at the time of data collection and unable to provide reliable responses were excluded from the study.
2.4. Sample Size Determination
The minimum sample size (n = 423) was calculated using the Leslie Kish formula for single proportion:
Where:
Z = standard normal deviate at 95% confidence level (1.96)
p = estimated prevalence from a previous study in Ethiopia
| [12] | Adinew YM, Worku AG, Mengesha ZB: Knowledge of reproductive and sexual rights among University students in Ethiopia: institution-based cross-sectional. BMC Int Health Hum Rights. 2013, 13: 12. https://doi.org/10.1186/1472-698X-13-12 |
[12]
.
d = margin of error set at 5%
A 10% non-response rate was added to obtain the final sample size.
2.5. Sampling Technique
A multistage sampling technique was used to select respondents.
1) Two LGAs were selected from Ibadan metropolis.
2) Wards were selected within each LGA using simple random sampling.
3) Enumeration areas were selected from each ward.
4) Households were selected using systematic sampling.
5) Eligible ever-married women within selected households were recruited.
Where more than one eligible woman was present in a household, one respondent was selected using simple random sampling.
2.6. Data Collection
Data were collected using both quantitative and qualitative methods.
2.6.1. Quantitative Data
Quantitative data was collected using a semi-structured interviewer-administered questionnaire. The questionnaire included sections on:
1) socio-demographic characteristics (This have been reported previously in another study
, however, the present study focuses specifically on SRHR violations and their exercise.”).
2) experience of violation of SRHRs
3) exercise of SRHRs
4) actions taken following violations
2.6.2. Qualitative Data
Qualitative data were collected using Focus Group Discussions (FGDs).
Five FGD sessions were conducted among married women in the selected communities. Each FGD consisted of 8–10 participants and explored:
1) understanding of SRHR violations
2) personal or observed experiences of violations
3) strategies used by women to exercise their SRHRs
4) community responses to SRHR violations
5) suggestions for addressing SRHR violations in the community
FGDs were conducted in the local language and audio-recorded with participants’ consent.
2.7. Data Management and Analysis
2.7.1. Quantitative Analysis
Quantitative data were entered and analysed using statistical software.
Descriptive statistics were used to summarise variables, and results were presented using frequency tables and charts. Associations between categorical variables were assessed using the Chi-square test at a significance level of p < 0.05.
Binary logistic regression analysis was conducted for variables that were statistically significant at p < 0.10 in the bivariate analysis to identify predictors of the exercise of SRHRs.
2.7.2. Qualitative Analysis
Audio recordings from the FGDs were transcribed verbatim and analysed using a thematic framework approach. The transcripts were reviewed independently by the researcher, an analyst, and a field expert. Emerging themes related to experiences of SRHR violations, exercise of rights, and community responses were identified and organised into thematic categories.
2.7.3. Operational Definitions
Violation of SRHRs: Defined as a “Yes” response to the question: "Has any of your sexual and reproductive health rights ever been abused?"
Exercise of SRHRs: Engagement in actions reflecting autonomy in reproductive and sexual decision-making (e.g., use of family planning, choice of partner, access to services).
Response to SRHR violations: Defined as a “Took action” response to the question: "Have you ever taken any form of action against a violation of your SRHRs or against the abuser?"
2.8. Ethical Considerations
Ethical approval was obtained from the Oyo State Research Ethics Review Committee, Ministry of Health, Oyo State, prior to data collection.
Informed consent was obtained from all participants before participation in the study. Confidentiality and anonymity of respondents were maintained throughout the research process.
3. Results
3.1. Experience of Violation of Sexual and Reproductive Health Rights (Table 1) Approximately one-quarter of respondents (25.1%) reported having experienced at least one form of violation of their sexual and reproductive health rights (
Table 1), while the majority (74.9%) reported no experience of abuse.
Among those who experienced violations (n=106), the most frequently reported abuse was the right to freedom from sexual violence (29.3%). Other reported violations included abuse related to marital sexual relations, freedom from abuse, childcare, and family planning.
Husbands were identified as the most common perpetrators of SRHR violations (38.7%), followed by friends (29.2%), relatives (17.0%) and parents (7.5%).
3.2. Exercise of Sexual and Reproductive Health Rights (Table 2) The majority of respondents (90.1%) reported exercising at least one sexual and reproductive health right (
Table 2). The most commonly reported rights exercised were the right to marry a partner of choice (27.9%) and the right to use family planning (25.1%).
Respondents reported several ways in which these rights were exercised. The most frequently mentioned actions included marrying a partner of their choice, using family planning with spousal support, and taking responsibility for childcare. More than half of the respondents (56.0%) indicated that their cultural and religious beliefs supported women’s ability to exercise bodily control.
3.3. Exercise of SRHRs Following Violation (Table 3) Among respondents who reported experiencing violations of SRHRs (n = 106), half (50.0%) reported taking no action, while the remaining half took some form of action (
Table 3). A larger proportion (78.3%) did not take action directly against the perpetrator.
Overall, 57.5% of respondents who experienced violations reported exercising their SRHRs by taking action against the violation, the abuser, or both.
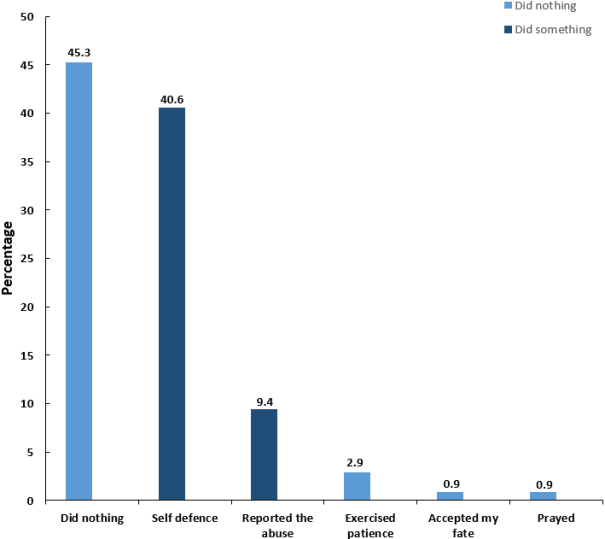
3.4. Patterns of Actions Taken Against Violations (Figure 1) While
Table 3 presents a binary classification of action taken,
Figure 1 further disaggregates the specific types of responses.” The most common response to violations of SRHRs was taking no action (45.3%), followed by self-defence (40.6%), reporting the abuse (9.4%), and other coping mechanisms, such as patience or prayer (
Figure 1).
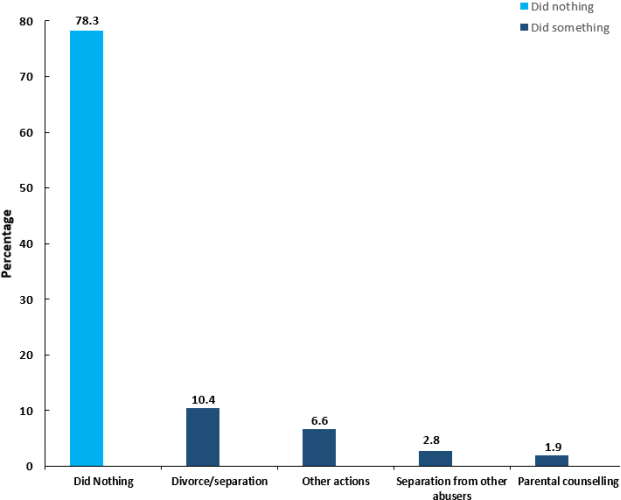
3.5. Actions Taken Against Perpetrators of SRHR Violations (Figure 2) Figure 2 shows the actions taken by respondents against perpetrators of SRHR violations. The majority of respondents (78.3%) reported taking no action against the perpetrator.
Among those who took action, divorce or separation from abusive husbands (10.4%) was the most frequently reported response. Other actions included unspecified responses (6.6%), separation from other abusers (2.8%), and parental counselling (1.9%).
3.6. Qualitative Findings
The focus group discussions provided additional insights into women’s experiences of SRHR violations and their responses to them.
Participants frequently reported sexual violence and coercion by intimate partners, often associated with pressure to continue childbearing or comply with marital sexual expectations. Several participants described severe physical abuse and its health consequences, including miscarriage, hypertension, and psychological distress.
Some participants also highlighted the influence of cultural norms and gender expectations, which often discourage women from challenging abusive behaviour or seeking external help. Many reported that violations of SRHRs are typically managed within families or through mediation by community elders rather than through formal legal systems.
Despite these challenges, some women described strategies for exercising their reproductive rights, including negotiating family planning with their spouses, using contraception discreetly, or seeking support from family members and community leaders.
4. Discussion
This study examined the experience of violations and the exercise of sexual and reproductive health rights among ever-married women in Ibadan metropolis. The findings highlight that violations of SRHRs remain relatively common, with approximately one in four respondents reporting experiencing abuse of their rights.
The most frequently reported violation was sexual violence, which aligns with findings from the Nigeria Demographic and Health Survey (NDHS) indicating that a substantial proportion of women experience violence from intimate partners
| [9] | National Population Commission: Nigeria Demographic and Health Survey. 2019. |
[9]
. However, the prevalence of sexual violence observed in this study was slightly higher than national estimates. This difference may be explained by methodological variations, particularly the lifetime measurement of sexual violence in this study compared with the NDHS focus on violence within the preceding 12 months.
Similar findings have been reported in other Nigerian studies. For instance, research conducted in Ile-Ife documented sexual violence prevalence ranging from 21% to 30% among women of reproductive age
| [13] | Mapayi B, Makanjuola ROA, Mosaku SK, Adewuya OA, Afolabi O, Aloba OO, Akinsulore A: Impact of intimate partner violence on anxiety and depression amongst women in Ile-Ife, Nigeria. Arch Womens Ment Health. 2013, 16: 11–8.
https://doi.org/10.1007/s00737-012-0307-x |
[13]
. Another study in Ibadan reported lower levels of sexual violence but higher prevalence of physical violence
| [14] | Owoaje E, OlaOlorun F: Women at risk of physical intimate partner violence: a cross-sectional analysis of a low-income community in southwest Nigeria - PubMed. Afr J Reprod Health. 2012, 16: 43–53. |
[14]
. These variations may reflect differences in cultural contexts, partner behaviours such as alcohol consumption, and differences in study design.
Husbands were identified as the primary perpetrators of sexual violence in this study, a finding that reinforces evidence that intimate partner violence is a major contributor to violations of women’s reproductive rights. National data similarly indicate that intimate partners account for the majority of violence experienced by women in Nigeria
| [9] | National Population Commission: Nigeria Demographic and Health Survey. 2019. |
[9]
. This pattern reflects entrenched patriarchal norms and unequal gender power relations that often limit women's autonomy within marriage.
Despite the prevalence of violations, more than half of the respondents who experienced abuse reported taking some form of action against the violation or the perpetrator. This proportion is higher than the NDHS estimate, where only about one-third of women reported seeking help after experiencing violence
| [9] | National Population Commission: Nigeria Demographic and Health Survey. 2019. |
[9]
. The difference may be explained by the study population, which focused specifically on ever-married women who may have stronger family support networks or greater agency in addressing marital conflicts.
The qualitative findings provide additional insights into how SRHR violations are managed within communities. Many participants reported that such issues are typically addressed within families or through mediation by community elders rather than through formal legal or institutional mechanisms. Similar patterns have been observed in other African contexts where cultural norms favour family-based dispute resolution rather than formal justice systems.
The limited use of formal legal channels also highlights potential gaps in awareness of available support services and weak enforcement of laws protecting women's reproductive rights. Nigeria’s legal framework addressing SRHR violations has been described as fragmented and inadequately enforced, potentially discouraging women from seeking formal redress
| [15] | Mairiga AG, Geidam AD, Bako B, Ibrahim A: Nigerian Lawyers and Reproductive Health Rights : A Survey of Knowledge, Practices and Opinions on Law Reforms among the Bar and Bench in North Eastern Nigeria. Afr J Reprod Health. 2012. 16(1): 69–74. https://doi.org/10.4314/ajrh.v16i1 |
[15]
.
Overall, the findings underscore the complex interplay between cultural norms, gender relations, and institutional factors in shaping women’s experiences of reproductive rights. Interventions aimed at improving women's ability to exercise their SRHRs should therefore address both structural barriers and socio-cultural attitudes that perpetuate gender inequality. Community-based programmes aimed at preventing intimate partner violence and promoting reproductive autonomy should integrate education on sexual and reproductive health rights, legal literacy, and access to support services. Strengthening primary healthcare systems and community health programmes to include SRHR counselling and referral pathways may improve early detection and response to violations. Such interventions are essential for advancing gender equality and improving reproductive health outcomes in Nigeria.
5. Conclusion
One in four respondents reported experiencing violations of sexual and reproductive health rights, with sexual violence being the most prevalent form of abuse and husbands identified as the main perpetrators. Although many women reported exercising their SRHRs in different ways, responses to violations were often limited and largely managed within family structures rather than through formal institutional mechanisms. Strengthening awareness, legal protection, and community-based support systems is essential to improve women’s ability to exercise their sexual and reproductive health rights and reduce violations.
6. Recommendation
Efforts to address SRHR violations should involve community education, policy reforms, and improved enforcement of laws protecting women’s rights. Community leaders, healthcare providers, and government agencies should collaborate to promote awareness of SRHRs and provide support services for victims of abuse.
Abbreviations
SRHRs | Sexual and Reproductive Health Rights |
ICPD | International Conference on Population and Development |
SDGs | Sustainable Development Goals |
LGAs | Local Government Areas |
FGDs | Focus Group Discussions |
NDHS | Nigerian Demographic and Health Survey |
Author Contributions
Sarah Eseoghene Abraham: Formal Analysis, Investigation, Methodology, Resources, Writing – original draft
Ayodeji Matthew Adebayo: Conceptualization, Supervision
Conflicts of Interest
The authors declare that there is no conflict of interest regarding the publication of this paper.
Appendix
Table 1. Experience of violation of SRHRs by respondents (N=423).
Variable | Total n (%) |
Ever abused of SRHRs (N=423) | |
Yes | 106 (25.1) |
No | 317 (74.9) |
SRHRs abused (n=106) | |
Right to freedom from violence* | 31 (29.3) |
Right to freedom from abuse** | 20 (18.7) |
Right to marital sexual harmony | 12 (11.3) |
Right to childcare | 8 (7.5) |
Right to family planning | 7 (6.6) |
Right to health programs/services | 3 (2.8) |
Right to consent to marriage | 4 (3.8) |
Right to marriage | 2 (1.8) |
Right to childbearing | 2 (1.8) |
Right to postnatal care | 2 (1.8) |
Other SRHR violations | 5 (4.7) |
Non SRHR violations reported | 10 (9.4) |
SRHRs abuser (n=106) | |
Husband | 41 (38.7) |
Friend | 31 (29.2) |
Relatives | 18 (17.0) |
Parents | 8 (7.5) |
Neighbour | 5 (4.7) |
Others* | 3 (2.8) |
Other SRHR violations include right to abortion, body control, freedom from discrimination, motherhood, and resistance to genital mutilation.
* Sexual-27, Unspecified-4
** Unspecified form-20, Verbal-8, Non-consensual body touch-2.
*** Right to abortion-1, Right to body control-1, Right to freedom from discrimination-1,
Right to motherhood-1, Right to resist genital mutilation-1
**** Right to choice of religion-1, Right to financial provision-4, Right to homecare-3,
Right to freedom of movement-1, Right to work-1
Table 2. Exercise of SRHRs by respondents.
Variable | n (%) |
Ever used any SRHRs (n=423) | |
Yes | 381 (90.1) |
No | 42 (9.9) |
SRHRs ever used (n=381) | |
Right to marriage | 118 (27.9) |
Right to family planning | 108 (25.1) |
Right to childcare | 24 (5.7) |
Right to have sex | 20 (4.7) |
Right to child bearing | 19 (4.5) |
Right to freedom from abuse/violence | 12 (2.8) |
Right to health programs/services | 12 (2.8) |
Right to body control | 11 (2.6) |
Right to antenatal care | 8 (1.9) |
Right to consent to marriage | 5 (1.2) |
Right to maternity services | 3 (0.7) |
Right to immunization | 1 (0.2) |
Non-SRHR responses | 15 (3.5) |
None reported | 45 (10.2) |
Table 3. Actions Taken Following Violation of SRHRs (n=106).
Variable | n (%) |
Action taken against Violation | |
Took no action | 53 (50.0) |
Took action | 53 (50.0) |
Action against the perpetrator | |
Took no action | 83 (78.3) |
Took action | 23 (21.7) |
Overall exercise of SRHR after violation | |
Yes | 61 (57.5) |
No | 45 (42.5) |
Table 4. Socio-demographic characteristics of FGD participants (N = 43).
Variable | n (%) |
Marital status | |
Married | 29 (67.4) |
Cohabiting | 10 (23.3) |
Widowed | 3 (7.0) |
Separated | 1 (2.3) |
Family type | |
Monogamous | 23 (53.5) |
Polygamous | 20 (46.5) |
Number of children | |
None | 4 (9.3) |
1-2 | 12 (28.0) |
3-4 | 22 (51.1) |
5-6 | 5 (11.6) |
Mean number of children ± SD | 2.8 ±1.5 |
Level of education | |
No formal education | 3 (7.0) |
Primary education | 18 (41.9) |
Secondary education | 19 (44.2) |
Tertiary education | 3 (7.0) |
Occupation | |
Unemployed/ Housewife | 1 (2.3) |
Artisan | 7 (16.3) |
Trader | 33 (76.7) |
Teacher/Civil servant | 2 (4.7) |
Ethnicity | |
Yoruba | 43 (100) |
Religion | |
Islam | 26 (60.5) |
Christianity | 17 (49.5) |
Figure 1. Actions taken following violation of SRHRs.
Figure 2. Actions taken against abusers of SRHRs.
References
| [1] |
Amnesty International USA: Sexual and Reproductive Health Rights. What is sexual and reproductive health? 2015.
|
| [2] |
World Health Organization: WHO working definition. Geneva; 2010.
|
| [3] |
Guttmacher Institute: A Time to Lead: A Roadmap for Progress on Sexual and Reproductive Health and Rights Worldwide. 2018.
|
| [4] |
International Planned Parenthood Federation: Sexual and reproductive health and rights are the key to gender equality and sustainable development | IPPF. 2015.
|
| [5] |
World Health Organization: Global and regional estimates of violence against women Prevalence and health effects of intimate partner violence and non-partner sexual violence. World Health Organization: Geneva; 2013.
|
| [6] |
Muluneh MD, Stulz V, Francis L, Agho K: Gender Based Violence against Women in Sub-Saharan Africa: A Systematic Review and Meta-Analysis of Cross-Sectional Studies. Int J Environ Res Public Health. 2020, 17: 903.
https://doi.org/10.3390/ijerph17030903
|
| [7] |
United Nations Human Rights: Sexual and reproductive health and rights. 2015.
|
| [8] |
United Nations Human Rights: Declaration on the Elimination of Violence against Women | OHCHR. United Nations Hum. Rights. (1993), 1–4.. Accessed: August 8, 2022.
https://www.ohchr.org/en/instruments-mechanisms/instruments/declaration-elimination-violence-against-women
|
| [9] |
National Population Commission: Nigeria Demographic and Health Survey. 2019.
|
| [10] |
World Health Organization: Promoting sexual and reproductive health for persons with disabilities. 2009.
|
| [11] |
Makinde OA, Adebayo AM: Knowledge and perception of sexual and reproductive rights among married women in Nigeria. Sex Reprod Heal Matters. 2020, 28: 1731297.
https://doi.org/10.1080/26410397.2020.1731297
|
| [12] |
Adinew YM, Worku AG, Mengesha ZB: Knowledge of reproductive and sexual rights among University students in Ethiopia: institution-based cross-sectional. BMC Int Health Hum Rights. 2013, 13: 12.
https://doi.org/10.1186/1472-698X-13-12
|
| [13] |
Mapayi B, Makanjuola ROA, Mosaku SK, Adewuya OA, Afolabi O, Aloba OO, Akinsulore A: Impact of intimate partner violence on anxiety and depression amongst women in Ile-Ife, Nigeria. Arch Womens Ment Health. 2013, 16: 11–8.
https://doi.org/10.1007/s00737-012-0307-x
|
| [14] |
Owoaje E, OlaOlorun F: Women at risk of physical intimate partner violence: a cross-sectional analysis of a low-income community in southwest Nigeria - PubMed. Afr J Reprod Health. 2012, 16: 43–53.
|
| [15] |
Mairiga AG, Geidam AD, Bako B, Ibrahim A: Nigerian Lawyers and Reproductive Health Rights : A Survey of Knowledge, Practices and Opinions on Law Reforms among the Bar and Bench in North Eastern Nigeria. Afr J Reprod Health. 2012. 16(1): 69–74.
https://doi.org/10.4314/ajrh.v16i1
|
Cite This Article
-
APA Style
Abraham, S. E., Adebayo, A. M. (2026). Violation and Exercise of Sexual and Reproductive Health Rights Among Ever-Married Women in Ibadan Metropolis: A Mixed-method Approach. European Journal of Preventive Medicine, 14(2), 25-33. https://doi.org/10.11648/j.ejpm.20261402.12
 Copy
|
Copy
|
 Download
Download
ACS Style
Abraham, S. E.; Adebayo, A. M. Violation and Exercise of Sexual and Reproductive Health Rights Among Ever-Married Women in Ibadan Metropolis: A Mixed-method Approach. Eur. J. Prev. Med. 2026, 14(2), 25-33. doi: 10.11648/j.ejpm.20261402.12
Copy
|
Download
AMA Style
Abraham SE, Adebayo AM. Violation and Exercise of Sexual and Reproductive Health Rights Among Ever-Married Women in Ibadan Metropolis: A Mixed-method Approach. Eur J Prev Med. 2026;14(2):25-33. doi: 10.11648/j.ejpm.20261402.12
Copy
|
Download
-
@article{10.11648/j.ejpm.20261402.12,
author = {Sarah Eseoghene Abraham and Ayodeji Matthew Adebayo},
title = {Violation and Exercise of Sexual and Reproductive Health Rights Among Ever-Married Women in Ibadan Metropolis: A Mixed-method Approach},
journal = {European Journal of Preventive Medicine},
volume = {14},
number = {2},
pages = {25-33},
doi = {10.11648/j.ejpm.20261402.12},
url = {https://doi.org/10.11648/j.ejpm.20261402.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ejpm.20261402.12},
abstract = {Sexual and reproductive health rights (SRHRs) are fundamental human rights that underpin gender equality, health, and sustainable development, yet violations remain widespread among women in many low- and middle-income settings due to entrenched socio-cultural norms, gender inequality, and unequal power relations within marriage. This study assessed both the violations and the exercise of SRHRs among ever-married women in Ibadan metropolis, Nigeria, using a community-based cross-sectional mixed-methods design. A total of 423 ever-married women aged 15–49 years were selected through multistage sampling from two Local Government Areas, with quantitative data collected via semi-structured interviewer-administered questionnaires and qualitative insights obtained from five focus group discussions; quantitative data were analysed using descriptive statistics and logistic regression, while qualitative data were subjected to thematic analysis. Overall, 25.1% of respondents reported experiencing violations of SRHRs, with the most common being violations of the right to freedom from sexual violence (29.3%), and husbands identified as the primary perpetrators (38.7%). Despite this, 90.1% of respondents reported exercising at least one SRHR, most commonly the right to marriage (27.9%) and the right to family planning (25.1%), and among those who experienced violations, 57.5% reported taking some form of action against the violation, the perpetrator, or both. Qualitative findings further highlighted intimate partner violence, coercive childbearing, and socio-cultural expectations as key drivers of SRHR violations. These findings indicate that SRHR violations remain prevalent among married women in Ibadan, underscoring the need to strengthen awareness, legal protections, and community support mechanisms to enhance women’s capacity to exercise their sexual and reproductive health rights.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Violation and Exercise of Sexual and Reproductive Health Rights Among Ever-Married Women in Ibadan Metropolis: A Mixed-method Approach
AU - Sarah Eseoghene Abraham
AU - Ayodeji Matthew Adebayo
Y1 - 2026/05/28
PY - 2026
N1 - https://doi.org/10.11648/j.ejpm.20261402.12
DO - 10.11648/j.ejpm.20261402.12
T2 - European Journal of Preventive Medicine
JF - European Journal of Preventive Medicine
JO - European Journal of Preventive Medicine
SP - 25
EP - 33
PB - Science Publishing Group
SN - 2330-8230
UR - https://doi.org/10.11648/j.ejpm.20261402.12
AB - Sexual and reproductive health rights (SRHRs) are fundamental human rights that underpin gender equality, health, and sustainable development, yet violations remain widespread among women in many low- and middle-income settings due to entrenched socio-cultural norms, gender inequality, and unequal power relations within marriage. This study assessed both the violations and the exercise of SRHRs among ever-married women in Ibadan metropolis, Nigeria, using a community-based cross-sectional mixed-methods design. A total of 423 ever-married women aged 15–49 years were selected through multistage sampling from two Local Government Areas, with quantitative data collected via semi-structured interviewer-administered questionnaires and qualitative insights obtained from five focus group discussions; quantitative data were analysed using descriptive statistics and logistic regression, while qualitative data were subjected to thematic analysis. Overall, 25.1% of respondents reported experiencing violations of SRHRs, with the most common being violations of the right to freedom from sexual violence (29.3%), and husbands identified as the primary perpetrators (38.7%). Despite this, 90.1% of respondents reported exercising at least one SRHR, most commonly the right to marriage (27.9%) and the right to family planning (25.1%), and among those who experienced violations, 57.5% reported taking some form of action against the violation, the perpetrator, or both. Qualitative findings further highlighted intimate partner violence, coercive childbearing, and socio-cultural expectations as key drivers of SRHR violations. These findings indicate that SRHR violations remain prevalent among married women in Ibadan, underscoring the need to strengthen awareness, legal protections, and community support mechanisms to enhance women’s capacity to exercise their sexual and reproductive health rights.
VL - 14
IS - 2
ER -
Copy
|
Download